
Abstract
Background
Transanal Minimally Invasive Surgery (TAMIS) has revolutionized local excision of mid and high rectal lesions; benign or malignant. It is a technique that is developed as a hybrid between Transanal Endoscopic Microsurgery (TEM) and laparoscopic surgery for resection of rectal lesions.
Methods
We retrospectively reviewed prospectively collected data on patients who underwent TAMIS for benign and early malignant rectal lesions between Jan 2015 and Sept 2019, at Hamad General Hospital, Doha, Qatar.
We assessed the following outcomes: feasibility, fragmentation of specimen, operative time, length of stay (LOS) post-operative complications, and margin negativity.
Results
Seventeen consecutive patients underwent TAMIS for benign and malignant rectal lesions. The average length of stay (LOS) is 1.5 days (1–6 days). Seven patients had different types of benign adenomas, five patients had proven adenocarcinoma, three patients had well-differentiated neuroendocrine tumors, one patient with hyperplastic polyp, and one patient had inflammatory polyp. No fragmentation occurred or detected by histopathologic examination, except in a patient who had inflammatory polyp, where the lesion removed in two fragments.
Conclusion
TAMIS procedure is feasible and safe even in a relatively low-volume colorectal unit. Using this tool, many patients can avoid unnecessary radical surgery. Therefore, we believe that TAMIS should form part of every specialized colorectal service repertoire. To our knowledge, this is the largest series in the gulf region.
Similar content being viewed by others

Background
Management of rectal lesions, benign or malignant, evolved with the improvement of surgical tools and techniques. Total mesorectal excision (TME) and proctectomy remain the gold standard curative procedure [1, 2]. Based on evidence from multiple large randomized controlled trials (RCTs), minimally invasive TME operations using laparoscopy and robotic systems have been implemented and used widely across the globe.
Rectal lesions are increasingly detected with increased screening and awareness. This is connected to improved tools of diagnosis and management of these lesions.
Local excision (LE) of benign and early malignant rectal lesions was traditionally described to remove lesions within 8 cm from the anal verge [3]. Higher lesions in the rectum rendered amenable for local excision using Transanal Endoscopic Microsurgery system described by Buess et al. more than three decades ago [4]. It became more attractive for many reasons; such as better functional outcomes, less morbidity, faster recovery and avoidance of radical resections [3].
Transanal Minimally Invasive Surgery (TAMIS) has revolutionized local excision of mid and high rectal lesions; benign or malignant. Since its introduction in 2009 by Atallah et al., this hybrid tool between single port laparoscopy and Transanal Endoscopic Microsurgery (TEM), has gained wider acceptance and popularity than TEM or the traditional Parks Transanal Excision (TAE), due to its superior surgical outcomes, shallow learning curve, and low cost, in addition to easier setup and more flexibility during the procedure [5].
Methods
We retrospectively reviewed prospectively collected data on patients who underwent TAMIS for benign and early malignant rectal lesions between Jan 2015 and Sept 2019, at Hamad General Hospital, Doha, Qatar. All cases were discussed in colorectal multidisciplinary team (MDT) and the procedures were done by a single colorectal surgeon or under his direct guidance.
For malignant lesions, preoperative staging accomplished by CT scan and Rectal MRI. All cases were discussed in the tumor board before the procedure.
We assessed the following outcomes: feasibility, fragmentation of specimen, operative time, length of stay (LOS) post-operative complications, and margin negativity.
All patients underwent TAMIS in Lioyd-Davies position under general anesthesia (GA), except one patient who refused GA and had spinal anesthesia. We used GelPOINT path transanal access platform, and maintained pneumorectum to pressure of 15 mmHg with AirSeal system insufflator. As a standard operative preparation; all patients were positioned in Lloyd Davis position with a Bean Bag underneath the patient, in case laparoscopic access to the peritoneal cavity was to be required. All patients were given rectal phosphate enema approximately 4 h before the procedure. All patients received standard DVT prophylaxis. Prophylactic antibiotics were also administered at induction of anesthesia.
