
Abstract
Background
Pregnant women exposed to lead are at risk of suffering reproductive damages, such as miscarriage, preeclampsia, premature delivery and low birth weight. Despite that the workplace offers the greatest potential for lead exposure, there is relatively little information about occupational exposure to lead during pregnancy. This study aims to assess the association between blood lead levels and occupational exposure in pregnant women from Durango, Mexico.
Methods
A cross-sectional study was carried out in a population of 299 pregnant women. Blood lead was measured in 31 women who worked in jobs where lead is used (exposed group) and 268 who did not work in those places (control group). Chi-square test was applied to compare exposed and control groups with regard to blood lead levels. Odds ratio (OR) and 95% confidence intervals (CI) were calculated. Multivariable regression analysis was applied to determine significant predictors of blood lead concentrations in the exposed group.
Results
Exposed women had higher blood lead levels than those in the control group (4.00 ± 4.08 μg/dL vs 2.65 ± 1.75 μg/dL, p = 0.002). Furthermore, women in the exposed group had 3.82 times higher probability of having blood lead levels ≥ 5 μg/dL than those in the control group. Wearing of special workwear, changing clothes after work, living near a painting store, printing office, junkyard or rubbish dump, and washing the workwear together with other clothes resulted as significant predictors of elevated blood lead levels in the exposed group.
Conclusions
Pregnant working women may be at risk of lead poisoning because of occupational and environmental exposure. The risk increases if they do not improve the use of protective equipment and their personal hygiene.
Similar content being viewed by others


Background
Lead has been clearly shown to be a neurotoxic agent widely distributed in the environment [1]. Excessive lead exposure may occur in the workplace. Some jobs that expose people to lead include: mining, smelting, foundry work, construction, plumbing, radiator manufacturing, lead-acid battery recycling, manufacturing of rubber products, and the chemical industry. Years ago, lead was also used regularly in paint, ceramics, and pipe solder among other things. Because of its potential health problems, the amount of lead used in these products today has lessened or has been removed. However, lead is still common in many industries, including construction, mining, and manufacturing [2].
Lead can harm many of the body’s organ systems. Human exposure to lead can result in a wide range of biological effects [3]. It is well known that childhood and pregnancy are the most sensitive population to lead exposure. A pregnant woman with an elevated blood lead concentration may expose her fetus to the toxic effect of lead. Elevated blood lead levels (BLLs) in children cause learning and behavioral deficits [4, 5]. Low-level lead exposure, including prenatal exposure, has been linked to decreased performance on IQ tests for school children [6–9]. Several studies have suggested that any level of exposure is potentially detrimental and no threshold for these effects has been identified [10, 11].
Lead concentrations have declined in the last decades due to the increase in health interventions [12]. In spite of this, lead exposure remains a risk factor for female reproductive health, even at low levels of lead in blood [13]. Once absorbed from the gastrointestinal tract or the respiratory system, lead is transported bound to erythrocytes and accumulates in bone [14]. During pregnancy, calcium demands increase. This leads to increased bone turnover, with a consequential release of lead from bone and increased blood lead levels [15, 16]. Lead can cross the placenta and expose the fetus to the harmful effects of this toxic, thus affecting the embryonic development of multiple organs and causing neurobehavioral impairments in infancy and early childhood [4, 5, 9, 17]. Therefore, pregnancy is considered a critical time for exposure to lead for the mother and the fetus [14, 18].
Over the past several decades there has been a remarkable reduction in environmental sources of lead and a decreasing trend in the prevalence of elevated blood lead levels [2]. However, some reproductive health damages at levels of lead in blood below 10 μg/dL have been reported. Therefore, in recent years, many studies have focused on the health effects at low levels of lead in blood. Low blood lead concentrations in pregnant women have been associated with miscarriage [19, 20], pregnancy hypertension, or preeclampsia [12, 21–24] premature delivery [13], premature rupture of the membranes [25], and low birth weight [26, 27]. On the other hand, it is considered that lead-related toxicity can occur at levels as low as 5 μg/dL [28]. Hence, maternal exposure to lead plays an important role in adverse pregnancy outcomes.
