
Abstract
Background
Leg pain, especially of the knees and hips, is common among senior workers and may limit the ability to perform physically demanding work. In light of the aging workforce, this study determined the joint association of physical work demands and leg pain intensity for work-limiting pain in senior workers.
Methods
Currently employed senior workers (≥50 years) participated in the SeniorWorkingLife study in 2018 (n = 12,879). Associations between the combination of physical work demands and leg pain intensity (interaction) with work-limiting pain (outcome) were modeled using binary logistic regression analyses while controlling for potential covariates.
Results
We found a significant interaction (P < 0.001) between physical work demands and leg pain intensity for work-limiting pain. The combination of higher physical work demands and higher leg pain intensity had the worst outcome in terms of the odds of experiencing work-limiting pain. For example, 70% of those with the combination of high physical work demands and leg pain intensity ≥7 (scale 0–10) experienced that the pain limited them to at least some degree in their work.
Conclusions
The combination of high physical work demands and high leg pain intensity are associated with limited ability to perform work among senior workers. These findings highlight the importance of prioritizing the physical work environment in physically demanding occupations, particularly among senior workers, for prolonging working life. Thus, adjusting the work demands, e.g. through use of assistive devices, and lowering the pain, e.g. through physical rehabilitation, may be necessary to sustain work ability to a high age in this group of workers.
Trial registration
This was registered as a cohort study in ClinicalTrials.gov (Identifier: NCT03634410) on the 18th of August 2018 (Retrospectively registered).
Similar content being viewed by others


Background
Musculoskeletal disorders (MSD) in both upper and lower body are highly prevalent and debilitating worldwide, with upper body MSD such as low-back pain and neck-shoulder pain estimated to affect approximately 577 and 289 millions (~ 8 and 4% of the global population in 2017) worldwide, respectively, and lower body MSD in form of osteoarthritis of the hip and particularly the knee estimated to affect around 300 millions wordwide (4% of the global population in 2017) [1, 2]. However, recent research reviews indicate that knee−/hip osteoarthritis and other lower body MSD have received less attention in research in work environmental rehabilitation than low-back and neck-shoulder pain [3]. The reason for this may be that lower body MSD is less prevalent in the working population as a whole, and therefore largely overseen as a problem in specific target groups such as older [2, 4] and female workers [4,5,6], who are generally more affected by MSDs like low-back pain and osteoarthritis.
MSD are associated with high personal costs such as negatively affecting the ability to work [7,8,9,10] and quality of life [11]. Also, MSD may affect employers and society through increased risk of sickness absence [9, 12,13,14,15,16] and increased risk of premature exit from the labour market [17,18,19]. A recent survey suggested that approximately 28% of Danish senior workers aged 50–64 years feel limited in their job due to MSD, with even higher prevalences among senior workers in manual occupations [20]. Self-reported work limitation due to musculoskeletal pain has previously been associated with a 54% increased risk of long-term sickness absence [16], emphasizing the relation between MSDs, health, and work.
In Denmark, a relatively large proportion of the working population holds manual jobs that are physically demanding (depending on definitions) [21]. According to a large-scale study among the general working population in Denmark, approximately 40% of Danish workers report to walk or stand for at least ¾ of their workday, while approximately 17% report to be squatting or kneeling at least ¼ of their workday [22]. While the etiology of MSD is multifactorial [23], the working environment plays a huge role in the occurrence and retention of MSD, with physically demanding manual labour being associated with an increased risk of MSD [24, 25]. Knowing that physical capacity decreases inherently with age [26], some senior workers may not have the capacity to overcome the physical demands at work. In combination with the increased prevalence of MSD with age [21, 27], this could lower work ability [28,29,30] and increase the risk of leaving the labour market prematurely. Due to the demographical developments, the number of older workers is gradually increasing [31], and determining factors that could mediate the practical consequences of MSD may provide useful knowledge for the practitioners at the workplace to act on in the pursuit of sustainable employment [32].
Importantly, many workers have MSD without reporting lower work ability and increased sickness absence [29, 33], which may be explained by – amongst others – factors as musculoskeletal pain intensity and location, physical work demands, age, and sex [8,9,10, 14, 29, 34,35,36,37,38,39,40]. For example, it is possible that a senior employee with MSD may be capable of going to work and take full care of his/her work duties if it is a sedentary office job, whereas another senior employee with MSD may not be able to perform his or her job tasks if it is a job that is physically demanding. Also, women may be predisposed to work limitations compared to men as they typically possess lower muscle mass and muscle strength [41] and thus lower physical capacity to compensate with when dealing with MSD. Furthermore, a study among healthcare workers showed that the pain thresholds associated with increased long-term sickness absence differed between pain locations, with knee pain being associated with increased long-term sickness absence at the lowest pain threshold (i.e. ≥3 on a scale from 0 to 9) compared to low-back and neck−/shoulder pain (5 and 4, respectively) [14], potentially indicating a relatively larger impact of knee pain on working functional capacity compared to low-back and neck−/shoulder MSDs. This study and others [8, 9, 40] underline the importance of pain intensity on the degree of functional limitation, with higher pain intensities being associated with higher risks of work disability and sickness absence.
