
Abstract
Background
Malaria is still a vital global health issue. The greatest disease burden is in sub-Saharan Africa. A. aspera is one of the medicinal herbs commonly used traditionally. The continuous resistance of Plasmodium falciparum, to available anti-malarial agents has led to the search for an alternative substance to combat malaria; hence, the study aimed to establish the potential of the extract from the shoot of Achyranthes aspera as an alternative anti-malarial agent against Plasmodium berghei (NK-65) strain in mice model. Acute toxicity test was performed as per the Organization for Economic Cooperative Development guidelines, 425. Rodent malaria parasite P. berghei at 1 × 107 parastemia was inoculated into Swiss albino mice of both sexes intraperitoneally. The extract was administered through oral route by an intra-gastric tube once daily for 5 days according to the Rane’s curative test. Chloroquine and Artemisinin were used as standard drugs and were administered through the same route.
Results
Phytochemical screening of A. aspera revealed the presence of phenols, tannins, alkaloids, saponins, flavonoids, and balsam. A. aspera extract neither caused any sign of gross toxicity nor caused mortality in the mice up to a single dose of 5000 mg/kg/bwt. The aqueous extract, of A. aspera, showed significant reduction (p < 0.05) in parasitemia at dose 400 mg/kg/day and 600 mg/kg/day in Swiss albino mice compared to negative control. The treated mice had prolonged survival time at all doses. Extracts prevented P. berghei induced body weight loss and temperature reduction compared to the negative control.
Conclusion
We conclude that the shoot extract of A. aspera is safe and displayed promising anti-malarial activity. This may account for its traditional use for malaria treatment among some locals in Nigeria.
Similar content being viewed by others


Background
Malaria is one of the major infectious diseases responsible for the high rate of mortality and morbidity in developing countries (Alli, Adesokan, & Salawu, 2016). It is transmitted to people through the bites of infected female Anopheles mosquitoes (Dunavan, 2005). It is preventable and curable (World Health Organisation (WHO), 2020). Human malaria is caused by an apicomplexan parasite of the genus Plasmodium. Four species are known to cause human malaria namely, Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, and Plasmodium malariae. Nevertheless, P. falciparum has been found to be the most lethal of all malaria parasites. Most of the severe clinical cases and death were caused by Plasmodium falciparum this parasite causes epidemics in malaria endemic countries, resulting in large number of deaths (Mbugi et al., 2006). In particular, young children less than 5 years of age, pregnant women, and non-immune visitors to malarious areas are at greatest risk of severe or fatal illness (Bloland, and Organization, W.H., 2001). An infection with P. falciparum begins when sporozoites are injected into the blood stream of the vertebrate host through mosquito bite. The sporozoites invade hepatocytes where they form merozoites which are then released into the blood stream of infected erythrocytes (Halder, Bhattacharjee, & Safeukui, 2018).
According to WHO report 70-80% of worlds population rely on non-conventional primary health care (Chan, 2003; WHO, 2003), Africa carries disproportionately high share of the global malaria burden with 94% of malaria cases and malaria deaths. Nigeria has a global malaria share of 25%, of global malaria cases in 2019 and accounted for the highest number of death (24% of global malaria deaths). Nigeria is among one of the five countries which accounted for nearly half of global malaria cases and reported more malaria cases and deaths, than any other countries (Krishna & Kumar, 2019; World Health Organization, 2019). Despite the efforts of WHO to eradicate the disease, malaria still remain an endemic disease in many tropical countries. Several anti-malarial agents have been developed to control and eliminate malaria, but none of these remains effective against the pathogen over time. As a result, P. falciparum malaria infection remains a major public health problem especially in the tropics (Aung, Jordi, Daniel, & Francios, 2017; Jeanne, Yaye, Marie, & Deise, 2019). Artemisinin combination therapies (ACTs), which have been widely used since the mid 2000 are the current frontline therapy for the treatment of P. falciparum malaria as recommended by the World Health Organization (WHO, 2019). The emergence and spread of resistance to anti-malarial drugs is challenging for malaria control. Plasmodium falciparum has developed resistance to all anti-malarial drug during the past 50 years (Yakoob et al., 2018).
Malaria is transmitted all over Nigeria; 76% of the populations live in high transmission area, while 24% of the population lives in low transmission areas (WHO, 2019). Malaria accounts for 60% of outpatients’ visits, 30% of inpatients hospital admissions and 300,000 of inpatients deaths in Nigeria. Nigeria suffers the world’s greatest malaria burden with approximately 51 million cases and 207,000 deaths, reported annually (Owoeye, Akinyemi, & Yusuf, 2018). The control of malaria has taken a multi-dimensional approach, which involve the control of the vector and the use of drugs for treatment (WHO, 2019).
