
Abstract
Reperfusion injury is mediated, in part, by the accumulation of platelets and leucocytes in the microvasculature after reflow. These components of the blood pool form aggregates that can obstruct flow in small vessels. In addition, mediators released from leucocytes and platelets further damage the reperfused myocardium. A strategy to limit reperfusion injury exploits the important role of membrane-bound adhesion molecules that attach platelets and leucocytes to themselves and to the vascular endothelium. Monoclonal antibodies against specific adhesion receptors effectively eliminate the function of the receptor. The most widely investigated receptors are P-selectin, present on platelets and the endothelium, CD11/CD18, present on leucocytes, and the fibrinogen receptor on platelets. Numerous animal studies have strongly supported the use of these monoclonal antibodies to block adhesion receptors as adjunctive reperfusion therapy. However, recent human trials have yielded disappointing results.
Similar content being viewed by others

Reperfusion injury is a critical cause of morbidity and mortality after myocardial infarction (MI). Numerous animal studies to date have demonstrated reduced infarct size following treatment with various inhibitors of reperfusion injury. Reperfusion injury is common to many different clinical states, including MI, cardiopulmonary bypass, stroke, shock liver, and intestinal ischaemia. Biodrugs such as monoclonal antibodies that bind to and block adhesive cell surface receptors on platelets and neutrophils are being investigated extensively at present. This article includes a brief review of the theory behind reperfusion injury and the experimental data gathered thus far addressing the use of monoclonal antibodies to prevent this type of injury.
Reperfusion is defined as resumption of blood flow after a transient period of cessation of flow. Percutaneous transluminal coronary angioplasty (PTCA) and thrombolysis are currently considered the standard reperfusion strategies for patients with acute MI associated with ST segment elevation or a new left bundle branch block. Yet despite the evidence that restoration of normal blood flow reduces infarct size and improves left ventricular performance and patient survival, reperfusion can also lead to further myocardial injury. Patients undergoing cardiopulmonary bypass also experience reperfusion once they are taken off bypass, and inhibition of reperfusion injury has been shown to decrease morbidity and mortality.[1] In fact, one autopsy-based study concluded that reperfusion injury was responsible for a quarter of all post-cardiopulmonary bypass deaths.[2] Thus, a large number of patients each year experience reperfusion and the injury created by it. There are 4 types of reperfusion injury that have been reviewed elsewhere: lethal cell death due to reperfusion, micro-vascular reperfusion injury, stunned myocardium, and reperfusion arrhythmias.[3] The injury observed after reperfusion is thought to be due to release of toxic oxygen free radicals.[4,5] These radicals are primarily released by neutrophils, which are activated and migrate into the reperfused myocardium.[6] Oxygen free radicals damage cells by peroxidation of lipids in cell membranes, and by degradation of proteins and nucleic acids.[7] Activated neutrophils generate oxygen radicals and the more potent hypochlorous acid via NADPH oxidase and myeloperoxidase.[8] There is evidence that oxidant stress during reperfusion does occur in humans, as indicated by the formation of iso-prostanes IFP2α-I and 8-epi-prostaglandin F2α.[9] Leucocyte aggregates may also obstruct the micro-vasculature and produce areas of poor blood flow. Thus, it seems that therapies preventing neutrophil accumulation in reperfused tissue would hold promise in attenuating reperfusion injury.
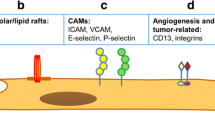
The initial event in leucocyte adhesion to endothelial cells of reperfused vasculature is called rolling. Selectins mediate the rolling interaction between activated leucocytes, endothelial cells and platelets. L-selectin is present on leucocytes, E- and P-selectins are present on endothelial cells, and P-selectin is present on platelets. Sialyl Lewisx (PSGL-1) is the ligand for E- and P-selectins. After the initial adhesion of neutrophils to the endothelium by selectins, the Mac-1 receptor and the LFA-1 receptor strengthen the attachment. The Mac-1 receptor, an integrin, is composed of 2 subunits: α (CD11b) and β (CD18). The Mac-1 receptor is expressed on phagocytic cells, minor subsets of B and T cells, and natural killer cells. It recognises and interacts with intercellular adhesion molecule-1 (ICAM-1),[10] as well as other ligands including fibrinogen and glycoprotein-1 b onplatelets.[11] Patients with unstable angina pectoris tend to have higher expression of Mac-1 receptors in coronary sinus blood,[12] and reperfused patients after MI have higher CD11b expression on neutrophils.[13] The ICAM-1 receptor further strengthens the neutrophil-endothelial cell interaction and results in the cessation of rolling; this activity is necessary for the subsequent migration of neutrophils across the vessel wall.[14] In theory, inhibition of any of these receptors responsible for neutrophil adhesion and migration holds promise in attenuating or preventing reperfusion injury.