In this confirmatory cross-sectional study among senior workers, we aim to investigate the joint associations of physical work demands and leg pain intensity with work limitations due to leg pain stratified by sex. In addition, we explored potential sex differences herein. We hypothesize that higher physical work demands and higher leg pain intensity increase the odds of experiencing pain that limits the ability to work.
Methods
Study design and setting
The present cross-sectional study regarding work-limiting pain and physical work demands bases upon data from the first wave of the SeniorWorkingLife study [42], which has been registered as a cohort study in ClinicalTrials.gov (Identifier: NCT03634410). SeniorWorkingLife is a comprehensive questionnaire survey assessing work environment and health among senior workers in Denmark (≥50 years) [42]. The SeniorWorkingLife baseline questionnaire survey was sent out between July and October 2018. Specific questions used in the present analysis are specified below. The reporting of the study followed the guidelines for the reporting of observational studies in epidemiology (STROBE) [43].
Participants
Statistics Denmark drew a probability sample of a total of 30,000 Danes ≥50 years (18,000 in employment, 7000 unemployed, 3000 on voluntary early retirement, 2000 on disability pension), who were invited to participate in the questionnaire survey by a personal link via a web-based digital mailbox linked to each worker’s social security number (‘E-boks’) [42]. Subsequently, the survey data were merged with high-quality national registers provided by Statistics Denmark. We only included senior workers who confirmed on the questionnaire that they were employed at the time of the reply. The response rate for completing all questions in the questionnaire was 56% among currently employed workers, but in the present analyses, we also included those who did not fill out all the questions in the questionnaire (n = 11,786). Granted that not all participants filled in all survey questions, the exact number of participants for each analysis varies. Data from the SeniorWorkingLife study regarding the joint association of low-back pain and physical work demands with work limitations have previously been published [44].
Ethical approval
Danish law permits scientific usage of questionnaire- and register data without collecting informed consent or applying for approval by ethical and scientific committees [45]. Statistics Denmark were responsible for depersonalizing and storing all data on their servers from where the researchers performed the analyses through remote access.
Explanatory variables
Physical work demands
Physical work demands were assessed by the following survey-question: ‘How would you describe the physical activity level in your current job?’, with response options being 1) ‘Mostly sedentary work that is not physically demanding’, 2) ‘Mostly standing and walking work that otherwise is not physically demanding’, 3) ‘Standing or walking work with some lifting and carrying tasks’ and 4) ‘Heavy or fast work that is physically demanding’ [46, 47].
Leg pain
Participants were classified as having low, moderate, high, and very high leg pain intensities if they reported average pain intensities in the legs (hips, knees, feet) during the past three months at 0–2, 3–4, 5–6, and 7–10, respectively, on a scale from 0 to 10, where 0 indicated no pain and 10 indicated the worst possible pain.
Outcome variable
We used the following modified version of the Standardised Nordic Questionnaire for Musculoskeletal Symptoms [48] to assess work-limiting musculoskeletal pain: ‘To which degree did the pain limit you in your work during the last 3 months?’. The response options were 1) to a very high degree, 2) to a high degree, 3) to some degree, 4) to a small degree and 5) not at all. As done in our previous publications [16, 44], these response options were subsequently dichotomized to 1) not at all to a small degree and 2) some degree to a very high degree.
Covariates
We controlled for the following potential covariates: age, sex, BMI, smoking status, educational level, psychosocial work factors as well as musculoskeletal pain in the other body regions. Age (years), body mass index (BMI) (kg/m2), psychosocial work environment (0–100, specified below), and musculoskeletal pain during the past three months in the low-back, neck/shoulders, and arms (0–10, see above) were assessed on continuous scales, whereas sex (‘male’ or ‘female’), educational level (see below), smoking status (‘No, never’, ‘Ex-smoker’, ‘Yes, but not every day’ and ‘Yes, every day’), and physical activity during leisure (see definitions below) were categorical variables.