We used the GelPOINT path transanal access platform (Applied Medical, Rancho Santa Margarita, CA), AirSeal port (Conmed, NY, USA) to establish and sustain pneumorectum, and 30 degrees scope. We always approximate the defect after excision with V-Loc™ Vicryl (Medtronic, Minneapolis, MN, USA) The specimen then sent oriented to the histopathology department (Fig. 1).

a Colonoscopic appearance of rectal sessile polyp. b TAMIS view of the same polyp. c the polyp post TAMIS resection before closure. d resection site post closure
Results
Seventeen consecutive patients underwent TAMIS for benign and malignant rectal lesions, in the period between Jan 2015 and September 2019. The patients’ population consisted of 6 women (34%) and 11 men (64%), with an average age of 52 years (28–88). Nine patients had an ASA score of 2, six patients of ASA score 3, and three patients with an ASA score of 1 (Table 1).
The average length of stay (LOS) is 1.5 days (1–6 days). Eleven out of the eighteen patients discharged on day 1 post operatively. One patient stayed 6 days because of post-operative hypotension which was managed conservatively.
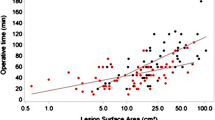
The average operative time was 74.17 min (20–180 min). The average distance of the lesion from the anal verge is 7.47 cm (3–18 cm). Eight patients (47%) had the lesion > 7 cm from the anal verge.
Seven patients had different types of benign adenomas, five patients had proven adenocarcinoma, three patients had well-differentiated neuroendocrine tumors, one patient with hyperplastic polyp, and one patient had inflammatory polyp.
No fragmentation occurred or detected by histopathologic examination, except in a patient who had inflammatory polyp, where the lesion removed in two fragments. The average size of the excised lesions is 2.62 cm (1.2–7 cm). All resection margins were free, the nearest margin was 4 mm in a tubular adenoma specimen. Six patients had a discrepancy between the preoperative and the post-operative histopathology; one of the patients down-staged from polyp adenocarcinoma to polyp high-grade dysplasia. Another patient was diagnosed as moderately differentiated adenocarcinoma pre-operatively; which is located 5 cm from the anal verge, down-staged to benign lesion on final histopathology following TAMIS excision. Both of these patients were spared radical resections (Table 2).
In one patient, the peritoneum is entered during the excision of a tubular adenoma 10 cm from the anal verge. Laparoscopic closure of the peritoneum was achieved as well as transanal closure. The patient was discharged 2 days post operatively, with no complications.
There was one procedure-related complication during excision of a serrated adenoma located 10 cm from the anal verge, were the peritoneum was breached. Immediate laparoscopic repair was done, and the patient discharged home on day 2 post-operatively with no complications.
Another patient had minimal post-operative fresh bleeding per rectum which required no transfusion.
There were no other procedure-related immediate or 30-day complications in any of the other patients.
Discussion
Transanal Minimally Invasive Surgery (TAMIS) is a technique that is developed as a hybrid between Transanal Endoscopic Microsurgery (TEM) and laparoscopic surgery for resection of rectal lesions. Adoption of the technique has spread widely due to availability of the laparoscopic tools and insufflators and the single-site port, as well as the shallow learning curve, and most importantly the comparable safety and oncologic outcomes.
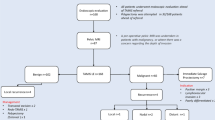
NCCN guidelines have defined the lesions which are appropriate for local excision using any system: mobile rectal tumors, less than 3 cm in size, occupying less than one-third of the circumference of the bowel, not extending beyond the submucosa, with well to moderate differentiation, and low-risk histopathological features. Transanal local excision is not appropriate for rectal tumors with high-risk characteristics, including lymphovascular invasion, perineural invasion, and mucinous components [1].
We have demonstrated a congruent result of safety and oncologic outcomes using TAMIS compared to the existing literature and case series [6,7,8]. All our malignant lesion resections as well as NET resections were margin negative. The reported positive margin in a recent large series of 200 patients was 7% [9], and up to 2 out of 3 NET resections in some series [10] (Tables 3 and 4).
