
Abstract
The endothelial TIE1 and TIE2 receptor tyrosine kinases form a distinct subfamily characterized by their unique extracellular domains. Together with the angiopoietin growth factors (ANGPT1, ANGPT2, ANGPT4, also abbreviated as ANG), the TIE receptors form an endothelial specific signaling pathway with important functions in the regulation of lymphatic and cardiovascular development and vascular homeostasis. Angiopoietins exist in multimeric forms that activate the TIE receptors via unique mechanism. In endothelial cell–cell contacts, angiopoietins induce the formation of homomeric in trans TIE receptor complexes extending across the cell junctions, whereas matrix-bound angiopoietin-1 (ANG1) activates the TIE receptors in a cis configuration. In comparison to the vascular endothelial growth factor receptors, the TIE receptors undergo little ubiquitin-mediated degradation after activation, whereas TIE2 signaling is negatively regulated by the vascular endothelial protein tyrosine phosphatase, VE-PTP. ANG1 activation of TIE2 supports vascular stabilization, whereas angiopoietin-2 (ANG2), a context-dependent weak TIE2 agonist/antagonist, promotes pathological tumor angiogenesis, vascular permeability, and inflammation. Recently, ANG2 has been found to mediate some of its vascular destabilizing and angiogenic functions via integrin signalling. The circulating levels of ANG2 are increased in cancer, and in several human diseases associated with inflammation and vascular leak, for example, in sepsis. Blocking of ANG2 has emerged as a potential novel therapeutic strategy for these diseases. In addition, preclinical results demonstrate that genetic TIE1 deletion in mice inhibits the vascularization and growth of tumor isografts and protects from atherosclerosis, with little effect on normal vascular homeostasis in adult mice. The ability of the ANG-TIE pathway to control vessel stability and angiogenesis makes it an interesting vascular target for the treatment of the various diseases.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
16.1 Introduction to the TIE Receptor Tyrosine Kinase Family
TIE1 and TIE2 receptor tyrosine kinases (RTK) were isolated in the beginning of the 1990s [1–4]. They constitute a distinct RTK subfamily with a unique extracellular structure consisting of epidermal growth factor, immunoglobulin, and fibronectin type III domains (Fig. 16.1, Table 16.1). Angiopoietin growth factors (ANGPT1, ANGPT2, ANGPT4, also called ANG1, ANG2, ANG4 in humans) are ligands for TIE2 [5–7], while TIE1 is an orphan receptor. Besides the vascular endothelial growth factors (VEGFs) and their receptors, the angiopoietins and TIE receptors define the second endothelial specific RTK signaling pathway. The ANG-TIE system is important for cardiac, blood vascular, and lymphatic vessel development and for the homeostasis of the mature vasculature. The ANG-TIE system also regulates tumor angiogenesis, lymphangiogenesis, and metastasis as well as pathological endothelial inflammation and vascular leak in numerous diseases (reviewed in [8, 9]).

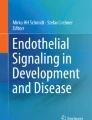
Schematic presentation of the angiopoietin-induced TIE1 and TIE2 receptor signaling complexes. Angiopoietin growth factors bind to the TIE2 receptor tyrosine kinase with similar affinity, inducing TIE receptor clustering. The activating ANG1 ligand induces phosphorylation of TIE2, and to some extent also TIE1 in cell–matrix (top, right) and cell–cellFig. 16.1 (continued) (top, left) contacts. In cell–cell contacts, the activated TIE2 receptor signals to stabilize the endothelium after angiogenic processes, and improve the endothelial barrier function, while in cell–matrix contacts, TIE2 stimulates endothelial migration. Pericellular matrix - α5β1-integrin interaction has been reported to promote ANG1-TIE2 signaling for cell survival and cell motility. Vascular sprouting may also involve ANG1 interactions with integrins on non-endothelial cells, such as astrocytes. ANG2 is a weak TIE2 agonist/antagonist, which can counteract ANG1 signaling in cell junctions (bottom, left), especially when its expression is increased, for example, in sepsis. High ANG2 levels also activate β1-integrin, which induces further destabilization of endothelial cell junctions, promoting vascular permeability (bottom, right). In endothelial tip cells, which express ANG2 but low levels of TIE2, ANG2 signals via integrins to promote vascular sprouting. In the tumor vasculature, and in stressed endothelial cells which are exposed to low levels of ANG1 signaling, ANG2 may provide cell survival signals. Deletion of the ligand-less TIE1 receptor inhibits atherosclerosis and tumor angiogenesis, and results in reduced TIE2 phosphorylation in Tie1 gene-targeted mice. The colors of the TIE receptor domains refer to the corresponding exon colors in Fig. 16.3

ANG2-β1-integrin signaling promotes endothelial destabilization. In shScramble (shScr) transfected control cells, β1-integrin promotes cell-cell adhesion and cortical actin cytoskeleton in the cell periphery via focal adhesions. In TIE2 silenced (shTIE2) endothelial cells, and in the endothelium of ANG2 transgenic mice [60] β1-integrin is localized in elongated matrix adhesions that connect to actin stress fibres and reduce the integrity of vascular endothelial-cadherin-containing cell–cell junctions. ANG2 was found to signal via β1-integrin when ANG2 levels were elevated or when TIE2 levels were decreased, leading to endothelial β1-integrin activation and cellular tension, which should contribute to reduced barrier function in diseased conditions, such as sepsis [60]. Image provided by Laura Hakanpää
16.2 The Role of the TIE Receptor Tyrosine Kinase Family in Vascular Development
After the initial assembly of the primary vascular plexus, which requires VEGF-dependent signals, the ANG-TIE system is necessary for cardiac development and for the remodeling of both the blood and lymphatic vasculatures after mid-gestation [8]. Gene-targeted mouse models have revealed a unique function for the ANG1-TIE2 pathway during cardiac development and for TIE1 and TIE2 during later stages of angiogenic capillary growth. Furthermore, TIE1, ANG2 and ANG1 regulate postnatal growth of the retinal vasculature [10–13]. The TIE receptors and their angiopoietin ligands are also required for lymphatic development via effects on vessel remodeling, maturation and valve morphogenesis [14–17].
16.2.1 Ang1 and Tie2 in Cardiac and Vascular Development
Tie2 gene-targeted mouse embryos show severely impaired cardiac development, reduced numbers of endothelial cells, and hemorrhages, resulting in embryonic lethality by E10.5 [18]. Gene-targeted embryos deficient of the Tie2 ligand Ang1 die by E12.5 [5]. They have a very similar phenotype, including impaired cardiac development and less complex vascular structures. In addition, the endothelial cells in the Ang1 −/− embryos are rounded and poorly associated with basement membranes [5]. Myocardial Ang1 expression appears to stimulate coronary vein formation, by promoting the proliferation, migration, and differentiation of immature endothelial cells derived from the sinus venosus [19]. Interestingly, cardiac-specific Ang1 deletion during embryogenesis largely phenocopied the ubiquitous loss of Ang1. The deletion of Ang1 after E13.5 was compatible with life; however, postnatal retinal angiogenesis was defective [11, 12]. Ang1 does not appear to be required for normal homeostasis in the adult vasculature, but it is required to limit pathological angiogenic responses and fibrosis after injury or during microvascular stress [11, 12].
16.2.2 Tie1 Regulates Vascular and Lymphatic Development
Endothelial integrity is impaired in the Tie1 gene-targeted mouse embryos, resulting in hemorrhages and lethality at E13.5 [20]. Tie1 is required for endothelial cell survival and for capillary growth during late phases of embryonic angiogenesis, especially in the developing kidney and the brain [21]. The deletion of both Tie1 and Tie2 causes more severe defects in vascular integrity than single gene deletions, and mosaic analysis has demonstrated that both Tie1 and Tie2 are required in endothelial cells during late phases of embryonic development and in adult tissues [22]. Postnatal conditional deletion of Tie1 decreased angiogenic sprouting in the developing retinal vasculature, but had little effect on mature vessels in adult tissues [13].
Tie1 is also critical for lymphatic vascular development. Conditionally targeted Tie1 embryos showed severe edema and abnormal formation of jugular lymph sacs at E13.5–14.5 [14, 15]. A genetic Tie1 mouse model, with conditionally targeted Tie1 endodomain, demonstrated abnormal lymphatic collecting vessels and defective lymphatic valve formation between E15.5 and E18.5, and during postnatal life [16].
16.2.3 Ang2/Ang1-Tie2 Pathway Is Critical for Lymphatic Vascular Remodeling
Ang2-deficient mice die postnatally or survive until adulthood, depending on the genetic background [10]. Newborn Ang2-deleted mice suffer from generalized lymphatic dysfunction, including subcutaneous edema and chylous ascites [10]. Their collecting lymphatic vessels fail to undergo proper postnatal maturation and have abnormal smooth muscle cell coating, whereas the lymphatic capillaries are hypoplastic and disorganized [10, 23].
Ang2 is indispensable for lymphatic remodeling; genetic deletion or administration of blocking ANG2 antibodies at different stages during embryonic development prevented the maturation of zipper-like junctions to button-like junctions of the lymphatic capillary endothelium and inhibited the phosphorylation of VE-cadherin at Tyr685, whereas in the collecting lymphatic vessels the adherens junctions were disrupted, resulting in compromised lymph drainage [24]. Embryonic Ang2-blockade suppressed also the formation and maturation of the lymphatic valves [24].
When expressed in the Ang2 genetic locus, Ang1 was able to complement the lymphatic defects of Ang2 gene-targeted mice, indicating that Ang2 and Ang1 function similarly in the lymphatic vasculature, likely as Tie2 agonists [10].
Conditional deletion of Ang1 and Ang2 in double knockout mice demonstrated lack of Schlemm’s canal and lymphatic capillaries in the corneal limbus, leading to a dramatic increase in intraocular pressure and glaucoma [25]. The lymphatic defects in the Ang1 and Ang2 double knockout mice were more severe than in the Ang2 single knockout mice, suggesting that both Ang1 and Ang2 contribute to the formation of the lymphatic vasculature in the eye [25]. Furthermore, deletion of both Ang1 and Ang2 at E12.5, but not Ang2 alone, resulted in subcutaneous edema in the embryos. The lymphatic phenotypes of Ang1 and Ang2 double knockout mice resembled those observed upon conditional Tie2 deletion, suggesting that compensatory mechanisms regulate lymphatic development via Tie2 [25].
Ectopic overexpression of Ang2 in developing mouse embryos resulted in blood vascular defects similar to those in Ang1- and Tie2-deficient embryos, which initially suggested that ANG2 acts as a TIE2 antagonist in the vascular endothelium [6]. However, the blood vascular defects of Ang2 −/− mice were limited to the development of the postnatal ocular vasculature, where Ang2 was required for the regression of the hyaloid vessels and for sprouting of the retinal vasculature [10]. These results suggest that ANG2 may present its context-dependent antagonistic function during development of the eye vasculature, where it functions to destabilize the existing hyaloid blood vessels.
16.3 The Role of the TIE Receptor Tyrosine Kinase Family in Physiology and Disease
The ANG-TIE system regulates vascular homeostasis and it is also implicated in numerous vascular diseases. Therefore, the ANG-TIE system has become a target of investigational vascular therapies [26]. ANG1 mediates vascular protection via TIE2 activation, and recombinant or viral vector delivery of ANG1 protein has been considered as a potential means for alleviating vascular complications of diabetes and sepsis, which may result in acute lung and kidney injury [27]. The potential of ANG1 to induce organized neovascularization with non-leaky vessels has stimulated research on ANG1 as a therapy for ischemic diseases [28–30]. Reduced TIE receptor expression has been associated with susceptibility to vascular complications caused by hemorrhagic Ebola virus infection, whereas activating TIE2 mutations contribute to the development of cutaneomucosal venous malformations [31, 32]. In contrast, inhibition of ANG2 has shown beneficial effects in reducing vascular leakage, alleviating e.g. sepsis-induced lung injury and harmful inflammation associated with cardiac transplant rejection [33, 34]. Inhibition of ANG2 [35] and TIE1 may provide protection from atherosclerosis, and inhibition of both ANG2 and TIE1 has been demonstrated to decrease tumor angiogenesis and growth [13, 36–39].