1. Targeting the Mac-1 Receptor
1.1 Anti-Mac-1 Receptor Antibodies in Animal Models of Reperfusion Injury
Numerous animal experiments aimed at preventing reperfusion injury have been performed using antibodies directed against components of the Mac-1 receptor. The first such investigation studied open-chest anaesthetised dogs that had left circumflex artery (LCX) occlusions for 90 minutes followed by reperfusion for 6 hours. Administration of an anti-Mac-1 antibody, Mo-1 (a monoclonal antibody directed against CD11b/CD18), did not alter baseline neutrophil counts, suggesting that its mechanism of action was not related to a decrease in the number of neutrophils. The mean size of the resultant myocardial infarct was reduced by 46% in the group receiving the antibody, and ST segment elevation analysis suggested that anti-Mo1 reduced infarct size independently of the severity of ischaemia.[15]
A study of ischaemia and reperfusion in cats showed similar results. Pentobarbital-anaesthetised cats were subjected to 1.5 hours of occlusion of the left anterior descending coronary artery (LAD) and 4.5 hours of reperfusion. One group received MAb R15.7, an antibody directed against the common β-chain (CD18) of the Mac-1 receptor, while the other group received placebo. The antibody-treated animals had a lower plasma creatine kinase level at every time-point after 2 hours, a reduced area of cardiac necrosis, lower myelo-peroxidase activity, and significantly preserved vasorelaxant responses of LAD coronary rings to the endothelium-dependent vasodilators acetyl-choline and the calcium ionophore A-23187.[16]
A canine study of an anti-CD18 antibody evaluated neutrophil localisation. The LCX was occluded for 1 hour in open-chest animals followed by reperfusion for 1, 2, 3 or 4 hours. During the first hour of reperfusion, neutrophil localisation, as assessed by 99mTc-labelled autologous neutrophils, occurred preferentially in the subendocardial region and was inversely correlated with blood flow. Neutrophil localisation decreased after the first hour. Dogs were given the anti-CD18 monoclonal antibody R15.7 (MAb R15.7, 1 mg/kg intravenously) before 1 hour of occlusion followed by 1 hour of reperfusion. When compared with control animals, the antibody-treated animals demonstrated significant attenuation of neutrophil localisation in the subendocardial region.[17] These data suggest that reperfusion injury occurs very quickly after reperfusion and that, optimally, therapies should be given before attempting reperfusion by PTCA or thrombolysis.
The role of anti-CD18 antibodies in preserving left ventricular function has also been described in a canine model. Animals undergoing 90-minute LCX occlusion and 48-hour reperfusion received either 1 mg/kg bodyweight of MAb R15.7 or saline 10 minutes prior to reperfusion. Contrast ventriculography was performed at baseline, during occlusion and at 48 hours. The antibody reduced infarct size after adjusting for collateral flow. At 48 hours after reperfusion, the ejection fraction and inferior wall regional cord shortening were both higher in the antibody-treated group than in controls.[18] Protection against reperfusion injury may indeed have immediate benefits in preventing morbidity and mortality in cardiogenic shock and congestive heart failure resulting from a low cardiac output state. However, the effect of acute reperfusion injury reduction on long term cardiac function is still not known.
There are data in laboratory studies of rats which show that antibodies against CD18 also reduce reperfusion injury. Langendorff-perfused rat hearts were subjected to 20 minutes of global ischaemia followed by 45 minutes of reperfusion. Human polymorphonuclear neutrophils (PMNs) and rat plasma were infused directly into the coronary circulation of nonischaemic and postischaemic hearts. When rat plasma was infused into nonischaemic hearts, no significant alterations in coronary flow, left ventricular developed pressure or left ventricular end-diastolic pressure were observed. When the same hearts were reperfused, a marked impairment of contractile function and a reduction in coronary flow were noted throughout the reperfusion period, as well as an elevation in left ventricular end-diastolic pressure. In rats treated with MAb R15.7 (20 µg/ml) at the time of reperfusion, a greater recovery of coronary flow and left ventricular developed pressure, as well as an attenuation of the elevation seen in left ventricular end-diastolic pressure, were observed.[19] Despite the obvious limitations of the study, it nevertheless seems that the use of monoclonal blocking antibodies against CD18 holds promise in helping to preserve cardiac function after MI or cardiopulmonary bypass.
