
Abstract
Background
Increased serum neopterin had been described in older age two decades ago. Neopterin is a biomarker of systemic adaptive immune activation that could be potentially implicated in metabolic syndrome (MetS). Measurements of waist circumference, triglycerides, high-density lipoprotein cholesterol (HDLC), systolic and diastolic blood pressure, glycated hemoglobin as components of MetS definition, and plasma total neopterin concentrations were performed in 594 participants recruited in the European Prospective Investigation into Cancer and Nutrition (EPIC).
Results
Higher total neopterin concentrations were associated with reduced HDLC (9.7 %, p < 0.01 for men and 9.2 %, p < 0.01 for women), whereas no association was observed with the rest of the MetS components as well as with MetS overall (per 10 nmol/L: OR = 1.42, 95 % CI = 0.85-2.39 for men and OR = 1.38, 95 % CI = 0.79-2.43).
Conclusions
These data suggest that high total neopterin concentrations are cross-sectionally associated with reduced HDLC, but not with overall MetS.
Similar content being viewed by others

Background
Neopterin, a biomarker of systemic adaptive immune activation, is synthesized by monocyte-derived macrophages and dendritic cells upon stimulation of interferon-gamma (IFN-γ) and is considered a reliable proxy to assess the rate of IFN-γ production [1–4]. The concentrations of neopterin increase with the dose of interferon, thereby help to monitor the activity of INF-γ inducible inflammation. Thus, the measurement of neopterin concentrations in body fluids provides information about activation of T-helper cell derived systemic adaptive immune activation [5]. As high neopterin is associated with increased production of reactive oxygen species, neopterin can also be regarded as an indicator for oxidative stress due to immune activation [6].
Neopterin has been used clinically in the assessment of bacterial and viral infections, autoimmune diseases, and malignant conditions [7]. Increased blood neopterin concentrations had been described in older age [8, 9] and have been positively related to aging-related chronic disorders, including metabolic syndrome (MetS) [3], cancer, cardio-vascular disease, as well as overall mortality [2–4, 10–13].
An emerging field of research - immunometabolism - recognizes the existence of an interplay between immunity, inflammation, and impaired metabolism [14]. Central to this theory, inflammation and immune activation are involved in the development of obesity, insulin resistance and potentially also in MetS [14–16]. Despite biological plausibility, only a few epidemiological studies have explored the relation between neopterin and selected metabolic factors. In a study of 3946 patients with acute coronary syndrome, higher plasma concentrations of neopterin were associated with older age, a prior history of hypertension or diabetes, lower low-density lipoprotein cholesterol levels, and higher high-sensitivity C-reactive protein (hsCRP) levels [17]. In another study among 592 patients with high prevalence of MetS, plasma neopterin concentrations were correlated, though weakly, with abdominal obesity, high-density lipoprotein cholesterol (HDLC), and insulin resistance [2]. Similarly, a weak correlation between neopterin and abdominal obesity was reported in another patient cohort of 477 middle-aged and older white individuals at high risk for type 2 diabetes and cardiovascular disease [18].
It remains unclear whether the potential association of neopterin with MetS and its components, may be independent of age and markers of chronic inflammation such as hsCRP. Such knowledge may provide important insights into the potential link between immune activation and impaired metabolism. Therefore, the aim of the study was to investigate the association of plasma total neopterin concentrations with MetS and its components in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort.
Results
Overall, the geometric mean of total neopterin concentrations in the study population were 18.74 (standard deviations, SD: 1.50) for men and 18.63 (SD: 1.40) for women. Table 1 shows the characteristics of the study population.
Table 2 presents the Spearman’s partial correlation coefficients of clinical markers of MetS and total neopterin concentrations. Total neopterin was inversely correlated with pyridoxal 5′-phosphate (PLP) and HDLC but positively correlated with hsCRP.