Natural products, mainly plants, are fundamental source of diverse drugs and therapeutics. The most important and effective drugs used in malaria treatment have been derived from the plants. According to WHO report, about 70–80% of world’s population relies on non-conventional primary health care (Chan, 2003). However, there is lack of enough scientific evidence for the anti-plasmodial activity of A. aspera (shoot).
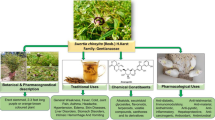
Achyranthes aspera, locally known as “Kiban katangare” (Burkill, 1985) and commonly known as “Pricky Chaff flower” in English, is an annual herb that grows throughout India, Africa, and some parts of Nigeria. It consists of 160 genera and approximately 2400 species of shrubs, herbs, and climbers. Traditionally, A. aspera is known for its diuretic and hepatoprotective properties and are used to cure several diseases including malaria fever, dysentery, asthma, hypertension, and diabetics. A. aspera is widely studied for its vast properties, such as immunostimulatory properties (Edwin et al., 2008) anti-inflammatory (Kumar, Sankar, & Varatharajan, 2009), and wound healing activity (Alam, Karim, & Khan, 2009). However, amongst others, limited data to verify their traditional claims exist on the anti-plasmodial activity of the plant shoot. The anti-malarial activity is based on the ability to inoculate P. berghei into animal model. The use of rodents as model organism in the in vivo studies is based on the physiological similarities between species. Rodent malaria has been validated through the identification of several anti-malarials and remains a standard part of drug discovery and development pathways (Fidock, Rosenthal, Croft, Brun, & Nwaka, 2004).
The present study has been carried out to evaluate the anti-plasmodial efficacy of the extract of A. aspera shoot, as well as asses its safety in mice model.
Methods
Chemicals and reagents
All chemicals, solvents, and reagents used were of analytical grade. Chemicals and solvents were obtained from Sigma-Aldrich, USA, and BDH, England.
Sample collection
A. aspera collection
The A. aspera shoots were collected between the months of May and October 2018, from “Nchiya” which is located in Mangu LGA of Plateau State, Nigeria. The plant was authenticated by a taxonomist and a voucher specimen was deposited at the Herbarium of the Forestry Research Institute (FRIN) Jos, Plateau State, Nigeria. The shoot was air dried at room temperature under shade and ground to a powder using mortar and pestle.
Plant extraction
A total of 80 g dried shoots powder of A. aspera was macerated in 300 ml of distilled water in an Erlenmeyer flask (1 L) for 72 h. The extraction was facilitated by using orbital shaker (Gallenhamp, England) at 120 rpm. The mixture was first filtered with gauze and then Whatman filter paper No. 1. The marc was remacerated for another 72 h twice and filtered. The combined aqueous filtrates were then concentrated in an oven at a temperature of 40 °C. After drying, the extract was stored in tightly closed bottle container in refrigerator at – 20 °C, until used (Sasidharani, Chen, Saravan, Sundram, & Yogalatha, 2011; Yared, Mekonnen, & Debella, 2012).
Experimental animals
Swiss albino mice (male and female, weighing 19–29 g and aged 6–8 weeks), from Animal House Unit Pharmacology Department, Faculty of Pharmaceutical Sciences, University of Jos, were used in the anti-malarial activity study, and all females were used in the toxicity test. The mice were kept in a clean cage in a well-ventilated room and exposed to standard environmental conditions, and had access to standard feed (Vital Feeds-Jos, Plateau), and water ad libitum. Ethics approval and consent to participate with approval number UJ/FPS/F17-00379 was obtained from Ethical Committee of the Department of Pharmacognosy. Experimental protocol was carried out in line with national and international laws and guidelines for Care and Use of Laboratory Animals, as in principle of Laboratory Animal Care (NIH, 1985).
Parasite and inoculation
Chloroquine-sensitive Plasmodium berghei (NK-65) strain, obtained from National Institute of Medical Research (NIMR), University of Ibadan, Oyo State, Ibadan, Nigeria, was used. The parasites were maintained in vivo by serial passage of blood from infected mouse to healthy mouse on weekly basis. Blood from donor mice obtained from the tail was collected on a Petri dish containing 0.5% trisodium citrate. The blood was diluted with physiological saline (0.9%). Mouse was injected intraperitoneally with 0.2 ml infected blood containing 1 × 107 P. berghei-infected red blood cells.