16.3.1 TIE2 Mutations in Vascular Malformations
Vascular anomalies are developmental vascular defects and consist of a variety of hereditary and sporadic disorders. Germline TIE2 mutations (most common is the point mutation R849W) cause the inherited cutaneomucosal venous malformation (VMCM) syndrome, which is characterized by multifocal small bluish cutaneous and mucosal lesions, composed of enlarged, tortuous venous channels [40]. The patients are also affected by somatic ‘second hit’ mutations causing loss of function of the second TIE2 allele [31].
Somatic TIE2 mutations cause a more common, sporadic form of venous malformation (VM), characterized by extensive unifocal lesions and enlarged venous channels with patchy smooth-muscle cell layers and a thin, continuous TIE2-positive endothelial cell layer [31, 41]. When ectopically expressed in cultured endothelial cells, the VM-associated mutant TIE2 proteins, including the R849W mutant, were hyperphosphorylated. However, the level of hyperphosphorylation did not correlate with the clinical phenotype of the patients [31]. Some of the TIE2 mutations, for example, L914F, affected the subcellular localization of TIE2, resulting in impaired receptor localization on the cell surface, increased Akt and STAT1 phosphorylation, and decreased platelet-derived growth factor B expression, which may contribute to the weak pericyte–endothelial cell association observed in the VM lesions [31, 42].
16.3.2 ANG-TIE System in Cancer
Circulating ANG2 levels have been identified as an independent factor predicting poor prognosis in many human cancers, including metastatic melanoma, colorectal cancer (CRC), and chronic lymphocytic leukemia [26]. Several approaches to target the ANG-TIE system are in clinical development for the treatment of human cancer, some of these have advanced into phase III trials [43]. In contrast to VEGF, which is highly expressed by many tumor cells, tumor cell lines express very little ANG2 [8]. Instead, ANG2 mRNA expression was detected in cells of the tumor stroma in patients with metastatic CRC [44], in line with preclinical data from mouse tumor models [45]. Interestingly, low pre-therapeutic circulating ANG2 levels were associated with a better response to bevacizumab in CRC patients, suggesting that circulating ANG2 may provide a biomarker for anti-angiogenic therapies in CRC, where bevacizumab is used in combination with chemotherapy [44].
In preclinical models, blocking of the ANG-TIE interaction has been demonstrated to inhibit tumor angiogenesis and lymphangiogenesis. These studies used different ANG2 and ANG1/ANG2 blocking agents in various mouse tumor or xenograft models, either as monotherapy or in combination with VEGF signaling inhibitors, which showed synergistic effects (reviewed in [9]). Mechanistically, the function of ANG2 in tumor angiogenesis is not well known. ANG2 expression has been detected as one of the first markers of the activated endothelium of co-opted tumor blood vessels. ANG2 is thought to cause endothelial destabilization, leading to vessel regression, hypoxia, and increased expression of both ANG2 and VEGF, which together induce robust angiogenesis in the tumor (angiogenic switch) [45]. However, ANG2 has been also proposed to act as a TIE2 agonist in tumors, promoting endothelial cell survival in the tumor vasculature, where the ANG2/ANG1 ratio is elevated [46].
In addition, ANG2 appears to contribute to the vascular phenotype of tumors by inducing pericyte detachment and endothelial cell sprouting [47, 48], while blocking ANG2 results in the normalization of tumor vessels with increased levels of adhesion molecules at endothelial cell-cell junctions, increased pericyte coverage, reduced endothelial cell sprouting, and vascular remodeling, producing smaller, more uniform vessels [36]. Some of the vascular normalization effects of ANG2 blocking therapies may be mediated by ANG1 [36]. A chimeric cartilage oligomeric matrix protein-angiopoietin-1 (COMP-ANG1) induced vessel normalization and improved vessel perfusion, potentiating chemotherapy in a syngeneic mouse tumor model [49, 50].
Anti-angiogenic therapies have been suggested to enhance invasive tumor growth [51, 52], while ANG2 blocking inhibits tumor lymphangiogenesis and decreases lymph node and distant metastasis [37, 39]. Anti-ANG2 antibodies inhibited tumor cell extravasation and lung metastasis by improving endothelial cell–cell junctions of tumor-associated pulmonary capillaries [39]. Mechanistically, the ANG2 blocking antibody not only inhibited ANG2 binding to TIE2, but also induced the internalization of the ANG2-TIE2 complexes [39]. Blocking ANG2 was also reported to modulate the functions of TIE2-expressing macrophages (TEMs), which form a subpopulation of tumor-associated proangiogenic myeloid cells [37]. Furthermore, ANG2 neutralization effectively reduced the growth of pancreatic RIP1-Tag2 tumors, which developed evasive resistance to VEGFR-2 inhibitors partly via increased ANG2/TIE2 expression [53].
16.3.3 Tie1 in Cancer and Cardiovascular Disease
TIE1 is expressed in the endothelium of tumor vessels [54]. Recent results demonstrated reduced tumor growth and postnatal angiogenesis in mice with endothelial Tie1 deletion [13]. Endothelial cell apoptosis was increased in tumors grown in Tie1-deficient mice, whereas the normal vasculature was not affected [13]. In addition, Tie1 deletion reduced tumor growth and angiogenesis to a similar extent as VEGF signaling inhibitors. Interestingly, additive tumor growth inhibition was obtained with the soluble Tie2 ectodomain capable of neutralizing ANG ligands, but not with VEGF inhibitors when used in the Tie1-deficient mouse background [13].
Furthermore, Tie1 deletion appears to protect mice from atherosclerosis. Tie1 is induced at sites of turbulent vascular flow in arteries, and the deletion of Tie1 provided a benefit for Apoe −/− mice on regular diet, by decreasing the number of atherosclerosis plaques [38].
16.3.4 ANG-TIE System in Vascular Leak and Therapeutic Angiogenesis
Circulating ANG2 levels are significantly elevated in diseases characterized by endothelial destabilization and vascular leak, such as sepsis, acute lung and kidney injury and acute respiratory distress syndrome (ARDS) [55]. Ang2 appears to contribute to endothelial barrier disruption in sepsis-associated lung injury, but excess systemic Ang2 has been also reported to provoke pulmonary vascular leak and congestion in otherwise healthy adult mice [56].
Mice heterozygous for Ang2 were protected from sepsis-induced kidney and lung injury, demonstrating less tissue inflammation and vascular leakage compared to wild-type mice, whereas Tie2 heterozygous mice were more susceptible to endotoxin-induced lung injury [27, 57]. In addition, ANG2 blocking antibodies reduced hemodynamic alterations and mortality rate in mice with lipopolysaccharide (LPS)-induced sepsis [33]. Furthermore, siRNA silencing of Ang2 in the pulmonary endothelium improved the survival of mice following cecal ligation and puncture, both as a pretreatment and as a rescue intervention [58]. On the other hand, ectopically provided ANG1 alleviated sepsis-induced lung injury [27]. These results suggest that ANG2 promotes, whereas ANG1-TIE2 signaling protects from the drastic consequences of sepsis. The vascular protective signals emanating from ANG1-TIE2 receptor complexes are well studied, whereas ANG2 signaling mechanisms in vascular pathologies are less well understood. However, ANG2 can increase vascular leak induced by many inflammatory cytokines [59]. Decreased Tie2 levels have been reported in the vasculature during septic shock; these may further aggravate the disease [27]. Reduced Tie2 expression was also associated with susceptibility to fatal vascular complications induced by hemorrhagic Ebola virus infection in mice [32]. A recent study demonstrated that when TIE2 levels are reduced or when ANG2 levels are increased, ANG2 can signal via β1-integrin to induce endothelial retraction and destabilization of endothelial cell junctions, a mechanism that may be in place in conditions with increased vascular leak [60] (Fig. 16.2).
ANG2 is also a pro-inflammatory molecule: ANG2 sensitizes endothelial cells to TNF-α signaling to induce expression of endothelial cell adhesion molecules [61]. In a mouse model of chronic airway inflammation, ANG2 blocking agents decreased the remodeling of mucosal capillaries into venules, the amount of leukocyte recruitment, and disease severity [62]. Ang2 is also highly upregulated in the retinas of diabetic rats. Reduced Ang2 gene dosage inhibited diabetes-induced pericyte loss and the formation of acellular capillary segments, suggesting a critical function for ANG2 in diabetic retinopathy [63]. ANG2-induced pericyte apoptosis seems to occur under high glucose via an integrin-dependent pathway [64].
In contrast to ANG2, ANG1 is anti-inflammatory, stimulates endothelial cell survival, and inhibits vascular permeability via multiple mechanisms including direct effects on the endothelial cell glycocalyx [65]. The potential of ANG1 to promote vascular stability and barrier function as well as to stimulate organized vascular remodeling resulting in non-leaky vessels makes ANG1 a potential therapeutic agent in numerous diseases [28, 30]. For example, ANG1 can improve the integrity of lymphatic vessels in inflamed skin after UVB irradiation by modulating expression of tight junction molecules [66]. The recombinant-soluble ANG1 protein, COMP-ANG1, promoted angiogenesis and suppressed inflammation in sciatic nerves of diabetic (ob/ob) mice, suggesting that COMP-ANG1 could improve the morphologic and molecular changes associated with diabetic neuropathy [67]. Adenoviral delivery of COMP-ANG1 also promoted diabetic wound healing by enhancing angiogenesis, lymphangiogenesis, and blood flow [68]. The genetic deletion of Ang1 in adult mice demonstrated that Ang1 limits pathological tissue fibrosis during wound healing and protects from microvascular disease in streptozotocin-induced diabetes [11]. In preclinical mouse models, endothelial dysfunction during hypertension was reduced by expression of the COMP-ANG1 protein. The treatment reduced the hypertension-associated cardiovascular and renal damage and prevented further elevation of blood pressure [69].
Ischemia followed by reperfusion occurs as a consequence of organ transplantation, treatment of hypotension, and major surgeries and may induce microvascular endothelial cell injury, leading to deregulation of vascular tone, tissue perfusion, permeability, and inflammation. In a renal ischemia–reperfusion model, COMP-ANG1 reduced vascular defects, vascular permeability and interstitial fibrosis, and preserved tissue perfusion, thereby improving renal function [70]. Similar beneficial effects were observed in a renal artery clamping model when rats were treated with simvastatin, a HMG-CoA reductase inhibitor, which inhibits hypoxia-induced release of ANG2 from endothelial Weibel-Palade bodies [71]. During cardiac transplantation, ischemia–reperfusion injury can trigger innate and adaptive immune responses that may lead to rejection, myocardial injury, and death, a series of events associated with increased ANG2 levels [34]. Interestingly, a single ex vivo intracoronary injection of ANG2 blocking antibodies reduced vascular permeability, myocardial injury, and associated inflammation by preventing leukocyte infiltration and expression of endothelial cell adhesion molecules, eventually leading to prolonged allograft survival [34].
Use of ANG1 for therapeutic neovascularization of ischemic tissues has gained interest because initial attempts to sustain neovascularization with VEGF family growth factors resulted in serious side effects. A recombinant protein made by fusion of the receptor-binding domains of VEGF and ANG1 growth factors, the VA1 chimera, was shown to be a potent angiogenic factor that triggers a novel mode of VEGFR-2 activation, promoting less vessel leakiness, less tissue inflammation, and better perfusion in ischemic muscle than VEGF [29]. In contrast, transgenic expression of ANG2 was shown to inhibit collateral artery growth and smooth muscle cell recruitment after arterial occlusion, thereby impairing perfusion and increasing necrosis in the ischemic limb [72].
16.4 TIE1 and TIE2 Genes
The TIE1 and TIE2 genes are conserved in numerous species, and their orthologues are present in chordates, but not e.g. in C. elegans or D. melanogaster. TIE1 and TIE2 are expressed mainly in the endothelial cells, with some expression in certain hematopoietic cell lineages, including TIE2-positive hematopoietic stem cells and a subpopulation of proangiogenic TIE2-positive macrophages [73–77]. Tie1 expression is induced during vascular remodeling, in tumors, and by disturbed flow in vascular bifurcations and branching points of arteries, whereas TIE1 expression is reduced by shear stress [54, 78, 79]. TIE1, ANGPT2, and TIE2 mRNAs are strongly expressed also in cells of Kaposi’s sarcoma tumor cells, and in cutaneous angiosarcomas [80].