High total neopterin concentrations were associated with lower HDLC, but not with other components of MetS (Table 3). After mutual adjustment, the mean total neopterin concentrations remained different according to HDLC categories (p < 0.01 for both men and women). Figure 1 shows the adjusted means and 95 % CI of total neopterin by increasing number of MetS components. The average differences per component was 4.0 % (P difference = 0.07) for men and 0.8 % (P difference = 0.64) for women.

Adjusted means1 and 95 % confidence intervals of total neopterin by increasing number of metabolic syndrome components2. 1. The means were calculated by exponentiating the natural-log transformed means, which were estimated from multiple linear regression and adjusted for age at blood collection (years), sex, education (none or primary school completed, technical or professional school, secondary school, above secondary school, and not specified), smoking status (never, former, current, and unknown), and physical activity (low, medium, high, very high, missing). 2. The markers were considered abnormal when waist circumference ≥94 cm in men and ≥88 in women; triglycerides ≥1.7 mmol/L; high-density lipoprotein cholesterol <1.03 in men, <1.29 mmol/L in women; systolic blood pressure ≥130 or diastolic ≥85 mmHg; and HbA1c ≥5.7 % or self-reported ever physician diagnosed diabetes
In our study, increased total neopterin was associated with reduced HDLC (OR per 10 nmol/L = 2.22, 95 % CI = 1.24-3.97 for men and OR per 10 nmol/L = 2.82, 95 % CI = 1.68-4.73 for women), and these associations were independent of PLP (Table 4). Further adjustment for hsCRP did not change the results (OR per 10 nmol/L = 2.14, 95 % CI = 1.17-3.91 for men and OR per 10 nmol/L = 2.70, 95 % CI = 1.58-4.61, data not shown). Increased plasma total neopterin was not associated with overall MetS, defined as presence of any three of the MetS components (OR per 10 nmol/L = 1.42, 95 % CI = 0.85-2.39 for men and OR per 10 nmol/L = 1.38, 95 % CI = 0.79-2.43 for women).
Discussion
In this study, high total neopterin concentrations were associated with reduced HDLC, but not with overall MetS. These data indicate that immune activation may be related to lipid changes; however, the cross-sectional nature of the study does not provide sufficient information for interpreting the direction of these relations.
Previously only three studies investigated the association of neopterin concentrations with clinical markers of MetS; however, these studies were conducted in participants with underlying diseases, including cardiovascular disease, type 2 diabetes and MetS [2, 18, 19]. In agreement with the study of Oxengrug et al. 2011 [2], we observed an inverse association of total neopterin with HDLC.
Our data suggest an inverse association of total neopterin with HDLC, as well as low-density lipoprotein cholesterol and total cholesterol. This association was independent of age, sex, EPIC study center and smoking status as well as PLP and hsCRP levels. Similar findings have been reported, in patients with HIV infection [20], cardiovascular diseases [4] and MetS [2]. HDLC helps to remove excess cholesterol from peripheral tissue and transport it to the liver for excretion. The functions of HDL include anti-inflammatory and anti-oxidant activities [21]. If the function is impaired, cholesterol accumulates in peripheral tissue and causes inflammation and atherosclerosis. Despite the concept of HDL dysfunction evolved over the last decades, little is known on factors that underline possible alterations between functional and dysfunctional HDL. Recently, immunity was suggested as one of the main pathophysiological pathways of HDLC functionality via modulating cholesterol content in immune cells [22]. It has been shown that inhibition of cholesterol efflux mechanisms in macrophages promotes an inflammatory phenotype in these cells [23]. The raised neopterin levels may indicate activated immune response in individuals with low HDL cholesterol levels. Neopterin had been associated with cardiovascular events [4, 24, 25], suggesting a potential involvement of adaptive immunity and inflammation in modulating the association between cholesterol metabolism and cardio-metabolic risk. From a practical perspective, measurement of neopterin in addition to HDLC may aid in identifying HDL anti-inflammatory/proinflammatory function and could likely yield important additional information beyond that available from simple measurement of HDLC in an individual. However, future studies are needed in order to evaluate potential practical implication of these findings. Of note, despite the association with HDLC, we observed no association with previous diagnosis of hyperlipidemia (data not shown). This can be partly explained by the observation that total neopterin concentrations were lower in those who used lipid-lowering drugs [4].