Experimental design
For evaluating the anti-malarial effects of the crude aqueous extract of A. aspera, a total of 35 Swiss albino mice, males and females, were used for the experiment. Chloroquine (CQ) and artemisinin combination therapies (ACTs) were used as standard drugs. After the inoculation, the infected mice were divided into 6 groups of 5 mice each. Five uninfected and untreated mice were used as normal control group. Treatment was given as follows:
Group I: | (Negative control): mice in this group were infected with 0.2 ml P. berghei and left untreated. They received normal feed and distilled water only. |
Group II: | Mice in this group were infected with 0.2 ml P. berghei and treated with 200 mg/kg body weight of aqueous extract of A. aspera shoot. |
Group III: | Mice in this group were infected with 0.2 ml P. berghei and treated with 400 mg/kg body weight of aqueous extract of A. aspera |
Group VI: | Mice in this group were infected with 0.2 ml P. berghei and treated with 600 mg/kg body weight of aqueous extract of A. aspera |
Group V: | (Standard control-1): Mice in this group were infected with 0.2 ml P. berghei and treated with 10 mg/kg of chloroquine. |
Group VI: | (Standard drug control-2): mice in this group were infected with 0.2 ml P. berghei and treated with 25 mg/kg artemisinin combination therapies (ACTs) |
Group VII: | The mice in this group were not infected and treated, they were given normal feed and distilled water only |
Parasitemia were determined using the method described by Ryley and Peters, 1970. Treatment lasted for 5 days, while experiments lasted for the period of 29 days. After the experiment, mice were not killed, but the survival for each mouse in each group was recorded. Extracts and drugs were administered orally to these groups, and treatment was given once daily for 5 days.
Phytochemical screening (qualitative and quantitative)
Preliminary qualitative screening of secondary metabolites of A. aspera shoot was carried out to identify the classes of constituent using the standard method (Harbone, 1998; Trease & Evans, 1989).
The quantitative determination of phytochemical content was assessed using standard method: flavonoid (Bohr & Kocipal-Abayazan, 1994; Obadani & Ochuko, 2002), Alkaloids (Harbone, 1973), and Saponins (Obadani & Ochuko, 2002).
Acute toxicity studies
The acute toxicity study for the crude aqueous extract was performed according to guidelines of Organization of Economic Cooperative and Development, 425 (OECD). All female Swiss albino mice, five for each dosage, were used. Animals were fasted overnight. The A. aspera aqueous extracts was administered in as single dose of 2000 mg/kg and 5000 mg/kg body weight using oral gastric tube, and the animals were observed individually for 24 h and thereafter, for a total of 14 days to assess safety of the extract. Animals were observed for gross behavioral changes such as loss of appetite, hair erection, lacrimation, diarrhea, deaths, and other signs of overt toxicity (The Organization of Economic Co-operation and Development (OECD), 2008).
Anti-malarial activity (curative test)
Determination of parasitemia
The standard method of Ryley and Peters (1970) was followed to evaluate curative activity. Standard inoculation of 1 × 107 P. berghei parasitized red blood cells was injected intraperitoneally into mice on the first day. After 72 h, mice were divided into six groups of five mice in each group. The parasitemia level of mice in all groups were monitored daily through the collection of blood sample from the tail of each mouse and the smear were made on microscope slides (76 × 26 mm) after fixing with absolute methanol, thin smears were stained with 10% giemsa for 10 min and rinsed with water. Immersion oil was added on the stained slides and viewed under the Olympus microscope (Olympus-CH) × 100 magnification. Three different fields on each slide were then examined in order to calculate the average parasitemia (Hilou, Nacoulma, & Guiguemede, 2006).
Monitoring mean survival time (MST)
The mean survival time was monitored in all the treatment and control groups by finding the average survival time (days) of mice (post-inoculation) over a period of 30 days (D0–D29). As a principle, compound that prolonged survival time beyond 12 days is regarded as active (Ural, Kayalar, Durmuskahya, Carus, & Ozbilgim, 2014)
Determination of packed cell volume (PCV)
Packed cell volume (PCV) was measured by taking blood from the tail of the mouse with heparinized micro-hematocrit tubules. The capillary tubes were filled to ¾ of the height, with blood sealed at the dry end with sealing clay. The tubes were placed in micro-hematocrit centrifuge for 5 min at 12,000 rpm. PCV was determined using micro-hematocrit reader (Hawskley and Sons, England) and calculated (Gilmour & Skyle, 1951). PCV is a measure of proportion of RBC to plasma and measured before inoculating the parasite and treatment using the following:
Measurement of body weight and rectal body temperature of mice
The body weight of mice were measured using sensitive weight balance (Ohaus Corp., USA) on day 0 before infection and day 8 in the curative test. The average body weight was compared with control group over time in each group as described by Dikasso, Mekonnen, and Debella (2006). The rectal body temperature of mice in all groups was measured using clinical digital thermometer. The mean body temperature was compared with control group overtime in each group.
Statistical analysis
Data were analyzed using SPSS 22.0 Statitical Software (SPSS, IBM, Corperation, Armonk, NY, USA), (SPSS INC, 2007). Values are expressed as mean ± standard error mean (SEM). Mean were analyzed by one way analysis of Variance (ANOVA), and compared by Duncan's multiple range rest (DMRT) (Duncan, 1957). Significant difference was accepted at p < 0.05.
