
Abstract
Background
Ageing, socioeconomic level, obesity, fertility, relaxed natural selection and urbanization have been postulated as the risk factors of ovarian cancer (OC56). We sought to identify which factor plays the most significant role in predicting OC56 incidence rate worldwide.
Methods
Bivariate correlation analysis was performed to assess the relationships between country-specific estimates of ageing (measured by life expectancy), GDP PPP (Purchasing power parity), obesity prevalence, fertility (indexed by the crude birth rate), opportunity for natural selection (Ibs) and urbanization. Partial correlation was used to compare contribution of different variables. Fisher A-to-Z was used to compare the correlation coefficients. Multiple linear regression (Enter and Stepwise) was conducted to identify significant determinants of OC56 incidence. ANOVA with post hoc Bonferroni analysis was performed to compare differences between the means of OC56 incidence rate and residuals of OC56 standardised on fertility and GDP respectively between the six WHO regions.
Results
Bivariate analyses revealed that OC56 was significantly and strongly correlated to ageing, GDP, obesity, low fertility, Ibs and urbanization. However, partial correlation analysis identified that fertility and ageing were the only variables that had a significant correlation to OC56 incidence when the other five variables were kept statistically constant. Fisher A-to-Z revealed that OC56 had a significantly stronger correlation to low fertility than to ageing. Stepwise linear regression analysis only identified fertility as the significant predictor of OC56. ANOVA showed that, between the six WHO regions, multiple mean differences of OC56 incidence were significant, but all disappeared when the contributing effect of fertility on OC56 incidence rate was removed.
Conclusions
Low fertility may be the most significant determining predictor of OC56 incidence worldwide.
Similar content being viewed by others


Background
Ovarian Cancer (OC56, abbreviated as per the International Classification of Diseases published by the WHO) [1] ranks among the top ten most commonly diagnosed cancers and top five deadliest cancers in most countries [2, 3]. In 2015, OC56 was present in 1.2 million women and resulted in 161,100 deaths worldwide [4] . In the twenty-first century, a woman’s overall lifetime risk of developing OC56 is around 1.6% [2, 5, 6], and her chance of dying of the disease is 1 in 100 [2, 6].
Although OC56 has been known to medical scientists for over 150 years [7], the aetiology of this lethal disease is not well understood. Most research on the aetiology of OC56 has focused on genetic and environmental carcinogenic factors, such as talc, pesticides, red meat and alcohol in diet, smoking, and herbicides. However, to date, none of these factors has been consistently shown to be a major risk factor for the development of OC56 [8]. Alternative hypotheses for the aetiology of the disease have also been suggested. Several studies have suggested that, obese women (those with a body mass index of at least 30 kg/m2) may have a greater risk of developing OC56 because of their elevated levels of circulating estrogen [9,10,11]. An accumulation of somatic mutations has been suggested as the mechanism for the higher incidence of the disease in women over the age of 45 [9]. Urbanization may have improved public hygiene, sanitation and access to health care for women [12], but it has been associated with public health issues, including OC56 [13] due to the changes in occupational, dietary and exercise patterns [6, 12, 14, 15].
Natural selection, as one of the key mechanisms of evolution, differentiates phenotypes’ survival and/or fertility that reflect genetic differences. The Biological State Index (Ibs) has been constructed to measure the opportunity for natural selection through differential mortality at the population level. The Ibs calculation combines life table function dx (number of deaths at age x) with the age-specific completed relative fertility rate sx (fraction of total fertility rate to a woman up to age x): Ibs = 1 – Σdxsx [16,17,18,19,20,21]. Ibs can be used as a way of measuring the opportunity for an individual born into a given population to pass on its genes to the next generation [17, 19, 22,23,24]. Ibs has been postulated to reflect changes in the mutation-selection balance as a result of the effect of improved healthcare on relaxing natural selection and thus measure the magnitude of accumulation of the deleterious genes [16], including those responsible for cancers such as OC56 [17], type 1 diabetes [18] and obesity [18, 19] in human populations.
The association between low fertility and OC56 risk has been well described and it has been postulated that this risk increases in women who have ovulated less over their lifetime either through infertility or administering the combined birth controls, such as contraceptive pills [6, 25,26,27,28,29,30,31,32].