Finally, primate studies have been performed and show similar promise in decreasing infarct size with the use of an anti-CD18 antibody. In closed-chest baboons, a protocol of LAD occlusion for 90 minutes followed by 4 hours of reflow was studied. Animals were treated with CLB54, a monoclonal immunoglobulin (Ig) G4 antibody directed against CD18, 20 minutes prior to reperfusion. Coronary flow was assessed using radiolabelled microspheres. Infarct size was measured by triphenyl-tetrazolium chloride staining, and global and regional ventricular function were assessed by contrast ventriculography. Neutrophil accumulation was quantitated by a myeloperoxidase assay. CLB54 treatment reduced infarct size, expressed as a percentage of the risk region, by approximately 50%. Therapy was also associated with diminished myeloperoxidase activity and greater postreperfusion coronary flow in the risk region.[20] These primate data are promising. However, the effect of CLB54 in the setting of coronary thrombosis is not known. This limitation, shared by the previous investigations, reduces effective correlations with the human situation following emergent PTCA or thrombolytics in the setting of acute MI.
1.2 Anti-Mac-1 Receptor Antibodies in Human Trials
1.2.1 HALT MI Trial
There have been 2 reported human trials evaluating the safety and efficacy of monoclonal anti-CD11/CD18 antibodies as adjunctive therapy in patients with acute MI.[21,22] The HALT MI study was designed to test the hypothesis that the humanised anti-CD11/CD18 monoclonal antibody rovelizumab (Hu23F2G) would reduce infarct size in patients treated with primary angioplasty.[21] Enrolled patients (n = 420) had either anterior MI [ST segment elevation ≥2mm in at least 2 contiguous precordial leads (33% of patients)], new left bundle branch block, or inferior MI (ST segment elevation ≥1mm in 2 or more inferior leads with reciprocal ST segment depression of ≥0.5mm in 2 or more precordial leads). Patients were randomised to receive 0.3 mg/kg (n = 128), 0.1 mg/kg (n = 139) or placebo (n = 153). The study drug was administered as a bolus over 1 to 2 minutes. It had been previously demonstrated that this dosage inhibited 80% of CD11/CD18 receptors for up to 24 hours. The humanised monoclonal antibody inhibited all forms of the CD11/CD18-integrin complex. The primary end-point was infarct size, as determined by 99Tc sestamibi single photon emission computed tomography imaging 5 to 9 days later after initial presentation.
The final results of the trial were disappointing, showing no effect of the drug in reducing infarct size. Similarly, the TIMI frame count, an indicator of coronary blood flow, also did not differ between study groups. There are several potential explanations for the lack of benefit. Many patients (70%) received abciximab, and the effect of this drug may also have ‘diluted’ the effect of rovelizumab, since it has also been reported that abciximab inhibits CD11b/CD18. The percentage of patients with large infarcts was overall fairly small, and thus a beneficial effect of the drug in reducing the size of large infarcts may have been missed. The dose and duration of therapy may also have been insufficient. Despite the overwhelming benefits observed in animal trials, it is possible that adhesive molecules other than CD11/CD18 receptors are more important in initial leucocyte influx into the reperfused myocardium in humans. Finally, the leucocyte may not hold the key to reperfusion injury in humans reperfused by primary angioplasty.
1.2.2 LIMIT AMI Trial
Results of the LIMIT AMI study[22] were similar to those of the HALT MI Trial. This study assessed the safety of another monoconal antibody, a recombinant humanised antibody against CD18, erlizumab (rHuMab CD18), which had also been demonstrated to reduce infarct size in animal models. In LIMIT AMI, 413 patients with acute MI were treated with alteplase and received high or low dose erlizumab or placebo. Over two-thirds of the patient population received angioplasty in addition to other interventions. No benefits with respect to TIMI frame count, rate of ST segment resolution or infarct size were demonstrated. Clinical end-points also were not affected. As in HALT MI, infections were most common in the high dose treatment groups. None of the infections that developed were life-threatening; they included urinary tract infections and gingivitis.
2. Targeting P-Selectin
Antibodies directed against P-selectin can also decrease reperfusion injury. P-selectin is stored in the α granules and Weibel-Palade bodies of endo-thelial cells and is rapidly expressed on the cell surface upon activation, such as by hypoxia/reoxygenation.[23] Antibodies against P-selectin have been shown to inhibit platelet and PMN aggregation in vitro. The mechanism behind this phenomenon is the triggering of Mac-1 phosphorylation and inactivation by P-selectin, accompanied, and probably regulated, by tyrosine phos-phorylation of a 110kD protein.[24] The major ligand for P-selectin is a mucin-like glycoprotein, P-selectin glycoprotein ligand-1 (PSGL-1).[25,26] Blocking the function of PSGL-1 effectively antagonises P-selectin.