Results
Phytochemical screening
The result of the phytochemical screening of shoot of A. aspera (aqueous extract) (Table 1) showed that the extract revealed the presence of flavonoids, tannins, alkaloids, saponins, balsam, and phenols (Table 1). The phytochemical contents of A. aspera shoot gave various levels of alkaloids, flavonoids, saponins, and phenols with saponins occurring in large quantities (Table 2).
Acute toxicity test
In the in vivo acute toxicity studies of the plant extract, there were no gross physical and behavioral changes such as diarrhea, hair erection, and lacrimation. No mortality was recorded at both doses (2000 mg/kg and 5000 mg/kg). Extract was safe in the animals up to 5000 mg/kg, indicating that LD50 of plants extracts is beyond 5000 mg/kg. All the mice survived within the 2 weeks period of observation.
Anti-malarial activity
Curative effect (Rane’s test)
In the curative evaluation the crude extract of A. aspera shoot, all the three doses significantly reduced parasite level on day 6 as compared to day 4. The parasitemia reduction was in a dose-dependent manner. The highest parasitemia reduction was seen by 600 mg/kg dose of extract (Fig. 1). Chloroquine-treated group showed none on the established P. berghei infection. ACTs showed appreciable reduction in parasitemia level progressive increase in the parasitemia level from day 4 to day 7 of the negative control group was observed.

Effects of Aqueous extract of A. aspera shoot on the parasitemia level of mice infected with P. berghei (NK-65). Mice + AAE = infected mice treated with Achyranthes aspera aqueous extract, Con IU = infected mice untreated, Con CQ = infected mice treated with chloroquine (10 mg/kg), Con ACT = infected mice treated with artemisinin (25 mg/kg) and NC = normal control group
Mean survival time (MST)
The effect of extract of A. aspera on the mean survival time of infected mice is presented in Fig. 2. In mean survival time, only the 400 mg/kg and 600 mg/kg extract dose prolonged survival time compared to standard drug, ACTs. However, the mean survival time of mice treated with chloroquine was significantly (P ≤ 0.05) higher than the negative control and also the extract dose-treated groups. (Fig. 2).

Effects of aqueous extract of A. aspera on the MST level of mice infected with P. berghei (NK-65). Mice + AAE = infected mice treated with Achyranthes aspera aqueous extract, mice + IU = infected mice untreated, mice + CQ = infected mice treated with chloroquine (10 mg/kg), mice + ACT = infected mice treated with artemisinin (25 mg/kg), NC = normal control group. Values are expressed as mean ± SEM (n = 5) values with different superscript are significantly different at p < 0.05
Packed cell volume (PCV)
The effects of extracts of A. aspera on the packed cell volume of infected mice are presented in Fig. 3. The A. aspera shoot extract had effect on PCV of the animals compared to the baseline. At all dose levels, the extract did not show preventive effect on the decline in the PCV levels of mice infected with P. berghei (Fig. 3). The reduction in PCV at 600 mg/kg dose level on day 6 was not significant (p < 0.05) compared to the standard drug chloroquine. There was substantial (p < 0.05) increase in the PCV of the control group treated with chloroquine on day 6.

Effect of aqueous extract of A. aspera on the PCV level of mice infected with P. berghei (NK-65). Mice + AAE = infected mice treated with Achyranthes aspera aqueous extract, mice + IU = infected mice untreated, mice + CQ = infected mice treated with chloroquine (10 mg/kg), mice + ACT = infected mice treated with artemisinin (25 mg/kg) and NC = normal control group. Values with different superscript are significantly different at p < 0.05
Rectal body temperature
The effect of extract of A. aspera on rectal body temperature of infected mice is presented in Fig. 4. The analysis of rectal body temperature of P. berghei-infected and treated mice indicated that crude extract of A. aspera prevented loss of body temperature at 400 mg/kg dose level on day 8. The control group treated with chloroquine and artemisinin maintained their temperature on day 8.

Effect of aqueous extract of A. aspera shoot on the body temperature of mice infected with P. berghei (NK-65). Mice + AAE = infected mice treated with Achyranthes aspera aqueous extract, Con IU = infected mice untreated, Con CQ = infected mice treated with chloroquine (10 mg/kg), Con ACT = infected mice treated with artemisinin (25 mg/kg), and NC = normal control group. Values with different superscript are significantly different at p < 0.05
Body weight
The effect of extract of A. aspera on the body weight of mice infected with P. berghei, is presented in Fig. 5. Analysis of body weight of P. berghei-infected and treated mice indicated that the negative control showed significant loss in body weight. The extract treated group at dose of 400 mg/kg bwt, showed significant (p < 0.05) increase in body weight of mice.