To the best of our knowledge, despite that low fertility is a well-established risk factor for OC56, no research has compared the contributing effects of fertility to OC56 with other OC56 risk factors, such as ageing, Ibs (index of magnitude of OC56 genes accumulation in human populations), obesity and socioeconomic factors (GDP and urbanization).
There is significant variation in the incidence of OC56 between different geographic regions globally [2, 3, 33,34,35]. This phenomenon has also been observed in different populations [6, 13] within the same countries [36, 37]. A number of publications suggest that the disparity between regions and populations is related to socioeconomic level.
In this study, empirical macro-level data have been used to test the hypothesis that fertility (measured by the crude birth rate) is the principal determinant of developing OC56, and that it is fertility, instead of GDP, that is most important factor in shaping the regional variation of OC56 incidence rate.
Methods
Data sources
The following country specific data published by the agencies of the United Nations were analysed for this study.
-
1.
The GLOBOCAN 2012 estimates of incidence rate of female OC56 [34].
GLOBOCAN provides contemporary population level estimates by cancer site and sex [2]. This project is conducted by the WHO research agency, the International Agency for Research on Cancer (IARC).
OC56 incidence rate is expressed as the number per 100,000 females who were diagnosed with OC56 in 2012. The age-standardized OC56 incidence rate was selected in the interest of the data comparability between countries.
-
2.
The World Bank published data on crude birth rate, per capita GDP PPP and urbanization [38]
Crude birth rate (CBR) indicates the number of live births occurring during the year, per 1000 population estimated at midyear. CBR was used to index the fertility in this study over a 20 year period (1992) to reflect long exposure with delayed presentation of OC56. Terms “birth rate” and “fertility” are interchangeable in this paper.
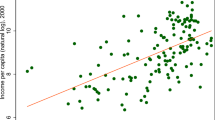
Socio-economic level has been associated with OC56 risk [2, 34, 39, 40]. We chose per capita GDP purchasing power rate (GDP PPP in 2012 international $) because it takes into account the relative cost of local goods, services and inflation rates of the country.
Urbanization has been postulated as a major OC56 predictor [41, 42] because it represents the major demographic shift entailing lifestyle changes [12, 43, 44]. Urbanization is expressed with the country-specific percentage of total population living in urban areas in 2012.
-
3.
The United Nations statistics division estimates of the life expectancy [45]
Country-specific life expectancy, which reflects ageing, has been well established to be correlated with OC56 incidence [46, 47]. Therefore, we selected life expectancy of older people (e65, 2005–2010) [45] to index the ageing process at population level.
-
4.
The magnitude of OC56 gene accumulation in a population indexed with the biological state index (Ibs)
The country specific Ibs was downloaded from the previous publication [19]. It has been postulated that reduced natural selection (measured by Ibs) may have allowed accumulation of deleterious genes of non-communicable diseases [17,18,19], such as OC56 [17].
-
5.
The WHO Global Health Observatory (GHO) data on obesity prevalence
Obese females may be at greater risk of developing OC56 than those who are not obese [48]. The country-specific percentage of the females aged 18+ with a BMI ≥ 30 kg/m2 in 2010 was extracted from the GHO data repository [49].
Data selection
Country specific OC56 incidence rates, ageing, fertility, GDP, Ibs, obesity and urbanization were collated for all countries where data were available. We extracted OC56 incidence rates for 182 countries and then the other variables were matched individually with OC56.
Each country was treated as an individual study subject in the data analysis. Not all the countries (subjects) had information for all the variables.
The relevant United Nations agencies offer free online access to data required for the analyses in this study. No ethics approval was required as there were no individual patients involved in the study.
Data multicollinearity check
In order to avoid the inter-correlation between predictor variables, the multicollinearity statistics were calculated to test the correlations among the variables. Each variable was alternated as the dependent variable, and all the others were considered as the predictor variables in our analysis with the regression model. It was found that the collinearities between variables were not significant since only the tolerance of less than 0.20 and a VIF of more than 5 indicates a multicollinearity problem [50]. Values in our study were more than 0.20 and less than 5 respectively. Details are provided in Additional file 1.