P-selectin is crucial in endothelial physiology, not only with respect to neutrophils, but also T helper cells, eosinophils and monocytes. T helper 1 cells are able to bind P-selectin.[27] These cells are crucial in immune function and may contribute to releasing cytokines and paracrine substances, which play a major role in reperfusion injury. Eosinophils also bind to P-selectin. Monoclonal antibodies to P-selectin can prevent eosinophil tethering on inflammatory endothelium.[28] Anti-PSGL-1 monoclonal antibodies decrease monocyte string formation and, in combination with an L-selectin antibody, prevent monocyte strings and inhibit 86% of accumulation.[29]
A murine study was conducted to determine whether endothelial or platelet P-selectin plays the key role in postischaemic platelet-endothelial cell interactions. P-selectin or wild-type platelets were transfused into P-selectin-deficient or wild-type mice. The study demonstrated that endothelial P-selectin was necessary for platelet rolling and adhesion, but platelet P-selectin was not. Ischaemia followed by reperfusion also increases endothelial cell expression of P-selectin.[30]
Leucocyte rolling along endothelial cells is one of the hallmarks of early reperfusion injury. Increased expression of P-selectin on coronary endothelial cells is also noted in reperfused rat hearts.[31] In theory, the therapeutic potential of inhibitors of P-selectin to decrease rolling exists. Using intravital microscopy, P-selectin-induced rolling was observed after 60 minutes of ischaemia. Rolling was decreased by 60% after administration of an anti-P-selectin antibody,[32] lending support to this hypothesis. Inhibitors of P-selectin other than monoclonal antibodies have also been described, including adenosine[33] and CY-1503,[34] and have been studied in ischaemia/reperfusion models.
2.1 P-Selectin Antagonists in Animal Models of Reperfusion Injury
2.1.1 Anti-P-Selectin MAb PB1.3
Various animal models of reperfusion injury have been developed to study the effect of anti-P-selectin antibodies on reperfusion injury. A lamb model using blood-perfused, isolated neonatal lamb hearts underwent 2 hours of hypothermic cardioplegic arrest and 2 hours of reperfusion. Immediately before reperfusion, a murine anti-ovine P-selectin monoclonal antibody named 6F3 was added to the perfusate (15 µg/ml) group. At 30 minutes of reperfusion, hearts treated with monoclonal antibody to P-selectin achieved significantly greater recovery of maximum developed pressure, maximum positive first derivative of pressure (dP/dt), and maximum negative dP/dt compared with controls.[35] Thus, inhibition of P-selectin by monoclonal antibodies seems to show promise in preserving cardiac function after reperfusion.
A canine model of ischaemia/reperfusion evaluating the effect of an anti-P-selectin antibody in providing meaningful long term protection and preservation of left ventricular function has been reported.[36] Closed-chest dogs underwent 90-minute LAD occlusion and 48 hours of reperfusion. Animals were randomly assigned to receive either 1 mg/kg of the P-selectin blocking antibody PB 1.3, 1 mg/kg of the nonblocking antibody PNB1.6, or an equivalent volume of saline 10 minutes prior to reperfusion. The P-selectin blocking antibody decreased neutrophil activation and reduced infarct size by 25%. However, the blocking antibody did not preserve blood flow to the ischaemic-reperfused myocardium, nor did it improve global or regional left ventricular function.[36]
A similar feline model has been created.[37] Anaesthetised cats were given MAb PB1.3 after 80 minutes of ischaemia and 10 minutes prior to reperfusion. To prove that decreased infarct size was due to blocking of P-selectin, a nonblocking antibody for P-selectin was administered to 1 group. The study found a significant decrease in myocardial necrosis in the cats receiving the blocking antibody. MAb PB 1.3 also decreased the adherence of unstimulated PMNs to thrombin- and histamine-stimulated endothelial cells in a concentration-dependent manner and helped preserve secretion of endothelium-derived relaxing factor.[37] As with the other studies, the anti-P-selectin antibody appeared to decrease infarct size after reperfusion. However, the functional consequences of decreased infarct size were not evaluated.
Anti-P-selectin antibodies may also hold promise as an adjunct to thrombolysis through their inhibition of leucocyte attachment to platelets as well as to the injured arterial wall. In theory, preventing leucocyte adhesion to the endothelium wall may help to prevent further vessel wall injury via toxic oxygen free radicals and recruitment of platelets through cytokine signalling. Subsequently, there may be less thrombosis, as well as reduced reperfusion injury. In addition, the interactions mediated by P-selectin between neutrophils and platelets could be used to target thrombolytics to the site of vascular injury during acute MI, stroke or thrombo-embolic disease.