Despite that the workplace offers the greatest potential for lead exposure, there is relatively little information about the occupational exposure to lead during pregnancy. It is necessary to identify sources of lead exposure relevant to this population. Some of the jobs that commonly involve lead exposure are battery manufacture or repair; construction (welding or cutting lead-painted metal); radiator manufacture or repair; wire cable cutting and manufacture, and cable, battery, or scrap metal salvage, plating operations; manufacturing or using leaded paints, dyes or pigments, or lead soldering in the electronics industry, among others [29]. In Mexico, and in other developing countries, it is common to find pregnant women working in places with potential sources of lead exposure. The aim of this study was to assess the association between blood lead levels and occupational exposure in pregnant women from Durango, Mexico.
Methods
Study population
From June 2007 to May 2008 a cross-sectional study was conducted to evaluate the association between BLLs and some risk factors in pregnant women who received health attention in the State of Durango, Mexico [30]. The study population consisted of pregnant women who received medical attention in two sanitary jurisdictions pertaining to the Secretary of Health. The total estimated number of pregnant women seen in these two jurisdictions during a 1 year period was obtained from the Secretariat of Health databases, and the sample required was distributed equally in 12 municipalities. The participants were recruited from Obstetrics and Gynecology Departments of the municipal hospitals. All women who presented for prenatal care on the days that the study team visited, independent of their gestational age, were asked to participate in the study if they met the inclusion criteria. The inclusion criteria were: being pregnant, living in Durango, able to understand Spanish, and receiving health care paid for by the Secretary of Health. Each municipality was visited two or three times during the recruitment period, until the sample size was completed. Of the 337 pregnant women who presented for prenatal care on the days of the visits, 12 women were excluded because they did not live in Durango and 26 declined to participate in the study. A total of 299 women were included in the study (Aditional file 1). The interviewer’s interaction with patients was standardized. All patients gave their informed written consent and answered a set of questions in a face-to-face interview. The research protocol was approved by the Ethical Committee of Durango General Hospital.
First, the group was treated as a cohort. After that, a regression with lead levels as outcome allowed to attribute the proportion of risk from occupational and non-occupational exposure. For assessment of the association between blood lead levels and occupational exposure, subjects were classified into two groups: women who worked in places where lead is used (exposed group) and women who did not work in those places (control group). Women who worked in automotive repair shops, mining laboratories, welding workshops, automotive harness factories, hairdressing salons, and road sweepers were included in the exposed group. Unemployed women and those women who had a job where lead-containing materials are not used, were included in the control group.
Blood lead measurement
Blood samples were collected using lead-free tubes containing EDTA. Samples were stored in the original tube at 4o C before being transferred to the Environmental Toxicology Laboratory, Faculty of Medicine, Juarez University of Durango State. The time between receipt and analysis varied from 1 to 3 weeks. During which time, the specimens were stored refrigerated at 4 °C. Lead concentration was determined by graphite furnace atomic absorption spectrometry. Bovine blood obtained from the National Institute of Standards and Technology (NIST) was used as standard reference material.
Statistical analysis
Data were analyzed to describe demographic characteristics, BLLs, and potential sources of lead exposure. The normality of the variables was tested using the Kolmogorov-Smirnov test. BLLs were log-transformed prior to analysis. Multivariable regression analysis was conducted to determine the proportion of risk from each occupational and non-occupational exposure. After that, the study population was divided into two groups according to occupation (occupationally exposed and non-occupationally exposed). Student t-test was applied for comparison of quantitative variables. Chi-square test was applied to compare exposed and control groups regarding blood lead levels (BLLs ≥ 5 μg/dL vs BLLs < 5 μg/dL). Odds ratio (OR) and 95% confidence intervals were calculated. To identify non-occupational sources of lead exposure for pregnant women we explored the following: the way in which workwear is washed (together with other clothes or alone), use of lead-glazed pottery, use of hair dyes, living near workplaces where lead is used (mining zones, battery workshops, junkyards, rubbish dumps and painting workshops), pica behavior and living with someone who works with lead, in both exposed and control groups. These activities have been documented to be lead-related. Chi-square test was also used to compare both groups regarding non-occupational sources of lead exposure. Student t-test was also used to compare blood lead levels according to some protection habits in the exposed group. Use of respiratory protective equipment, habit of wearing gloves, wearing of special workwear, handwashing before eating, changing clothes after work, and use of any protective equipment were analyzed as dichotomous variables. Finally, backward stepwise multivariable regression analysis was applied to determine significant predictors of blood lead concentrations in the exposed group. A set of variables selected on the basis of previous knowledge or because of associations with lead levels in bivariate analyses (at p < 0.25) were entered into the model. The full model was followed by stepwise backward elimination to determine whether each variable remained significant after non-significant covariates were excluded. All statistical analyses were performed using SPSS for Windows statistical package version 15.0. A p-value < 0.05 was considered statistically significant.