Leisure-time physical activity level was assessed by replying to the following question: ‘How would you describe your physical activity level during leisure for the last 12 months?’. Respondents were given the following response options 1) ‘Mostly sedentary’, 2) ‘Light exercise at least 4 h a week’, 3) ‘Sports or heavy physical activity at least 4 h per week’ and 4) ‘Training and competing regularly and several times a week’ [49]. Psychosocial work factors, i.e. influence at work and recognition from colleagues, were assessed on a continuous scale from 0 to 100 (with 100 being best) by specific questions from the comprehensive and validated Copenhagen Psychosocial Questionnaire [50]. Thus, the greater the score, the higher/better the collegial recognition and influence at work.
Highest attained educational level was drawn from the linked register: 1) Primary school or unknown, 2) High school, 3) Short-term higher education, 4) Medium-term higher education, and 5) Long-term higher education.
We controlled for these variables because previous studies have shown associations between work ability and sickness absence and these occupational and lifestyle factors, i.e., age [28, 29], sex [28, 29], smoking [28], overweight [51], leisure-time physical activity [49], MSD [7,8,9] and psychosocial work environment [29].
Statistical analyses
The statistical analyses were carried out and controlled for potential covariates in the SAS statistical software for Windows (Proc Glimmix, SAS version 9.4, SAS Institute, Cary, NC). We applied two different statistical models. Statistical model 1 was adjusted for age, sex, and pain in the other body regions, whereas the fully adjusted model 2 was additionally adjusted for smoking status, body mass index (BMI), psychosocial work factors, educational level, and physical activity level during leisure. In order to make estimates representative for the population of senior workers, model-assisted statistical weights were applied in all analyses. Weights included sex, age, origin, highest completed education, occupational industry, as well as family income and type.
We performed logistic regression analyses of the associations between work-limiting pain (dichotomous outcome variable) and physical work demands (exposure variables), leg pain intensity, and the interaction between physical work demands and leg pain intensity. Due to the presence of a statistically significant interaction, the results are reported stratified by leg pain intensity. Results are presented as odds ratios (OR) and 95% confidence intervals (CI) unless otherwise stated, with alpha levels below 0.05 considered statistically significant differences.
Results
The baseline characteristics of the study sample are provided in Table 1. The mean age of the respondents was 56.6 years, with around 47, 24, 23, and 6% in occupations characterized by ‘Mostly sedentary work that is not physically demanding’, ‘Mostly standing and walking work that otherwise is not physically demanding’, ‘Standing or walking work with some lifting and carrying tasks’ and ‘Heavy or fast work that is physically demanding’, respectively. Approximately 35, 37, 24, and 36% of the respondents had experienced musculoskeletal pain in the low-back, neck-shoulders, arms, or legs during the last three months, respectively, with average pain intensites of 2.8, 2.9, 1.9, and 2.8, respectively. More specifically, 11% of the entire sample reported doctor-diagnosed osteoarthritis. Overall, around 18% reported work-limitations due to pain (in all four body regions) to some, a large or very large degree, whereas the remaining 82% were either not at all or only to a small degree work-limited due to pain.
Physical work demands and work-limiting pain
The weighted prevalences of work-limiting pain by physical work demands and leg pain intensity among the whole sample are provided in Fig. 1, while the associations between physical work demands and work-limiting pain stratified by sex and leg pain intensity are presented in Table 2.

Weighted prevalences (%) of work-limiting pain among senior workers stratified by physical work demands and leg pain intensity
Overall, we observed a significant dose-response association (p < 0.0001) between leg pain intensity and work-limiting pain among senior workers. We also observed a significant exposure-response association between physical work demands and work-limiting pain (p < 0.0001). In addition, a significant interaction (p < 0.001) between pain intensity and physical work demands for work-limiting pain existed, and the results are therefore stratified by leg pain intensity.
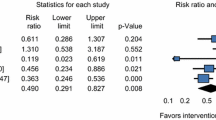
As it appears, the weighted prevalences of work-limiting pain generally increase with physical work demands and leg pain intensity, with a weighted prevalence of approximately 68% among senior workers with very high leg pain intensity (≥7/10) in occupations characterized by ‘heavy or fast work that is physically demanding’ (Fig. 1). As an example based on statistical model 1, the odds of work-limiting pain was significantly increased among senior workers with ‘mostly standing and walking work that otherwise is not physically demanding’ and moderate leg pain (pain intensity: 3–4/10) compared to senior workers having ‘mostly sedentary work that is not physically demanding’ (OR: 1.66, 95% CI: 1.58–1.76), and even higher odds among senior workers with ‘heavy or fast work that is physically demanding’ and moderate leg pain (OR: 3.82, 95% CI: 3.58–4.08). While the sex-stratified odds ratios follow the same aforementioned pattern (increased leg pain intensity and physical work demands being associated with increased odds of work-limiting pain) between sexes, women seem at higher odds for work-limitations due to pain compared to men, especially women with heavy or fast work.