2.1.2 P-Selectin Antagonist rPSGL-Ig
A soluble PSGL-1-Ig chimera (rPSGL-Ig), consisting of a truncated form of recombinant human PSGL-1 covalently linked to IgG, has also been studied as an adjunct to thrombolytic therapy.[38] This fusion peptide is a competitive inhibitor of PSGL-1, and therefore functions as an inhibitor of neutrophil-endothelial cell adherence via P-selectin. In a copper coil thrombosis model, Yorkshire pigs received heparin and then 15 minutes later either a carrier solution alone or the carrier solution and rPSGL-Ig. All of the animals also received alteplase at a dose of 25mg with 10% of the total dose administered as an initial bolus. Arteriograms were taken every 10 minutes for up to 60 minutes, and flow through the arteries was graded on a scale of 0 to 3, with 0 representing an occluded vessel and 3 representing normal flow. The study’s end-point was time to establish near normal TIMI (grade 2 or 3) flow. Eight of 9 control pigs had reoccluded arteries at the end of the alteplase infusion, compared with 1 of 9 rPSGL-Ig-treated pigs. In addition, near normal flow after thrombolysis was achieved approximately 60% faster in the rPSGL-Ig-treated pigs.[38] This study suggests that adding rPSGL-Ig to thrombolytic regimens may be promising in establishing reflow early and preventing reocclusion.
2.2 Anti-P-Selectin Antibodies in Human Trials
Human antibodies to P-selectin have been studied in monkeys. Multiple murine antibodies to P-selectin have been developed, but murine antibodies in humans have short circulating half-lives and generally induce potent human antimouse antibody responses. Through genetic engineering, a human version of the antibody mEP-5C7 incorporating human γ4 heavy and κ light chain regions was developed and named HuEP5C7.g4. However, this antibody was even more rapidly eliminated than the original murine antibody when given to rhesus monkeys. In an effort to increase the half-life of the antibody, the human γ4 region was replaced with a γ2 constant region. This new form displayed a long circulation half-life, which was typical of human antibodies.[39] Genetically engineered antibodies could make investigation of an anti-P-selectin antibody in humans with acute thrombotic events a reality. There are no reported clinical studies of anti-P-selectin antibodies in patients with acute myocardial or cerebral infarction.
3. Targeting E-Selectin
E-selectin is a molecule present on neutrophils, monocytes and lymphocytes that allows adherence to vessel walls, where it binds specific ligands. E-selectin is expressed on endothelial cells in response to inflammatory cytokines such as tissue tumour necrosis factor-α or interleukin-1. Thus, inhibition of E-selectin with monoclonal antibodies may be a possible strategy for the prevention of ischaemia/reperfusion injury.
A rat experimental model has been performed to evaluate the effect of ischaemia/reperfusion injury modulation by blocking E-selectin. Pento-barbital-anaesthetised rats underwent 1 hour of ischaemia followed by 1 hour of reperfusion. A control group consisted of rats receiving a sham operation. Rats receiving a hyperimmune serum containing antibodies against E-selectin had a markedly improved survival rate, reduced myocardial injury, lowered serum creatine kinase activity and decreased myeloperoxidase activity in the area at risk. Thus, E-selectin could be a possible adhesive molecule to target in humans to reduce the morbidity and mortality of MI.[40]
4. Targeting the Fibrinogen Receptor α IIb β3 (Abciximab)
The monoclonal antibody abciximab has also been investigated to prevent reperfusion injury.[41,42] This antibody binds to the fibrinogen receptor α IIb β3 on platelets and is a powerful antiplatelet agent. It has been studied extensively in various acute cardiac states and has been shown to reduce morbidity and mortality, presumably by its antiplatelet effect. Its role in attenuating thrombosis by blocking the α IIb β3 receptor has been established and is not further discussed in this review. Abciximab also binds to both activated αM β2 receptors and αV β3 receptors. These receptors are present on granulocytes and monocytes and have been implicated in atherosclerosis, initial hyper-plasia after vascular injury, reperfusion injury and thrombin generation. In addition, αV β3 may mediate platelet adhesion to osteopontin.[43] Abciximab affects leucocyte adhesive function via decreased expression of Mac-1. One study showed that binding of an anti-CD11 monoclonal antibody was not affected by high dose abciximab.[44] Another study suggests that abciximab does reduce the expression of CD11b on leucocytes in whole blood.[45]
There are further animal data that suggest abciximab may be a useful agent for protection from reperfusion injury. A PMN/platelet perfused rat model of ischaemia for 20 minutes followed by 45 minutes of reperfusion has been reported. Ten minutes before reperfusion, 1 group of rats received 6.5 µg/kg of abciximab. The rats receiving abciximab had improved postreperfusion coronary flow and preserved postreperfusion left ventricular developed pressure and maximum dP/dt. On a microscopic level, abciximab seemed to have an effect on the migration of PMNs into tissue after reperfusion, with abciximab-treated hearts having 7 ± 1 PMNs/mm2 compared with 38 ± 1 PMNs/mm2 in control hearts. Similar results were obtained in rat hearts perfused with PMNs but not platelets, suggesting that abciximab can prevent neutrophil accumulation by directly affecting neutrophils.[46]
At present, abciximab is commonly used in clinical practice after PTCA and stenting to prevent acute thrombotic occlusion. Abciximab, as an antiplatelet agent, may also have a role in the prevention of cyclic flow reductions following coronary catheter-based interventions. It has also been shown that abciximab can lead to better recovery of left ventricular function following acute MI treated by catheter-based therapy. This latter effect may be mediated by a reduction in microvascular plugging by platelets and possibly leucocytes.