Results
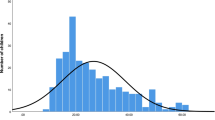
The mean blood lead concentration in the study population was 2.79 μg/dL (SD 2.14), geometric mean 2.38 μg/dL, 95% CI (2.25 – 2.54). Among the 299 pregnant women enrolled in the study, 31 (10.4%) worked in places where lead is used, and 268 (89.6%) did not work where lead-containing materials are used (Table 1). Results of multiple linear regression on association between blood lead levels and risk factors are shown in Table 2. Living in a mine zone was associated with increased blood lead (p = 0.044). However, working in places where lead is used was the main factor associated with blood lead concentration. On the basis of this result, the study population was divided into two groups: exposed and non-exposed.
Table 3 summarizes the main characteristics of both groups. There were no significant differences between the groups regarding age, gestational age, number of pregnancies, body mass index (BMI), hemoglobin and monthly income per person. However, the blood lead concentration of the exposed group was significantly higher than that of the control group (p = 0.002).
Frequency of BLLs ≥ 5 μg/dL is depicted in Table 4. The proportion of women with BLLs ≥ 5 μg/dL in the exposed group was significantly higher compared to the control group (22.6% vs 7.1%; p < 0.01). In addition, women in the exposed group had 3.8 times more probability to have BLLs above 5 μg/dL than those in the control group.
Non-occupational sources of lead exposure for exposed and control groups are summarized in Table 5. The proportion of women who had the habit of dyeing their hair was significantly higher in exposed women when compared to the control group (p = 0.010) and the same was observed in the exposed group regarding living near workplaces where lead is used when compared with control women (p = 0.043). However, there were no significant differences in other variables between the compared groups.
To evaluate the influence of some work conditions on blood lead levels in the exposed group, some protection habits were explored (Table 6). Blood lead levels were significantly higher in women who did not wear special workwear (p = 0.028) and in those who did not have the habit of changing clothes after work (p = 0.025).
Table 7 displays potential sources of blood lead in the exposed group. After multivariable analysis, seven variables were retained in the final model: wearing of special workwear, changing clothes after work, living near a painting store, living near a printing office, living near a junkyard, living near a rubbish dump and washing the workwear together with other clothes. These variables accounted for 86.5% of the total variance. The model was adjusted by age, educational level and gestational age.
Discussion
In this cross-sectional study, we examined the association of blood lead levels with occupational exposure in pregnant women. The blood lead levels in our study population (2.79 ± 2.14 μg/dL) did not exceed the accepted threshold of 10 μg/dL. They are even below the 5 μg/dL recommended by the CDC [31]. Furthermore, the mean blood lead level in our test subjects is lower compared to values reported in some populations of pregnant women. A study by Taylor et al. [14] reported mean BLL of 3.67 ± 1.47 μg/dL in a cohort of pregnant women in The United Kingdom. In China, the lead concentrations during the three pregnancy trimesters and postpartum were 5.95 ± 2.27 μg/dL, 5.51 ± 1.93 μg/dL, 5.57 ± 1.85 μg/dL, and 6.88 ± 1.90 μg/dl; respectively [32]. In addition, Gerhardsson and Lundh [33] reported median blood lead of 11.0 μg/L (range 4.2–79 μg/L) in pregnant females residing in Sweden; and Alvarez et al. [34] found a blood lead average of 11.63 ± 4.64 μg/dL in pregnant women living in the island of Tenerife, Spain. However, some researchers have reported lower blood lead concentrations in pregnant women. Mean blood lead levels of 2.551 ± 2.592 μg/dL were found in pregnant women from Saudi Arabia [35]. In a socioeconomically disadvantaged population of New York, a geometric mean of 1.58 μg/dL was reported by Schell et al. [15]. Moreover, Bakhireva et al. [36] found mean blood lead of 1.06 ± 1.55 μg/dL in a cross-sectional study designed to ascertain risk factors of lead exposure among pregnant women in New Mexico, United States.