Discussion
The present study confirms that physical work demands and pain intensity are important factors to consider in terms of the practical consequences of MSD among senior workers, and particularly among women. In support of our hypothesis, we found a dose-response association of both physical activity during work and leg pain intensity with work limitations due to pain. These findings may call for a differentiated approach in the pursuit of sustainable employment through aging.
Leg pain prevalence and intensity and work limitations
Low-back and neck-shoulder pain remain highly prevalent and debilitating pain regions globally [1] and have accordingly received much scientific and work environmental rehabilitative attention [3]. However, in our study among senior workers, we found equally high prevalences of musculoskeletal pain in the low-back, neck-shoulders, and legs of 35, 37, and 36%, respectively. Of the entire sample, 11% reported doctor-diagnosed osteoarthritis, which may explain some of the high leg pain prevalence, although not all cases. Overall, this underscores that the societal impact of lower body leg pain – specifically among senior workers – should not be underrated, especially not considering that lower body knee pain, specifically, has been associated with long-term sickness absence at a proportionately lower pain intensity threshold than low-back and neck-shoulder pain [14].
For the entire study sample of senior workers, we found a significant dose-response association (p < 0.0001) between leg pain intensity and work-limiting pain. Our results thus elaborate on previous findings demonstrating the importance of not just the presence of pain but also the severity of pain and functional limitation for long-term sickness absence and the ability to work [8, 9, 14, 40]. For instance, we have previously demonstrated strong dose-response associations of increasing pain intensities in the low-back, neck-shoulders, and knees with increased risk of long-term sickness absence in healthcare workers [14]. In accordance, Hallman and colleagues reported that sick leave increased and work ability decreased across all longitudinal trajectory classes of neck-shoulder pain (i.e. from low, moderate, strong fluctuating to severe persistent pain) [9]. From a rehabilitation perspective, it seems that even a small decrease in leg pain intensity could lead to a parallel decrease in work limitation due to pain. This indicates that senior workers do not have to be pain-free in order to reduce work limitations due to pain. Previous research has shown that strength training at the workplace is effective for reducing pain intensity [3, 52]. Even though strength training does not completely eliminate the pain, it reduces pain intensity with moderate to large effect sizes, making it a potent tool for workplace rehabilitation of senior workers with work limitations due to pain.
Physical work demands and work-limiting pain
In the present study, we also demonstrated a significant exposure-response association between physical work demands and work-limiting pain among senior workers (p < 0.0001). This finding is in accordance with previous studies reporting a higher risk of low work ability [10, 29, 37] as well as sickness absence [33,34,35,36, 53] and disability pension [54] among workers with MSD and high physical work demands, which further emphasizes the practical consequences of MSD.
However, and importantly, our analysis demonstrated a strong significant interaction between physical work demands (p < 0.001) and pain intensity, indicating a combined and interacting effect of physical work demands and leg pain intensity on work-limiting pain.
Several studies have reported compromised work ability and productivity (presenteeism) among workers with MSD having manual jobs characterized by higher physical work demands as compared to workers with MSD in more sedentary jobs [10, 29, 37,38,39,40]. A Dutch study reported that high physical workload (including high exposures of heavy lifting, awkward and static postures) compared to low physical workload was associated with low work ability among workers with physician-diagnosed MSD [37], whereas Pensola and coworkers demonstrated that having jobs with predominantly ‘strenuous’ work tasks was associated with lower work ability compared to jobs with ‘moderately heavy’ or ‘light’ work tasks among workers with multi-site pain (including lower extremity pain) [29]. More specifically, semi-manual and manual labour was found to be significant risk factors for work-limitations (presenteeism) among workers with chronic knee pain [39]. In opposition, Wilkie and colleagues did not report manual labour as a risk factor for developing work restriction among older workers (50–59 years) with lower body MSD [40].
With regards to sickness absence, manual labour has been associated with an increased risk of sickness absence among workers with MSD [33,34,35,36]. Haukka demonstrated that having a physically light job with no exposure to lifting, carrying, kneeling, squatting and other physical work demands was associated with a lower risk of sickness absence among Finns with multi-site MSD [33]. More specifically, lower body pain due to hip and especially knee osteoarthritis has been associated with an increased risk of sickness absence in manual workers compared to non-manual workers [35, 36]. Thus, these studies together with our data could indicate larger practical consequences of having MSD among manual workers than among sedentary workers, which should call for differentiated action between working groups.
