
Abstract
Background
Currently, Brazil has 26 million people aged ≥ 60 years. Population aging is associated with a higher prevalence of chronic health conditions which, in turn, are associated with functional dependence and the need for institutionalization. The aim of the study was to evaluate the nutritional status of a sample of institutionalized and non-institutionalized older people in the Brazilian city of Bauru and determine whether the institutionalized individuals had more inadequate nutritional status compared to the community dwellers.
Methods
Ninety-five individuals from 10 long-term care homes in Bauru, São Paulo state, and 101 community-dwelling users of three centers for the aged in Bauru, São Paulo state, were assessed. After collection of sociodemographic and clinical data, the evaluation of nutritional status was conducted using body mass index.
Results
Sixty-one (60.4%) non-institutionalized and 51 (53.9%) community dwellers were classified as inadequate (underweight or overweight) based on nutritional status. In the multivariate analysis, an ordinal logistic regression model was adjusted for the variable “nutritional status.” Regarding body mass index, elderly living in the community were 2.9 times more likely to shift from the underweight to overweight category [OR = 2.9, 95%CI 1.0–8.0, P = 0.0477)].
Conclusions
In this study, it was concluded that institutionalization was not associated with poorer nutritional status compared to community dwellers.
Similar content being viewed by others

Background
Population aging is a global phenomenon [1]. In Brazil, there has been a rapid growth in the elderly population [2]. Currently, Brazil has 26 million people aged ≥ 60 years and, according to estimates, this figure will rise to 37 million by 2027 [3].
There are 3549 long-term institutions (LTCI) in Brazil, with 103,000 elderly residents, representing approximately 0.8% of the elderly population [3]. It is unclear whether all Brazilian LTCI have nutrition programs devised by professionals in this area.
Aging is not a homogeneous process since it depends on socioeconomic and health aspects [4, 5]. The Brazilian elderly population has a higher risk of being underweight compared to the younger adult population [6,7,8].
Among the various techniques used for nutritional assessment, body mass index (BMI) is the most used method for tracking changes in nutritional status. Lower mortality risk among adults is associated with an adequate BMI [9,10,11]. BMI is also associated with functional capacity, mobility, maintenance of mental health, as well as morbidity and mortality in older people [1].
Considering the aging population and the prevalence of nutritional problems in this group, it is essential for the health of elderly that nutritional status be assessed to both detect inadequacy and implement early interventions for reducing disability rates [1].
The aim of the present study was to determine the nutritional status of a sample of institutionalized and non-institutionalized elderly.
Methods
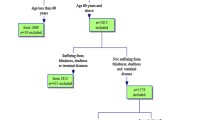
This cross-sectional study was conducted in Bauru, Brazil, between February 1 and June 30, 2016. A total of 196 older people of both genders were evaluated: 95 institutionalized and 101 non-institutionalized (community-dwelling) elderly.
The city of Bauru has 33 long-term care institutions (LTCI), all of which are registered with the National Health Surveillance Agency (ANVISA). The institutionalized individuals assessed were from 10 LTCI in Bauru. The LTCI were randomly selected from the ANVISA list. The community-dwelling elderly were users of private and government-run projects for the elderly in Bauru: the “Open University for the Elderly”, the “Community Center,” and the “Center for the Elderly.”
Of these projects, only Open University for the Elderly is private. On both projects, focus is towards the development of actions for the integration of older people aiming the improvement of quality of life through the insertion and cultural updating as well as availability of knowledge.
All individuals from the LTCI and centers for the elderly were assessed and screened for cognitive impairment using the Mini-Mental State Examination (MMSE) [12]. Having an MMSE score greater than or equal to the value expected for the individual’s formal education level was an inclusion criterion. In the institutionalized group, the elderly had to have resided at the institution for at least 6 months.
The basic evaluation, entailing face-to-face interviews (LTCI and centers for the elderly) and assessment of medical charts (LTCI), collected the following information: instrumental activities of daily living (Lawton’s Scale) [13], falls or hospitalizations in the last 12 months, regular use of prescription medication, engagement in physical activity, number of chronic diseases, and nutritional status (body mass index) [14]. BMI consists of a measure obtained by means of two primary measures, weight (kg) divided by height (m) squared. The nutritional classification adopted for the elderly proposed by Lipschitz (1994) is low weight (< 22.0), eutrophism (≥ 22.0 < 27.0), and overweight (≥ 27.0) [14].
The whole sample signed the Free and Informed Consent Form (FICF) which was approved by the Research Ethics Committee of the Botucatu Medical School, São Paulo State University, UNESP (n°1.356,465) and was interviewed by the same researcher responsible for standardizing interviews. The LTCI approved the conducting of the study by signing a document of approval.