In Mexico, the Secretary of Health is the health care institution which attends the smallest workforces. Nevertheless, we found 31 women working in places where lead is used and who represent 10.4% of the recruited subjects. In spite of this, lead in the workplace results a significant determinant of blood lead levels. Therefore, similar results may be expected in other pregnant populations with low income and low level of employment.
Our exposed group was made up of women who worked in automotive repair shops, mining laboratories, welding workshops, automotive harness factories, hairdressing salons, and as road sweepers, regardless of intensity and exposure time. At any rate, we found significantly higher blood lead concentrations in exposed women than in the control group (4.24 ± 4.60 μg/dL vs. 2.66 ± 1.73 μg/dL). Our findings are consistent with a study by Popovic et al. [37], who found mean blood lead of 2.73 ± 2.39 μg/dL in women formerly working in a smelter, and 1.25 ± 2.10 μg/dL in women with no known occupational exposure to lead.
In the present study, no difference was observed in hemoglobin level between exposed women and the control group. This is expected considering the low BLLs obtained for this population. According to previous studies, lead anemia appears at BLLs higher than 40 μg/dL [3, 38]. On the other hand, the US Environmental Protection Agency (EPA) suggests a threshold BLL of 20 – 40 μg/dL for risk of anemia [39]. However, blood lead concentrations in our compared groups are much lower.
Recent findings concerning lead-related adverse reproductive outcomes suggested that pregnant women should avoid lead exposure that would result in blood lead concentrations higher than 5 μg/dL [3]. Among the 299 women included in our study, 26 (8.7%) had BLLs ≥ 5 μg/dL. In a cohort of 4, 285 pregnant women, Taylor et al. [14] reported 14.4% of women with BLLs of 5 μg/dL or higher; cigarette smoking, alcohol, and coffee drinking were found to be predictors of BLLs. However, in our study the frequencies of smoking, alcohol and coffee drinking among the women were very low; therefore, these variables were not included in the analysis. Regarding occupation, the 2005 – 2007 Adult Lead Epidemiology and Surveillance (ALES) by the United States of America Centers for Disease Control and Prevention reported that 32% of women of childbearing age with BLL ≥ 5 μg/dL were occupationally exposed to lead [38]. Zhu et al. [40] evaluated reasons for testing and potential sources of exposure among women, and reported that 29.2% of women with blood lead of 5–14.9 μg/dL had a job with potential lead exposure.
Our results indicated that exposed women were more than 3.8 times likely to have BLLs ≥ 5 μg/dL than non-exposed women. This finding suggests that occupation represents an important factor for elevated blood lead concentrations in our studied population. According to a study by Kosnett et al. [3], it is recommendable for pregnant women to avoid lead exposure that would result in blood lead levels above 5 μg/dL, due to the raised concerns regarding the toxicity of this blood lead concentration. Several studies have associated blood lead levels above 5 μg/dL with miscarriage [19, 20], pregnancy hypertension [12, 21–24, 41], premature delivery [13], premature rupture of the membranes [25], and low birth weight [26, 27]. According to CDC recommendations [28], pregnant women with a current or past BLL ≥5 μg/dL should be assessed for the adequacy of their diet and provided with prenatal vitamins, calcium and iron supplements.
We found a higher proportion of women living near workplaces where lead is used among exposed women compared with the control group. There was also a significant association between the BLLs and the habit of dyeing the hair. Some hair dyes may contain lead and other harmful substances. Our results agree with Marzulli [42] who reported a significant correlation between blood lead and hair lead in people who used lead contained hair dyes. Use of these products by a pregnant woman may harm the health of her unborn child. None of the cited investigations, carried out in an occupational cohort, analyzed non-occupational exposure. However, our findings suggest that the contribution of non-occupational activities must be explored for determining total lead exposure and subsequent health effects.