Data analysis
To assess the population level determinants of OC56, the analysis proceeded in five steps.
-
1.
Scatter plots were produced with the original data in Microsoft Excel® to explore and visualize the strength, shape and direction of correlations of OC56 to fertility and GDP respectively.
-
2.
Data were logarithmed to improve their homoscedasticity for linear regression analyses. Bivariate (Pearson’s r and nonparametric Spearman’s rho) correlations were performed to evaluate the direction and strength of the correlations between all the variables of all the subjects and effects possible effects of non-normality of distributions on the strength of moment-product correlations.
-
3.
Partial correlation analysis of Pearson’s moment-product approach was performed. We alternated each of the six variables (ageing, fertility, GDP, Ibs, obesity and urbanization) as the independent predictor when all other five variables were included as the potential confounding factors.
Fisher’s r-to-z transformation was applied to assess the significance level of difference between pairs of correlation coefficients.
-
4.
Standard multiple linear regression (enter) was performed to describe the correlations between the dependent variable (OC56) and the predicting variables. In order to explore if low fertility can partially explain why ageing, GDP, Ibs, obesity and urbanization are correlated with OC56, the enter multiple linear regression was performed to determine the correlations between OC56 incidence and the risk factors in two models: (1) when fertility was incorporated; and (2) excluded as a predicting variable
Subsequently, standard multiple linear regression (Stepwise) was performed to select the predicting variable (s) which have the greatest influence on OC56 in two versions: (1) when fertility was incorporated and (2) excluded as a predicting variable.
-
5.
The equations of the best fitting non-linear trendlines displayed in the scatter plots analysis of relationships between OC56 incidence and fertility (y = 0.006 × 2–0.504× + 14.816, R2 = 0.485) and GDP PPP (y = 0.7167× + 0.2225, R2 = 0.2571) were used to calculate and remove the contributing effects of GDP PPP on OC56 incidence rate respectively by using regressions of OC56 residuals around fertility and GDP PPP. This allowed us to create two new dependent variables, “Residual of OC56 standardised on fertility” and “Residual of OC56 standardised on GDP PPP”
Means of the OC56 incidence rate, the “Residuals of OC56 standardised on fertility” and “Residuals of OC56 standardised on GDP PPP” of all the countries were calculated for mean difference comparisons.
Analysis of variance (ANOVA) was conducted to detect the significant differences among the means of OC56 incidence rate, “Residual of OC56 standardised on fertility” and “Residual of OC56 standardised on GDP PPP” between the six WHO regions [51]. Further post-hoc (Bonferroni) tests were performed to identify the source (pairs) of significant differences.
Bivariate correlations, multiple linear regression analysis (Enter and Stepwise) and ANOVA were conducted with SPSS v. 24. The raw data were used for calculation of mean OC56 incidence rate and “Residual of OC56 standardised on fertility” and “Residual of OC56 standardised on GDP PPP”. The significance was kept at the 0.05 level, but 0.01 and 0.001 levels were also reported. Standard multiple linear regression analysis criteria were set at probability of F to enter ≤0.05 and probability of F to remove ≥0.10.
Results
The relationship identified in the scatterplots between fertility and OC56 was noted to be polynomial with a strong, but inverse (negative) correlation (R2 = 0.485, p < 0.001, n = 179, Fig. 1).

The relationship between fertility and ovarian cancer incidence rate
The strong relationship between fertility and OC56 identified in the scatterplots was confirmed by the subsequent nonparametric and Pearson r analyses based on the log-transformed data.
Globally, fertility was significantly and negatively correlated to OC56 incidence (r = − 0.632 and rho = − 0.655, p < 0.001 respectively in Pearson and non-parametric analyses) (Table 1).
It is also found that ageing, GDP, Ibs, obesity and urbanization had strong and significant correlations to OC56 incidence in both Pearson and non-parametric analyses respectively (Table 1).