Our series showed that despite the fact that a relatively small number of patients dispersed over a period of nearly 5 years, the surgical outcomes, operative time, and quality of specimens did not compare unfavorably. One of our patients had a lesion 10 cm from anal verge with malignant features of T3 tumor by MRI, which was difficult to diagnose using colonoscopy due to superficial biopsy. TAMIS used in this patient to obtain adequate biopsies, which confirmed adenocarcinoma enabling the patient to receive neoadjuvant chemoradiotherapy.
Conclusions
TAMIS procedure is feasible and safe even in a relatively low-volume colorectal unit. Using this tool, many patients can avoid unnecessary radical surgery. Therefore, we believe that TAMIS should form part of every specialized colorectal service repertoire. To our knowledge, this is the largest series in the gulf region.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- TAMIS:
-
Transanal Minimally Invasive Surgery
- TEM:
-
Transanal endoscopic microsurgery
- TAE:
-
Transanal excision
- LE:
-
Local excision
- MDT:
-
Multidisciplinary team
- NET:
-
Neuroendocrine tumor
- LOS:
-
Length of stay
- ASA:
-
American College of Anesthesiologists Physical Status Classification
- RCT:
-
Randomized controlled trial
- CT scan:
-
Computerized tomography scan
- MRI:
-
Magnetic resonance imaging
References
Heafner TA, Glasgow SC. A critical review of the role of local excision in the treatment of early (T1 and T2) rectal tumors. J Gastrointest Oncol. 2014;5(5):345–52.
Keller DS, Haas EM. Transanal minimally invasive surgery: state of the art. J Gastrointest Surg. 2016;20(2):463–9.
Lee TG, Lee SJ. Transanal single-port microsurgery for rectal tumors: minimal invasive surgery under spinal anesthesia. Surg Endosc. 2014;28(1):271–80.
Buess G, Hutterer F, Theiss J, Bobel M, Isselhard W, Pichlmaier H. A system for a transanal endoscopic rectum operation. Chirurg. 1984;55(10):677–80.
Caycedo-Marulanda A, Jiang HY, Kohtakangas EL. Transanal minimally invasive surgery for benign large rectal polyps and early malignant rectal cancers: experience and outcomes from the first Canadian centre to adopt the technique. Can J Surg. 2017;60(6):416–23.
Albert MR, Atallah SB, DeBeche-Adams TC, Izfar S, Larach SW. Transanal minimally invasive surgery (TAMIS) for local excision of benign neoplasms and early-stage rectal cancer: efficacy and outcomes in the first 50 patients. Dis Colon Rectum. 2013;56(3):301–7.
Martin-Perez B, Andrade-Ribeiro GD, Hunter L, Atallah S. A systematic review of transanal minimally invasive surgery (TAMIS) from 2010 to 2013. Tech Coloproctol. 2014;18(9):775–88.
McLemore EC, Weston LA, Coker AM, et al. Transanal minimally invasive surgery for benign and malignant rectal neoplasia. Am J Surg. 2014;208(3):372–81.
Lee L, Burke JP, Debeche-Adams T, et al. Transanal minimally invasive surgery for local excision of benign and malignant rectal neoplasia. Ann Surg. 2018;267(5):910–6.
Chen N, Peng YF, Yao YF, Gu J. Trans-anal minimally invasive surgery for rectal neoplasia: experience from single tertiary institution in China. World J Gastrointest Oncol. 2018;10(6):i-144.
Acknowledgements
The publication of this article was funded by the Qatar National Library.
Funding
The processing fees for publication of this article was funded by the Qatar National Library.
Author information
Authors and Affiliations
Contributions
AGA Data acquisition and analysis, drafting the manuscript, AA Data analysis and critical revision of manuscript. MA Data acquisition and critical revision of manuscript. MK: Study concept and design, data analysis, writing and revision of the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Abutaka, A., Ahmed, A., Abunada, M. et al. Transanal Minimally Invasive Surgery (TAMIS) in Qatar: initial experience. BMC Surg 20, 138 (2020). https://doi.org/10.1186/s12893-020-00797-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-020-00797-6