Occupational lead exposure can occur because of the use of lead material and products. For that reason, employers should provide their employees with adequate working conditions and protection information regarding hazards at their worksites. Exposed workers should use protective equipment and practice personal hygiene, such as showering and changing into clean clothes at the end of the shift [43]. In this study, working women who did not change their clothes after work showed significantly higher blood lead concentration in comparison with those women who had this habit. There was also statistical association of BLLs related to the use of special workwear. It is well known that appropriate workwear can greatly reduce exposure to hazardous substances [44]. In addition, clothing contaminated with lead can be an important route of exposure for pregnant women.
Despite the scientific data and practical considerations regarding the prevention of lead exposure during pregnancy, routine blood lead testing for pregnant women is not established in many countries. Nevertheless, it is the main way to make sure that women have not been affected by lead. Furthermore, some researchers have demonstrated that lead exposure during pregnancy affects children’s physical neonatal development, and available evidence suggests there are no BLLs without risk of health effects [41].
Relatively little is known about the current prevalence, risk factors, and sources of lead poisoning among pregnant women [45]. Our study identified some risk factors associated with blood lead in occupationally exposed women. Despite the growing evidence that relatively low levels of environmental lead exposure may be associated with adverse pregnancy outcomes, there is no specific regulation in existence regarding occupational lead exposure during pregnancy in Mexico. Therefore, it is necessary to improve engineering controls and personal hygiene to reduce the risk of lead exposure during pregnancy. Much work needs to be done to reduce environmental lead exposure. Furthermore, exposed women should undergo blood lead testing to prevent lead poisoning.
We have recognized that our study has several limitations. First, the cross-sectional design did not allow an evaluation of the length and the extent of the exposure. Consequently, all the exposed women were included in a single group, regardless of the time spent in the working place. Longitudinal studies are needed to evaluate the changes in blood lead levels during the exposure time. Second, in our study calcium supplementation, dietary iron intake and indicators of iron status were not measured. It has been documented that low calcium intake may contribute to lead mobilization from the maternal skeleton during pregnancy [46] and that calcium supplementation reduces bone resorption [47] and minimizes release of lead from bone stores with subsequent fetal lead exposure [48, 49]. On the other hand, an inverse relationship between body stores of iron and lead retention has also been observed [50, 51]. Nevertheless, to our knowledge, it is the first study on this topic conducted in occupationally exposed pregnant women in Mexico. Therefore, the results of the present research can be used for comparison with future investigations regarding occupational exposure to lead during pregnancy.
Conclusions
Our results constitute evidence that pregnant women who work in some places where lead products are used may be at risk for presenting higher blood lead levels if they do not use protective equipment and do not practice adequate personal hygiene. The risk increases if women live near some places that are considered sources of lead exposure such as a painting store, a printing office, a junkyard, or a rubbish dump. Additional studies using larger sample sizes and multiple prospective measurements are needed to verify our findings.
Abbreviations
- ALES:
-
Adult lead epidemiology surveillance
- BLLs:
-
Blood lead levels
- BMI:
-
Body mass index
- CDC:
-
Centers for disease control and prevention
- CI:
-
Confidence interval
- EDTA:
-
Ethylenediaminetetraacetic acid
- NIST:
-
National Institute for Standard Technology
- OR:
-
Odds ratio
- SD:
-
Standard deviation
References
Casas JS, Sordo J. An overview of the historical importance, occurrence, isolation, properties and applications of lead. In: Casas JS, Sordo J, editors. Lead: Chemistry, analytical aspects, environmental impact and health effects. Barcelona: Universidad de Santiago de Compostela; 2006. p. 1–40.
Centers for Disease Control and Prevention. Lead. Workplace safety & health topics. 2013. http://www.cdc.gov/niosh/topics/lead/. Accessed 15 Jan 2014.
Kosnett M, Wedeen R, Rothenberg S, Hipkins K, Materna B, Schwartz B, Hu H, Woolf A. Recommendations for Medical Management of Adult Lead Exposure. Environ Health Persp. 2007;115:463–71.
Mostafa G, El-Shahawi H, Mokhtar A. Blood lead levels in Egyptian children from high and low lead-polluted areas: impact on cognitive function. Acta Neurol Scand. 2009;20:30–7.
Roy A, Bellinger D, Hu H, Schwartz J, Ettinger A, Wrigth R, et al. Lead exposure and behavior among young children in Chennai, India. Environ Health Persp. 2009;117:1607–11.
