
Abstract
Background
Sertoli - Leydig cell tumors (SLCTs) are sex-cord stromal tumors that account less than 0.5 % of primary ovarian neoplasms. They are mostly benign and occur in reproductive age women. Variants with heterologous mesenchymal elements are exceptionaly rare. The usual presentation of SLCTs is with signs of androgen excess as majority of them produce androgens.
Case presentation
We present a case of a SLCT occurring in a 70 year old woman. Her presenting complaint was abdominal distension and pain. She had no signs of androgen or estrogen excess. Transvaginal ultrasound (TVUS) and CT scan showed a multilocular adnexal tumor and level of CA 125 was raised. A complete cytoreduction was achieved with surgical procedure. Histopathological examination revealed moderately differentiated SLCT with retiform areas and owergrowth of heterologous component in form of embrional rhabdomyosarcoma (RMS). She returned 7 months after the surgery with a large abdominal mass, ascites, right- sided hydronephrosis and massive pulmonary embolism. Due to the widespread disease and her poor general condition, she received only palliative care. She died 15 days after the admission. No autopsy was performed.
Conclusions
Due to the rarity of SLCTs, especially those with retiform areas and heterologous elements, their management remains challenging. There is no firm evidence that adjuvant chemotherapy is effective in improving survival in SLCTs with malignant heterologous elements. Further studies with a higher number of cases and a longer follow-up are needed to better predicting the prognosis and determine the role of chemotherapy in such cases.
Similar content being viewed by others


Background
Sertoli – Leydig cell tumors (SLCT) are sex cord-stromal tumors that account for less than 0.5 % of primary ovarian neoplasms [1]. Because of their scarcity SLCT represent a challenge in diagnosis and management.
The vast majority of SLCT (90 %) occur in the reproductive age and the rest before menarche or after menopause [2]. They are usually unilateral and confined to the ovary at the time of diagnosis. Approximately 80 % of SLCT are hormonally active with elevated serum testosterone and androstenedione levels and one third of these tumors is discovered due to the clinical signs and symptoms of excess androgen production (virilization, voice deepening, male pattern baldness, amenorrhea, clitoromegaly) [3]. Occasionaly patients have estrogenic manifestations (menometrorrhagia, postmenopausal bleeding) [4]. Abdominal mass, pain and distension and ascites are the clinical presentations in approximately 50 % of these tumors [5].
According to the WHO classification [6] SLCTs are subdivided into well, moderately and poorly differentiated tumors depending on the degree of tubular differentiation of the Sertoli cell component (with poorly differentiated tumors having the least tubular differentiation). Heterologous mesenchymal or epithelial elements are found in up to 20 % of SLCTs and they occur only in moderately and poorly differentiated tumors or tumors with retiform pattern [7]. The prognosis depends on the patient’s age, stage of the tumor and the degree of differentiation with the presence of heterologous elements or retiform pattern being a bad prognostic feature [1].
We report an extremely rare case of moderately differentiated retiform SLCT with extensive owergrowth of heterologous rhabdomyosarcomatous (RMS) component occurring in a postmenopausal patient.
Case presentation
A 70 – year-old, para 2, was referred to our centre with severe right-sided lower abdominal pain that started a few days prior to her visit. She had gained 4 kg, noticed abdominal distension and occasional dull right-sided lower abdominal pain in the 2 months prior to admission. She was otherwise healthy, without any regular medical therapy. She had two vaginal deliveries and her last period was at the age of 46. She had no significant gynecological history. Speculum examination revealed normal-looking vagina and cervix. Upon bimanual palpation a large, smooth and mobile tumor formation, extending from the top of a normal sized uterus up to the umbilicus, was felt. Transvaginal ultrasound (TVUS) examination showed a large, well-vascularized, pelvic mass with solid and cystic components above the uterus and a small amount of ascites in the pouch of Douglas. Contrast enhanced computed tomography (CT) scan of the abdomen showed a well circumscribed, multilocular, complex tumor formation measuring 19 × 12 × 21 cm that appeared to originate from adnexal area, and a thickened, 15 mm, non-homogenous endometrium. Chest X ray showed no evidence of pulmonary nodules. Laboratory tests showed increased serum level of CA-125 at 135.5 U/ml whereas CA 15–3, CA 19–9, CEA were within the normal range. Serum testosterone levels were not determined as there were no signs of androgen excess and they are not a part of a routine pre-operative evaluation at our clinic. Subsequently, exploratory laparotomy was performed. Right ovary with the tumor was removed and sent for intra-operative frozen section evaluation, which revealed features of ovarian malignancy. Hysterectomy with left salpingo-oopherectomy, appendectomy, omentectomy, peritoneal biopsies, pelvic and para-aortic lymphadenectomy were therefore performed and there was no macroscopic disease remnant at the end of the procedure.