The variable “age” exhibited a normal distribution and was expressed as mean and standard deviation. The categorical variables were expressed as absolute and relative frequency and compared using the chi-square test. Ordinal logistic regression was used for the multivariate analysis. The data were analyzed using the statistical program SPSS (version 22). The significance level adopted was 0.05.
Results
Sixty-one (60.4%) non-institutionalized (GNI) and 51 (53.9%) institutionalized elderly (GI) were classified as having inadequate nutritional status (underweight or overweight). Comparisons of nutritional status between non-institutionalized and institutionalized groups are shown in Table 1.
The mean age of the community-dwelling group was 68.8 (± 7.0) years and of the institutionalized group was 78.9 (± 10.3) years. There was a statistically significant difference between the two groups regarding age (P < 0.001). One hundred and fifty-five (79%) elderly were female and 89.2% had at least one chronic disease; 82.2% were partially or totally dependent for activities of daily living activities and 18.9% were classified as underweight.
Comparisons of the distribution of proportions of the variables between the institutionalized and non-institutionalized groups are shown in Table 2.
There was a statistically significant difference between the two groups for distribution of marital status of the individuals where the proportion of widowed and single individuals was higher among the GNI. There was also a statistically significant difference for falls and hospitalizations in the last year, with higher rates for these variables in the GI. Regarding engagement in physical activities and activities of daily living, the proportion of elderly that routinely participated in physical activities was higher among the GNI, whereas the proportion of elderly with some degree of dependence for activities of daily living was higher in the GI.
The adjusted model for ordinal logistic regression, considering nutritional status as the dependent variable, is shown in Table 3.
In the multivariate analysis, the ordinal logistic regression model (or proportional odds model) was adjusted for the variable “nutritional status.” The reference nutritional status was underweight. The independent variables included in the regression model were age, self-perceived health, instrumental daily life activities, basic daily life activities and quality of life. Regarding body mass index, the elderly living in the community were 2.9 times more likely to shift from the underweight towards the overweight category [OR = 2.9; 95%CI 1.0–8.0, (P = 0.0477)].
Discussion
The aging of the population is irreversible and so there is a need to identify factors that induce healthy aging. Adequate nutrition over the years is one of these factors. Maintaining adequate nutritional status does not necessarily translate to greater survival, but has a positive influence, allowing more people to attain their full life span [11].
Analysis of the rate of mortality due to underweight in Brazil compared with other countries shows that the risk of dying from underweight during old age is 71% higher than in the USA and 32.1% higher than in Costa Rica [1, 15].
In the present study, 28% of the institutionalized elderly population was underweight. In a previous study, the prevalence of underweight in an institutionalized elderly population ranged from 25 to 60% [16]. Another study of 308 elderly individuals from public and private institutions in Pernambuco, Brazil, found that 14.9% were classified as underweight.
In the present study, 50.5% of the non-institutionalized elderly group was overweight. A study of 621 non-institutionalized elderly in the city of Viçosa, Brazil, found a prevalence of overweight of 45%, although there was a tendency for weight decrease with advancing age [2]. The data of the cited study mirrors those of the present study, where the mean age of the non-institutionalized elderly was lower than the institutionalized.
The greater proportion of overweight elderly in the non-institutionalized compared to the institutionalized group was striking since these individuals belonged to groups for the aged in which physical activities are basic components of the programs.
With regard to the institutionalized group, the higher prevalence of underweight may be related to the fact that the institutionalized elderly are older.
Some limitations should be considered in relation to the present study. The categorization of nutritional status, based on body mass index, is not the best option when used alone because it does not reflect the distribution of body fat [17]. Nevertheless, body mass index is the most used instrument in clinical practice since it is easy to perform and has good correlation with morbidity and mortality. The use of body mass index in research and clinical practice is justified provided that specific cut-off points are used for the geriatric age group [18,19,20]. This is a cross-sectional study with a convenience sample, limiting the interpretation of the data found.
Conclusion
In this study, it was concluded that institutionalization was not associated with poorer nutritional status, that is, with inadequate nutritional status (low weight or overweight) when compared to non-institutionalized elderly people through BMI. There is a need for future studies to ascertain why non-institutionalized older adults had more inadequate nutritional status than the institutionalized, and also to evaluate whether this community population involved in institutions for the aged is being well cared for in terms of nutritional status.
Abbreviations
- ANVISA:
-
National Health Surveillance Agency
- BMI:
-
Body mass index
- FICF:
-
Free and Informed Consent Form
- GI:
-
Group of institutionalized elderly
- GNI:
-
Group of non-institutionalized elderly
- LTCI:
-
Long-term care institutions
- MMSE:
-
Mini-mental state examination
- SPSS:
-
Statistical Package for the Social Sciences
- UNESP:
-
São Paulo State University
- USA:
-
United States of America
References
Leite-Cavalcanti C, Rodrigues-Gonçalves MC, Rios-Asciutti LS, Leite-Cavalcanti A. Prevalência de doenças crônicas e estado nutricional em um grupo de idosos brasileiros. Rev Salud Pública. 2009;11(6):865–77.