Previous studies have reported positive associations between neopterin and waist circumference [2, 10, 18, 26, 27]. In one of these; however, such association disappeared after adjustment for other metabolic biomarkers [18]. Thewissen et al. (2011) reported that the association between abdominal fat and neopterin - considered a marker of adaptive immune activation - was mediated, by elevations in hsCRP and other immune activation markers [18]. They hypothesized that it is not merely an increased mass of adipose tissue that directly leads to attenuation of insulin action, but rather adipose tissue inflammation mediated by activated immune system in obese individuals that leads to insulin resistance. In our study, we only observed a non-statistically significant marginal association between abdominal obesity and total neopterin concentrations. Further prospective studies are needed to test this hypothesis.
Similarly to a previous report [4], we found no association between total neopterin concentrations and triglycerides (TG). There was no association between total neopterin concentrations and measured systolic or diastolic blood pressure (BP), including pre-defined cutoffs for hypertension. There have been reports suggesting that neopterin could be a predictive marker for cardiovascular events [4, 19, 24, 25, 28–31], including an elevated diastolic BP [29, 32]. However, its associations with hypertension (or BP) have been inconsistent across studies. In this context, our results might suggest that although hypertension is an important component of cardiovascular diseases, it might not be directly associated with inflammation or IFN-γ mediated inflammation.
Previous studies have also reported that neopterin concentrations were positively associated with glucose concentrations [10]. However, we did not observe an association between total neopterin concentrations and diabetes, either using the glycated haemoglobin (HbA1C), a marker of long-term blood glucose levels, or with self-reported diabetes. Similar findings have been obtained in a small saline-controlled crossover study on six healthy men (mean age 22 years) for IFN-γ [33].
Limitations of the present study have to be taken into account. First, the mean and median concentrations of total neopterin in this study population was somewhat higher than previously reported [2, 27]. An explanation is that our assay measures total neopterin, which is the sum of 7,8-dihydroneopterin and neopterin, in contrast to ELISA method which measures only neopterin. Nevertheless, both neopterin and total neopterin reflect inflammation and the associations between total neopterin and hsCRP, as well as the other metabolic biomarkers were comparable with previous reports (9). In addition, in our data no unexpected correlations between neopterin and basic characteristics were observed, as well as main findings were also in line with the previous reports. Secondly, the study population included controls of a nested case–control study; therefore, it may not be representative of the general population. However, when compared to the overall EPIC population, we have not seen major differences according to baseline characteristics, except for that our study population was slightly older, included a higher proportion of men, and a higher proportion of smokers. The range of the concentration of total neopterin reported here may not be fully representative of the general population. Thirdly, the relation between total neopterin and MetS components was assessed within the context of a cross-sectional study design, which does not allow inference about the direction of the associations. Finally, about 70 % of the study participants provided non-fasting blood samples, which may have affected the TG levels; however, we have been accounting for fasting status and found essentially the same results after excluding non-fasting participants.
Conclusions
In conclusion, high total neopterin concentrations are associated with reduced HDLC, but not with overall MetS. These data support the emerging knowledge on the interplay of immune response and cholesterol metabolism. Future studies are warranted to better understand the potential role of these interrelations in chronic disease development.
Methods
Study population
The design of the EPIC cohort has been described previously [34]. In brief, EPIC recruited 518,408 volunteers from 23 centers in 10 countries (Sweden, Denmark, Norway, the Netherlands, United Kingdom, France, Germany, Spain, Italy, and Greece) between 1992 and 2000. The eligibility criteria for participation was primarily decided within each cohort. In general, apparently healthy, middle-aged subjects who agreed to participate in the study and to have their health status followed up for the rest of their lives, were recruited. The questionnaires were completed and the blood samples were taken at recruitment.