16.4.1 TIE1
The human TIE1 gene, located in chromosome 1p34-p33, is expressed in an endothelial cell-specific manner [73]. High expression of Tie1 is found in adult lung, heart, and placenta. Moderate levels are present in the kidney, while skeletal muscle, brain, liver, and pancreas have less prominent expression. Tie1 expression starts at about E8.5 during mouse embryonic development [78]. Tie1 mRNA is detected in differentiating angioblasts of the head mesenchyme, in the splanchnopleura and dorsal aorta, as well as in migrating endothelial cells of the developing heart, in the heart endocardium, and in endothelial cells forming the lung vasculature [78].
A TATA- or CAAT-box is absent from the TIE1 promoter. Critical promoter/enhancer elements that determine endothelial expression are located within several hundred nucleotides upstream of the major transcription initiation site. These elements include several binding sites for members of the Ets transcription factor family (NERF-2, ELF-1, and ETS2) and an octamer transcription factor binding site [81]. This part of the promoter is conserved between mice and humans [73], and it contains most of the promoter specificity determining sequences [82]. Hence, it has been frequently utilized to drive endothelial cell-specific expression of transgenes [82, 83].
TIE1 is also expressed in cultured endothelial cells, some hematopoietic progenitor cells, and some myeloid leukemia cell lines having erythroid and megakaryoblastoid characteristics [76] and in adult acute myelogenous leukemia [84].
16.4.2 TIE2
The TIE2 gene (TEK) is very similar to the TIE1 gene (Fig. 16.3). It features also 23 exons, although they span a much larger genomic region than TIE1 exons (121 kb on chromosome 9p21 in comparison with 22 kb for the TIE1 gene). Endothelial specific expression is controlled by transcription factor binding sites in the first intron of the Tie2 gene [83, 85, 86]. In addition, TIE2 is expressed in several hematopoietic cells, most notably in hematopoietic stem cells (HSCs), where ANG1-induced signals regulate HSC niche regeneration and vascular leakiness [74, 77]. TIE2 is also expressed in a subpopulation of type M2 monocytes (TEMs), with tumor and angiogenesis-promoting properties [75] and in the muscle satellite cells, located among skeletal myofibers and associated with the microvasculature [87]. Ang1 derived from the quiescent satellite cells or fibroblasts in the muscle microenvironment promotes satellite cell quiescence for long-term self-renewal of adult muscle stem cells [87].

The exon/intron structures of the human and mouse TIE1 and TIE2 genes. Exons are shown as solid boxes and introns as brown lines. Exons are colored according to the domain structure: red, signal peptide/SP; green, immunoglobulin-like domain/Ig; magenta, epidermal growth factor-like domain/EGF; orange, fibronectin type 3 domain/FN3; cyan, transmembrane domain/TM; blue, tyrosine kinase domain/TK; black, not assigned to any domain. The black numbers above the exons indicate the exon length. The numbers for the first and last exons are split into the coding (black) and untranslated sequences (gray). The brown numbers under the larger introns indicate the intron length. The colored numbers under the exons refer to the corresponding amino acid residues. The total number of amino acid residues in the receptors is shown in black. *1,123 amino acid residues as deduced from the mouse genome project and one cDNA, and 1,122 amino acid residues according to the UniProtKB/Swiss-Prot database as deduced from three cDNAs. The assignment of the domain structure is according to the SMART protein domain research tool, except for the Ig-like and EGF-like domains, which are according to the TIE2 crystal structure determined by Barton et al. [103]
16.4.3 Alternative Splicing and Conservation
The exon–intron structure is highly conserved between TIE1 and TIE2 and also between the mouse and human TIE genes. Many alternative splice variants of TIE1 and TIE2 have been cloned or are found among EST sequences (see Alternative Splicing Database or Ensemble). Most but not all of the putative proteins resulting from such splice variants are likely not produced due to the lack of a functional signal peptide and thus their significance is unknown [88].
16.4.4 Gene Variants, Polymorphisms, and Somatic Mutations
No variants of the human TIE1 gene have been reported. However, somatic mutations affecting the extracellular and tyrosine kinase domains have been identified in cancer, including angiosarcoma [89, 90]. In contrast, mouse TIE1 features several sequence variants, which may be polymorphisms [4, 91, 92].
Multiple missense point mutations have been described in the human TIE2 gene. Most of them are located in sequences encoding the tyrosine kinase domain. They result in increased ligand-independent autophosphorylation and kinase activation and are linked to VMs [31, 39, 93, 94]. The mouse sequences for TIE2 similarly feature plenty of single amino acid variants, some of which correspond to human disease variants (for example, mouse R913G and human R915H). Notable is also a single valine insertion after position 786 of mouse TIE2, which is present in some cDNA sequences [29], but absent from others [2, 3, 34, 66]. This results from alternative splicing at the intron 14–15 splice donor site. Larger variations involving stretches of 7 to 17 amino acid residues likely represent sequencing artifacts since they represent frameshifted versions of the wild-type sequence with junctions at sites of repeated calls of individual bases [70]. Given the critical location of many of these sequence conflicts, the origin, verification, and documentation of TIE sequences used for experimental research are paramount.
16.4.5 Regulation of Transcription
Increased TIE2 expression has been reported in hypoxia in both endothelial cells and TEMs [95, 96]. The response is at least partially mediated by transcriptional activation, presumably involving the HIF-2 transcription factor [97]. However, there seems to be significant heterogeneity in the hypoxic response depending on the origin of the endothelial cells. Also, inflammatory cytokines such as TNFα and IL-1β upregulate TIE2 [95].
TIE1 expression is increased during wound healing, in proliferating ovarian capillaries during hormone-induced superovulation, and in tumor blood vessels [54, 78]. Tie1 is downregulated by shear stress [98], but induced by disturbed flow in vascular bifurcations and branching points of arteries [79]. TIE1, along with ANGPT2 and TEK mRNAs, is strongly expressed in cells of Kaposi’s sarcoma tumor cells, and in cutaneous angiosarcomas [80].
16.4.6 TIE Genes in Different Species
The TIE family has been considered not only metazoan specific, but also chordate specific as no TIE orthologues have been found in C. elegans or D. melanogaster [86, 99]. Receptor tyrosine kinase genes resembling the TIE gene (MBRTK1/RTKB5 and others) have been identified in the unicellular choanoflagellate Monosiga brevicollis. However, the weak similarity with the chordate Tie family might be due to convergent evolution [100, 101].
tie1 and tie2 orthologues are found in zebrafish, but they appear to have different functions than their mouse counterparts. In contrast to the phenotype of the Tie2 −/− mouse, tie2 −/− mutant fish are viable and have no vascular or heart phenotype. However, knockdown of zebrafish tie1 in the tie2 mutant background results in phenotypes similar to those of the Tie2 −/− mouse [102]. This suggests for functional redundancy between the fish tie2 and tie1 proteins. Furthermore, study of tie1 knockdown in fish suggests that tie1 but not tie2 is required for early stages of heart development. However, both tie1 and tie2 are indispensable in the later developmental stages for the maintenance of endocardial–myocardial interaction, a phenotype similar to that seen in Tie2 −/− mice, where poor association between endothelial cells and the myocardium is evident.
16.5 TIE1 and TIE2 Proteins
The TIE RTKs are characterized by a unique extracellular domain (ECD) for ligand binding, a single-pass transmembrane domain, and a cytoplasmic protein tyrosine kinase (TK) domain. The TIE ECDs consist of immunoglobulin, epidermal growth factor-like, and fibronectin type III repeats. Crystal structures of the angiopoietin–TIE2 complexes demonstrate that ANG1 and ANG2 bind to the same sites in TIE2 in a largely similar manner [103]. The mechanism of TIE2 activation remains elusive, although the oligomerization of angiopoietin ligands suggests that TIE2 activation requires its oligomerization [104–106]. Similar to other RTKs, the TIE2 oligomerization is likely to involve interactions between the ECDs and TIE2/TIE1 heterodimerization is mediated by interactions between their ECDs. Activation of the intracellular TIE tyrosine kinase domains is associated with phosphorylation of multiple tyrosine residues in the kinase domains and the C-terminal tail, which couples the TIE receptors to downstream signaling events [107].
16.5.1 Domain Structure and Posttranslational Modifications
The ECD of the TIE receptors is unique and consists of two immunoglobulin (Ig)-like domains, followed by three N-terminal epidermal growth factor (EGF)-like motifs, a third immunoglobulin (Ig)-like domain, and three fibronectin type III (FNIII) domains [1, 3]. The presence of the second Ig-like domain was revealed by the determination of the crystal structure of the TIE2 ligand-binding domain (LBD, residues 23–445) in complex with the ANG2 fibrinogen-like domain [103]. The crystal structure (Fig. 16.4) revealed a compact, arrowhead-shaped molecule containing the Ig-like domains (Ig1–Ig3) and the EGF-like domains (EGF1–EGF3). The surface loops of Ig2 are at the tip of the TIE2 arrowhead and alone comprise the ANG2 binding site [103]. Recently, a TIE2 structure including the first FNIII domain (FNIII-1) was solved in complex with the ANG1 fibrinogen-like domain [108]. The inflexible associations between Ig3 and FNIII-1 and the orientation of FNIII-1 to the opposite direction of the ligand-binding site suggest a rigid and elongated molecular architecture for the TIE2 ECD.

Crystal structures of the ANG2/TIE2 complex and the TIE2 kinase domain. (a) ANG2 fibrinogen-like domain in complex with TIE2 ligand-binding domain. TIE2 ligand-binding domain and ANG2 are colored in light blue and in light orange, respectively. TIE2 asparagine-linked carbohydrate groups are colored in red and shown as sticks. (b) Close-up view of the ANG2/TIE2 interface in (a). TIE2 Ig2 domain interacts with ANG2 P-domain. Hydrophobic residues, including Phe469 and Tyr475 from ANG2 and Phe161 from TIE2, dominate the interface. TIE2 Arg167 and ANG2 Asp448 mediate a salt-bridge. (c) TIE2 kinase domain. The N-terminal domain is colored green, C-terminal tail in light blue and the kinase insert domain (KID) in blue. The activation loop (A-loop) is highlighted in red
The TIE1 and TIE2 ECDs have an amino acid identity of 31 % and homology modeling of TIE1 revealed similar conserved overall folds and hydrophobic surfaces [109]. However, comparison of the surface electrostatic potentials revealed that TIE2 ECD has a slight negative overall charge, whereas TIE1 ECD has a positive overall charge, suggesting that patches of oppositely charged molecular surfaces in TIE1 and TIE2 may be involved in TIE1–TIE2 heterodimerization [109].
The intracellular domains of the TIE receptors are similar to those of VEGFR and PDGFR family members. Overall amino acid sequence identity between TIE1 and TIE2 intracellular domains is 76 %, which is much higher than for their extracellular domains. The kinase domain of human TIE2, residues 808–1124, folds into two domains, with catalysis occurring in a cleft between the two [110]. The structure contains an N-terminal domain (residues 808–904) responsible for ligating ATP and a C-terminal domain (residues 905–1,124) having the catalytic core. A short kinase insert domain (KID) comprised of two α-helical segments pack against the C-terminal tail. The overall fold of the TIE2 kinase domain is similar to that observed in other serine/threonine and tyrosine kinase structures. However, the activation loop (A-loop), the nucleotide-binding loop, and the C-terminal tail in the TIE2 kinase domain structure adopt self-inhibitory conformations [110]. The activation loop in TIE2, residues 982–1,008, contains a single tyrosine at position 992 and adopts an “activated-like” conformation. The nucleotide-binding loop contains residues responsible for binding of the ATP phosphate groups. In the TIE2 kinase domain, this loop, residues 831–836, occupies the ATP binding site. The C-terminal tail adopts an extended conformation to the active site and may inhibit substrate binding. Conformational changes needed for kinase domain activation may represent additional steps in the regulation of TIE2 activity.