Effect of aqueous extract of A. aspera on the body weight of mice infected with P. berghei (NK-65). Mice + AAE = infected mice treated with Achyranthes aspera aqueous extract, Con IU = infected mice untreated, Con CQ = infected mice treated with chloroquine (10 mg/kg), Con ACT = infected mice treated with artemisinin (25 mg/kg) and NC = normal control group. Values with different superscript are significantly different at p < 0.05
Discussion
A. aspera is widely used in the traditional medicinal practice in Nigeria. Medicinal plants have been utilized by majority of the world population for primary health care (Angell & Kassier, 1998; Chan, 2003). The result of the Phytochemical screening of A. aspera, revealed the presence of flavonoids, alkaloids, saponins, phenols, and balsam in the crude aqueous extract. The Medicinal values of these chemical substance, have been linked by several reports to antimalarial activity (You-you, Mu-yun & Yu-Ron, 1982; Switch & Jarrilo, 2004; Etim, Adebayo & Ifeanyi, 2019). Alkaloids have been shown to have in vivo anti-malarial activity by blocking protein synthesis in P. falciparum (Liu, Yang, Roberts, Elfords, & Phillipson, 1992). Flavonoids and phenolics, act by various mechanism which include inhibiting the fatty acid biosynthesis (FAS II) of parasite (Girma, Giday, & Mamo, 2015), evaluating the red blood cell oxidation, inhibiting the parasites protection synthesis, and counter acting the oxidative stress induced by malaria (Builders, Wannang, & Aguiyi, 2011). The mechanism of action by which saponins work might be through different effect on cell membrane (Francis, Kerem, Makkar, & Becker, 2002).
The result of the acute toxicity of A. aspera, revealed that there was no mortality observed up to the maximum dose of level of 5000 mg/kg body weights of extracts administered orally. Signs of toxicity were not visible, as no physical and behavioral changes were observed. Thus, 5000 mg/kg of the extracts was found safe. This indicates that the median lethal dose (LD50) of the extract in the experimental mice was beyond 500 mg/kg. The result observed in the acute toxicity studies of A. aspera is in agreement with those previous studies (Sadashiv & Khrishna, 2011). Anti-malarial studies usually employ in vivo animal models for possible pro-drug effect as well as possible interference of immune system in eradication of the pathogens (Fidock et al., 2004).
In the curative test, the crude extract displayed significant (p < 0.05) curative effect against the parasites. The extract reduced parasitemia in a 5-day test. The extract dose range of 200–600 mg/kg was more effective, with the most effective to be 600 mg/kg body weight of extract. The activity of the extract could be attributed to the active components present. These compounds could be in higher concentration in the higher dose level (600 mg/kg) to have exerted the observed anti-plasmodial activity. The anti-malarial activity could also be attributed to the synergistic activity of phytochemicals. Rodents were used as model organisms to study human disease; this is based on the genetic and physiological similarities between species (Fidock et al., 2004). Plasmodium berghei (NK-65) is a lethal rodent malaria parasite; mice infected with parasite die within 7–10 days of infection in normal course of infection (Chandel & Bagai, 2010). The result observed is in agreement with those in the previous study (Hilou et al., 2006; Waako et al., 2005; Zaruwa et al., 2018; Bantie et al., 2014). The curative anti-plasmodial property of A. aspera may also be related to the anti-inflammatory properties (Vijaya, Sankar, & Varatharajan, 2009) and antioxidant property (Priya, Kumar, Karthik, & Rao, 2010).
All the dose level of the extract prolonged survival time of mice, compared to the negative control. This indicated that extract reduced the parasite growth and overall pathological effects of the parasites in mice. The median dose (400 mg/kg) of the extract prolonged survival time beyond 12 days post infection, is regarded as active (Mulisa et al., 2018; Ural et al., 2014).
Rodent malaria causes parasitemia-induced fall of PCV, which occurred approximately 48 h post-infection (Mace et al., 2015); P. berghei-infected mice suffer from anemia because of erythrocytes destruction, either by parasite multiplication or by spleen reticuloendothelial cell action as the presence of many abnormal erythrocytes stimulates the spleen to produce many phagocytes (Lamikanra, 2005). All of these mechanisms are accountable to malaria induced anemia in both mice and humans (Chinchilla, Aharca, & Caobo, 1998). It was noted that crude extract of A. aspera did not avert the reduction of PCV at all dose levels. A. aspera contains saponins which are known to be responsible for hemolytic effects (Yang, Sun, & Fang, 2005).
Body weight is an important factor to monitor the health of an animal. Loss in body weight is frequently the first indicator of the onset of an adverse effect. Plants with an anti-malarial activity are expected to prevent body weight loss in infected mice resulting from rise in parasitemia. The crude extract of A. aspera prevented body weight loss. P. berghei mice showed decrease in metabolism rate before death, which as a result caused decline in internal body temperature. Thus, plant extract with anti-malarial activity must prevent falling in body temperature (Mengiste, Mekonnen, & Urga, 2012). Crude extracts at 400 mg/kg prevented temperature loss, indicating better stability of internal metabolism in the animal. It is expected that an active compound should prevent the rapid temperature dropping (Dascombe & Sidara, 1994). Effect of the extract was comparable to that of chloroquine, revealing a temperature retaining effect.