Sex differences
While our sex-stratified analyses show similar patterns between sexes, women generally seem at higher odds of work-limiting pain. At a similar pain intensity, women with high physical work demands (heavy or fast work) seem at particularly high risk of work-limitiations due to pain (ORs of 5.49, 3.20, and 5.63 in women with moderate, high, and very high pain, respectively) compared to men with equally high physical work demands (ORs of 2.64, 2.96, 2.97, respectively). High physical work demands (by job title) have previously been associated with increased risk of sick leave and disability pension among both women and men with knee osteoarthritis [35]. As pertains to sex, arthritis-attributable work limitations have been reported to be more prevalent among women than men [55]. Likewise, sick leave and disability pension are also more prevelant among women with knee osteoarthritis than men with knee osteoarthritis [56]. Further, in a previous study pertaining work factors facilitating working beyond state pension age, women tended to be more affected by high physical work demands [57]. In opposition, the female gender (as compared to male) has been associated with good work ability among workers with multi-site pain [29], whereas other studies have reported no gender differences in the odds for work restrictions, absenteeism and presenteeism as well as risk of sick leave among workers with lower limb joint pain, chronic knee pain and knee and osteoarthritis, respectively [36, 39, 40].
Thus, both reducing the physical work demands and pain intensity may be targets that are worth pursuing by work environment professionals. As mentioned above, workplace-based exercise in terms of strength training is a well-documented beneficial means to reduce MSD pain intensity [2, 45] that may be particularly effective in terms of reducing work-limitation among senior workers with manual jobs.
Another viable strategy may be tailoring the physical work demands (e.g. reducing) to the capacities and age of the worker with MSD [58]. As example, Haukka reported that the possibility to sufficiently adjust the length of the working day was a protective factor for sickness absence in workers with MSD [33]. In the Nordic countries, however, it currently seems that older manual workers experience similar or even higher occupational physical demands compared to younger workers [58, 59]. In addition, we have previously reported a strong labour market inequality in opportunities offered by the workplace for supporting a long and healthy worklife, whereby senior workers in manual labour are offered fewer opportunities such as exercise training during work compared to sedentary senior workers [60]. This poses a further threat to prolonging worklife among senior manual workers [47] and needs to be further addressed in future studies.
Strengths and limitations
The present study contains several strengths and limitations. It is a clear strength of the study that the invitation of potential participants was based on a probability sample drawn by Statistics Denmark among all eligible Danish residents ≥50 years. Further, all analyses were performed by employing statistical weights based on national registers, which ensured that the data was representative of senior workers in Denmark, and reduced the potential influence of non-response bias. The large and representative sample strengthens the statistical power and reduces the chances of statistical type II errors. A limitation of the study is the cross-sectional design, which does not allow for causal inferences and entails the risk of reverse causation.
The step-wise adjustment for potential covariates in the statistical models only changed the odds-estimates to a very small extent. Thus, it seems that educational attainment, physical exercise, smoking, BMI, and psychosocial work factors are less important factors for the interplay between pain intensity and work-limiting pain. However, other studies show that both overweight and smoking may be work-limiting in terms of increasing the risk of sickness absence [61].
The presented results may also be biased by ‘the healthy worker effect’ as we only included senior workers still capable of working and excluded those that have left the labor market prematurely or changed to a less physically demanding job due to health problems such as MSD. Thus, it cannot be ruled out that individuals with the longest history of physically and mentally demanding work could already be outside the labour market or in another job when the SeniorWorkingLife study was initiated. Hence, we consider our odds estimates to be relatively conservative and may thus underestimate the actual odds estimates. We used self-reports to determine physical activity during work, which may have introduced self-report bias and inaccuracy [62], and hence represent a limitation to the study. However, we have previously demonstrated strong agreement between the specific research item used regarding physical work characteristics and grouping based on ISCO (International Standard Classification of Occupations 1), where respondents are stratified into occupational groups based on high-quality national registers [47]. Additionally, self-reporting can result in common method variance where the answers may be influenced by e.g. the respondents mood, health status and socioeconomic status [63]. Furthermore, different time frames between variables (leg pain intensity, physical activity in leisure, current physical work characteristics etc) also constitute a limitation of the study. Future studies investigating the joint association of physical work demands and pain intensity with work-limiting pain may employ other methods such as technical measurements of physical activity during a working day or using job titles.
Conclusion
Physical work demands and pain intensity are important factors to consider with regards to the practical consequences of MSD among both female and male senior workers. Here, we report dose-response associations of both physical activity during work and leg pain intensity with work limitations due to pain, with stronger associations noted in women than men. These findings suggest that approaches in the pursuit of sustainable employment through aging should be differentiated between work groups and sexes.