Bellinger DC, Stiles KM, Needleman HL. Low-level lead exposure, intelligence and academic achievement: a long-term follow-up study. Pediatrics. 1992;90(6):855–61.
Canfield R, Henderson C, Cory-Slechta D, Cox C, Jusko T, Lanphear B. Intellectual impairment in children with blood lead concentrations below 10 μg per deciliter. New Engl J Med. 2003;348:1517–26.
Chiodo L, Jacobson S, Jacobson J. Neurodevelopmental effects of postnatal lead exposure at very low levels. Neurotoxico Teratol. 2004;26:359–71.
Schnaas L, Rothenberg SJ, Flores MF, Martinez S, Hernandez C, Osorio E, et al. Reduced intellectual development in children with prenatal lead exposure. Environ Health Persp. 2006;114:791–7.
Schwartz J. Low-level lead exposure and children’s IQ: a meta-analysis and search for a threshold. Environ Res. 1994;65:42–55.
Lanphear B, Hornung R, Khoury J, Yolton K, Baghurst P, Bellinger D, et al. Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. Environ Health Persp. 2005;113:894–9.
Sowers M, Jannausch M, Scholl T, Li W, Kemp F, Bogden J. Blood lead concentrations and pregnancy outcomes. Arch Environ Health. 2002;57:489–95.
Cantonwine D, Hu H, Sanchez B, Lamadrid-Figueroa H, Smith D, Ettinger A, et al. Critical Windows of Fetal Lead Exposure: Adverse Impacts on Length of Gestation and Risk of Premature Delivery. J Occup Environ Med. 2010;52:1106–11.
Taylor CM, Golding J, Hibbeln J, Emond AM. Environmental factors predicting blood lead levels in pregnant women in the UK: The ALSPAC Study. PLoS ONE. 2013;8(9):1–8.
Schell L, Denham M, Stark A, Gomez M, Ravenscroft J, Parsons P, et al. Maternal blood lead concentration, diet during pregnancy, and anthropometry predict neonatal blood lead in a socioeconomically disadvantaged population. Environ Health Persp. 2003;111:195–200.
Téllez-Rojo M, Hernandez-Avila M, Lamadrid-Figueroa H, Smith D, Hernandez-Cadena L, Mercado A, et al. Impact of bone lead and bone resorption on plasma and whole blood lead levels during pregnancy. Am J Epidemiol. 2004;160:668–78.
Bellinger D, Sloman J, Leviton A, Rabinowitz M, Needleman HL, Waternaux C. Low-level lead exposure and children’s cognitive function in the preschool years. Pediatrics. 1991;87(2):219.
Amaral J, Rezende V, Quintana S, Gerlach R, Barbosa J, Tanus-Santos J. The relationship between blood and serum lead levels in peripartum women and their respective umbilical cords. Basic Clin Pharmacol Toxicol. 2010;107:971–5.
Borja-Aburto V, Hertz-Picciotto I, Lopez M, Farias P, Rios C, Blanco J. Blood lead levels measured prospectively and risk of spontaneous abortion. Am J Epidemiol. 1999;150:590–7.
Lamadrid-Figueroa H, Téllez-Rojo M, Hernández-Avila M, Trejo-Valdivia B, Solano-González M, Mercado-García A, et al. Association between the plasma/whole blood lead ratio and history of spontaneous abortion: a nested cross-sectional study. BMC Pregnancy Childb. 2007;7:22–9.
Vigeh M, Yokoyama K, Mazaheri M, Beheshti S, Ghazizadeh S, Sakai T, et al. Relationship between increased Blood Lead and Pregnancy Hypertension in Women without Occupational Lead Exposure in Tehran, Iran. Arch Environ Health. 2004;59:70–5.
Vigeh M, Yokoyama K, Ramezanzadeh F, Dahaghin M, Sakai T, Morita Y, et al. Lead and other trace metals in preeclampsia: a case-control study in Tehran, Iran. Environ Res. 2006;100:268–75.
Wells E, Navas-Acien A, Herbstman J, Apelberg B, Silbergeld E. Caldwell, et al. Low-level lead exposure and elevations in blood pressure during pregnancy. Environ Health Persp. 2011;119:664–9.
Yazbeck C, Thiebaugeorges O, Moreau T, Goua V, Debotte G, Sahuquillo J, et al. Maternal blood lead levels and the risk of pregnancy-induced hypertension: The EDEN cohort study. Environ Health Persp. 2009;117:1526–30.