The relationship between OC56 and each independent variable (ageing, fertility, GDP, Ibs, obesity and urbanization) was tested by keeping the other five variables statistically constant in partial correlation analysis. Fertility was the only predictor showing a substantial significant correlation (r = − 0.448, p < 0.001) with OC56 independent of the other five variables (Table 2). Ageing showed significant, but weak correlation to OC56 (r = − 0.178, p < 0.05). The Fisher r-to-z transformation revealed that OC56 was in significant stronger correlation with fertility than with ageing (z = 2.68, p < 0.01). GDP, Ibs, obesity and urbanization showed significant correlation to OC56 in the bivariate correlation analyses respectively. However, none of these variables showed a significant correlation with OC56 independent of the other five predictors. This indicates that fertility is the only significant predictor of OC56 independent of the secondary association between OC56 incidence and Ibs (magnitude of OC56 accumulation) and environmental factors (ageing, fertility, GDP, obesity and urbanization).
Standard multiple linear regression (enter) analysis was applied to predict OC56 incidence when ageing, fertility, GDP, obesity and urbanization were included as the independent predicting variables.
When fertility was excluded as one of the independent variables, GDP PPP (β = 0.471, p < 0.001) and Ibs (β = 0.250, p < 0.05) were the two significant variables related to OC56 incidence. However, when fertility was included as an independent predictor, only the correlation between fertility and OC56 incidence was strong and significant. None of the other five predictors showed strong and significant correlation to OC56 (Table 3). Similarly, in a stepwise linear regression model, when fertility was not included as one of the independent predictors, GDP and Ibs were selected as the variables having the greatest influence on the development of OC56. However, when fertility was included together with the other five independent variables, only fertility was selected as the most influential predictor of OC56 with the R2 increase from 0.278 to 0.434. This suggested that GDP and Ibs did not appear to account for the major part of the impact on OC56 incidence. This finding supports our previous suggestion that fertility is the significant predictor of OC56 incidence in partial correlation analysis.
Table 4 showed that the mean OC56 incidence rate was lowest in Africa (4.19) and highest in Europe (8.70). The means of OC56 in the other four regions were 5.89 (Americas), 5.19 (Eastern Mediterranean), 5.90 (South East Asia) and 6.63 (Western Pacific). A post hoc Bonferroni analysis conducted on the multiple comparisons of means revealed that there were a number of significant differences in mean OC56 incidence rates between different WHO regions (Table 4). Mean of OC56 incidence in Europe was significantly greater than in Africa, Americas, East Mediterranean, South East Asia and West Pacific. Mean of OC56 in Americas was significantly greater than in Africa. The regions with greater means of fertility had lower means of OC56 incidence rates (r = 0.985, p < 0.001, n = 6).
A subsequent ANOVA with post hoc Bonferroni procedure performed on the means of “Residual of OC56 standardised on fertility” in different WHO regions showed there was no significant difference among and between regions (Table 4). Whilst the same procedure was performed on the means of “Residual of OC56 standardised on GDP PPP”, the developed region, Europe still had the significantly higher “Residual of OC56 standardised on GDP PPP” than Africa, Americas and East Mediterranean (Table 4). The results from the post hoc Bonferroni tests conducted on comparisons between the WHO regions suggested that regional variations of OC56 incidence may only reach statistically significant levels if the contributing effect of their respective fertility was included. In other words, except for fertility, the total contribution of the other OC56 risk factors to OC56 incidence may not be sufficient for the difference in mean rates to reach significance level. This result was supported by the findings identified in our previous partial correlation (Table 2) and multiple linear regression analyses (Table 3) that fertility is the critical risk factor for OC56.
Discussion
The worldwide secular trend of increased OC56 incidence may have multiple etiologies, which may act through multiple mechanisms at different magnitudes. By examining the correlations of OC56 with low fertility, ageing, GDP, Ibs, obesity and urbanization respectively, this study has shown that only fertility and aging were correlated with the OC56 incidence significantly, although the latter was not as strongly. Statistically, this may suggest that low fertility was the most significant risk factor for OC56 when compared to ageing, GDP, Ibs, obesity and urbanization. This finding is in agreement with three studies conducted by Hankinson et al. [32], Vachon et al. [31] and Cramer et al. [52] respectively which concluded that fertility is a significantly greater predictor of OC56 risk than other commonly used epidemiological variables.