Assessment of anthropometry and lifestyle data
The lifestyle questionnaires, which were completed by participants, included questions on diet, education, occupation, previous illnesses, alcohol, tobacco consumption, and physical activity. Informed consent forms were filled at each local center and the study was approved by the Institutional Review Board at the International Agency for Research on Cancer (IARC) and the local ethics committees. Waist circumference was measured either at the narrowest torso circumference or at the midpoint between the lower ribs and iliac crest. Systolic BP and diastolic BP were measured by trained personnel. Two readings were performed on the right arm in a sitting position (spaced by 1–5 minutes) by use of a standard mercury manometer or oscillometric device. To avoid any possible white coat effect, we used the second reading, and when unavailable, the first reading.
Definition of MetS
The definition of MetS and its components have been described previously [35]. In general, we followed the harmonized definition published by Alberti et al. in 2009 [36] with slight modification in determining abnormal glucose metabolism. Briefly, MetS was defined as having any three of the following five components: 1) abdominal obesity, i.e. waist circumference is greater than or equal to 94 cm in men or 80 cm in women; 2) elevated TG, i.e. greater than or equal to 1.7 mmol/L, after correction for the fasting status of the study subjects; that is, subtracting the sex-specific geometric mean difference between non-fasting and fasting subjects from the individual levels of non-fasting subjects; 3) reduced HDLC, i.e. less than 1.03 mmol/L in men and 1.29 mmol/L in women; 4) elevated BP, i.e. systolic BP 130 mmHg or more or diastolic BP 85 mmHg or more or self-reported physician diagnosed hypertension; and 5) abnormal glucose metabolism, i.e. self-reported physician diagnosed diabetes status or HbA1c of 5.7 %, which corresponds to fasting plasma glucose levels of 100 mg/dL .
Laboratory assays
Plasma concentration of total neopterin (7,8-dihydroneopterin + neopterin) and PLP was determined by liquid chromatography-tandem mass spectrometry (LC-MS/MS) [37] at Bevital A/S (http://www.bevital.no), Bergen, Norway. Serum hsCRP was measured by a high-sensitivity assay (Beckman-Coulter, Woerden, the Netherlands), and the HDLC and TG concentrations by a colorimetric method, on a Synchron LX-20 Pro autoanalyzer (Beckman-Coulter, [38]). Measurements of HbA1c in erythrocyte hemolysate were carried out using high-performance liquid chromatography with a Bio-Rad Variant II instrument (Bio-Rad Laboratories, Hercules, California) [39]. The within and between day coefficients of variance (CV) were 3-10 % for total neopterin and PLP [37]. The inter-assay CV were 6.0 % and 6.5 % at CRP concentrations of 1.16 and 1.89 mg/L, respectively, 4.1 %, 3.4 %, and 3.6 % at HDLC concentrations of 0.62, 1.20, and 1.65 mmol/L, respectively, and 3.3 %, 2.1 %, and 2.0 % at TG concentrations at 86.6, 165.9, and 227.0 mg/dL, respectively. The intra-batch CV was 2.5 % for HbA1c [39].
Statistical analysis
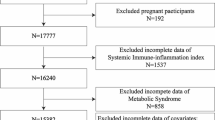
The current analysis is based on 845 subjects (375 men and 470 women) who served as controls in matched case–control studies of colorectal cancer nested within the EPIC. The original aims of the nested case–control studies were to explore the risk of colon and rectal cancer in relation to MetS [35] and one-carbon metabolism biomarkers [40, 41]. MetS component measurements were not available subjects from Norway and Malmo center of Sweden. We further excluded 207 subjects who received treatment or the treatment information were missing for hyperlipidemia (n = 94), hypertension (n = 175), or diabetes (n = 15). Additional 44 subjects were excluded because their total neopterin measurements were not available. The final sample size for the analysis was 594.