TIE1 and TIE2 receptors contain multiple potential N-glycosylation sites. The structure of the TIE2 ligand binding domain revealed N-glycosylation in four of these sites, in Asn140 and Asn158 in Ig2 as well as in Asn399 and Asn438 in Ig3 [103]. Of these, only Asn158 (Asn161) is conserved in TIE1. The human TIE2 sequence contains additional, potential N-glycosylation sites in Asn464, Asn560, Asn596, Asn649, and Asn691. On the other hand, the human TIE1 sequence contains additional, potential N-glycosylation sites in Asn83, Asn503, Asn596, and Asn709. The crystal structure of the TIE2 ligand-binding domain revealed also fourteen disulfide bonds apparently stabilizing the structures of the individual TIE2 domains: one in both Ig1 and Ig3, and four in each of the EGF repeats.
16.5.2 Phosphorylation Sites and Primary Signaling Molecules
A characteristic feature of RTKs, such as VEGFRs, is their dimerization induced by the binding of a dimeric ligand, followed by autophosphorylation of the intracellular kinase domains. TIE receptor function is also regulated by ligand binding to the extracellular domain of the receptor. However, at least a trimeric ligand is required for TIE2 activation in endothelial cells, suggesting that the active TIE2 receptor complex is composed of more than two receptor subunits [104].
Following binding of the activating ANG1 ligand, TIE2 is autophosphorylated and intracellular signaling pathways are activated [111]. The C-terminal tail of TIE2 contains three tyrosine residues. Using a yeast two-hybrid system, it was demonstrated that five molecules, GRB2, GRB7, GRB14, the non-receptor-type protein tyrosine phosphatase 11 (PTPN11), and the p85 subunit of phosphatidylinositol 3-kinase (PI3K), interact with TIE2 in a phosphotyrosine-dependent manner [112]. Mapping of the binding sites of these molecules on TIE2 revealed a multisubstrate-docking site around Tyr1100 (mouse numbering) and a mutation of this site abolished GRB2 and GRB7 binding to TIE2. The p85 subunit of the PI3K has been shown also to associate with TIE2 Tyr1100 (cited Tyr1101 in [110]). This association results in PI3K activation [113]. Targeted mutation of the Tyr1100 in Tie2 showed impaired cardiac development as well as defective development of hematopoietic and endothelial cells in the mutant mice, but unlike the Tie2 knockout mice, the perivascular cells were normally associated with the blood vessels [114]. Site-directed mutagenesis of Tyr1100 reduced the association of GRB2, as expected, but PTPN11 association remained intact [115]. Conversely, the Y1111F (cited Y1112F in [110]) mutation did not affect GRB2 association but decreased association of PTPN11, indicating that PTPN11 is a phospho-Tyr1111-specific signaling molecule. On the other hand, Tyr1106 of mouse Tie2 (1,108 in human) was identified as an ANG1-dependent autophosphorylation site that is required for the binding and phosphorylation of the docking protein Dok-R [116]. Notably, phosphorylation of this Tie2 residue was reduced in Tie1-deficient mice [13]. No tyrosine residue equivalent to Tyr1106 is present in TIE1.
16.6 Ligands of the Tie Receptor Family
Angiopoietin growth factors (ANG1/ANGPT1, ANGPT2, and ANGPT4) are ligands for the TIE2 receptor, whereas TIE1 is an orphan receptor [117]. Yet, ANG1 activates TIE1, likely via an interaction with TIE2 [118, 119]. Angiopoietins have a unique structure, with a C-terminal TIE2 binding fibrinogen-like domain and N-terminal coiled-coil and superclustering domains that mediate angiopoietin oligomerization into dimers, trimers, and higher-order oligomers [105]. ANG1 is a strong activating ligand, whereas ANG2 is a weak ligand, despite homologous receptor-binding mechanisms [6]. Angiopoietin oligomerization is required for efficient TIE2 activation and clustering. The degree of angiopoietin oligomerization varies, and the possible regulation of various angiopoietin forms in vivo remains to be determined.
16.6.1 Angiopoietin Structure and Receptor Binding
The angiopoietin growth factors (ANGPT1, ANGPT2, and ANGPT4) consist of an N-terminal region lacking homology to any other structures, a coiled-coil domain (ANG1; residues 79–263) similar to structures found in proteins that induce multimerization, and a C-terminal fibrinogen-like region (ANG1, residues 284–498), which contains the TIE2-binding portion [6, 117, 120]. Indeed, crystal structure of the ANG2 fibrinogen-like region revealed a fibrinogen fold with a unique C-terminal P domain [121]. Furthermore, conservation analysis and structure-based mutagenesis identified a groove on the P domain surface that mediates TIE2 recognition and binding. The mechanism of ligand binding to TIE2 was confirmed by the determination of the crystal structures of the ANG1/TIE2 ECD and ANG2/TIE2 ECD complexes [103, 108]. Both ANG1 and ANG2 interact exclusively with the Ig2 domain of TIE2 via their C-terminal P domains.
Comparison of the free and receptor-bound ANG1 and ANG2 structures indicates that both ANG1 and ANG2 undergo only minor structural changes upon TIE2 binding and that the ANG1/TIE2 interface is very similar to the ANG2/TIE2 interface [108]. The TIE2 ligand-binding interface of about 1,300 Å2 is dominated by van der Waals interactions between non-polar side chains. In addition, several hydrogen bonds and salt bridges are also involved in stabilizing the ANG1/TIE2 and ANG2/TIE2 complexes. Structure-based mutagenesis of TIE2 abolished both ANG1 and ANG2 binding to TIE2 [103].
The angiopoietin fibrinogen-like domains are responsible for receptor recognition and binding, and it has been suggested that the coiled-coil motif mediates homo- or heterodimerization of angiopoietin monomers [104, 122, 123]. Mass spectroscopic analysis of fragments generated proteolytically from native ANG1 demonstrated that Cys265 in the coiled-coil domain is involved in covalent homodimerization by an intermolecular disulfide bridge [104]. ANG1 and ANG2 were observed as trimers and dimers, and especially ANG1 is further clustered to form higher-order oligomers, such as tetramers and hexamers, and even higher multimeric forms, in solution [104, 105, 123]. It is thought that the N-terminal region serves as a superclustering region assembling the angiopoietin coiled-coil dimers into higher-order oligomers. The angiopoietin fibrinogen-like domain has been found to bind TIE2 in a 1:1 stoichiometry [104, 121]. Because of the dimeric, trimeric, or multimeric structures of angiopoietins, the expected stoichiometry of the angiopoietin-receptor complex in vivo would be thus 2:2 or higher.
The angiopoietin fibrinogen-like regions contain also two other surface patches of particularly conserved residues, suggesting that these might be also involved in biologically important interactions [121]. However, mutations within these conserved surface regions in the fibrinogen-like A and B domains did not affect TIE2 binding [122].
16.6.2 Tie Receptor Specificity
All three angiopoietins bind to TIE2 [6, 117, 120]. Interestingly, ANG1 and ANG4 are TIE2 agonists, while ANG2 induces only weak TIE2 phosphorylation and can inhibit ANG1-induced TIE2 activation. The oligomeric structure of angiopoietins suggests that ANG1 and ANG4 activate TIE2 by bridging receptor molecules. However, simply bridging receptor molecules appears to be insufficient for TIE2 activation, because ANG2 activates TIE2 only poorly [106]. Also, ANG1 and ANG2 bind in a very similar manner to TIE2, indicating that altered ligand presentation is not sufficient to explain the differences in angiopoietin biological activities [108].
ANG1 oligomerization has been associated with enhanced TIE2 activity [49, 104, 105]. Monomeric and dimeric ANG1 proteins lacking the coiled-coil and superclustering domains or the superclustering domain alone were able to bind to but not activate TIE2 [104]. An ANG1 variant, ANG1-F1-Fc-F1, with four fibrinogen domains could phosphorylate TIE2 with a similar efficiency as native ANG1 [104]. To improve protein solubility, additional dimeric, trimeric, and pentameric ANG1 fusion proteins lacking the superclustering and coiled-coiled domains have been designed [49]. The pentameric ANG1 chimeric protein, COMP-Ang1, showed enhanced activity in comparison to native ANG1 [49]. The dimeric GCN4 fusion failed to activate the TIE2/Akt pathway, whereas the trimeric Matrilin fusion protein, Mat-ANG1, induced TIE2/Akt phosphorylation similarly as native ANG1. The Mat-ANG1 activity suggests that TIE2 could be activated already by trimeric ANG1 variants. The angiopoietin oligomerization state has been found to regulate subcellular trafficking of Tie2-ANG2 and TIE2-ANG1 complexes and ANG2-mediated cell-matrix interactions [106, 124]. Importantly, it is still not understood which oligomerization state of ANG1 is optimal for TIE2 activation, which ANG1 forms predominate in vivo, or whether the different forms have different signaling functions.
Despite extensive efforts to identify TIE1 ligands, TIE1 is still considered an orphan receptor. However, it has been shown that both native ANG1 and COMP-Ang1 stimulate TIE1 phosphorylation in primary endothelial cells expressing also TIE2 [119]. TIE1 phosphorylation occurs with same kinetics and doses of the stimulating angiopoietins as TIE2 phosphorylation, but is clearly weaker in intensity [119]. Also, TIE1 has been suggested to differentially modulate the binding of ANG1 and ANG2 to TIE2 [109, 125]. These data suggest the possibility that TIE1 is unable to bind a ligand in an independent manner, but acts as a co-receptor with TIE2.
16.7 TIE-1 and TIE-2 Activation and Signaling
ANG1 stimulates endothelial cell survival and migration, and promotes endothelial barrier function via TIE2 [112, 113, 126]. ANG1 activates the TIE receptors via a unique mechanism, which is not used by other growth factor receptors and which is dependent on the cellular microenvironment [106, 127]. In contacting cells, ANG1 stimulates TIE receptor complexes, which form in trans across the cell–cell junctions promoting cell–cell adhesion and cell survival (Fig. 16.1). In isolated cells, matrix-bound ANG1 promotes cell–matrix adhesion via the TIE receptor complexes, which accumulate at the rear of migrating cells [106, 127]. The vascular endothelial protein tyrosine phosphatase, VE-PTP, dephosphorylates TIE2 at cell–cell junctions, and VE-PTP inhibitors have shown promise in alleviating pathological retinal vascularization via vessel stabilization [128, 129]. The junctional TIE2 complexes contain also TIE1 and are induced not only by ANG1 but also by ANG2 [106]. ANG2 can inhibit ANG1-induced TIE2 activation, but its downstream signaling cascades are incompletely understood. Integrins, which regulate endothelial cell–cell and cell–matrix interactions, have been implicated in angiopoietin signaling, and likely regulate the context-dependent vascular functions of the angiopoietin growth factors during vascular destabilization and sprouting [60, 130–133].
16.7.1 Context-Dependent ANG-TIE Signaling
The binding of angiopoietins to TIE2 results in receptor activation via a unique mechanism, which is not used by other soluble growth factor ligands [106, 127]. When contacting endothelial cells are stimulated with angiopoietin ligands, TIE RTKs are rapidly translocated to cell-cell junctions. ANG1-TIE2 complexes reach in trans across the endothelial cell-cell junction and preferentially activate the PI3K–Akt pathway to promote cell survival, endothelial monolayer stability and barrier function [106, 127]. In mobile endothelial cells, matrix-bound ANG1 activates TIE2 in endothelial cell–matrix contacts to induce matrix adhesion and cell migration via activation of the extracellular-regulated kinases (ERK) [127] and the adaptor protein DokR [106].
The ANG1-activated Akt pathway, downstream of PI3K activation, enhances cell survival via phosphorylation and inhibition of the transcription factor forkhead box O1 (FOXO1) function [134]. FOXO1 induces the expression of genes associated with vascular destabilization and remodeling, such as ANG2, and inhibits the expression of, e.g., survivin, an apoptosis inhibitor [135]. ANG1 also induces the interaction of TIE2 with ABIN-2 (A20 binding inhibitor of NF-kappaB activation-2) which may promote cell survival and inflammatory signals [136].