On gross examination the tumor was cystic and solid with extensive areas of necrosis and hemorrhage.
Microscopically, most of the tumor consisted of a high grade spindle cell sarcoma with numerous mitoses, areas of necrosis and focal cells with ample eosinophilic cytoplasm, consistent with rhabdomyoblasts. Immunohistochemically, this component was diffusely positive for desmin and myogenin. At the periphery of this mass the tumor was composed of cords and nests of cells with clear cytoplasm intimately admixed with cells with more abundant eosinophilic cytoplasm; some cystically dilated structures were also present. Immunohistochemically, both types of cells were diffusely positive for inhibin and calretinin. A diagnosis of a Sertoli-Leydig cell tumor with retiform areas and heterologous rhabdomyosarcomatous component overgrowth was rendered. Morphological and immunohistochemical characteristics of the tumor are depicted in Figs. 1a-d and 2a-d.

a Microscopically, the tumor was composed of a Sertoli-Leydig cell and rhabdomyosarcomatous component (x100). b In some areas, dilated cystic structures were present (x100). c Sertoli-Leydig cell component composed of cords and islands of Sertoli cells surrounded by Leydig cells with more abundant eosinophilic cytoplasm (x200). d Sarcomatous component with many larger cells with abundant eosinophilic cytoplasm suggesting rhabdomyoblastic differentiation (x200)

Immunohistochemistrty revealed diffuse strong positivity for inhibin (a) and calretinin (b) in the Sertoli-Leydig cell component and for desmin (c) and myogenin (d) in the sarcomatous component (x200)
The tumor was staged IA and we decided not to administer postoperative chemo- or radiotherapy.
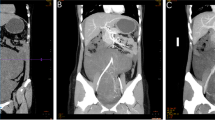
At her first post-operative check up, 8 weeks post procedure, clinical exam and TVUS showed no signs of disease recurrence and the patient was well. She returned to our clinic 7 months after the procedure with abdominal pain, ascites and a large palpable abdominal mass. She lost 5 kg in 1 month and noticed leg swelling 2 weeks before the admission. CT scan showed a large tumor mass extending from the pelvis measuring 21 × 16 × 20 cm (Fig. 3). Additional tumor masses measuring 10 × 15 × 15 cm below the left hemi-diafragm reaching to the spleen and a mass measuring 3 × 4 × 5.6 cm at the splenic hilum were seen. Serum testosterone level was slightly elevated at 1.7 nmol/L. Furthermore, CT scan showed approximately 2 l of ascites and a massive pulmonary embolism with pulmonary infarction and right-sided heart failure. The patient was treated with therapeutic dosage of low-molecular weight heparin and received several blood transfusions. Nephrostomy tube was inserted because of the right-sided hydronephrosis. Due to the widespread of the disease with poor prognosis and patient’s poor general condition, we decided not to perform the surgical procedure. She received paliative care. She died on the fifteenth day after the admission. Her family resigned from an autopsy.

CT scan of recurrent tumor
Discussion
SLCTs are mixed sex cord-stromal tumors composed of variable proportions of Sertoli cells, Leydig cells and in the case of moderately and poorly differentiated neoplasms primitive gonadal stroma and sometimes heterologous elements. When the tumor shows pattern wich can vary from anastomosing, slit-like spaces resembling rete testis to areas of papillary or multicystic pattern with sieve-like spaces, the term retiform SLCT is used. Retiform pattern is found in approximately 15 % of SLCTs [8]. Retiform SLCTs occur at a younger age (mean age 15 years) and mostly present with a large abdominal tumor and pain rather than virilization [9]. Approximately 20 % of SLCT contain heterologous elements [1, 2, 7]. Heterologous elements include epihelial and/or mesenchymal tissue and tumors arising from these tissues (mucinous gastro-intestinal epithelium, hepatocytes, skeletal muscle, cartilage, adipose tissue, mucinous carcinoma, carcinoid, rhabdomiosarcoma, neuroblastoma) [6]. The most common heterologous element is mucinous epithelium of enteric type, others are rare [1, 2]. Five percent of SLCTs contain mesenchymal elements [10]. Both retiform and heterologous elements are only found in moderately and poorly differentiated SLCTs.