The relationship between female reproductive performance and gynecological cancers has been known for over 300 years [30, 53]. Previous studies in multiple different populations have shown that nulliparous women have a 30–60% greater risk than parous women [52, 54]. Studies also reported that each additional full-term pregnancy lowers OC56 risk by approximately 15% [54, 55]. The mechanism of the influence of childbearing on reducing OC56 risk may be that full-term pregnancy, post-partum period and sometimes the subsequent lactation involve anovulation, suppress secretion of pituitary gonadotropins, lower levels of oestrogen [56,57,58,59], lessen exposure of the ovaries to chronic inflammation and mutation [60], and reduce proliferation of malignant transformations in the inclusion cysts and clefts which are invaginated and formed in the ovarian epithelium during ovulation [61].
Recent studies suggested that women with greater fertility may receive the protection against developing OC56 because:
-
1)
They may produce more oxytocin [62,63,64,65,66,67,68,69] due to positive interactions between family members, especially those between spouses [64, 65, 70, 71]. Oxytocin may inhibit the progression of human ovarian carcinoma cells [28, 29].
-
2)
They may have less stress due to more positive psychological well-being from greater family size, reduces stress levels. This may make their neuroendocrine and immune systems more efficient to reduce the risk of cancer (developing OC56) [72,73,74,75].
-
3)
They are more likely to seek health service and maintain a healthy lifestyle [76,77,78,79], which may have their developing OC56 diagnosed earlier and removed in time.
This study revealed that low fertility determines the variation of OC56 incidence rate among the WHO regions. This finding contradicts the WHO and IARC’s statement that socioeconomic level is the determinant of regional variation of OC56 incidence rate [2, 6, 34]. This may suggest that the correlation between fertility and socioeconomic status (SES) is spurious – caused by the correlation of both variables (SES and OC56 incidence) to the same one (fertility) [80,81,82].
The strength of this study is that it uses an ecological study approach, different from hitherto used approaches, to demonstrate that low fertility is a significant determinant of OC56 risk.
We need to note several limitations of this study:
-
1)
Each country was considered as a whole subject for the ecological study. The country-specific data included in this study may be different from those collected from individual participants. Therefore, the correlations identified from the data analysis may not hold true for all the individuals to have the risk in OC56 development.
-
2)
There may be some random errors that occurred when the United Nations and its agencies collected and aggregated data at country level. Data from developed countries may be more complete than those from developing countries.
-
3)
There are different categories of OC56, but we could not differentiate them for the correlation analysis due to the unavailability of such data.
Conclusion
Low fertility appears to be a significant and strong determinant of OC56 risk independent of ageing, GDP, Ibs, obesity and urbanization. These findings may be helpful for governments, policy-makers, funders, clinicians and researchers when determining future screening and primary presentation strategies for the disease [32, 83, 84].
Abbreviations
- FAO:
-
The Food and Agriculture Organization of the United Nations
- GDP PPP:
-
Gross domestic product purchasing power parity
- IARC:
-
International Agency for Research on Cancer
- Ibs :
-
Biological State Index
- OC56:
-
Ovarian Cancer
- UN:
-
The United Nations
- WHO:
-
World Health Organization
References
IARC. Cancer. 2017 22 December 2017]; Available from: http://globocan.iarc.fr/Pages/cancer.aspx.
Ferlay J, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–86.
Ferlay J, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–917.
Vos T, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–602.
Seiden MV. In: Longo DL KD, Jameson JL, Fauci AS, Hauser SL, Harrison LJ, editors. Gynecologic malignancies, in principles of internal medicine (18th ed.). New York: McGraw-Hill; 2012.
Reid BM, Permuth JB, Sellers TA. Epidemiology of ovarian cancer: a review. Cancer Biology & Medicine. 2017;14(1):9.
Vargas AN. Natural history of ovarian cancer. ecancermedicalscience. 2014;8:465.
The American Cancer Society. Do we know what causes ovarian Cancer? 2017; Available from: https://www.cancer.org/cancer/ovarian-cancer/causes-risks-prevention/what-causes.html.
Australian Government- Cancer Australia. What are the risk factors for ovarian cancer? 2017; Available from: https://ovarian-cancer.canceraustralia.gov.au/risk-factors.
Rodriguez C, et al. Body mass index, height, and the risk of ovarian cancer mortality in a prospective cohort of postmenopausal women. Cancer Epidemiology and Prevention Biomarkers. 2002;11(9):822–8.