Vigeh M, Yokoyama K, Shinohara A, Afshinrokh M, Yunesian M. Early pregnancy blood lead levels and the risk of premature rupture of the membranes. Reprod Toxicol. 2010;30:477–80.
Jelliffe-Pawlowski L, Miles S, Courtney J, Materna B, Charlton V. Effect of magnitude and timing of maternal pregnancy blood lead (Pb) levels on birth outcomes. J Perinatol. 2006;26:154–62.
Zhu M, Fitzgerald E, Gelberg K, Lin S, Druschel C. Maternal low-level lead exposure and fetal growth. Environ Health Persp. 2010;118:1471–5.
Centers for Disease Control and Prevention. Guidelines for the identification and management of lead exposure in pregnant and lactating women. 2010. http://www.cdc.gov/nceh/lead/publications/leadandpregnancy2010.pdf. Accessed 20 Jan 2012.
Swaran F, Bovinder F, Geetu S. Environmental occurrence, health effects and management of lead poisoning. 2006. In Casas, J, Sordo J, editors. Lead. Chemistry, analitical aspects, environmental impact and health effects; 2006. p. 158-228.
La-Llave-León O, Estrada-Martínez S, Salas-Pacheco JM, Peña-Elósegui R, Duarte-Sustaita J, Candelas Rangel JL, et al. Blood lead levels and risk factors in pregnant women from Durango, Mexico. Arch Environ Occup H. 2011;66:107–13.
Centers for Disease Control and Prevention. Response to the Advisory Committee on Childhood Lead Poisoning Prevention Report, Low Level Lead Exposure Harms Children: A Renewed Call for Primary Prevention. MMWR: Morbidity & Mortality Weekly Report. 2012;61(20):383
Jiang Y, Wang H, Chen J, Zhang G, Chen L, Dai W, et al. Blood lead levels during different trimesters of pregnancy and the possible influencing factors in Chengdu, China. Biol Trace Elem Res. 2011;144:27–35.
Gerhardsson L, Lundh T. Metal concentrations in blood and hair in pregnant females in Southern Sweden. J Environ Health. 2010;72(6):37–41.
Alvarez J, Gutiérrez A, Troyano-Luque J, Rubio C, González-Weller D, Hardisson A. Lead and cadmium in the amniotic fluid of pregnant women in Canary Islands. Trace Elem and Electroly. 2013;30:35–40.
Al-Saleh I, Shinwari N, Mashhour A, Rabah A. Birht outcomes measures and maternal exposure to heavy metals (lead, cadmium and mercury) in Saudi Arabian population. Int J Hyg Envir Heal. 2013;217:205–18.
Bakhireva L, Rowland A, Young B, Cano S, Phelan S, Artyushkova K, et al. Sources of potential lead exposure among pregnant women in New Mexico. Matern Child Hlth J. 2013;17:172–9.
Popovic M, McNeill F, Chettle D, Webber C, Lee C, Kaye W. Impact of occupational exposure on lead levels in women. Environ Health Persp. 2005;113:478–84.
Hipkings KL, Kosnett MJ. Lead poisoning. In: Bowlerand R, Cone J, editors. Occupational medicine secrets. Philadelphia, PA: Hanley & Belfus; 2006. p. 60–70.
Committee on Potential Health Risks from Recurrent Lead Exposure of DOD Firing-Range Personnel; Committee on Toxicology; Board on Environmental Studies and Toxicology; Division on Earth and Life Studies; National Research Council. Potential Health Risks to DOD Firing-Range Personnel from Recurrent Lead Exposure. Washington (DC): National Academies Press (US); 2012 Dec 3. 4, Noncancer Health Effects. https://www.ncbi.nlm.nih.gov/books/NBK206965/. Accessed 19 June 2013.
Centers for Disease Control and Prevention. Lead exposure among females of childbearing age - United States, 2004. Morb Mortal Wkly Rep. 2007;56(16):397–400.
Zhu M, Fitzgerald E, Gelberg K. Exposure sources and reasons for testing among women with low blood lead levels. Int Enviro Heal R. 2011;21:286–93.