Nascimento CM, Ribeiro AQ, Cotta RM, Acurcio FA, Peixoto SV, Priore SE, et al. Estado nutricional e fatores associados em idosos do Município de Viçosa, Minas Gerais. Brasil Cad Saúde Pública. 2011;27(12):2409–18.
Instituto Brasileiro de Geografia e Estatística (IBGE). Síntese de indicadores sociais: uma análise das condições de vida da população brasileira [Internet]. Rio de Janeiro: IBGE; 2016 [citado 2018 Fev 20]. Disponível em: https://biblioteca.ibge.gov.br/visualizacao/livros/liv98965.pdf
Ribeiro RL, Tonini KA, Presta FM, Souza VM, Picanco E. Avaliação nutricional de idosos residentes e não residentes em instituições geriátricas no município de Duque de Caxias/ RJ. Rev Eletrônica Novo Enfoque. 2011;12(12):39–46.
Gordilho A, Silvestre J, Ramos LR, Freire MP, Espindola N, Veras R, et al. Desafios a serem enfrentados no terceiro milênio pelo setor saúde na atenção integral ao idoso. Rio de Janeiro: UnATI; 2000.
Spinelli RB. Estudo comparativo do estado nutricional de idosos independentes institucionalizados e não institucionalizados no município de Erechim, RS [Dissertação]. Rio Grande do Sul: Pontifícia Universidade Católica do Rio Grande do Sul; 2008.
Menezes TN, Lopes FJ, Marucci MF. Estudo domiciliar da população idosa de Fortaleza/CE: aspectos metodológicos e características sócio demográficas. Rev Bras Epidemiol. 2007;10(2):168–77.
Marchini JS, Ferriolli E, Moriguti JC. Suporte nutricional no paciente idoso: definição, diagnóstico, avaliação e intervenção. Rev Med Rib Pret. 1998;31(1):54–61.
Anjos LA. Índice de massa corporal (massa corporal.estatura-2) como indicador do estado nutricional de adultos: revisão da literatura. Rev Saúde Públ. 1992;26(6):431–6.
Coelho AK, Fausto MA. Avaliação pelo nutricionista. In: MACIEL A, editor. Avaliação multidisciplinar do paciente geriátrico. Rio de Janeiro: Revinter; 2002.
Campos MA, Pedroso ER, Lamounier JA, Colosimo EA, Arrantes MM. Estado nutricional e fatores associados em idosos. Rev Assoc Med Bras. 2006;52(4):214–21.
Wachholz PA, Rodrigues SC, Yamane R. Estado nutricional e a qualidade de vida em homens idosos vivendo em instituição de longa permanência em Curitiba. PR Rev Bras Geriatr Gerontol. 2011;14(4):625–35.
Brucki SM, Nitrini R, Caramelli P, Bertolucci PH, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuropsiquiatr. 2003;61(3-B):777–81.
Lawton MP, Brody EM. Assessment of older people: self maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3):179–86.
Perracini MR, Flo CM. Funcionalidade e envelhecimento. 2a ed. Rio de Janeiro: Guanabara-Koogan; 2011.
Rauen MS, Moreira EA, Calvo MC, Lobo AS. Avaliação do estado nutricional de idosos institucionalizados. Rev Nutr. 2008;21(3):303–10.
Busnello FM. Aspectos nutricionais no processo do envelhecimento. São Paulo: Atheneu; 2007. p. 3–99.
Nascimento CM, Ribeiro AQ, Cotta RM, Acurcio FA, Peixoto SV, Priore SE, et al. Estado nutricional e fatores associados em idosos do Município de Viçosa, Minas Gerais. Brasil. Cad Saúde Pública. 2011;27(12):2409–18.
Cuppari L. Nutrição clínica no adulto: guia de medicina ambulatorial e hospitalar. 2a ed. UNIFESP/Escola Paulista de Medicina: São Paulo; 2002.
Cervi A, Franceschini SC, Priori SE. Análise crítica do uso de índice de massa corporal para idosos. Rev Nutr. 1998;18(6):765–75.
Acknowledgements
We would like to thank everyone who participated in the survey to further knowledge in this area.
Author information
Authors and Affiliations
Contributions
FNC designed the study, collected data and wrote the manuscript. LVdAS analyzed data and revised the manuscript. AFJ designed the study, analyzed data and wrote the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Nascimento Costa, F., Vaz de Arruda Silveira, L. & Ferrari Jacinto, A. Is living in the community associated with better nutritional status than living in long-term care facilities?. Nutrire 43, 20 (2018). https://doi.org/10.1186/s41110-018-0079-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41110-018-0079-9