The correlation between total neopterin and components were examined by Spearman’s partial correlation coefficients (r), adjusted for age, sex, country, and smoking status. Adjusted means for total neopterin according to tertiles of each MetS component were calculated using multiple linear regression models. Because the range of the middle category of TG is narrow, we categorized TG at 1.7 and 3.4 mmol/L. The dependent variable, total neopterin concentrations, was natural log-transformed and the normality assumption was tested by graphic examination of the residual distribution. The models were adjusted for age at blood collection (years), sex, country, education (none or primary school completed, technical or professional school, secondary school, above secondary school, and not specified), smoking status (never, former, current, and unknown), and physical activity (low, medium, high, very high, and missing). The adjusted means were also assessed by mutual adjustment for the other MetS components as well as PLP, due to its role in INF-γ stimulated inflammatory responses [2, 27] and hsCRP, due to its association with low-grade inflammation. The adjusted means were then back-transformed by exponentiating the natural-log transformed means from the model. The associations between total neopterin and pre-defined cutoffs of each component of MetS and the composite MetS were also examined by calculating odds ratios (OR) and 95 % confidence intervals (CI) in logistic regression analysis, adjusted for age at blood collection (years), sex, country, education (none or primary school completed, technical or professional school, secondary school, above secondary school, and not specified), smoking status (never, former, current, and unknown), and physical activity (low, medium, high, very high, missing). Total neopterin was modeled in three categories according to sex-specific tertiles. Tests for trend were performed by modelling the median values of each category as a continuous variable. Subgroup analyses were performed by age (<55, 50–65, and ≥65 years old), sex, and body mass index (BMI, <30 and ≥30 kg/m2).
Analyses were performed using SAS 9.3. All tests were two sided and statistical significance was assessed at the level of 0.05.
Abbreviations
- AGM: BP:
-
blood pressure
- CI:
-
confidence interval
- CV:
-
coefficients of variance
- EPIC:
-
European Prospective Investigation into Cancer and Nutrition
- HbA1c:
-
glycated haemoglobin
- HDLC:
-
high-density lipoprotein cholesterol
- hsCRP:
-
high-sensitivity C-reactive protein
- IFN-γ:
-
Interferon-gamma
- MetS:
-
metabolic syndrome
- OR:
-
odds ratio
- PLP:
-
pyridoxal 5′-phosphate
- TG:
-
Triglycerides
Reference
Sucher R, Schroecksnadel K, Weiss G, Margreiter R, Fuchs D, Brandacher G. Neopterin, a prognostic marker in human malignancies. Cancer Lett. 2010;287:13–22.
Oxenkrug G, Tucker KL, Requintina P, Summergrad P. Neopterin, a marker of interferon-gamma-inducible inflammation, correlates with pyridoxal-5'-phosphate, waist circumference, hdl-cholesterol, insulin resistance and mortality risk in adult boston community dwellers of Puerto Rican origin. Am J Neuroprot Neuroregen. 2011;3:48–52.
Oxenkrug GF. Interferon-gamma-inducible kynurenines/pteridines inflammation cascade: implications for aging and aging-associated psychiatric and medical disorders. J Neural Transm. 2011;118:75–85.
Grammer TB, Fuchs D, Boehm BO, Winkelmann BR, Maerz W. Neopterin as a predictor of total and cardiovascular mortality in individuals undergoing angiography in the Ludwigshafen risk and cardiovascular health study. Clin Chem. 2009;55:1135–46.
Murr C, Widner B, Wirleitner B, Fuchs D. Neopterin as a marker for immune system activation. Curr Drug Metab. 2002;3:175–87.
Weiss G, Widner B, Zoller H, Schobersberger W, Fuchs D. Immune response and iron metabolism. Br J Anaesth. 1998;81 Suppl 1:6–9.