Cauley JA, et al. The epidemiology of serum sex hormones in postmenopausal women. Am J Epidemiol. 1989;129(6):1120–31.
Allender S, et al. Quantification of urbanization in relation to chronic diseases in developing countries: a systematic review. J Urban Health. 2008;85(6):938–51.
Huang Z, et al. Incidence and mortality of gynaecological cancers: secular trends in urban shanghai, China over 40 years. Eur J Cancer. 2016;63:1–10.
Zhang X, Nicosia SV, Bai W. Vitamin D receptor is a novel drug target for ovarian cancer treatment. Curr Cancer Drug Targets. 2006;6(3):229–44.
Jordan SJ, et al. Does smoking increase risk of ovarian cancer? A systematic review. Gynecol Oncol. 2006;103(3):1122–9.
Stephan CN, Henneberg M. Medicine may be reducing the human capacity to survive. Med Hypotheses. 2001;57(5):633–7.
You W, H. M. Cancer incidence increasing globally: The role of relaxed natural selection. Evol Appl. 2017;00:1–13.
You W, Henneberg M. Relaxed natural selection contributes to global obesity increase more in males than in females due to more environmental modifications in female body mass. PloS one. 2018;13(7):e0199594.
Budnik A, Henneberg M. Worldwide increase of obesity is related to the reduced opportunity for natural selection. PLoS One. 2017;12(1):e0170098.
Henneberg M, Piontek J. Biological state index of human groups. Przeglad Anthropologiczny. 1975;XLI:191–201.
Henneberg M. Reproductive possibilities and estimations of the biological dynamics of earlier human populations. J Hum Evol. 1976;5:41–8.
You W, Henneberg M. Type 1 diabetes prevalence increasing globally and regionally: the role of natural selection and life expectancy at birth. BMJ Open Diabetes Research and Care. 2016;4(1):e000161.
You W, et al. Decreasing birth rate determining worldwide incidence and regional variation of female breast Cancer. Advances in Breast Cancer Research. 2018;07(01):1–14.
Staub K, et al. Increasing variability of body mass and health correlates in Swiss conscripts, a possible role of relaxed natural selection? Evol Med Public Health. 2018;2018(1):116–26. (accepted April 23, 2018)
Cancer Research UK. Ovarian cancer risks and causes. [Document] 2016 28/07/2016 13:29 20.08.2016]; Available from: http://www.cancerresearchuk.org.
McLemore MR, et al. Epidemiologic and genetic factors associated with ovarian cancer. Cancer Nurs. 2009;32(4):281.
Fraumeni JF, et al. Cancer mortality among nuns: role of marital status in etiology of neoplastic disease in women. J Natl Cancer Inst. 1969;42(3):455–68.
Imanieh MH, et al. Oxytocin has therapeutic effects on cancer, a hypothesis. Eur J Pharmacol. 2014;741:112–23.
Morita T, et al. Oxytocin inhibits the progression of human ovarian carcinoma cells in vitro and in vivo. Int J Cancer. 2004;109(4):525–32.
Britt K, Short R. The plight of nuns: hazards of nulliparity. Lancet. 2012;379(9834):2322–3.
Vachon CM, et al. Association of parity and ovarian cancer risk by family history of breast or ovarian cancer in a population-based study of postmenopausal women. Epidemiology. 2002;13(1):66–71.
Hankinson SE, et al. A prospective study of reproductive factors and risk of epithelial ovarian cancer. Cancer. 1995;76(2):284–90.
Jayson GC, et al. Ovarian cancer. Lancet. 2014;384(9951):1376–88.
Ferlay, J., et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. 2013 28.05.2016]; Available from: http://globocan.iarc.fr.
Jemal A, et al. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90.
Wei K, et al. Ovary cancer incidence and mortality in China, 2011. Chin J Cancer Res. 2015;27(1):38.
Horner M, et al. National Cancer Institute. Bethesda. MD. 1975-2006;2009
The World Bank Group. World Bank Open Data. 2016 12.07.2016]; Available from: http://data.worldbank.org/.