5. Other Monoclonal Antibodies and Receptor Antagonists
Platelet-endothelial cell adhesion molecule-1 (PECAM-1) mediates neutrophil transmigration, presumably through an interaction between platelets, neutrophils and endothelial cells. A human polyclonal antibody against PECAM-1 has been developed. Cross-reactivity of this antibody to feline coronary vascular cells and neutrophils has been observed by immunohistochemistry and flow cytometry. Anti-PECAM-1 antibody was administered 10 minutes before reperfusion of feline hearts. Animals receiving the anti-PECAM antibody had significantly decreased infarct size (12 ± 2 vs 29 ± 4% of area at risk) compared with cats receiving a control rabbit IgG and the rise in plasma creatine kinase was attenuated.[47]
As previously described, the ligands for P- and L-selectin are carbohydrate-containing moieties such as the sialyl Lewis-containing oligosaccharide (SLex-OS). In another feline model of myocardial ischaemia and reperfusion, animals were treated with SLex-OS 10 minutes prior to reperfusion. Compared with the control group, the SLex-OS group had preserved cardiac contractility and endothelium-dependent relaxation to acetyl-choline in coronary artery rings. In addition, in vitro PMN adherence to coronary vascular endo-thelium after 270 minutes of reperfusion was significantly attenuated in the SLex-OS-treated group.[48] Administration of exogenous SLex-Os serves to competitively inhibit the endogenous ligands and therefore the interaction with L- or P-selectin.
6. Conclusion
Injury induced by reperfusion is a major component of total injury resulting from acute MI in animal studies. As our understanding of the patho-physiology of reperfusion injury grows, novel treatments aimed at reducing tissue damage are being developed. Numerous monoclonal antibodies to platelet, endothelial and neutrophil receptors have been developed and show promise in animal studies. These include antibodies targeting the Mac-1 receptor, P-selectin, E-selectin, the fibrinogen receptor α IIb β3, and PECAM-1. In animal models, these antibodies decrease infarct size, preserve contractility, improve haemodynamics and help maintain acetylcholine-dependent endothelial relaxation.
However, preliminary investigations in humans with antileucocyte antibodies, specifically those directed against the CD11/CD18 receptor complex, have not shared the results observed in animal studies. Many explanations have been proposed for these discouraging results. Nevertheless, the sponsors of the LIMIT AMI and HALT MI trials do not appear willing to further develop these agents as adjuncts to standard reperfusion therapy for acute MI. This decision is particularly unfortunate, as the inherent benefit of the drug may have been missed because of specific design issues of these investigations. For instance, abciximab was given to a high proportion of the patients in both trials, as many patients had intracoronary stent placement. Abciximab has an effect on Mac-1 by itself, and perceiving a benefit of the other monoclonal antibody may be difficult to differentiate from that of abciximab alone. Second, as there are multiple platelet receptors involved in the dynamic thrombotic process during MI, theoretically blocking more than one adhesive molecule pathway at once with multiple monoclonal antibodies might hold promise. Finally, these drugs may benefit only patients with the largest infarcts. Further investigations limited to such patients appear warranted.