Hoffmann G, Wirleitner B, Fuchs D. Potential role of immune system activation-associated production of neopterin derivatives in humans. Inflamm Res. 2003;52:313–21.
Oxenkrug G. Interferon-gamma - inducible inflammation: contribution to aging and aging-associated psychiatric disorders. Aging Dis. 2011;2:474–86.
Capuron L, Geisler S, Kurz K, Leblhuber F, Sperner-Unterweger B, Fuchs D. Activated immune system and inflammation in healthy ageing: relevance for tryptophan and neopterin metabolism. Curr Pharm Des. 2014;20:6048–57.
Ledochowski M, Murr C, Widner B, Fuchs D. Association between insulin resistance, body mass and neopterin concentrations. Clin Chim Acta. 1999;282:115–23.
Spencer ME, Jain A, Matteini A, Beamer BA, Wang NY, Leng SX, et al. Serum levels of the immune activation marker neopterin change with age and gender and are modified by race, BMI, and percentage of body fat. J Gerontol A Biol Sci Med Sci. 2010;65:858–65.
Oxenkrug GF. Metabolic syndrome, age-associated neuroendocrine disorders, and dysregulation of tryptophan-kynurenine metabolism. Ann N Y Acad Sci. 2010;1199:1–14.
Avanzas P, Arroyo-Espliguero R, Kaski JC. Neopterin and cardiovascular disease: growing evidence for a role in patient risk stratification. Clin Chem. 2009;55:1056–7.
Mathis D, Shoelson SE. Immunometabolism: an emerging frontier. Nat Rev Immunol. 2011;11:81.
Odegaard JI, Chawla A. The immune system as a sensor of the metabolic state. Immunity. 2013;38:644–54.
Osborn O, Olefsky JM. The cellular and signaling networks linking the immune system and metabolism in disease. Nat Med. 2012;18:363–74.
Ray KK, Morrow DA, Sabatine MS, Shui A, Rifai N, Cannon CP, et al. Long-term prognostic value of neopterin: a novel marker of monocyte activation in patients with acute coronary syndrome. Circulation. 2007;115:3071–8.
Thewissen MM, Damoiseaux JG, Duijvestijn AM, van Greevenbroek MM, van der Kallen CJ, Feskens EJ, et al. Abdominal fat mass is associated with adaptive immune activation: the CODAM Study. Obesity (Silver Spring). 2011;19:1690–8.
Kaski JC, Consuegra-Sanchez L, Fernandez-Berges DJ, Cruz-Fernandez JM, Garcia-Moll X, Marrugat J, et al. Elevated serum neopterin levels and adverse cardiac events at 6 months follow-up in Mediterranean patients with non-ST-segment elevation acute coronary syndrome. Atherosclerosis. 2008;201:176–83.
Zangerle R, Sarcletti M, Gallati H, Reibnegger G, Wachter H, Fuchs D. Decreased plasma concentrations of HDL cholesterol in HIV-infected individuals are associated with immune activation. J Acquir Immune Defic Syndr. 1994;7:1149–56.
Eren E, Yilmaz N, Aydin O. High density lipoprotein and it's dysfunction. Open Biochem J. 2012;6:78–93.
Norata GD, Pirillo A, Ammirati E, Catapano AL. Emerging role of high density lipoproteins as a player in the immune system. Atherosclerosis. 2012;220:11–21.
Holven KB, Retterstol K, Ueland T, Ulven SM, Nenseter MS, Sandvik M, et al. Subjects with low plasma HDL cholesterol levels are characterized by an inflammatory and oxidative phenotype. PLoS One. 2013;8, e78241.
Garcia-Moll X, Cole D, Zouridakis E, Kaski JC. Increased serum neopterin: a marker of coronary artery disease activity in women. Heart. 2000;83:346–50.
Sulo G, Vollset SE, Nygard O, Midttun O, Ueland PM, Eussen SJ, et al. Neopterin and kynurenine-tryptophan ratio as predictors of coronary events in older adults, the Hordaland Health Study. Int J Cardiol. 2013;168(2):1435–40.