Ness RB, et al. Racial differences in ovarian cancer risk. J Natl Med Assoc. 2000;92(4):176.
Bertone-Johnson ER. Epidemiology of ovarian cancer: a status report. Lancet. 2005;365(9454):101–2.
Jin F, et al. Incidence trends for cancers of the breast, ovary, and corpus uteri in urban shanghai, 1972–89. Cancer Causes Control. 1993;4(4):355–60.
Lefkowitz ES, Garland CF. Sunlight, vitamin D, and ovarian cancer mortality rates in US women. Int J Epidemiol. 1994;23(6):1133–6.
Moore M, Gould P, Keary BS. Global urbanization and impact on health. Int J Hyg Environ Health. 2003;206(4):269–78.
WHO. Urbanization and health. WHO 2010 2010–12–07 15:20:05 2 November 2016]; Available from: http://www.who.int/bulletin/volumes/88/4/10-010410/en/.
United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects: The 2012 Revision, DVD Edition. 2013.
John EM, et al. Characteristics relating to ovarian cancer risk: collaborative analysis of seven US case-control studies. Epithelial ovarian cancer in black women. J Natl Cancer Inst. 1993;85(2):142–7.
Russo A, et al. Hereditary ovarian cancer. Crit Rev Oncol Hematol. 2009;69(1):28–44.
Engeland A, Tretli S, Bjørge T. Height, body mass index, and ovarian cancer: a follow-up of 1.1 million Norwegian women. J Natl Cancer Inst. 2003;95(16):1244–8.
WHO. Global Health Observatory, the data repository. WHO 2015 [11.26.2015]; Available from: http://www.who.int/gho/database/en/.
O’brien RM. A caution regarding rules of thumb for variance inflation factors. Quality & Quantity. 2007;41(5):673–90.
WHO. Global Health Risks Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva: Geneva: World Health Organization; 2009.
Cramer DW, et al. Determinants of Ovarian Cancer Risk. I. Reproductive Experiences and Family History23. JNCI, Journal of the National Cancer Institute. 1983;71:711.
Ramazzini Ba. De morbis artificum Bernardini Ramazzini diatriba = Diseases of workers: the Latin text of 1713 revised, with translation and notes/by Wilmer Cave Wright. In: Wright WCet, B I, editors. Classics of Medicine Library Special edition/privately printed for the members of the Classics of Medicine Library. ed. Diseases of workers. Birmingham, Alabama: The Classics of Medicine Library; 1983.
Moorman PG, et al. Reproductive factors and ovarian cancer risk in African-American women. Ann Epidemiol. 2016;26(9):654–62.
Adami H-O, et al. Parity, age at first childbirth, and risk of ovarian cancer. Lancet. 1994;344(8932):1250–4.
Riman T, Nilsson S, Persson IR. Review of epidemiological evidence for reproductive and hormonal factors in relation to the risk of epithelial ovarian malignancies. Acta Obstet Gynecol Scand. 2004;83(9):783–95.
Casagrande J, et al. “ Incessant ovulation” and ovarian cancer. Lancet. 1979;314(8135):170–3.
Fathalla M. Incessant ovulation and ovarian cancer–a hypothesis re-visited. Facts, views & vision in ObGyn. 2013;5(4):292.
WHO. Bulletin of the World Health Organization: The breast cancer conundrum, in Bull World Health Organ; 2013. p. 626–7.
Ness RB, et al. Factors related to inflammation of the ovarian epithelium and risk of ovarian cancer. Epidemiology. 2000;11(2):111–7.
Choi J-H, et al. Gonadotropins and ovarian cancer. Endocr Rev. 2007;28(4):440–61.
Kendrick KM. The neurobiology of social bonds. J Neuroendocrinol. 2004;16(12):1007–8.
Weisman O, Zagoory-Sharon O, Feldman R. Oxytocin administration to parent enhances infant physiological and behavioral readiness for social engagement. Biol Psychiatry. 2012;72(12):982–9.
Angeles L. Children and life satisfaction. J Happiness Stud. 2009;11(4):523–38.
Nan H, et al. Psychometric evaluation of the Chinese version of the subjective happiness scale: evidence from the Hong Kong FAMILY cohort. Int J Behav Med. 2014;21(4):646–52.