In the stalk cells of sprouting vessels, ANG1 may engage TIE2 at cell-cell junctions to mediate vascular stabilization. ANG2 stimulation results also in TIE2 translocation to endothelial cell junctions, but while ANG1 induces TIE2 activation, ANG2 induces only weak TIE2 tyrosine phosphorylation, and may act as an antagonist to inhibit ANG1-induced TIE2 activation [106]. ANG2 is stored in the endothelial Weibel–Palade bodies from where it can be secreted in response to e.g. inflammatory stimuli [137]. Increased ANG2 levels promote endothelial destabilization, whereas in concert with VEGF, ANG2 induces angiogenesis [45]. However, ANG2 has been also suggested to function as an endothelial cell survival factor in stressed cells, where ANG1-stimulated Akt activation is low. In this setting, ANG2 would be induced, via the transcription factor FOXO1 to function as a TIE2 agonist, augmenting Akt activity to provide negative feedback to FOXO1-regulated transcription and apoptosis [138].
Multiple signaling mechanisms have been reported to mediate the barrier promoting functions of ANG1. ANG1 stabilizes the cortical actin cytoskeleton, via the IQ domain GTPase-activating protein 1 (IQGAP1) and Rac1 [139]. ANG1 also induces the expression of Kruppel-like factor 2, a transcription factor involved in vascular quiescence [140], upregulation of the tight junction protein zonula occludens protein-2 (ZO-2) [141], and activation of sphingosine kinase-1 (SK-1) [142]. ANG1 counteracts VEGF-induced permeability and VE-cadherin internalization by inhibiting VEGF-activated Src via mDia [143]. Another study shows that ANG1 inhibits VEGF-induced nitric oxide (NO) increase and permeability via activation of the atypical protein kinase C-ζ (PKC- ζ (zeta)), which phosphorylates the inhibitory Thr497 residue in endothelial nitric oxide synthetase (eNOS) [144], while in some studies ANG1 has been shown to induce phosphorylation of the activating Ser1177 in eNOS and NO production [145]. These results highlight the complexity of ANG1-mediated improvement of endothelial barrier function in response to various permeability increasing agents.
16.7.2 Negative Regulation of ANG-TIE Signaling
VE-PTP (also known as HPTPβ, PTPRB, RPTPβ) is an endothelial cell-specific protein tyrosine phosphatase, and a negative regulator of TIE2. VE-PTP is indispensable during mouse vascular development, and it has an important function in promoting endothelial barrier function in part by associating with VE-cadherin [146–149]. Furthermore, the localization of VE-PTP in cell–cell junctions is promoted by ANG1 [106]. Inhibition of VE-PTP using function-blocking antibodies resulted in enlarged vascular structures in the developing embryonic allantoic membrane [128], as well as in experimental tumors [150]. In addition, a small molecule inhibitor of VE-PTP increased Tie2 activity and suppressed neovascularization in a mouse model of neovascular age-related macular degeneration by stabilizing retinal and choroidal blood vessels [129]. As the TIE receptors undergo significantly less ubiquitinylation following ligand binding than the VEGFRs and are less efficiently internalized and degraded [29], transmembrane phosphatase-mediated dephosphorylation of TIE2 may be a significant mechanism of TIE2 regulation.
16.7.3 Mechanisms of ANG2/TIE1 Signaling
ANG2 signaling mechanisms are not well understood. Although ANG2 can inhibit the ANG1-induced TIE2 activation, it may, depending on the context, such as incubation time and ligand concentration, also act as an agonist. ANG2 has been suggested to support endothelial cell migration and cell survival under stressed conditions, in the absence of ANG1 and in the tumor vasculature [46, 138, 151], and to induce actin stress fiber formation and endothelial gap formation via myosin light chain (MLC) phosphorylation [55]. Furthermore, genetic mouse models have revealed that Ang2 functions as a Tie2 agonist in the lymphatic vasculature [10, 25]. In addition, ANG2 has been found to signal via integrins, independently of Tie2, promoting endothelial monolayer destabilization and cell migration (see 16.7.4).
The signaling mechanisms of TIE1 have remained poorly characterized. TIE1 can interact with TIE2 [109, 118, 119], and it is phosphorylated in an ANG1-dependent manner [119, 152]. TIE1 has been proposed to function as an inhibitor of TIE2 activation [109]; however, the results from a Tie1 genetic mouse model did not support this possibility [13]. Furthermore, it has been reported that a chimeric c-fms-TIE1 receptor with the TIE1 intracellular domain can activate the PI3K-Akt pathway [153].
TIE1 is regulated by proteolytic cleavages, and these cleavages are enhanced by phorbol 12-myristate 13-acetate (PMA) and VEGF [154]. The first cleavage occurs close to the plasma membrane and requires a metalloprotease, resulting in the release of the TIE1 ectodomain. The second, γ-secretase-dependent cleavage, releases the membrane-bound endodomain [155]. TIE2 has been also reported to undergo ectodomain cleavage, but with different kinetics than TIE1, affecting the relative levels of TIE1 and TIE2 and thereby possibly contributing to the ANG1 ligand responsiveness of endothelial cells [156, 157].
16.7.4 ANG-TIE System and Integrins
Multiple integrin heterodimers, which regulate cell–cell and cell–matrix interactions, are expressed in endothelial cells and are known to cross talk with the ANG-TIE signaling system. Angiopoietins have been reported to signal directly via the integrins or via TIE receptor-integrin complexes. Integrin α5β1 was found to co-immunoprecipitate with TIE2, sensitizing TIE2 to ANG1 signals, when cells adhered on fibronectin [130]. On the other hand, ANG2 was reported to induce interaction of TIE2 with the αvβ3 integrin, stimulating the proteosomal degradation of αvβ3, an event that may be linked to endothelial destabilization [131].
In addition, both ANG1 and ANG2 have been shown to directly interact with different integrin subunits, also in the absence of TIE2. In the tip cells of vascular sprouts, which express ANG2, but less TIE2, ANG2 is expected to stimulate sprouting via integrins [132]. Recently, clues to the binding of ANG2 to α5β1 have been elucidated. ANG2 is able to bind α5β1 integrin in the absence of TIE2, and the molecular mechanism seems to require both integrin α and β subunits. ANG2 was found to interact with the tailpiece of the α5 subunit via a region around Gln362 in the C-terminal ANG2 fibrinogen-like domain [133]. In another study, the ANG2 N-terminal domain, but not that of ANG1, was found to induce α5β1-integrin activation [60]. In high glucose environments, such as those observed in diabetic retinopathy, ANG2 stimulated pericyte apoptosis in a process that required the α3β1-integrin, but not TIE2 [64]. ANG1 regulates postnatal retinal angiogenesis; these signals appear to be mediated via astrocyte expressed αvβ5 integrin [12]. During vascular sprouting, the retinal astrocytes secrete fibronectin, a matrix molecule that guides endothelial tip cell migration. Intravitreal ANG1 injection resulted in increased fibronectin deposition, astrocyte distribution, and FAK activation in astrocytes in an αvβ5 integrin-dependent manner, guiding directional sprouting into the avascular region of the retina [12]. In endothelial monolayers silenced for Tie2, and in aortic endothelium of Ang2 transgenic mice, ANG2 activation of β1-integrin resulted in altered endothelial cell-matrix adhesion and the formation of actin stress fibers that promote endothelial retraction and junction destabilization. This alternative Ang2-β1-integrin signalling pathway is likely activated in diseases with increased vascular leak, where Ang2 levels are elevated and Tie2 levels reduced [60]. The integrin dependent functions of angiopoietins should be considered when blocking reagents targeting Ang2 are developed for the treatment of cancer and other human diseases characterized with pathological vascular leakage.
16.8 Conclusions
The ANG-TIE system is an important regulator of endothelial cell functions. It provides critical signals for embryonic and postnatal cardiovascular and lymphatic development. Due to the vascular stabilization and vessel remodeling signals induced by the ANG1-TIE2 pathway, ways to reinforce this signaling axis are being investigated, including recombinant ANG1 proteins and small molecule inhibitors of the TIE2 inactivating phosphatase, VE-PTP, for alleviating pathological vascularization and endothelial destabilization, as well as stimulating neovascularization of ischemic tissues. In contrast, approaches to neutralize increased ANG2 levels are being developed to counteract its increased activity during inflammation and injury, and in tumors. Furthermore, TIE1 may provide a target for inhibition of atherosclerosis and tumor angiogenesis. However, future work is required to better understand the signaling mechanisms of the TIE1 receptor. In addition, increased understanding of the interplay of the ANG–TIE system with integrins may open up novel ways to better exploit the ANG-TIE system as a therapeutic target.
References
Partanen J, Armstrong E, Makela TP, Korhonen J, Sandberg M, Renkonen R, et al. A novel endothelial cell surface receptor tyrosine kinase with extracellular epidermal growth factor homology domains. Mol Cell Biol. 1992;12(4):1698–707.
Dumont DJ, Yamaguchi TP, Conlon RA, Rossant J, Breitman ML. tek, a novel tyrosine kinase gene located on mouse chromosome 4, is expressed in endothelial cells and their presumptive precursors. Oncogene. 1992;7(8):1471–80.
Dumont DJ, Gradwohl GJ, Fong GH, Auerbach R, Breitman ML. The endothelial-specific receptor tyrosine kinase, tek, is a member of a new subfamily of receptors. Oncogene. 1993;8(5):1293–301.
Iwama A, Hamaguchi I, Hashiyama M, Murayama Y, Yasunaga K, Suda T. Molecular cloning and characterization of mouse TIE and TEK receptor tyrosine kinase genes and their expression in hematopoietic stem cells. Biochem Biophys Res Commun. 1993;195(1):301–9.
Suri C, Jones PF, Patan S, Bartunkova S, Maisonpierre PC, Davis S, et al. Requisite role of angiopoietin-1, a ligand for the TIE2 receptor, during embryonic angiogenesis. Cell. 1996;87(7):1171–80.
Maisonpierre PC, Suri C, Jones PF, Bartunkova S, Wiegand SJ, Radziejewski C, et al. Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science. 1997;277(5322):55–60.
Lee HJ, Cho CH, Hwang SJ, Choi HH, Kim KT, Ahn SY, et al. Biological characterization of angiopoietin-3 and angiopoietin-4. FASEB J. 2004;18(11):1200–8.
Augustin HG, Koh GY, Thurston G, Alitalo K. Control of vascular morphogenesis and homeostasis through the angiopoietin-Tie system. Nat Rev. 2009;10(3):165–77.
Saharinen P, Eklund L, Pulkki K, Bono P, Alitalo K. VEGF and angiopoietin signaling in tumor angiogenesis and metastasis. Trends Mol Med. 2011;17(7):347–62.
Gale NW, Thurston G, Hackett SF, Renard R, Wang Q, McClain J, et al. Angiopoietin-2 is required for postnatal angiogenesis and lymphatic patterning, and only the latter role is rescued by Angiopoietin-1. Dev Cell. 2002;3(3):411–23.
Jeansson M, Gawlik A, Anderson G, Li C, Kerjaschki D, Henkelman M, et al. Angiopoietin-1 is essential in mouse vasculature during development and in response to injury. J Clin Invest. 2011;121(6):2278–89.
Lee J, Kim KE, Choi DK, Jang JY, Jung JJ, Kiyonari H, et al. Angiopoietin-1 guides directional angiogenesis through integrin alphavbeta5 signaling for recovery of ischemic retinopathy. Sci Transl Med. 2013;5(203):203ra127.
D'Amico G, Korhonen EA, Anisimov A, Zarkada G, Holopainen T, Hagerling R, et al. Tie1 deletion inhibits tumor growth and improves angiopoietin antagonist therapy. J Clin Invest. 2014;124(2):824–34.
D’Amico G, Korhonen EA, Waltari M, Saharinen P, Laakkonen P, Alitalo K. Loss of endothelial Tie1 receptor impairs lymphatic vessel development-brief report. Arterioscler Thromb Vasc Biol. 2010;30(2):207–9.
Qu X, Tompkins K, Batts LE, Puri M, Baldwin S. Abnormal embryonic lymphatic vessel development in Tie1 hypomorphic mice. Development. 2010;137(8):1285–95.
Shen B, Shang Z, Wang B, Zhang L, Zhou F, Li T, et al. Genetic dissection of tie pathway in mouse lymphatic maturation and valve development. Arterioscler Thromb Vasc Biol. 2014;34(6):1221–30.