Little is known about the pathogenesis of ovarian SLCT however, germ-line mutations in the microRNA processing gene DICER1 have been shown to be related with the development of benign tumors that are susceptible to malignant transformation [11]. These tumors include ovarian SLCT, multinodular goiter, multilocular cystic nephroma and pleuropulmonary blastoma [12–14]. Heravi-Moussavi et al. [12] report a 60 % prevalence of DICER1 mutations in SLCT. Similarly, in the study of Conlon et al. [15] DICER1 mutations were present in 63 % of SLCT. They also report that there is no association between DICER1 mutation and tumor differentiation as mutations in poorly differentiated and moderately differentiated SLCT were found to have similar frequencies. It has been established, that reduced expression of DICER1 is associated with a poor cancer outcome [16]. The exact mechanism underlying tumorigenesis associated with DICER1 mutations remains to be determined, however.
The prognosis of SLCTs is overall favorable and depends on the stage and histological grade of the tumor and the age of the patient. The overall 5- year survival rate for stage I is 95 % and for stages III and IV almost 0 %. Histological grade also correlates with prognosis as a study of 207 cases of SLCTs reported that well-differentiated tumors behaved benign whereas 11 % of moderately differentiated, 19 % of those with heterologous elements and 59 % of poorly differentiated were clinically malignant [1]. The presence of a retiform pattern seems to have an adverse affect on the prognosis, however, the malignant potential of this pattern remains uncertain [9, 17]. Also, the presence of heterologous mesenchymal elements appears to be associated with a poor prognosis [18].
Because SLCTs are very rare, a standardized approach for treatment has not been established yet. Unilateral salpingo-oopherectomy seems to be sufficient in well-differentiated unilateral SLCTs [19]. In cases of moderately and poorly differentiated SLCTs and SLCTs with heterologous elements hysterectomy, bilateral salpingo-oopherectomy and staging (omentectomy, appendectomy and pelvic lymphadenectomy) should be performed [20]. Maximal tumor debulking is recommended for SLCTs with extra-ovarian spread. Adjuvant chemotherapy has been suggested for cases of stage IB to IV, recurrent SLCTs and poorly differentiated SLCTs with heterologous elements [21] however, the value of adjuvant chemotherapy has not yet been determined [22]. Grove et al. [23] suggested that for moderately differentiated SLCTs with heterologous elements, the percentage of sarcoma and its cellular differentiation should be evaluated to decide whether or not to use adjuvant chemotherapy. Their patient had a moderately differentiated SLCT with RMS elements and did not receive postoperative chemotherapy. Despite that, she was disease free 4 years after the procedure. On the other hand, Prat et al. [18] suggested that in cases of SLCTs with mesenchymal elements the prognosis is as poor as in primary ovarian sarcomas and thus adjuvant chemotherapy should be given for all disease stages.
In our case, a moderately differentiated retiform SLCT with retiform areas and overgrowth of the heterologous RMS component occurred in a postmenopausal patient. Two of the previously described cases of moderately differentiated SLCTs with RMS elements occupying only small parts of the tumor had a benign disease course [23, 24]. In contrast, a case where the RMS component almost overgrew the SLCT, had a malignant disease course with recurrence 6 and 10 months post surgical therapy [25]. The recurrent tumor was composed exclusively of RMS elements. Brief summarization of cases of SLCTs containing malignant heterologous mesenchymal elements can be found in Table 1.
Our patient had a FIGO stage IA tumor at the time of the surgical treatment and complete macroscopic cytoreduction was achieved. Despite that, her disease recurred in 7 months confirming the aggressive behavior of SLCT containing RMS and/or retiform elements. We assume that the recurrent tumor was mainly composed of RMS elements due to the aggressive disease course and only slightly elevated serum testosterone levels. The rapid disease progression implies that the presence of RMS and/or retiform component in primary SLCTs causes an unfavorable disease course and that it is the heterologous component in the SLCTs that affects the prognosis and not the grade of the Sertoli – Leydig component itself, as it has already been suggested [1]. However, the incidence of moderately differentiated SLCTs with RMS and SLCTs with retiform component is very low, and we are not able to conclude how these elements truly affect the disease course.
Ovarian RMS is an extremely rare tumor with a very aggressive disease course and poor outcome regardless of treatment [26]. It has been shown that optimal cytoreduction to no gross residual disease improves survival outcome in ovarian sarcomas [27, 28] and that age of the patient and stage of the tumor are associated with overall survival as well [28]. On the other hand, there are no established guidelines whether patients with these tumors should receive postoperative chemotherapy and which regimen would be optimal. Bacalbasa et al. [29] report of a case of primary ovarian RMS where the patient had a disease recurrence 2 months post surgical treatment and died 4.5 months after the second surgical intervention despite receiving adjuvant chemotherapy.