References
Hill GE. Cardiopulmonary bypass-induced inflammation: is it important? J Cardiothorac Vasc Anesth 1998; 12 (2 Suppl. 1): 21–5
Weman SM, Karhunen PJ, Penttila A, et al. Reperfusion injury associated with one-fourth of deaths after coronary artery bypass grafting. Ann Thorac Surg 2000; 70(2): 807–12
Kloner RA. Does reperfusion injury exist in humans? J Am Coll Cardiol 1993; 21(2): 537–45
McCord JM. Free radicals and myocardial ischemia: overview and outlook. Free Radic Biol Med 1998; 4: 9–14
Zweier JL, Rayburn BK, Flaherty JT, et al. Recombinant superoxide dismutase reduces oxygen free radical concentrations in reperfused myocardium. J Clin Invest 1987; 80: 1728–34
Schaper W, Schaper J. Problems associated with reperfusion of ischemic myocardium. Pathophysiol Severe Myocard Injury 1990; 41: 269
Becker LC, Ambrosio G. Myocardial consequences of reperfusion. Prog Cardiovasc Dis 1987; 30: 23–44
Lucchesi BR, Mullane KM. Leukocytes and ischemia induced myocardial injury. Annu Rev Pharmacol Toxicol 1988; 26: 201–24
Reilly MP, Delanty N, Roy L, et al. Increased formation of the isoprostanes IPF2alpha-I and 8-epi-prostaglandin F2alpha in acute coronary angioplasty: evidence for oxidant stress during coronary reperfusion in humans. Circulation 1997; 96(10): 3314–20
Ross GD, Vetvicka V. CR3 (CD11b, CD18): a phagocyte and NK cell membrane receptor with multiple ligand specificities and functions. Clin Exp Immunol 1993; 92(2): 181–4
Simon DI, Chen Z, Xu H, et al. Platelet glycoprotein Ib alpha is a counterreceptor for the leukocyte integrin Mac-1 (CD11b/CD18). J Exp Med 2000; 192(2): 193–240
De Servi S, Mazzone A, Ricevuti G, et al. Clinical and angiographic correlates of leukocyte activation in unstable angina. J Am Coll Cardiol 1995; 26(5): 1146–50
Neumann FJ, Ott I, Gawaz M, et al. Cardiac release of cytokines and inflammatory responses in acute myocardial infarction. Circulation 1995; 92(4): 748–55
Gurbel PA, Kolodgie F, Serebruany V, et al. Myocardial cell injury during ischemia and reflow. In: Bittar E, Bittar N, editors. Principles of medical biology. Stamford, CT: JAI Press, 1998: 127–66
Simpson PJ, Todd RD, Fantone JC, et al. Reduction of experimental canine myocardial reperfusion injury by a monoclonal antibody (anti-Mo1, anti-CD11b) that inhibits leukocyte adhesion. J Clin Invest 1988; 81(2): 624–9
Ma XL, Tsao PS, Lefer AM. Antibody to CD-18 exerts endothelial and cardiac protective effects in myocardial ischemia and reperfusion. J Clin Invest 1991; 88(4): 1237–43
Dreyer WJ, Michael LH, West MS, et al. Neutrophil accumulation in ischemic canine myocardium. Insights into time course, distribution, and mechanism of localization during early reperfusion. Circulation 1991; 84(1): 400–11
Arai M, Lefer DJ, So T, et al. An anti-CD 18 antibody limits infarct size and preserves left ventricular function in dogs with ischemia and 48-hour reperfusion. J Am Coll Cardiol 1996; 27(5): 1278–85
Lefer DJ, Shanelya SM, Serrano Jr CV, et al. Cardioprotective actions of a monoclonal antibody against CD-18 in myocardial ischemia-reperfusion injury. Circulation 1993; 88 (4 Pt 1): 1779–87
Aversano T, Zhou W, Nedelman M, et al. A chimeric IgG4 monoclonal antibody directed against CD 18 reduces infarct size in a primate model of myocardial ischemia and reperfusion. J Am Coll Cardiol 1995; 25(3): 781–8
Faxon DP, Gibbons RJ, Chronos NAF, et al. The effect of a CD11/CD18 inhibitor (Hu23F2G) on infarct size following direct angioplasty: the HALT MI study [abstract]. Circulation 1999; 100(18): I–791
Baran K. LIMIT AMI trial [oral presentation]. Presented at the Congress of the European Society of Cardiology; 2000 Aug 26-30: San Francisco
Pinsky DJ, Naka Y, Liao H, et al. Hypoxia-induced exocytosis of endothelial cell Weibel-Palade bodies. A mechanism for rapid neutrophil recruitment after cardiac preservation. J Clin Invest 1996; 97: 493
Evangelista V, Manarini S, Sideri R, et al. Platelet/polymorphonuclear leukocyte interaction: P-selectin triggers proteintyrosin phosphorylation-dependent CD11b/CD18 adhesion: role of PSGL-1 as a signaling molecule. Blood 1999; 93(3): 876–85
Moore KL, Stults NL, Diaz S, et al. Identification of a specific glycoprotein ligand for P-selectin (CD62) on myeloid cells. J Cell Biol 1992; 118:445–56
Sako D, Chang XJ, Barone KM, et al. Expression cloning of a functional glycoprotein ligand for P-selectin. Cell 1993; 75: 1179–86
Austrup F, Vestweber D, Borges E, et al. P- and E-selectin mediate recruitment of T-helper-1 but not T-helper-2 cells into inflamed tissues. Nature 1997; 385(6611): 81–3