Qu X, Zhou B, Baldwin SH. Tie1 is required for lymphatic valve and collecting vessel development. Dev Biol. 2015; 399(1):117–28.
Dumont DJ, Gradwohl G, Fong GH, Puri MC, Gertsenstein M, Auerbach A, et al. Dominant-negative and targeted null mutations in the endothelial receptor tyrosine kinase, tek, reveal a critical role in vasculogenesis of the embryo. Genes Dev. 1994;8(16):1897–909.
Arita Y, Nakaoka Y, Matsunaga T, Kidoya H, Yamamizu K, Arima Y, et al. Myocardium-derived angiopoietin-1 is essential for coronary vein formation in the developing heart. Nat Commun. 2014;5:4552.
Puri MC, Rossant J, Alitalo K, Bernstein A, Partanen J. The receptor tyrosine kinase TIE is required for integrity and survival of vascular endothelial cells. EMBO J. 1995;14(23):5884–91.
Partanen J, Puri MC, Schwartz L, Fischer KD, Bernstein A, Rossant J. Cell autonomous functions of the receptor tyrosine kinase TIE in a late phase of angiogenic capillary growth and endothelial cell survival during murine development. Development. 1996;122(10):3013–21.
Puri MC, Partanen J, Rossant J, Bernstein A. Interaction of the TEK and TIE receptor tyrosine kinases during cardiovascular development. Development. 1999;126(20):4569–80.
Dellinger M, Hunter R, Bernas M, Gale N, Yancopoulos G, Erickson R, et al. Defective remodeling and maturation of the lymphatic vasculature in Angiopoietin-2 deficient mice. Dev Biol. 2008;319(2):309–20.
Zheng W, Nurmi H, Appak S, Sabine A, Bovay E, Korhonen EA, et al. Angiopoietin 2 regulates the transformation and integrity of lymphatic endothelial cell junctions. Genes Dev. 2014;28(14):1592–603.
Thomson BR, Heinen S, Jeansson M, Ghosh AK, Fatima A, Sung HK, et al. A lymphatic defect causes ocular hypertension and glaucoma in mice. J Clin Invest. 2014;124(10):4320–4.
Eklund L, Saharinen P. Angiopoietin signaling in the vasculature. Exp Cell Res. 2013;319(9):1271–80.
McCarter SD, Mei SH, Lai PF, Zhang QW, Parker CH, Suen RS, et al. Cell-based angiopoietin-1 gene therapy for acute lung injury. Am J Respir Crit Care Med. 2007;175(10):1014–26.
Thurston G, Suri C, Smith K, McClain J, Sato TN, Yancopoulos GD et al. Leakage-resistant blood vessels in mice transgenically overexpressing angiopoietin-1. Science. 1999; 286(5449):2511–4.
Anisimov A, Tvorogov D, Alitalo A, Leppanen VM, An Y, Han EC, et al. Vascular endothelial growth factor-angiopoietin chimera with improved properties for therapeutic angiogenesis. Circulation. 2013;127(4):424–34.
Koh GY. Orchestral actions of angiopoietin-1 in vascular regeneration. Trends Mol Med. 2013;19(1):31–9.
Limaye N, Wouters V, Uebelhoer M, Tuominen M, Wirkkala R, Mulliken JB, et al. Somatic mutations in angiopoietin receptor gene TEK cause solitary and multiple sporadic venous malformations. Nat Genet. 2009;41(1):118–24.
Rasmussen AL, Okumura A, Ferris MT, Green R, Feldmann F, Kelly SM, et al. Host genetic diversity enables Ebola hemorrhagic fever pathogenesis and resistance. Science. 2014;346:987–91.
Ziegler T, Horstkotte J, Schwab C, Pfetsch V, Weinmann K, Dietzel S, et al. Angiopoietin 2 mediates microvascular and hemodynamic alterations in sepsis. J Clin Invest. 2013;123:3436–45.
Syrjala SO, Tuuminen R, Nykanen AI, Raissadati A, Dashkevich A, Keranen MA, et al. Angiopoietin-2 inhibition prevents transplant ischemia-reperfusion injury and chronic rejection in rat cardiac allografts. Am J Transplant. 2014;14(5):1096–108.
Theelen TL, Lappalainen JP, Sluimer JC, Gurzeler E, Cleutjens JP, Gijbels MJ, et al. Angiopoietin-2 blocking antibodies reduce early atherosclerotic plaque development in mice. Atherosclerosis. 2015;241(2):297–304.
Falcon BL, Hashizume H, Koumoutsakos P, Chou J, Bready JV, Coxon A, et al. Contrasting actions of selective inhibitors of angiopoietin-1 and angiopoietin-2 on the normalization of tumor blood vessels. Am J Pathol. 2009;175(5):2159–70.
Mazzieri R, Pucci F, Moi D, Zonari E, Ranghetti A, Berti A, et al. Targeting the ANG2/TIE2 Axis inhibits tumor growth and metastasis by impairing angiogenesis and disabling rebounds of proangiogenic myeloid cells. Cancer Cell. 2011;19(4):512–26.
Woo KV, Qu X, Babaev VR, Linton MF, Guzman RJ, Fazio S, et al. Tie1 attenuation reduces murine atherosclerosis in a dose-dependent and shear stress-specific manner. J Clin Invest. 2011;121:1624–35.
Holopainen T, Saharinen P, D’Amico G, Lampinen A, Eklund L, Sormunen R, et al. Effects of angiopoietin-2-blocking antibody on endothelial cell–cell junctions and lung metastasis. J Natl Cancer Inst. 2012;104(6):461–75.
Vikkula M, Boon LM, Carraway 3rd KL, Calvert JT, Diamonti AJ, Goumnerov B, et al. Vascular dysmorphogenesis caused by an activating mutation in the receptor tyrosine kinase TIE2. Cell. 1996;87(7):1181–90.
Soblet J, Limaye N, Uebelhoer M, Boon LM, Vikkula M. Variable Somatic TIE2 Mutations in Half of Sporadic Venous Malformations. Mol Syndromol. 2013;4(4):179–83.
Uebelhoer M, Natynki M, Kangas J, Mendola A, Nguyen HL, Soblet J, et al. Venous malformation-causative TIE2 mutations mediate an AKT-dependent decrease in PDGFB. Hum Mol Genet. 2013;22(17):3438–48.
Monk BJ, Poveda A, Vergote I, Raspagliesi F, Fujiwara K, Bae DS, et al. Anti-angiopoietin therapy with trebananib for recurrent ovarian cancer (TRINOVA-1): a randomised, multicentre, double-blind, placebo-controlled phase 3 trial. Lancet Oncol. 2014;15:799–808.
Goede V, Coutelle O, Neuneier J, Reinacher-Schick A, Schnell R, Koslowsky TC, et al. Identification of serum angiopoietin-2 as a biomarker for clinical outcome of colorectal cancer patients treated with bevacizumab-containing therapy. Br J Cancer. 2010;103(9):1407–14.
Holash J, Maisonpierre PC, Compton D, Boland P, Alexander CR, Zagzag D, et al. Vessel cooption, regression, and growth in tumors mediated by angiopoietins and VEGF. Science. 1999;284(5422):1994–8.
Daly C, Eichten A, Castanaro C, Pasnikowski E, Adler A, Lalani AS, et al. Angiopoietin-2 functions as a Tie2 agonist in tumor models, where it limits the effects of VEGF inhibition. Cancer Res. 2013;73(1):108–18.
Nasarre P, Thomas M, Kruse K, Helfrich I, Wolter V, Deppermann C, et al. Host-derived angiopoietin-2 affects early stages of tumor development and vessel maturation but is dispensable for later stages of tumor growth. Cancer Res. 2009;69(4):1324–33.
Reiss Y, Knedla A, Tal AO, Schmidt MH, Jugold M, Kiessling F, et al. Switching of vascular phenotypes within a murine breast cancer model induced by angiopoietin-2. J Pathol. 2009;217(4):571–80.
Cho CH, Kammerer RA, Lee HJ, Steinmetz MO, Ryu YS, Lee SH, et al. COMP-Ang1: a designed angiopoietin-1 variant with nonleaky angiogenic activity. Proc Natl Acad Sci USA. 2004;101(15):5547–52.
Hwang JA, Lee EH, Kim HW, Park JB, Jeon BH, Cho CH. COMP-Ang1 potentiates the antitumor activity of 5-fluorouracil by improving tissue perfusion in murine Lewis lung carcinoma. Mol Cancer Res. 2009;7(12):1920–7.
Ebos JM, Lee CR, Cruz-Munoz W, Bjarnason GA, Christensen JG, Kerbel RS. Accelerated metastasis after short-term treatment with a potent inhibitor of tumor angiogenesis. Cancer Cell. 2009;15(3):232–9.
Paez-Ribes M, Allen E, Hudock J, Takeda T, Okuyama H, Vinals F, et al. Antiangiogenic therapy elicits malignant progression of tumors to increased local invasion and distant metastasis. Cancer Cell. 2009;15(3):220–31.
Rigamonti N, Kadioglu E, Keklikoglou I, Wyser Rmili C, Leow CC, De Palma M. Role of angiopoietin-2 in adaptive tumor resistance to VEGF signaling blockade. Cell Rep. 2014;8(3):696–706.
Kaipainen A, Vlaykova T, Hatva E, Bohling T, Jekunen A, Pyrhonen S, et al. Enhanced expression of the tie receptor tyrosine kinase messenger RNA in the vascular endothelium of metastatic melanomas. Cancer Res. 1994;54(24):6571–7.
Parikh SM, Mammoto T, Schultz A, Yuan HT, Christiani D, Karumanchi SA, et al. Excess circulating angiopoietin-2 may contribute to pulmonary vascular leak in sepsis in humans. PLoS Med. 2006;3(3):e46.
Parikh SM. Dysregulation of the angiopoietin-Tie-2 axis in sepsis and ARDS. Virulence. 2013;4(6):517–24.
David S, Mukherjee A, Ghosh CC, Yano M, Khankin EV, Wenger JB, et al. Angiopoietin-2 may contribute to multiple organ dysfunction and death in sepsis*. Crit Care Med. 2012;40(11):3034–41.
Stiehl T, Thamm K, Kaufmann J, Schaeper U, Kirsch T, Haller H, et al. Lung-targeted RNA interference against angiopoietin-2 ameliorates multiple organ dysfunction and death in sepsis. Crit Care Med. 2014;42(10):e654–62.
Benest AV, Kruse K, Savant S, Thomas M, Laib AM, Loos EK, et al. Angiopoietin-2 is critical for cytokine-induced vascular leakage. PLoS One. 2013;8(8):e70459.
Hakanpaa L, Sipila T, Leppanen VM, Gautam P, Nurmi H, Jacquemet G et al. Endothelial destabilization by angiopoietin-2 via integrin β1 activation. Nat Commun. 2015; 6:5962.
Fiedler U, Reiss Y, Scharpfenecker M, Grunow V, Koidl S, Thurston G, et al. Angiopoietin-2 sensitizes endothelial cells to TNF-alpha and has a crucial role in the induction of inflammation. Nat Med. 2006;12(2):235–9.
Tabruyn SP, Colton K, Morisada T, Fuxe J, Wiegand SJ, Thurston G, et al. Angiopoietin-2-driven vascular remodeling in airway inflammation. Am J Pathol. 2010;177(6):3233–43.
Hammes HP, Lin J, Wagner P, Feng Y, Vom Hagen F, Krzizok T, et al. Angiopoietin-2 causes pericyte dropout in the normal retina: evidence for involvement in diabetic retinopathy. Diabetes. 2004;53(4):1104–10.
Park SW, Yun JH, Kim JH, Kim KW, Cho CH, Kim JH. Angiopoietin 2 induces pericyte apoptosis via alpha3beta1 integrin signaling in diabetic retinopathy. Diabetes. 2014;10.
Salmon AH, Neal CR, Sage LM, Glass CA, Harper SJ, Bates DO. Angiopoietin-1 alters microvascular permeability coefficients in vivo via modification of endothelial glycocalyx. Cardiovasc Res. 2009;83(1):24–33.