Carmichael MS, et al. Plasma oxytocin increases in the human sexual response. The Journal of Clinical Endocrinology & Metabolism. 1987;64(1):27–31.
Carmichael MS, et al. Relationships among cardiovascular, muscular, and oxytocin responses during human sexual activity. Arch Sex Behav. 1994;23(1):59–79.
Gordon G Jr, Burch RL, Platek SM. does semen have antidepressant properties? Arch Sex Behav. 2002;31(3):289–93.
Magon N, Kalra S. The orgasmic history of oxytocin: love, lust, and labor. Indian journal of endocrinology and metabolism. 2011;15(Suppl3):S156.
Insel TR, Hulihan TJ. A gender-specific mechanism for pair bonding: oxytocin and partner preference formation in monogamous voles. Behav Neurosci. 1995;109(4):782.
Young LJ, Murphy Young AZ, Hammock EA. Anatomy and neurochemistry of the pair bond. J Comp Neurol. 2005;493(1):51–7.
Antonova L, Mueller CR. Hydrocortisone down-regulates the tumor suppressor gene BRCA1 in mammary cells: a possible molecular link between stress and breast cancer. Genes Chromosomes Cancer. 2008;47(4):341–52.
Cohen S, Rodriguez MS. Pathways linking affective disturbances and physical disorders. Health Psychol. 1995;14(5):374–80.
Diener E, Chan MY. Happy people live longer: subjective well-being contributes to health and longevity. Applied Psychology: Health and Well-Being. 2011;3(1):1–43.
Williams RB, Schneiderman N. Resolved: psychosocial interventions can improve clinical outcomes in organic disease (pro). Psychosom Med. 2002;64:552–7.
Aizer AA, et al. Marital status and survival in patients with cancer. J Clin Oncol. 2013;31(31):3869–76.
Kim Y, et al. Psychological distress among healthy women with family histories of breast cancer: effects of recent life events. Psychooncology. 2005;14(7):555–63.
Peled R, et al. Breast cancer, psychological distress and life events among young women. BMC Cancer. 2008;8:245.
Bai A, et al. A survey of overall life satisfaction and its association with breast diseases in Chinese women. Cancer Med. 2016;5(1):111–9.
Myrskylä M, Kohler H-P, Billari FC. Advances in development reverse fertility declines. Nature. 2009;460(7256):741.
Galor O. The demographic transition: causes and consequences. Cliometrica. 2012;6(1):1–28.
Sinding SW. Population, poverty and economic development. Philosophical Transactions of the Royal Society B: Biological Sciences. 2009;364(1532):3023–30.
Whitaker L. The plight of nuns: hazards of nulliparity. Journal of Family Planning and Reproductive Health Care. 2012;38(2):116.
Kent A. Nuns and contraceptives. Reviews in Obstetrics and Gynecology. 2012;5(3–4):e166.
Acknowledgments
The authors express appreciation to Jacques Ferlay from the International Agency for Research on Cancer of World Health Organization for his assistance in locating and defining the data.
Funding
The authors wish to thank the Mäxi Foundation, Switzerland for supporting this research.
Availability of data and materials
All data for this study are publicly and freely available from the official websites of the United Agencies. Aim of these data use in this study meets the terms and conditions of the relevant UN agencies. There is no need to have the formal permission to use the data for this study. The data sources have been described in the section of “Methods”.
Author information
Authors and Affiliations
Contributions
WY conceived the hypothesis, and IS and MH consolidated the hypothesis. WY and MH conducted data analysis. All authors interpreted the data analysis results. IS and MH provided suggestions for WY to draft the manuscript. All authors reviewed, edited and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This paper does not contain any studies with human participants or animals performed by any of the authors. No ethical approval was required.
All the data supporting our findings in this paper were freely downloaded from the United Nations (UN) agencies’ websites.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
AF 1 Collinearity among the variables. (DOCX 16 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
You, W., Symonds, I. & Henneberg, M. Low fertility may be a significant determinant of ovarian cancer worldwide: an ecological analysis of cross- sectional data from 182 countries. J Ovarian Res 11, 68 (2018). https://doi.org/10.1186/s13048-018-0441-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13048-018-0441-9