There are no specific guidelines about the follow-up of patients after the surgery for SLCTs. In our case, the patient was followed up as patients with epithelial ovarian cancer. Despite the fact that at her first post-operative check-up, when clinical and TVUS examination were performed, she was disease free, the recurrent tumor 6 months later was widespread and therefore considered as not suitable for surgical treatment. Thus, we believe that imaging examination with a higher specificity and sensitivity should be used for detection of SLCTs recurrence. Recently, positron emission positron emission tomography (PET) combined with computed tomography (CT) has been proposed as an imaging modality for early detection of recurrence of ovarian cancer [30]. Gu et al. [31] reports of a 93 % pooled specificity and 91 % pooled sensitivity of PET CT for detection of recurrence of ovarian cancer. It has not yet been established however, whether it would have similar success detecting SLCT recurrence. Furthermore, there are no guidelines on when to start and how often to use PET-CT in patient follow-up after the treatment.
Conclusion
Management of ovarian SLCTs with malignant disease course is challenging due to the rarity of the disease and lack of experience. It seems that overgrowth of the SLCTs with RMS elements causes a very unfavorable disease course. Further reports of individual cases as well as randomized controlled studies are needed for establishment of management guidelines and the role of adjuvant chemotherapy in these tumors. At present, there is no good evidence that postoperative adjuvant chemotherapy is effective in preventing recurrence of malignant SLCTs. Toxicity and the ability to complete the chemotherapy regimen should be kept in mind when deciding about application of toxic medications.
Abbreviations
CT, comuted tomography; PET, positron emission tomography; RMS, rhabdomyosarcoma; SLCT, Sertoli Leydig cell tumor; TVUS, transvaginal ultrasound
References
Young RH, Scully RE. Ovarian Sertoli-Leydig cell tumors.A clinicopathological analysis of 207 cases. Am J Surg Pathol. 1985;9:543–69.
Roth LM, Anderson MC, Govan AD, Langley FA, Gowing NF, Woodcock AS. Sertoli - Leydig cell tumors a clinicopathologic study of 34 cases. Cancer. 1981;48:187–97.
Osborn RH, Yannone ME. Plasma androgens in the normal and androgenic female: A review. Obstet Gynecol Surv. 1971;26:195–228.
Zhang HY, Zhu JE, Huang W, Zhu J. Clinicopathologic features of ovarian Sertoli-Leydig cell tumors. Int J Clin Exp Pathol. 2014;7:6956–64.
Zanotti KM. The clinical manifestations and diagnosis of Sertoli-Leydig cell tumors of the ovary. CME J Gynecol Oncol. 2002;7:129–33.
Kurman RJ, Carcangiu ML, Herrington S, Zoung RH. WHO classification of tumours of female reproductive organs. Lyon: IARC; 2014.
Roth LM. Recent advances in the pathology and classification of ovarian sex cord-stromal tumors. Int J Gynecol Pathol. 2006;25:199–215.
Wilkinson N, Osborn S, Youngh RH. Sex cord-stromal tumours of the ovary: a review highlighting recent advances. Diagn Histopathol. 2008;14:388–400.
Lou W, Cao D, Yang J, Guo L, Shen K. Retiform Sertoli-Leydig cell tumor of ovary in a 9-year-old girl: case report and review of the literature. Int J Clin Oncol. 2011;16:705–8.
Young RH. Sertoli-Leydig cell tumors of the ovary: Review with emphasis on historical aspects and unusual variants. Int J Gynecol Pathol. 1993;12:141–7.
Bahubeshi A, Tischkowitz M, Foulkes WD. MiRNA processing and human cancer: DICER 1 cuts the mustard. Sci Transl Med. 2011;3:111ps46.
Heravi–Moussavi A, Anglesio MS, Cheng Grace SW, Senz J, Yang W, et al. Recurrent Somatic DICER1 Mutations in Nonepithelial Ovarian Cancers. N Engl J Med. 2012;366:234–42.
Bahubeshi A, Bal N, Rio Frio T, Hamel N, Pouchet C, Yilmaz A, Bouron-Dal Soglio D, Williams GM, Tischkowitz M, Priest JR, Foulkes WD. Germline DICER1 mutations and familial cystic nephroma. J Med Genet. 2010;47:863–6.
Rio Frio T, Bahubeshi A, Kanellopoulou C, Hamel N, Niedziela M, et al. DICER1 mutations in familial multinodular goiter with and without ovarian Sertoli-Leydig cell tumors. JAMA. 2011;305:68–77.