Ursavas A, Karadag M, Oral AY, Demirdogen E, Oral HB, Ege E. Association between serum neopterin, obesity and daytime sleepiness in patients with obstructive sleep apnea. Respir Med. 2008;102:1193–7.
Theofylaktopoulou D, Midttun O, Ulvik A, Ueland PM, Tell GS, Vollset SE, et al. A community-based study on determinants of circulating markers of cellular immune activation and kynurenines: the Hordaland Health Study. Clin Exp Immunol. 2013;173:121–30.
van Haelst PL, Liem A, van Boven AJ, Veeger NJ, van Veldhuisen DJ, Tervaert JW, et al. Usefulness of elevated neopterin and C-reactive protein levels in predicting cardiovascular events in patients with non-Q-wave myocardial infarction. Am J Cardiol. 2003;92:1201–3.
Avanzas P, Arroyo-Espliguero R, Cosin-Sales J, Quiles J, Zouridakis E, Kaski JC. Prognostic value of neopterin levels in treated patients with hypertension and chest pain but without obstructive coronary artery disease. Am J Cardiol. 2004;93:627–9.
Avanzas P, Arroyo-Espliguero R, Quiles J, Roy D, Kaski JC. Elevated serum neopterin predicts future adverse cardiac events in patients with chronic stable angina pectoris. Eur Heart J. 2005;26:457–63.
Pacileo M, Cirillo P, De RS, Ucci G, Petrillo G, Musto DS, et al. The role of neopterin in cardiovascular disease. Monaldi Arch Chest Dis. 2007;68:68–73.
Schennach H, Murr C, Gachter E, Mayersbach P, Schonitzer D, Fuchs D. Factors influencing serum neopterin concentrations in a population of blood donors. Clin Chem. 2002;48:643–5.
de Metz J, Sprangers F, Endert E, Ackermans MT, ten Berge IJ, Sauerwein HP, et al. Interferon-gamma has immunomodulatory effects with minor endocrine and metabolic effects in humans. J Appl Physiol. 1999;86:517–22.
Riboli E, Hunt KJ, Slimani N, Ferrari P, Norat T, Fahey M, et al. European Prospective Investigation into Cancer and Nutrition (EPIC): study populations and data collection. Public Health Nutr. 2002;5:1113–24.
Aleksandrova K, Boeing H, Jenab M, Bas Bueno-de-Mesquita H, Jansen E, van Duijnhoven FJ, et al. Metabolic syndrome and risks of colon and rectal cancer: the European prospective investigation into cancer and nutrition study. Cancer Prev Res (Phila). 2011;4:1873–83.
Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120:1640–5.
Midttun O, Hustad S, Ueland PM. Quantitative profiling of biomarkers related to B-vitamin status, tryptophan metabolism and inflammation in human plasma by liquid chromatography/tandem mass spectrometry. Rapid Commun Mass Spectrom. 2009;23:1371–9.
van Duijnhoven FJ, Bueno-de-Mesquita HB, Calligaro M, Jenab M, Pischon T, Jansen EH, et al. Blood lipid and lipoprotein concentrations and colorectal cancer risk in the European prospective investigation into cancer and nutrition. Gut. 2011;60:1094–102.
Rinaldi S, Rohrmann S, Jenab M, Biessy C, Sieri S, Palli D, et al. Glycosylated hemoglobin and risk of colorectal cancer in men and women, the European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev. 2008;17:3108–15.
Eussen SJ, Vollset SE, Igland J, Meyer K, Fredriksen A, Ueland PM, et al. Plasma folate, related genetic variants, and colorectal cancer risk in EPIC. Cancer Epidemiol Biomarkers Prev. 2010;19:1328–40.
Eussen SJ, Vollset SE, Hustad S, Midttun O, Meyer K, Fredriksen A, et al. Plasma vitamins B2, B6, and B12, and related genetic variants as predictors of colorectal cancer risk. Cancer Epidemiol Biomarkers Prev. 2010;19:2549–61.