Conclusion
In conclusion, the extract displayed good anti-malarial activity in the mice model, which could be due to secondary metabolites present. Extract was safe. It also prolonged survival time of the mice, prevented weight loss, and temperature reduction. This promising result from the crude extract could confirm the traditional medicinal claim for the use of the plant against malaria in Nigeria. However, further studies are required to determine the mechanism of action and characterization of its active anti-plasmodial components.
Availability of data and materials
The data and materials are available from the authors.
Abbreviations
- AAE:
-
Achyranthes aspera aqueous extract
- ACT:
-
Artemisinin-based combination therapies
- IU:
-
Infected with P. berghei and untreated
- CQ:
-
Chloroquine
- NC:
-
Normal control
References
Alam, M. T., Karim, M. M., & Khan, S. N. (2009). Antibacterial activity of different organic extracts of Achyranthes aspera ands Cassia alata. Journal of Scientific Research, 1, 393–398.
Alli, Adesokan, A., & Salawu, A. (2016). Antimalarial activity of fraction of aqueous extract of Acacia nilotica. Journal of Intellectual Enthnopharmacology, 15(2), 180–185.
Angell, M., & Kassier, J. (1998). Alternative medicine- the risk untested and unregulated remedies. North England Journal of Medicine, 339, 839–841.
Aung, M. T., Jordi, L., Daniel, M. P., & Francios, H. N. (2017). Combating multi-drug resistant Plasmodium falicparum malaria. FEBS Journal, 284(16), 2569–2578. https://doi.org/10.1111/fbs.14127.
Bantie, L., Assefa, S. S., Tekshamamanof, T., & Engidarra, E. (2014). In vivo anti-malarial activity of the crude leaf extract and solvent fraction of Croton macrostachyus Hoschet (Euohorbiaceae) against Plasmodium berghei in mice. BMC Complementary and Alternative Medicine, 14, 79.
Bloland, P. B., & Organization, W.H (2001). Drug resistance in malaria. Retrieved from D’alessandro, U., & Buthens, H. (2001). History and importance of antimalarial drug resistance. Tropical Medicine and International Health, 6(11), 845–848.
Bohr, B. A., & Kocipal-Abayazan, M. R. (1994). Flavonoids and condemned tannini from leaves of Hawaiian Vaccinlum reticulatum and V. calycinum (Ericaeae). Pacific Science, 48(4), 456–463.
Builders, M., Wannang, N. S., & Aguiyi, J. (2011). Antplasmodial activities of Parkea biglobosa leaves: in vivo and in vitro studies. Annals of Biological Research, 2(4), 8–20.
Burkill, H. M. (1985). The useful plants of West Tropical Africa (Entry for Achyranthes aspera Linn) Alika, (vol. 1, pp. 1–3).
Chan, K. (2003). Some aspects of toxic contaminants in herbal medicine. Chemosphere 52, 1371.
Chandel, S., & Bagai, U. (2010). Antiplasmodial activity of Ajuga bracteosa against Plasmodium berghei BALB/c mice. Indian Journal of Medical Research, 131, 440–444.
Chinchilla, M., Aharca, O., & Caobo, M. B. C. (1998). In vivo model to study the antimalarial capacity of plants extracts. Review in Biological Tropics, 46(1), 35–39.
Dascombe, M. J., & Sidara, J. Y. (1994). The absence of fever in rats malaria is associate with increased turnover of 5-hydroxytripptamine in the brain. In A. S. Milton (Ed.), Temperature regulation, (pp. 47–52). England: Birkhauzer Bassel.
Dikasso, D., Mekonnen, E., & Debella, A. (2006). In vivo antimalarial activity of Hydro alcoholic extract of Asparagus africanus Lam. in mice infected with Plasmodium berghei. Ethiopian Journal of Health and Development, 20, 112–118.
Dunavan, C. P. (2005). Tackling malaria. Scientific American, 293(6), 76–83.
Duncan, B. D. (1957). Multiple range test for correlated and heteroscedastic means. Biometrics, 13, 359–364.
Edwin, S., Edwin, J. E., Deb, L., Jain, H., Dutt, K. R., & Amal, R. A. (2008). Wound healing and antioxidant activity of Achyranthes aspera. Pharmaceutical Biology, 47(10), 973–975.
Etim, E. A., Adebayo, Y. A., & Ifeanyi, O. E. (2019). Effect of Achyranthes aspera leaf extracts on Hematological parameters of Swiss albino mice. World Journal of Public Health, 4(4), 96–101.