Availability of data and materials
The authors encourage collaboration and use of the data by other researchers. Data are stored on the server of Statistics Denmark, and researchers interested in using the data for scientific purposes should contact the project leader Prof. Lars L. Andersen, lla@nfa.dk, who is responsible for the study design, questionnaire development, definition of population, and data collection.
Abbreviations
- 95% CI:
-
95% confidence intervals
- BMI:
-
Body mass index
- OR:
-
Odds ratio
- MSD:
-
Musculoskeletal disorders
- LTSA:
-
Long-term sickness absence
References
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–858.
Institute for Health Metrics and Evaluation (IHME). GBD Compare Data Visualization, http://vizhub.healthdata.org/gbd-compare (accessed 28 July 2020).
Sundstrup E, Seeberg KGV, Bengtsen E, et al. A Systematic Review of Workplace Interventions to Rehabilitate Musculoskeletal Disorders Among Employees with Physical Demanding Work. J Occup Rehabil. Epub ahead of print 26 March 2020. DOI: https://doi.org/10.1007/s10926-020-09879-x.
Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393:1745–59.
Greenspan JD, Craft RM, LeResche L, et al. Studying sex and gender differences in pain and analgesia: a consensus report. Pain. 2007;132:S26–45.
Pereira D, Peleteiro B, Araújo J, et al. The effect of osteoarthritis definition on prevalence and incidence estimates: a systematic review. Osteoarthr Cartil. 2011;19:1270–85.
Miranda H, Kaila-Kangas L, Heliövaara M, et al. Musculoskeletal pain at multiple sites and its effects on work ability in a general working population. Occup Environ Med. 2010;67:449–55.
Bayattork M, Jakobsen MD, Sundstrup E, et al. Musculoskeletal pain in multiple body sites and work ability in the general working population: cross-sectional study among 10,000 wage earners. Scand J Pain. 2019;19:131–7.
Hallman DM, Holtermann A, Dencker-Larsen S, et al. Are trajectories of neck-shoulder pain associated with sick leave and work ability in workers? A 1-year prospective study. BMJ Open. 2019;9:e022006.
Neupane S, Virtanen P, Leino-Arjas P, et al. Multi-site pain and working conditions as predictors of work ability in a 4-year follow-up among food industry employees. Eur J Pain. 2013;17:444–51.
McDonald M, da Costa DBM, Ullman S. Musculoskeletal pain in the workforce: the effects of Back, arthritis, and fibromyalgia pain on quality of life and work productivity. J Occup Environ Med. 2011;53:765–70.
Andersen LL, Mortensen OS, Hansen JV, et al. A prospective cohort study on severe pain as a risk factor for long-term sickness absence in blue- and white-collar workers. Occup Environ Med. 2011;68:590–2.
Andersen LL, Clausen T, Mortensen OS, et al. A prospective cohort study on musculoskeletal risk factors for long-term sickness absence among healthcare workers in eldercare. Int Arch Occup Environ Health. 2012;85:615–22.
Andersen LL, Clausen T, Burr H, et al. Threshold of musculoskeletal pain intensity for increased risk of long-term sickness absence among female healthcare Workers in Eldercare. PLoS One. 2012;7:e41287.
Morken T, Riise T, Moen B, et al. Low back pain and widespread pain predict sickness absence among industrial workers. BMC Musculoskelet Disord. 2003;4:21.
Andersen LL, Thorsen SV, Flyvholm M-A, et al. Long-term sickness absence from combined factors related to physical work demands: prospective cohort study. Eur J Pub Health. 2018;28:824–9.
Natvig B, Eriksen W, Bruusgaard D. Low back pain as a predictor of long-term work disability. Scand J Public Health. 2002;30:288–92.
Øverland S, Harvey SB, Knudsen AK, et al. Widespread pain and medically certified disability pension in the Hordaland health study. Eur J Pain. 2012;16:611–20.
Haukka E, Kaila-Kangas L, Ojajärvi A, et al. Multisite musculoskeletal pain predicts medically certified disability retirement among Finns. Eur J Pain. 2015;19:1119–28.
Sundstrup E, Meng A, Poulsen OM, et al. Seniorers Arbejdsmiljø og Helbred - Analyse til Seniortænketanken for et længere & godt seniorarbejdsliv. p. 1–139.
National Research Centre for the Working Environment. Arbejdsmiljø og Helbred i Danmark 2012–2018, 2020 https://arbejdsmiljodata.nfa.dk/ ( accessed 27 August 2019).
Det Nationale Forskningscenter for Arbejdsmiljø. Fakta om Arbejdsmiljø og Helbred 2018. Det Nationale Forskningscenter for Arbejdsmiljø, (2019) https://nfa.dk/-/media/NFA/Arbejdsmiljodata/Fakta-om-Arbejdsmiljo-og-Helbred-2018.ashx?la=da.