Acknowledgements
We thank the participants, study and administrative staff, and researchers in the European Prospective Investigation into Cancer and Nutrition (EPIC) Cohort for their outstanding cooperation.
Contributors
We would like to specifically acknowledge the contribution of Joyce Kong and Heinz Freisling (International Agency for Research on Cancer IARC-WHO, Lyon, France) for critical revision of the manuscript, and to Ellen Kohlsdorf (German Institute of Human Nutrition) and Bertrand Hemon (International Agency for Research on Cancer IARC-WHO, Lyon, France) for data management.
Funding
The EPIC cohort is supported by the Europe Against Cancer Program of the European Commission (SANCO). The individual centers also received funding from: Denmark: Danish Cancer Society; France: Ligue centre le Cancer, Institut Gustave Roussy, Mutuelle Générale de l’Education Nationale, Institut National de la Santé et de la Recherche Médicale (INSERM); Greece: the Hellenic Health Foundation, the Stavros Niarchos Foundation, and the Hellenic Ministry of Health and Social Solidarity; Germany : German Cancer Aid, and Federal Ministry of Education and Research; Italy: Italian Association for Research on Cancer and the National Research Council; The Netherlands: Dutch Ministry of Public Health, Welfare and Sports (VWS), Netherlands Cancer Registry (NKR), LK Research Funds, Dutch Prevention Funds, Dutch ZON (Zorg Onderzoek Nederland), World Cancer Research Fund (WCRF), Statistics Netherlands; Norway: Helga – Nordforsk centre of excellence in food, nutrition and health and The Norwegian Extra Foundation for Health and Rehabilitation, The Norwegian Cancer Society; Spain: Health Research Fund (FIS) of the Spanish Ministry of Health (Exp 96/0032, RETICC DR06/0020), the Spanish Regional Governments of Andalusia, Asturias, Basque Country, Murcia (N0 6236), and the Navarra and the Catalan Institute of Oncology; Sweden: Swedish Cancer Society, Swedish Scientific Council, and Regional Governments of Skane and Västerbotten; UK: Cancer Research UK and Medical Research Council.
Grant supports for the biochemical measurements: HDL-C and TG were analysed with additional support from the Ministry of Public Health, Welfare and Sports, the Netherlands,German Cancer Aid, Federal Ministry for Education and Research, European Union, European Union and AIRC-ITALY , German Cancer Aid, Federal Ministry for Education and Research, European Union, Stavros Niarchos Foundation , Hellenic Ministry of Health, Hellenic Health Foundation, MRC and Cancer Research UK;Hba1c was analysed with additional support from National Cancer Institute grant 1RO1CA102460 and data analyses on CRP were performed with support from World Cancer Research Fund International and Wereld Kanker Onderzoek Fonds (WCRF NL).
The funders played no role in designing or conducting the study or in the collection, management, analysis, and interpretation of the data, nor did they have any input into the preparation, review, or approval of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interest.
Authors’ contributions
SCC, SEV, ØM, PMU, BB, PV, and KA participated in the data analysis, manuscript writing, and interpretation of the results. BB, ML, GF, MB, RK, TK, TP, DD, ATjønneland, KO, JQ, AA, EM, MD, JMH, AB, KTK, NJW, RT, ATrichopoulou, PL, DT, GM, CA, RT, AM, PHP, EW, RP, IL, MG, YL, AJC, ER, and PV were involved in data collection and interpretation of the results. All authors read and approved the final manuscript.
Dimitrios Trichopoulos Deceased.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chuang, SC., Boeing, H., Vollset, S.E. et al. Cellular immune activity biomarker neopterin is associated hyperlipidemia: results from a large population-based study. Immun Ageing 13, 5 (2016). https://doi.org/10.1186/s12979-016-0059-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12979-016-0059-y