Rothenberg S, Manalo M, Jian J, Khan F, Cuellar R, Reyes S, et al. Maternal blood lead level during pregnancy in South Central Los Angeles. Arch Environ Health. 1999;54:151–7.
Marzulli FN, Watlington PM, Maibach HI. Exploratory skin penetration findings relating to the use of lead acetate hair dyes. Hair as a test tissue for monitoring uptake of systemic lead. Curr Probl Dermatol. 1978;7:196–204.
Occupational Safety and Health Administration Protecting workers for lead hazards. 2005. https://www.osha.gov/OshDoc/data_Hurricane_Facts/LeadHazards.pdf. Accessed 18 Feb 2012.
Reynolds SJ, Seem R, Fourtes LJ, Sprince NL, Johnson J, Walkner L, et al. Prevalence of elevated blood lead and exposure to lead in construction trades in Iowa and Illinois. Am J Ind Med. 1999;36:07–16.
Klitzman S, Sharma A, Nicaj L, Vitkevich R, Leighton J. Lead poisoning among pregnant women in New York City: risk factors and screening practices. J Urban Health. 2002;79:225–37.
Janakiraman V, Ettinger A, Mercado-Garcia A, Hu H, Hernandez-Avila M. Calcium supplements and bone resorption in pregnancy: A randomized crossover trial. Am J Prev Med. 2003;24:260–4.
Ettinger A, Lamadrid-Figueroa H, Mercado-García A, Kordas K, Wood R, Peterson K, et al. Effect of calcium supplementation on bone resorption in pregnancy and the early postpartum: a randomized controlled trial in Mexican Women. Nutr J. 2014;13:49–67.
Gomaa A, Hu H, Bellinger D, Schwartz J, Tsaih S, Gonzalez-Cossio T, et al. Maternal bone lead as an independent risk factor for fetal neurotoxicity: a prospective study. Pediatrics. 2002;110:110–8.
Jackson L, Cromer B, Panneerselvamm A. Association between bone turnover, micronutrient intake, and blood lead levels in pre- and postmenopausal women, NHANES 1999-2002. Environ Health Persp. 2010;118:1590–6.
Wang H, Shi H, Chang L, Zhang X, Li J, Yang Y, et al. Association of blood lead with calcium, iron, zinc and hemoglobin in children aged 0-7 years: A large population-based study. Biol Trace Elem Res. 2012;149:143–7.
Acknowledgments
The authors are grateful to laboratory technicians, managers and researchers, who contributed to the completion of the present research. The authors would also like to thank Mr. Miranda Morales E.G. for the careful reading of the manuscript.
Funding
This study was supported by grant no. DGO-2006-C01-4490 from the Council of Science and Technology for the State of Durango (COCYTED), Mexico.
Availability of data and material
All data analyzed during this study are included in this published article, in the Additional file 1: DatabasePb.xls.
Authors’ contributions
OLLLL designed the study, participated in the elaboration of the questionnaire, prepared the background, results and discussion sections, as well as part of the methods sections, JMSP participated in the elaboration of the questionnaire, he was the field supervisor and contributed to the discussion of results, SEM collaborated in the statistical analysis and interpretation of results, EER carried out part of the literature review, participated in the process of data collection and contributed to the discussion and interpretation of results, FXCJ contributed to the discussion and interpretation of results and prepared part of the results and discussion sections, ASC participated in the elaboration of the questionnaire, in the process of data collection and critically reviewed the manuscript, AMLQ participated in the design of the questionnaire, carried out part of the literature review and collaborated to the interpretations of results, FVA collaborated in the statistical analysis and interpretation of results, EMMH contributed to the discussion of the findings, she also contributed in drafting and writing of the manuscript, GGV supervised the procedures for blood lead measurements and contributed to the discussion of the findings. JDS contributed with blood lead measurements, interpreting the results, and providing critical comments. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was approved by the Ethical Committee of Durango General Hospital. All participants gave their informed written consent before being enrolled.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
Database: Blood lead levels in pregnant women from Durango, Mexico. (XLS 733 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
La-Llave-León, O., Salas Pacheco, J.M., Estrada Martínez, S. et al. The relationship between blood lead levels and occupational exposure in a pregnant population. BMC Public Health 16, 1231 (2016). https://doi.org/10.1186/s12889-016-3902-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-016-3902-3