Moseley GL. Reconceptualising pain according to modern pain science. Phys Ther Rev. 2007;12:169–78.
Andersen JH, Haahr JP, Frost P. Risk factors for more severe regional musculoskeletal symptoms: a two-year prospective study of a general working population. Arthritis Rheum. 2007;56:1355–64.
da Costa BR, Vieira ER. Risk factors for work-related musculoskeletal disorders: a systematic review of recent longitudinal studies. Am J Ind Med. 2010;53:285–323.
Kenny GP, Groeller H, McGinn R, et al. Age, human performance, and physical employment standards. Appl Physiol Nutr Metab. 2016;41:S92–S107.
Det Nationale Forskningscenter for Arbejdsmiljø, (2020) Aalborg Universitet, TeamArbejdsliv. SeniorArbejdsLiv, https://www.seniorarbejdsliv.dk/.
El Fassi M, Bocquet V, Majery N, et al. Work ability assessment in a worker population: comparison and determinants of work ability index and work ability score. BMC Public Health. 2013;13:305.
Pensola T, Haukka E, Kaila-Kangas L, et al. Good work ability despite multisite musculoskeletal pain? A study among occupationally active Finns. Scand J Public Health. 2016;44:300–10.
Berg TIJ van den, Elders L a. M, Zwart BCH de, et al. The effects of work-related and individual factors on the work ability index: a systematic review. Occup Environ Med. 2009;66:211–20.
Ilmarinen J. The ageing workforce--challenges for occupational health. Occup Med (Lond). 2006;56:362–4.
Oakman J, Neupane S, Proper KI, et al. Workplace interventions to improve work ability: a systematic review and meta-analysis of their effectiveness. Scand J Work Environ Health. 2018;44:134–46.
Haukka E, Ojajärvi A, Kaila-Kangas L, et al. Protective determinants of sickness absence among employees with multisite pain-a 7-year follow-up. Pain. 2017;158:220–9.
Holtermann A, Hansen JV, Burr H, et al. Prognostic factors for long-term sickness absence among employees with neck-shoulder and low-back pain. Scand J Work Environ Health. 2010;36:34–41.
Hubertsson J, Turkiewicz A, Petersson IF, et al. Understanding occupation, sick leave, and disability pension due to knee and hip osteoarthritis from a sex perspective. Arthritis Care Res (Hoboken). 2017;69:226–33.
Pekkala J, Rahkonen O, Pietiläinen O, et al. Sickness absence due to different musculoskeletal diagnoses by occupational class: a register-based study among 1.2 million Finnish employees. Occup Environ Med. 2018;75:296–302.
van den Berg S, Burdorf A, Robroek SJW. Associations between common diseases and work ability and sick leave among health care workers. Int Arch Occup Environ Health. 2017;90:685–93.
Skovlund SV, Bláfoss R, Sundstrup E, et al. Association between physical work demands and work ability in workers with musculoskeletal pain: cross-sectional study. BMC Musculoskelet Disord. 2020;21:166.
Agaliotis M, Fransen M, Bridgett L, et al. Risk factors associated with reduced work productivity among people with chronic knee pain. Osteoarthr Cartil. 2013;21:1160–9.
Wilkie R, Blagojevic-Bucknall M, Jordan KP, et al. Onset of work restriction in employed adults with lower limb joint pain: individual factors and area-level socioeconomic conditions. J Occup Rehabil. 2013;23:180–8.
Miller AE, MacDougall JD, Tarnopolsky MA, et al. Gender differences in strength and muscle fiber characteristics. Eur J Appl Physiol Occup Physiol. 1993;66:254–62.
Andersen LL, Sundstrup E. Study protocol for SeniorWorkingLife - push and stay mechanisms for labour market participation among older workers. BMC Public Health. 2019;19:133.
von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344–9.
Nygaard PP, Skovlund SV, Sundstrup E, et al. Is low-back pain a limiting factor for senior workers with high physical work demands? A cross-sectional study. BMC Musculoskeletal Disord. 2020;21:622.
Committee System on Biomedical Research Ethics. Guidelines about Notification etc. of a Biomedical Research Project to the Committee System on Biomedical Research Ethics, (2011) http://www.nvk.dk/~/media/NVK/Dokumenter/Vejledning_Engelsk.pdf.
Bláfoss R, Micheletti JK, Sundstrup E, et al. Is fatigue after work a barrier for leisure-time physical activity? Cross-sectional study among 10,000 adults from the general working population. Scand J Public Health. 2019;47:383–91.