Conlon N, Schultheis AM, Piscuoglio S, Silva A, Guerra E, Tornos C, Reuter VE, Soslow RA, Young RH, Oliva E, Weigelt B. A survey of DICER1 hotspot mutations in ovarian and testicular sex cord-stromal tumors. Mod Pathol. 2015;28:1603–12.
Merritt WM, Lin YG, Han LY, Kamat AA, Spannuth WA, et al. Dicer, Drosha, and outcomes in patients with ovarian cancer. N Engl J Med. 2008;359:2641–50.
Mooney EE, Nogales FF, Bergeron C, Tavassoli FA. Retiform Sertoli-Leydig cell tumours: clinical, morphological and immunohistochemical findings. Histopathology. 2002;41:110–7.
Prat J, Young RH, Scully RE. Ovarian Sertoli- Leydig cell tumors with heterologous elements. II. Cartilage and skeletal muscle: a clinicopathologic analysis of twelve cases. Cancer. 1982;50:465–75.
Bhat RA, Lim YK, Chia YN, Yam KL. Sertoli- Leydig cell tumor of the ovary: analysis of a single institution database. J Obstet Gynaecol Res. 2013;39:305–10.
Gui T, Cao D, Shen K, et al. A clinicopathological analysis of 40 cases of ovarian Sertoli-Leydig cell tumors. Gynecol Oncol. 2012;127:384–9.
Schwartz PE, Price FV, Snyder MK. Management of ovarian stromal tumors. In: Rubin SC, Sutton GR, editors. Ovarian Cancer 2001. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2001. p. 383–98.
McCluggage WG, McKenna M, McBride HA. CD56 is a sensitive and diagnostically useful immunohistochemical marker of ovarian sex cord-stromal tumors. Int J Gynecol Pathol. 2007;26:322–7.
Grove A, Vestergaard V. Ovarian Sertoli-Leydig cell tumor of intermediate grade with heterologous elements of rhabdomyosarcoma. A case report and a review of the literature. Ann Diagn Pathol. 2006;10:288–93.
Kostopoulou E, Talerman A. Ovarian Sertoli-Leydig cell tumor of intermediate differentiation with immature skeletal muscle heterologous elements. Acta Obstet Gynecol Scand. 2003;82:197–8.
Guerard MJ, Ferenczy A. Ovarian Sertoli-Leydig cell tumor with rhabdomyosarcoma: an ultrastructural study. Ultrastruct Pathol. 1982;3:347–58.
George EM, Herzog TJ, Neugut AI, Lu YS, Burke WM, Lewin SN, Hershman DL, Wright JD. Carcinosarcoma of the Ovary: Natural History, Patterns of Treatment, and Outcome. Gynecol Oncol. 2013;131:42–5.
Dai Y, Shen K, Lang JH, Huang HF, Pan LY, Wu M, Yang JX, Zhong DR. Primary sarcoma of the ovary: clinicopathological characteristics, prognostic factors and evaluation of therapy. Chin Med J. 2011;124:1316–21.
Jernigan AM, Fader AN, Nutter B, Rose P, Tseng JH, Escobar PF. Ovarian carcinosarcoma: effects of cytoreductive status and platinum-based chemotherapy on survival. Obstet Gynecol Int. 2013;2013:490508.
Bacalbasa N, Balescu I, Dima S, Popescu I. Ovarian sarcoma carries a poorer prognosis than ovarian epithelial cancer throughout all FIGO stages: a single-center case–control matched study. Anticancer Res. 2014;34:7303–8.
Pan HS, Lee SL, Huang LW, Chen YK. Combined positron emission tomography-computed tomography and tumor markers for detecting recurrent ovarian cancer. Arch Gynecol Obstet. 2011;283:335–41.
Gu P, Pan LL, Wu SQ, Sun L, Huang G. CA 125, PET alone, PET-CT, CT and MRI in diagnosing recurrent ovarian carcinoma: a systematic review and meta-analysis. Eur J Radiol. 2009;71:164–74.
Funding
Not applicable.
Availability of data and materials
Not applicable.
Authors’ contributions
TBP collected clinical and pathological data and drafted the manuscript. SFG performed histopathological analyses, provided photographs, drafted the manuscript and revised the final version of the manuscript. BK supervised the study, provided clinical and surgical information and revised the final version of the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
A written informed consent for publication was obtained from patient’s relatives. All patient data used in the manuscript were anonymized.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Burnik Papler, T., Frković Grazio, S. & Kobal, B. Sertoli - Leydig cell tumor with retiform areas and overgrowth of rhabdomyosarcomatous elements: case report and literature review. J Ovarian Res 9, 46 (2016). https://doi.org/10.1186/s13048-016-0257-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13048-016-0257-4