Kitayama J, Fuhlbrigge RC, Puri KD, et al. P-selectin, L-selectin, and alpha 4 integrin have distinct roles in eosinophil tethering and arrest on vascular endothelial cells under physiological flow conditions. J Immunol 1997; 159(8): 3929–39
Lim YC, Snapp K, Kansas GS, et al. Important contributions of P-selectin glycoprotein ligand-1-mediated secondary capture to human monocyte adhesion to P-selectin, E-selectin, and TNF-alpha-activated endothelium under flow in vitro. J Immunol 1998; 161(5): 2501–8
Massberg S, Enders G, Leiderer R, et al. Platelet-endothelial cell interactions during ischemia/reperfusion: the role of P-selectin. Blood 1998; 92(2): 507–15
Lefer AM, Campbell B, Scalia R, et al. Synergism between platelets and neutrophils in provoking cardiac dysfunction after ischemia and reperfusion: role of selectins. Circulation 1998; 98(13): 1322–8
Kubes P, Jutila M, Payne D. Therapeutic potential of inhibiting leukocyte rolling in ischemia/reperfusion. J Clin Invest 1995; 95(6): 2510–9
Minamino T, Kitakaze M, Asanuma H, et al. Endogenous adenosine inhibits P-selectin-dependent formation of coronary thromboemboli during hypoperfusion in dogs. J Clin Invest 1998; 101(8): 1643–53
Park IY, Lee DS, Song MH, et al. Cylexin: a P-selectin inhibitor prolongs heart allograft survival in hypersensitized rat recipients. Transplant Proc 1998; 30(7): 2927–8
Nagashima M, Shin’oka T, Nollert G, et al. Effects of a monoclonal antibody to P-selectin on recovery of neonatal lamb hearts after cold cardioplegic ischemia. Circulation 1998; 98 (19 Suppl.): II391–7, discussion II397-8
Arai M, Masui Y, Goldschmidt-Clermont P, et al. P-selectin inhibition prevents early neutrophil activation but provides only modest protection against myocardial injury in dogs with ischemia and forty-eight hours reperfusion. J Am Coll Cardiol 1999; (34) 1:280–8
Weyrich AS, Ma XY, Lefer DJ, et al. In vivo neutralization of P-selectin protects feline heart and endothelium in myocardial ischemia and reperfusion injury. J Clin Invest 1993; 91(6): 2620–9
Kumar A, Villani MP, Keith Jr JC, et al. Recombinant soluble form of PSGL-1 accelerates thrombolysis and prevents reocclusion in a porcine model. Circulation 1999; 99(10): 1363–9
He XY, Xu Z, Melrose J, et al. Humanization and pharmacokinetics of a monoclonal antibody with specificity for both E-and P-selectin. J Immunol 1998; 160(2): 1029–35
Altavilla D, Squadrito F, Ioculano M, et al. E-selectin in the pathogenesis of experimental myocardial ischemia-reperfusion injury. Eur J Pharmacol 1994; 270(1): 45–51
Coller BS. Binding of abciximab to alphaVbeta3 and activated alphaMbeta2 receptors: with a review of platelet-leukocyte interaction. Thromb Haemost 1999; 82(2): 326–36
Neumann FJ, Blasini R, Schmitt C, et al. Effect of glycoprotein IIb/IIIa receptor blockade on recovery of coronary flow and left ventricular function after the placement of coronary-artery stents in acute myocardial infarction. Circulation 1998; 98(24): 2695–701
Coller BS. Potential non-glycoprotein IIb/IIIa effects of abciximab. Am Heart J 1999; 138 (1 Pt 2): S1–5
Neumann FJ, Zohlnhofer D, Fakhoury L, et al. Effect of glycoprotein IIb/IIIa receptor blockade on platelet-leukocyte interaction and surface expression of the leukocyte integrin Mac-1 in acute myocardial infarction. J Am Coll Cardiol 1999; 34(5): 1420–6
Mickelson J, Ali N, Kleiman NS, et al. Chimeric 7E3 Fab (ReoPro) decreases detectable CD11b on neutrophils from patients undergoing coronary angioplasty. J Am Coll Cardiol 1999; 33(1): 97–106
Campbell B, Chuhran CM, Lefer DJ, et al. Cardioprotective effects of abciximab (ReoPro) in an isolated perfused rat heart model of ischemia and reperfusion. Methods Find Exp Clin Pharmacol 1999; 21(8): 529–34
Murohara T, Delyani JA, Albelda SM, et al. Blockade of platelet endothelial cell adhesion molecule-1 protects against myocardial ischemia and reperfusion injury in cats. J Immunol 1996; 15(6): 3550–7
Buerke M, Weyrich AS, Zheng Z, et al. Sialyl Lewisx-containing oligosaccharide attenuates myocardial reperfusion injury in cats. J Clin Invest 1994; 93(3): 1140–8
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McKenzie, M.E., Gurbel, P.A. The Potential of Monoclonal Antibodies to Reduce Reperfusion Injury in Myocardial Infarction. BioDrugs 15, 395–404 (2001). https://doi.org/10.2165/00063030-200115060-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00063030-200115060-00005