Fidock, D. A., Rosenthal, R. J., Croft, S. L., Brun, R., & Nwaka, S. (2004). Antimalarial drug discovery, efficacy models for compounds screening. National Review and Drug Discovery, 3(6), 509–520. https://doi.org/10.1038/nrd1416.
Francis, G., Kerem, Z., Makkar, U. P., & Becker, K. (2002). the biological action of Saponn in Animal System A. Review British Journal of Nutrition, 88, 557–605.
Gilmour, D., & Skyle, A. J. (1951). Westergren and Wintrobe methods of estimating erythrocylic sedimentation rate (ESR) compounds. British Medical Journal, 1, 1496–1497.
Girma, S., Giday, B.E. & Mamo, H. (2015). Effect of crude leaf extract of Osyris quadripartita on P. berghei in Swiss albino mice, Biomed Central Complementrary and Alternative Medicine 15, 184
Halder, K., Bhattacharjee, S., & Safeukui, P. (2018). Drug resistance in Plasmodium. https://doi.org/10.1038/nrmicro.2017.161.
Harbone, J. B. (1973). Phenolic compounds in phytochemical methods. Chapman and Halll London, 33–38.
Harbone, J. B. (1998). Phytochemical method: A guide to modern technique of plant analysis, (pp. 182–190). London: Chapman and Hall.
Hilou, A., Nacoulma, G., & Guiguemede, T. C. (2006). In vivo antimalarial activities of extracts from Amaranthus spinosus and Borhaeva erecta in mice. Journal of Ethnopharmacology, 103, 236–240.
Jeanne, V. K. L., Yaye, D. N., Marie, K. B. A., & Deise, P. M. (2019). Increased frequency of pfdhps A581G mutation in Plasmodium falciparum isolates from Gabonese. HIV-infected individuals. Journal of Malaria Research and Treatment. https://doi.org/10.1155/2019/9523259.
Krishna, P. A., & Kumar, H. (2019). International Journal of Community medicine and Public Health, 6(4), 1760–1767. https://doi.org/10.18203/2394-6040.ijcmph20191418.
Kumar, S. V., Sankar, P., & Varatharajan, R. (2009). Anti-inflammatory activities of roots of Achyranthes aspera. Pharmaceutical Biology, 47(10), 973–975.
Lamikanra, A., Brown, D., Potocnik, A., Casaals-Pascials, C., Langhorne, J., & Roberts, D. (2007). Malarial anemia of mice and men. Journal of Blood, 110, 18-28.
Liu, K. C., Yang, S. I., Roberts, M. F., Elfords, B. L., & Phillipson, J. D. (1992). Antimalarial activity of Artemisinin annua flavonoids from whole plants and cell culture. Plant Cell Reports, 11(12), 637–640.
Mace, K. K., Kimberly, E., Chlawe, V., Katalenich, B. L., Namboli, M., Mubikayi, L. M., … Chikuli, K. (2015). Evaluation of sulphadoxin – pyrimethamine for intermittent preventive treatment of malaria in pregnancy, a retripetive birth outcome study in Mansa. Malaria Journal, 14, 1–11.
Mbugi, E.V., Mutayoba, B.M., Baithazaany, S.T., Malisa, A.L., Nyambo, T.B. & Mshinda, H. (2006). Multiplicity of infections and level of recrudence in Plasmodium falciparum malaria in Mlimba, Tanzania. African Journal of Biotechnology 5(18) 2001.
Mengiste, B., Mekonnen, E., & Urga, K. (2012). In vivo antimalarial activity of Dodonaea angustifolia seed extracts against Plasmodium berghei in mice model. Mumona Ethiopian Journal of Science, 4(1), 47–63.
Mulisa, E., Girma, B. A., Tesima, S., Yohanna, M., Zemene, E., & Amelo, W. (2018). Evaluation of in vivo antimalarial activities of leaves of Moringa olerifera against Plasmodiumberghei in mice. Jundishapur Journal of Natural Pharmaceutical Product, 12(1), eb0426. https://doi.org/10.5812/jjnpp.60426.
NIH (1985). The principles of laboratory animal care, NIH publication no. 85-23 revised. Bethesda: National Institute of Health.
Obadani, B. O., & Ochuko, P. O. (2002). Phyochemical studies and comparative efficacy of crude extracts of some heamoitate plants in Edo and Delta state of Nigeria. Global Journal of Pure and Applied Sciences, 8(2), 203–208.
Owoeye, D. O., Akinyemi, J. O., & Yusuf, O. B. (2018). Decomposition of changes in malaria prevalence amongst under five children in Nigeria. Malaria World Journal, 9(3), 1–6 www.malariaworld.org. ISSN 2214-4374.
Priya, C. I., Kumar, G., Karthik, L., & Rao, K. V. (2010). Antioxidant activity of Achyranthes aspera Linn. Stem Extracts Pharmacology Online, 2, 228–237.