Kajiya K, Kidoya H, Sawane M, Matsumoto-Okazaki Y, Yamanishi H, Furuse M, et al. Promotion of lymphatic integrity by angiopoietin-1/Tie2 signaling during inflammation. Am J Pathol. 2012;180(3):1273–82.
Kosacka J, Nowicki M, Kloting N, Kern M, Stumvoll M, Bechmann I, et al. COMP-angiopoietin-1 recovers molecular biomarkers of neuropathy and improves vascularisation in sciatic nerve of ob/ob mice. PLoS One. 2012;7(3):e32881.
Cho CH, Sung HK, Kim KT, Cheon HG, Oh GT, Hong HJ, et al. COMP-angiopoietin-1 promotes wound healing through enhanced angiogenesis, lymphangiogenesis, and blood flow in a diabetic mouse model. Proc Natl Acad Sci USA. 2006;103(13):4946–51.
Lee JS, Song SH, Kim JM, Shin IS, Kim KL, Suh YL, et al. Angiopoietin-1 prevents hypertension and target organ damage through its interaction with endothelial Tie2 receptor. Cardiovasc Res. 2008;78(3):572–80.
Jung YJ, Kim DH, Lee AS, Lee S, Kang KP, Lee SY, et al. Peritubular capillary preservation with COMP-angiopoietin-1 decreases ischemia-reperfusion-induced acute kidney injury. Am J Physiol Renal Physiol. 2009;297(4):F952–60.
Tuuminen R, Nykänen AI, Saharinen P, Gautam P, Keränen MA, Arnaudova R, et al. Donor simvastatin treatment prevents ischemia-reperfusion and acute kidney injury by preserving microvascular barrier function. Am J Transplant. 2013;13(8):2019–34.
Reiss Y, Droste J, Heil M, Tribulova S, Schmidt MH, Schaper W, et al. Angiopoietin-2 impairs revascularization after limb ischemia. Circ Res. 2007;101(1):88–96.
Korhonen J, Lahtinen I, Halmekyto M, Alhonen L, Janne J, Dumont D, et al. Endothelial-specific gene expression directed by the tie gene promoter in vivo. Blood. 1995;86(5):1828–35.
Zhou BO, Ding L, Morrison SJ. Hematopoietic stem and progenitor cells regulate the regeneration of their niche by secreting Angiopoietin-1. Elife. 2015 Mar 30;4. doi: 10.7554/eLife.05521.
De Palma M, Venneri MA, Galli R, Sergi Sergi L, Politi LS, Sampaolesi M, et al. Tie2 identifies a hematopoietic lineage of proangiogenic monocytes required for tumor vessel formation and a mesenchymal population of pericyte progenitors. Cancer Cell. 2005;8(3):211–26.
Batard P, Sansilvestri P, Scheinecker C, Knapp W, Debili N, Vainchenker W, et al. The Tie receptor tyrosine kinase is expressed by human hematopoietic progenitor cells and by a subset of megakaryocytic cells. Blood. 1996;87(6):2212–20.
Yano M, Iwama A, Nishio H, Suda J, Takada G, Suda T. Expression and function of murine receptor tyrosine kinases, TIE and TEK, in hematopoietic stem cells. Blood. 1997;89(12):4317–26.
Korhonen J, Partanen J, Armstrong E, Vaahtokari A, Elenius K, Jalkanen M, et al. Enhanced expression of the tie receptor tyrosine kinase in endothelial cells during neovascularization. Blood. 1992;80(10):2548–55.
Porat RM, Grunewald M, Globerman A, Itin A, Barshtein G, Alhonen L, et al. Specific induction of tie1 promoter by disturbed flow in atherosclerosis-prone vascular niches and flow-obstructing pathologies. Circ Res. 2004;94(3):394–401.
Brown LF, Dezube BJ, Tognazzi K, Dvorak HF, Yancopoulos GD. Expression of Tie1, Tie2, and angiopoietins 1, 2, and 4 in Kaposi’s sarcoma and cutaneous angiosarcoma. Am J Pathol. 2000;156(6):2179–83.
Iljin K, Dube A, Kontusaari S, Korhonen J, Lahtinen I, Oettgen P, et al. Role of ets factors in the activity and endothelial cell specificity of the mouse Tie gene promoter. FASEB J. 1999;13(2):377–86.
Iljin K, Petrova TV, Veikkola T, Kumar V, Poutanen M, Alitalo K. A fluorescent Tie1 reporter allows monitoring of vascular development and endothelial cell isolation from transgenic mouse embryos. FASEB J. 2002;16(13):1764–74.
White SJ, Papadakis ED, Rogers CA, Johnson JL, Biessen EA, Newby AC. In vitro and in vivo analysis of expression cassettes designed for vascular gene transfer. Gene Ther. 2008;15(5):340–6.
Kivivuori SM, Siitonen S, Porkka K, Vettenranta K, Alitalo R, Saarinen-Pihkala U. Expression of vascular endothelial growth factor receptor 3 and Tie1 tyrosine kinase receptor on acute leukemia cells. Pediatr Blood Cancer. 2007;48(4):387–92.
Schlaeger TM, Qin Y, Fujiwara Y, Magram J, Sato TN. Vascular endothelial cell lineage-specific promoter in transgenic mice. Development. 1995;121(4):1089–98.
Minami T, Kuivenhoven JA, Evans V, Kodama T, Rosenberg RD, Aird WC. Ets motifs are necessary for endothelial cell-specific expression of a 723-bp Tie-2 promoter/enhancer in Hprt targeted transgenic mice. Arterioscler Thromb Vasc Biol. 2003;23(11):2041–7.
Abou-Khalil R, Le Grand F, Pallafacchina G, Valable S, Authier FJ, Rudnicki MA, et al. Autocrine and paracrine angiopoietin 1/Tie-2 signaling promotes muscle satellite cell self-renewal. Cell Stem Cell. 2009;5(3):298–309.
Jin P, Zhang J, Sumariwalla PF, Ni I, Jorgensen B, Crawford D, et al. Novel splice variants derived from the receptor tyrosine kinase superfamily are potential therapeutics for rheumatoid arthritis. Arthritis Res Ther. 2008;10(4):R73.
Greenman C, Stephens P, Smith R, Dalgliesh GL, Hunter C, Bignell G, et al. Patterns of somatic mutation in human cancer genomes. Nature. 2007;446(7132):153–8.
Antonescu CR, Yoshida A, Guo T, Chang NE, Zhang L, Agaram NP, et al. KDR activating mutations in human angiosarcomas are sensitive to specific kinase inhibitors. Cancer Res. 2009;69(18):7175–9.
Sato TN, Qin Y, Kozak CA, Audus KL. Tie-1 and tie-2 define another class of putative receptor tyrosine kinase genes expressed in early embryonic vascular system. Proc Natl Acad Sci USA. 1993;90(20):9355–8.
Gerhard DS, Wagner L, Feingold EA, Shenmen CM, Grouse LH, Schuler G, et al. The status, quality, and expansion of the NIH full-length cDNA project: the mammalian gene collection (MGC). Genome Res. 2004;14(10B):2121–7.
Wang H, Zhang Y, Toratani S, Okamoto T. Transformation of vascular endothelial cells by a point mutation in the Tie2 gene from human intramuscular haemangioma. Oncogene. 2004;23(53):8700–4.
Wouters V, Limaye N, Uebelhoer M, Irrthum A, Boon LM, Mulliken JB, et al. Hereditary cutaneomucosal venous malformations are caused by TIE2 mutations with widely variable hyper-phosphorylating effects. Eur J Hum Genet. 2009;18(18):141–20.
Willam C, Koehne P, Jurgensen JS, Grafe M, Wagner KD, Bachmann S, et al. Tie2 receptor expression is stimulated by hypoxia and proinflammatory cytokines in human endothelial cells. Circ Res. 2000;87(5):370–7.
Murdoch C, Tazzyman S, Webster S, Lewis CE. Expression of Tie-2 by human monocytes and their responses to angiopoietin-2. J Immunol. 2007;178(11):7405–11.
Schlaeger TM, Bartunkova S, Lawitts JA, Teichmann G, Risau W, Deutsch U, et al. Uniform vascular-endothelial-cell-specific gene expression in both embryonic and adult transgenic mice. Proc Natl Acad Sci USA. 1997;94(7):3058–63.
Chen-Konak L, Guetta-Shubin Y, Yahav H, Shay-Salit A, Zilberman M, Binah O, et al. Transcriptional and post-translation regulation of the Tie1 receptor by fluid shear stress changes in vascular endothelial cells. FASEB J. 2003;17(14):2121–3.
Manning G, Plowman GD, Hunter T, Sudarsanam S. Evolution of protein kinase signaling from yeast to man. Trends Biochem Sci. 2002;27(10):514–20.
King N, Carroll SB. A receptor tyrosine kinase from choanoflagellates: molecular insights into early animal evolution. Proc Natl Acad Sci USA. 2001;98(26):15032–7.
Manning G, Young SL, Miller WT, Zhai Y. The protist, Monosiga brevicollis, has a tyrosine kinase signaling network more elaborate and diverse than found in any known metazoan. Proc Natl Acad Sci USA. 2008;105(28):9674–9.
Gjini E, Hekking LH, Kuchler A, Saharinen P, Wienholds E, Post JA, et al. Zebrafish Tie-2 shares a redundant role with Tie-1 in heart development and regulates vessel integrity. Dis Model Mech. 2011;4(1):57–66.
Barton WA, Tzvetkova-Robev D, Miranda EP, Kolev MV, Rajashankar KR, Himanen JP, et al. Crystal structures of the Tie2 receptor ectodomain and the angiopoietin-2-Tie2 complex. Nat Struct Mol Biol. 2006;13(6):524–32.
Davis S, Papadopoulos N, Aldrich TH, Maisonpierre PC, Huang T, Kovac L, et al. Angiopoietins have distinct modular domains essential for receptor binding, dimerization and superclustering. Nat Struct Biol. 2003;10(1):38–44.
Kim KT, Choi HH, Steinmetz MO, Maco B, Kammerer RA, Ahn SY, et al. Oligomerization and multimerization is critical for angiopoietin-1 to bind and phosphorylate tie2. J Biol Chem. 2005;280:20126–131.
Saharinen P, Eklund L, Miettinen J, Wirkkala R, Anisimov A, Winderlich M, et al. Angiopoietins assemble distinct Tie2 signalling complexes in endothelial cell-cell and cell-matrix contacts. Nat Cell Biol. 2008;10(5):527–37.
Peters KG, Kontos CD, Lin PC, Wong AL, Rao P, Huang L et al. Functional significance of Tie2 signaling in the adult vasculature. Recent Prog Horm Res. 2004;59:51–71.
Yu X, Seegar TC, Dalton AC, Tzvetkova-Robev D, Goldgur Y, Rajashankar KR, et al. Structural basis for angiopoietin-1-mediated signaling initiation. Proc Natl Acad Sci USA. 2013;110(18):7205–10.
Seegar TC, Eller B, Tzvetkova-Robev D, Kolev MV, Henderson SC, Nikolov DB, et al. Tie1–Tie2 interactions mediate functional differences between angiopoietin ligands. Mol Cell. 2010;37(5):643–55.
Shewchuk LM, Hassell AM, Ellis B, Holmes WD, Davis R, Horne EL, et al. Structure of the Tie2 RTK domain: self-inhibition by the nucleotide binding loop, activation loop, and C-terminal tail. Structure. 2000;8(11):1105–13.
Khan AA, Sandhya VK, Singh P, Parthasarathy D, Kumar A, Advani J, et al. Signaling network map of endothelial TEK tyrosine kinase. J Signal Transduct. 2014;2014:173026.
Jones N, Master Z, Jones J, Bouchard D, Gunji Y, Sasaki H, et al. Identification of Tek/Tie2 binding partners. Binding to a multifunctional docking site mediates cell survival and migration. J Biol Chem. 1999;274(43):30896–905.
Kontos CD, Stauffer TP, Yang WP, York JD, Huang L, Blanar MA, et al. Tyrosine 1101 of Tie2 is the major site of association of p85 and is required for activation of phosphatidylinositol 3-kinase and Akt. Mol Cell Biol. 1998;18(7):4131–40.