Andersen LL, Jensen PH, Sundstrup E. Barriers and opportunities for prolonging working life across different occupational groups: the SeniorWorkingLife study. Eur J Public Health. Epub ahead of print 29 August 2019. DOI: https://doi.org/10.1093/eurpub/ckz146.
Kuorinka I, Jonsson B, Kilbom A, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18:233–7.
Calatayud J, Jakobsen MD, Sundstrup E, et al. Dose-response association between leisure time physical activity and work ability: cross-sectional study among 3000 workers. Scand J Public Health. 2015;43:819–24.
Pejtersen JH, Kristensen TS, Borg V, et al. The second version of the Copenhagen psychosocial questionnaire. Scand J Public Health. 2010;38:8–24.
Andersen LL, Izquierdo M, Sundstrup E. Overweight and obesity are progressively associated with lower work ability in the general working population: cross-sectional study among 10,000 adults. Int Arch Occup Environ Health. 2017;90:779–87.
Van Eerd D, Munhall C, Irvin E, et al. Effectiveness of workplace interventions in the prevention of upper extremity musculoskeletal disorders and symptoms: an update of the evidence. Occup Environ Med. 2016;73:62–70.
Sundstrup E, Andersen LL. Hard physical work intensifies the occupational consequence of physician-diagnosed Back disorder: prospective cohort study with register follow-up among 10,000 workers. Int J Rheumatol. 2017;2017:1037051.
Hubertsson J, Englund M, Hallgårde U, et al. Sick leave patterns in common musculoskeletal disorders – a study of doctor prescribed sick leave. BMC Musculoskelet Disord. 2014;15:176.
THEIS KA, MURPHY L, HOOTMAN JM, et al. Prevalence and correlates of arthritis-attributable work limitation in the US population among persons ages 18–64: 2002 National Health Interview Survey Data. Arthritis Rheum. 2007;57:355–63.
Hubertsson J, Petersson IF, Thorstensson CA, et al. Risk of sick leave and disability pension in working-age women and men with knee osteoarthritis. Ann Rheum Dis. 2013;72:401–5.
Andersen LL, Thorsen SV, Larsen M, et al. Work factors facilitating working beyond state pension age: prospective cohort study with register follow-up. Scan J Work Environ Health. Epub ahead of print. 2020. https://doi.org/10.5271/sjweh.3904.
Oakman J, Clays E, Jørgensen MB, et al. Are occupational physical activities tailored to the age of cleaners and manufacturing workers? Int Arch Occup Environ Health. 2019;92:185–93.
Merkus SL, Lunde L-K, Koch M, et al. Physical capacity, occupational physical demands, and relative physical strain of older employees in construction and healthcare. Int Arch Occup Environ Health. 2019;92:295–307.
Andersen LL, Jensen PH, Meng A, et al. Strong Labour Market Inequality of Opportunities at the Workplace for Supporting a Long and Healthy Work-Life: The SeniorWorkingLife Study. Int J Environ Res Public Health; 16. Epub ahead of print 05 2019. DOI: https://doi.org/10.3390/ijerph16183264.
Labriola M, Lund T, Burr H. Prospective study of physical and psychosocial risk factors for sickness absence. Occup Med (Lond). 2006;56:469–74.
Lagersted-Olsen J, Korshøj M, Skotte J, et al. Comparison of objectively measured and self-reported time spent sitting. Int J Sports Med. 2014;35:534–40.
Podsakoff PM, MacKenzie SB, Lee J-Y, et al. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88:879–903.
Acknowledgements
The authors are grateful for important discussions and input during the development of the study to the many people from Aalborg University, Team Arbejdsliv, National Research Centre for the Working Environment, Statistics Denmark, as well as to the members of the Advisory Board.
Funding
This study was supported by a grant from the Danish foundation, TrygFonden. The funding body played no role in the design of the study or in the collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
LLA designed the study. SVS drafted the manuscript. LLA performed all statistical analysis. LLA, ES, RB, KT and SVS contributed to interpretation of data. All authors contributed substantially to the conception of the work, critically revised the manuscript draft, approved the final version of the manuscript for submission and agreed both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated, resolved, and the resolution documented in the literature.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Danish law permits scientific usage of questionnaire- and register data without collecting informed consent or applying for approval by ethical and scientific committees [45]. Statistics Denmark were responsible for depersonalizing and storing all data on their servers from where the researchers performed the analyses through remote access.
Consent for publication
Not applicable.
Competing interests
None declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Skovlund, S.V., Bláfoss, R., Sundstrup, E. et al. Joint association of physical work demands and leg pain intensity for work limitations due to pain in senior workers: cross-sectional study. BMC Public Health 20, 1741 (2020). https://doi.org/10.1186/s12889-020-09860-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-020-09860-6