Ryley, J. F., & Peters, W. (1970). The antimalarial activity of some quinolone esters. Annals of Tropical Medicine & Parasitology, 64(2), 209–222.
Sadashiv, P. S., & Khrishna, A. R. (2011). Acute toxicity study for Achyranthes aspera leaves. Journal of Pharmacological Research, 4(7), 2221–2222.
Sasidharani, S., Chen, Y., Saravan, D., Sundram, K., & Yogalatha, L. (2011). Extraction, isolation and characterization of bioactive compounds from plants extracts. African Journal of Traditional Complementary Alternative Medicine, 18, 1–10.
SPSS INC. (2007). SPSS for windows, version 22.0. Chicago: SPSS Inc.
Switch, S., & Jarilla, S. (2004). Herbal medicines of the American Southwest. Tucson Clinical Botany Medicine, 6, 196.
The Organization of Economic Co-operation and Development (OECD) (2008). The OECD guidelines for testing of chemicals 425, acute oral toxicity. France: Available from https://ntp.niehsninh.gov/iecram/suppdoc./feddocs/oecd425.pdf.
Trease, G., & Evans, W. (1989). Pharmacognosy, (11th ed., ). London: Bailliere Tindall.
Ural, I. O., Kayalar, H., Durmuskahya, C., Carus, F., & Ozbilgim, A. (2014). In vivo antimalarial activity of methanol and water extract of Eryngium thorifolim Roiss (Aoiaceae family) against P. berghei in infected mice. Tropical Journal of Pharmaceutical Research, 13(8), 1313–1317.
Vijaya, S., Sankar, P., & Varatharajan, R. (2009). Anti-inflammatory activity of roots of Achyranthea aspera. Pharmaceutical Biology, 47(10), 973–975. https://doi.org/10.138802009.
Waako, P. J., Gumede, B., Smith, P., & Folb, P. I. (2005). The in vitro and in vivo antimalarial activity of Cardiospermum halicacabum L. and Mormordica foerida Schamch. Journal of Ethnopharmacology, 99(1), 137–143. https://doi.org/10.1016/j.jep.2005.02.017.
WHO (2003). Fact sheet, traditional medicine. Geneva: World Health Organization.
World Health Organization (2020). Key facts World Malaria Report 2020.
World Health Organization (2019). World malaria report. Geneva: World Health Organization.
Yakoob, A., Khattak, A.A., NAdeem, M.F., Fatima, H., Mbambo, G., Quatttara, A., Adams, M., Zeeshan, N. & Takala, H.S. (2018). Prevalence of molecular markers of sulfadoxine pyrimehtamine and artemisinin resistance in Plasmodium falciparum from Pakistan. Malaria Journal 2018. https://doi.org/11.86/s12936-018-2720-y.
Yang, Z. G., Sun, H. X., & Fang, W. H. (2005). Hemolytic activities and adjuvant effect of Astragalus membranaceas saponin on the immune response to ovalbimin in mice. Vaccine, 23, 5796–5203.
Yared, D., Mekonnen, Y., & Debella, A. (2012). In vivo antimalarial activity of fractionated extracts of Asparagus africanus in mice infected with Plasmodium berghei. Pharmacology Online, 3, 88–94.
You-You, T., Mu-Yun, Yu-Ron, et al. (1982). Studies on the constituents of Artemisia annua part II. Planta Medica, 44, 143–144.
Zaruwa, M., Madu, J. O., Yusuf, A. A., & Muhammed, A. O. (2018). In vivo antiplasmodial activity of A. aspera and F. thoningii. International Biological Biomedical Journal, 4(1), 48–53 Winter.
Acknowledgements
The authors’ gratefully acknowledge the Department of Biochemistry and Department of Pharmacology University of Jos, for providing the necessary support.
Funding
This work received financial support from the African Center of Excellence in Phytomedicine Research and Development, in Collaboration with World Bank. (ACEPRD/UJ/028). The Funder supported us with scholarship during the cause of the study.
Author information
Authors and Affiliations
Contributions
MM/IL carried out the phytochemical analysis, in vivo anti-plasmodial studies, interpreted the data, and supervised by IL. MM/CL carried out the toxicity studies, supervised by CL. MM was a major contributor to writing the manuscript. All authors’ read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval and consent to participate with number UJ/FPS/F17-00379 was obtained from Ethical Committee of the Department of Pharmacognosy. Experimental protocol was carried out in line with National and International laws and guidelines for care and use of Laboratory animals.
Consent for publication
Not applicable.
Competing interests
All the authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mankilik, M.M., Longdet, I.Y. & Luka, C.D. Evaluation of Achyranthes aspera shoot extract as an alternative therapy for malaria. JoBAZ 82, 14 (2021). https://doi.org/10.1186/s41936-021-00211-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41936-021-00211-4