Tachibana K, Jones N, Dumont DJ, Puri MC, Bernstein A. Selective role of a distinct tyrosine residue on Tie2 in heart development and early hematopoiesis. Mol Cell Biol. 2005;25(11):4693–702.
Huang L, Turck CW, Rao P, Peters KG. GRB2 and SH-PTP2: potentially important endothelial signaling molecules downstream of the TEK/TIE2 receptor tyrosine kinase. Oncogene. 1995;11(10):2097–103.
Jones N, Chen SH, Sturk C, Master Z, Tran J, Kerbel RS, et al. A unique autophosphorylation site on Tie2/Tek mediates Dok-R phosphotyrosine binding domain binding and function. Mol Cell Biol. 2003;23(8):2658–68.
Davis S, Aldrich TH, Jones PF, Acheson A, Compton DL, Jain V, et al. Isolation of angiopoietin-1, a ligand for the TIE2 receptor, by secretion-trap expression cloning. Cell. 1996;87(7):1161–9.
Marron MB, Hughes DP, Edge MD, Forder CL, Brindle NP. Evidence for heterotypic interaction between the receptor tyrosine kinases TIE-1 and TIE-2. J Biol Chem. 2000;275(50):39741–6.
Saharinen P, Kerkela K, Ekman N, Marron M, Brindle N, Lee GM, et al. Multiple angiopoietin recombinant proteins activate the Tie1 receptor tyrosine kinase and promote its interaction with Tie2. J Cell Biol. 2005;169(2):239–43.
Valenzuela DM, Griffiths JA, Rojas J, Aldrich TH, Jones PF, Zhou H, et al. Angiopoietins 3 and 4: diverging gene counterparts in mice and humans. Proc Natl Acad Sci USA. 1999;96(5):1904–9.
Barton WA, Tzvetkova D, Nikolov DB. Structure of the angiopoietin-2 receptor binding domain and identification of surfaces involved in Tie2 recognition. Structure. 2005;13(5):825–32.
Procopio WN, Pelavin PI, Lee WM, Yeilding NM. Angiopoietin-1 and −2 coiled coil domains mediate distinct homo-oligomerization patterns, but fibrinogen-like domains mediate ligand activity. J Biol Chem. 1999;274(42):30196–201.
Fiedler U, Krissl T, Koidl S, Weiss C, Koblizek T, Deutsch U, et al. Angiopoietin-1 and angiopoietin-2 share the same binding domains in the Tie-2 receptor involving the first Ig-like loop and the epidermal growth factor-like repeats. J Biol Chem. 2003;278(3):1721–7.
Pietilä R, Nätynki M, Tammela T, Kangas J, Pulkki KH, Limaye N, et al. Ligand oligomerization state controls Tie2 receptor trafficking and angiopoietin-2-specific responses. J Cell Sci. 2012;125:2212–23.
Hansen TM, Singh H, Tahir TA, Brindle NP. Effects of angiopoietins-1 and −2 on the receptor tyrosine kinase Tie2 are differentially regulated at the endothelial cell surface. Cell Signal. 2010;22(3):527–32.
Gamble JR, Drew J, Trezise L, Underwood A, Parsons M, Kasminkas L et al. Angiopoietin-1 is an antipermeability and anti-inflammatory agent in vitro and targets cell junctions. Circ Res. 2000;87(7):603–7.
Fukuhara S, Sako K, Minami T, Noda K, Kim HZ, Kodama T, et al. Differential function of Tie2 at cell-cell contacts and cell-substratum contacts regulated by angiopoietin-1. Nat Cell Biol. 2008;10(5):513–26.
Winderlich M, Keller L, Cagna G, Broermann A, Kamenyeva O, Kiefer F, et al. VE-PTP controls blood vessel development by balancing Tie-2 activity. J Cell Biol. 2009;185(4):657–71.
Shen J, Frye M, Lee BL, Reinardy JL, McClung JM, Ding K, et al. Targeting VE-PTP activates TIE2 and stabilizes the ocular vasculature. J Clin Invest. 2014;124(10):4564–76.
Cascone I, Napione L, Maniero F, Serini G, Bussolino F. Stable interaction between {alpha}5{beta}1 integrin and tie2 tyrosine kinase receptor regulates endothelial cell response to ang-1. J Cell Biol. 2005;170:993–1004.
Thomas M, Felcht M, Kruse K, Kretschmer S, Deppermann C, Biesdorf A, et al. Angiopoietin-2 stimulation of endothelial cells induces alphavbeta3 integrin internalization and degradation. J Biol Chem. 2010;285(31):23842–9.
Felcht M, Luck R, Schering A, Seidel P, Srivastava K, Hu J, et al. Angiopoietin-2 differentially regulates angiogenesis through TIE2 and integrin signaling. J Clin Invest. 2012;122(6):1991–2005.
Lee HS, Oh SJ, Lee KH, Lee YS, Ko E, Kim KE, et al. Gln362 of Angiopoietin-2 Mediates Migration of Tumor and Endothelial Cells through Association with alpha5beta1 Integrin. J Biol Chem. 2014;289:31330–40.
Daly C, Wong V, Burova E, Wei Y, Zabski S, Griffiths J, et al. Angiopoietin-1 modulates endothelial cell function and gene expression via the transcription factor FKHR (FOXO1). Genes Dev. 2004;18(9):1060–71.
Papapetropoulos A, Fulton D, Mahboubi K, Kalb RG, O'Connor DS, Li F, et al. Angiopoietin-1 inhibits endothelial cell apoptosis via the Akt/survivin pathway. J Biol Chem. 2000;275(13):9102–5.
Hughes DP, Marron MB, Brindle NP. The antiinflammatory endothelial tyrosine kinase Tie2 interacts with a novel nuclear factor-kappaB inhibitor ABIN-2. Circ Res. 2003;92(6):630–6.
Fiedler U, Scharpfenecker M, Koidl S, Hegen A, Grunow V, Schmidt JM, et al. The Tie-2 ligand angiopoietin-2 is stored in and rapidly released upon stimulation from endothelial cell Weibel-Palade bodies. Blood. 2004;103(11):4150–6.
Daly C, Pasnikowski E, Burova E, Wong V, Aldrich TH, Griffiths J, et al. Angiopoietin-2 functions as an autocrine protective factor in stressed endothelial cells. Proc Natl Acad Sci USA. 2006;103(42):15491–6.
David S, Ghosh CC, Mukherjee A, Parikh SM. Angiopoietin-1 requires IQ domain GTPase-activating protein 1 to activate Rac1 and promote endothelial barrier defense. Arterioscler Thromb Vasc Biol. 2011;31(11):2643–52.
Sako K, Fukuhara S, Minami T, Hamakubo T, Song H, Kodama T, et al. Angiopoietin-1 induces Kruppel-like factor 2 expression through a phosphoinositide 3-kinase/AKT-dependent activation of myocyte enhancer factor 2. J Biol Chem. 2009;284(9):5592–601.
Lee SW, Kim WJ, Jun HO, Choi YK, Kim KW. Angiopoietin-1 reduces vascular endothelial growth factor-induced brain endothelial permeability via upregulation of ZO-2. Int J Mol Med. 2009;23(2):279–84.
Li X, Stankovic M, Bonder CS, Hahn CN, Parsons M, Pitson SM, et al. Basal and angiopoietin-1-mediated endothelial permeability is regulated by sphingosine kinase-1. Blood. 2008;111(7):3489–97.
Gavard J, Patel V, Gutkind JS. Angiopoietin-1 prevents VEGF-induced endothelial permeability by sequestering Src through mDia. Dev Cell. 2008;14(1):25–36.
Oubaha M, Gratton JP. Phosphorylation of endothelial nitric oxide synthase by atypical PKC zeta contributes to angiopoietin-1-dependent inhibition of VEGF-induced endothelial permeability in vitro. Blood. 2009;114(15):3343–51.
Babaei S, Teichert-Kuliszewska K, Zhang Q, Jones N, Dumont DJ, Stewart DJ. Angiogenic actions of angiopoietin-1 require endothelium-derived nitric oxide. Am J Pathol. 2003;162(6):1927–36.
Nawroth R, Poell G, Ranft A, Kloep S, Samulowitz U, Fachinger G, et al. VE-PTP and VE-cadherin ectodomains interact to facilitate regulation of phosphorylation and cell contacts. EMBO J. 2002;21(18):4885–95.
Nottebaum AF, Cagna G, Winderlich M, Gamp AC, Linnepe R, Polaschegg C, et al. VE-PTP maintains the endothelial barrier via plakoglobin and becomes dissociated from VE-cadherin by leukocytes and by VEGF. J Exp Med. 2008;205(12):2929–45.
Broermann A, Winderlich M, Block H, Frye M, Rossaint J, Zarbock A, et al. Dissociation of VE-PTP from VE-cadherin is required for leukocyte extravasation and for VEGF-induced vascular permeability in vivo. J Exp Med. 2011;208(12):2393–401.
Carra S, Foglia E, Cermenati S, Bresciani E, Giampietro C, Lora Lamia C, et al. Ve-ptp modulates vascular integrity by promoting adherens junction maturation. PLoS One. 2012;7(12):e51245.
Li Z, Huang H, Boland P, Dominguez MG, Burfeind P, Lai KM, et al. Embryonic stem cell tumor model reveals role of vascular endothelial receptor tyrosine phosphatase in regulating Tie2 pathway in tumor angiogenesis. Proc Natl Acad Sci USA. 2009;106:22399–404.
Yuan HT, Khankin EV, Karumanchi SA, Parikh SM. Angiopoietin 2 is a partial agonist/antagonist of Tie2 signaling in the endothelium. Mol Cell Biol. 2009;29(8):2011–22.
Yuan HT, Venkatesha S, Chan B, Deutsch U, Mammoto T, Sukhatme VP, et al. Activation of the orphan endothelial receptor Tie1 modifies Tie2-mediated intracellular signaling and cell survival. FASEB J. 2007;21:3171–83.
Kontos CD, Cha EH, York JD, Peters KG. The endothelial receptor tyrosine kinase Tie1 activates phosphatidylinositol 3-kinase and Akt to inhibit apoptosis. Mol Cell Biol. 2002;22(6):1704–13.
McCarthy MJ, Burrows R, Bell SC, Christie G, Bell PR, Brindle NP. Potential roles of metalloprotease mediated ectodomain cleavage in signaling by the endothelial receptor tyrosine kinase Tie-1. Lab Invest. 1999;79(7):889–95.
Marron MB, Singh H, Tahir TA, Kavumkal J, Kim HZ, Koh GY, et al. Regulated proteolytic processing of Tie1 modulates ligand responsiveness of the receptor-tyrosine kinase Tie2. J Biol Chem. 2007;282(42):30509–17.
Findley CM, Cudmore MJ, Ahmed A, Kontos CD. VEGF induces Tie2 shedding via a phosphoinositide 3-kinase/Akt dependent pathway to modulate Tie2 signaling. Arterioscler Thromb Vasc Biol. 2007;27(12):2619–26.
Singh H, Hansen TM, Patel N, Brindle NP. The molecular balance between receptor tyrosine kinases Tie1 and Tie2 is dynamically controlled by VEGF and TNFalpha and regulates angiopoietin signalling. PLoS One. 2012;7(1):e29319.
Acknowledgements
This work has received funding from the European Research Council (ERC-2010-AdG-26884), the People Programme (Marie Curie Actions) of the European Union’s Seventh Framework Programme FP7/2007–2013/ under REA grant agreement n° 317250, the Leducq Foundation (grant n:o 11CVD03), the Sigrid Juselius Foundation, the Finnish Cancer Organizations, the Worldwide Cancer Research (12-0181) and the Academy of Finland Centre of Excellence Program 2014–2019 (n:o 271845).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Saharinen, P., Jeltsch, M., Santoyo, M.M., Leppänen, VM., Alitalo, K. (2015). The TIE Receptor Family. In: Wheeler, D., Yarden, Y. (eds) Receptor Tyrosine Kinases: Family and Subfamilies. Springer, Cham. https://doi.org/10.1007/978-3-319-11888-8_16
Download citation
DOI: https://doi.org/10.1007/978-3-319-11888-8_16
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-11887-1
Online ISBN: 978-3-319-11888-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)