
Abstract
Background
Increased folic acid has been found to be latently protective against gynecological infection, including several kinds of vaginosis. In this study, we laid emphasis on whether RBC (Red Blood Cell) folate was associated with the infectious ratio of Trichomonas vaginalis, a kind of anaerobic parasitic protozoan.
Methods
We set RBC folate as the exposure variable and Trichomonas vaginalis as the outcome variable. Other subsidiary variables were regarded as covariates that may work as potential effect modifiers. The cross-sectional study was conducted with two merged waves of the National Health and Nutrition Examination Survey (NHANES) from 2001 to 2004, and a sample of 1274 eligible women (1212 negative and 62 positive in Trichomonas vaginalis infection) was integrated for the exploration of the association between RBC folate and Trichomonas vaginalis infection. Multivariate regression analyses, subgroup analyses, and subsequent smooth curve fittings were conducted to estimate the relationship between RBC folate and Trichomonas vaginalis in women.
Results
In the multivariable logistic regression analyses, a negative association was observed between stratified RBC folate status and Trichomonas vaginalis infection with all confounders adjusted. Referencing the lowest RBC folate concentration quartile, the higher concentration quartiles reported a relatively lower infection ratio, while there was a weak correlation between total RBC folate concentration and T. vaginalis (Trichomonas vaginalis) infection. In subgroup analyses stratified by BMI and age, this association was only found significant in high age and BMI groups.
Conclusions
The cross-sectional study indicated a negative association between RBC folic acid and Trichomonas vaginalis infection, and latent effects of BMI and age on the association were also found.
Similar content being viewed by others


Background
The pathology of Trichomoniasis is due to the damage to host epithelial cells by various processes during the infection, and its clinical manifestations also vary between men and women. 50 percent of women infected with Trichomonas vaginalis develop symptoms, and about 30 percent of asymptomatic cases develop itching and pain during sexual intercourse and secretion with foam 6 months after infection, while male infected people are generally asymptomatic, but they have mild urethritis, epididymitis and prostatitis [1, 2]. According to the World Health Organization (WHO), the global prevalence of Trichomoniasis in women is estimated at 5.3%, there were 156 million new cases of trichomoniasis in 2016 [3, 4], suggesting that Trichomonas vaginalis infection is a prevalent sexually transmitted disease [5]. It should be noted that asymptomatic Trichomonas vaginalis infection can be frequently found in women, causing misjudgment of its prevalence, which could interrupt the accurate diagnosis procedure [6]. Recent studies revealed associations between Trichomonas vaginalis infection and cervical cancer, pelvic inflammatory disease, adverse pregnancy, infertility, and transmission of HIV-1 [3, 7,8,9], making it a public health concern to investigate factors influencing T. vaginalis infection.
Folate is an essential trace element in the human body. It is involved in various metabolic activities and plays a vital role in the process of DNA methylation, biological metabolic transformation, cell proliferation, and differentiation [10]. Folic acid is a water-soluble vitamin, but humans cannot synthesize it alone. The concentration of folate in red blood cells (RBC) is an indicator of the body’s long-term folate status. Therefore, the major objective was to collect and analyze relevant data from the NHANES survey (2001–2004) among women of all races and explore the potential association.
Methods
Study population
The National Health and Nutrition Examination Survey (NHANES) is a program of studies designed to assess the health and nutritional status of adults and children in the United States and was conducted by the National Center of Health Statistics (NCHS) at the Centers for Disease Control and Prevention (CDC), providing us with a wealth of information about the nutrition and health of Americans through the use of multiple phases, probability sampling design and coding variables with the information collected concerning health and nutrition-related domains [11].
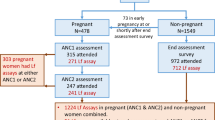
On the basis that the outcome variable, T. vaginalis infection was only coded in two circles of NHANES, we chose to merge the two circles, 2001–2002 and 2003–2004, and then conducted subsequent research. The flow chart for the inclusion and exclusion is shown in Fig. 1. With T. vaginalis infection and RBC folate uninterpreted and missing data (n = 18,407) were first excluded, then other variables including educational status, PIR (Poverty Income Ratio), alcohol use status, serum or plasma cholesterol, calcium dietary intake, BMI, and alcohol consumption missing data (n = 1481) dislodged, 1274 eligible women left were included in our analysis, whose baseline characteristics are shown in Table 1. The raw data and the filtered data were attached as Additional file 1 and 2.

Flow chart of participant enrollment. Flow chart of participant enrollment for the analysis from the National and Nutrition Examination Survey 2001–2004 dataset
Variables and covariates
The exposure variable was red blood cell folate, and the outcome variable was T. vaginalis infection. Erythrocyte folate was measured by collecting samples that were sent to the CDC’s National Centre for Environmental Health (NCEH) for analysis using a microbiological assay [12]. The samples were first diluted 1:11 with a solution of 1 g/dL ascorbic acid in water and either incubated for 90 min prior to assay or frozen immediately for later assay. The 90-min incubation or the freeze–thaw is necessary for hemolysis of the red blood cells, either allows the endogenous folate conjugates to hydrolyze the conjugated pteryl polyglutamates prior to assay. The sample is further diluted 1:2 with a protein diluent (human serum albumin), resulting in a matrix similar to that of the standards and serum samples. T. vaginalis infectious status was detected by performing PCR with primers from a region of the 18S rRNA gene that produce a 312 base pair product. By using hybridization, product specificity was validated with digoxigenin-labeled probes according to the method described in Boehringer Mannhein’s Genius System User Guide for Filter Hybridization. In particular, alcohol use status was categorized into nondrinker, moderate alcohol use, and heavy alcohol use through the criteria on daily alcohol consumption, which was defined by Ratten et al. [13], while the uncategorized alcohol consumption, i.e. average alcoholic beverage per day was adjusted in the analyses as a continuous covariate instead of the status to avoid the bias caused by classification. Except for the alcohol use status, methods of coding confounders are described in detail in the Data files, coding manuals, and frequencies for the National Health and Nutrition Survey, available at www.cdc.gov/Nchs/Nhanes, where acquisition processes on the variables and covariates are available.
Statistical analysis
All statistical analyses were carried out using the R package (www.R-project.org) and EmpowerStats software. In Table 1, the Kolmogorov‒Smirnov test was used to verify the normality of the distribution of continuous variables. Normality values were described as means with standard deviations and compared between the positive and negative groups using one-way ANOVA. With regard to abnormal ones, they were reported as median with interquartile range and compared using the independent-samples Kruskal‒Wallis test. Categorical variables were described as numbers with frequencies and compared using the chi-square test.
Folate in RBCs was stratified into quartiles: Q1 (70–203 ng/ml), Q2 (204–257 ng/ml), Q3 (258–328 ng/ml) and Q4 (329–1022 ng/ml). With the objective of determining the independent association between RBC folate and T. vaginalis infection and whether the correlation differed by BMI and age was analyzed by multivariate logistic regression and subgroup analysis stratified by BMI and age. Meanwhile, three models were introduced to enhance the credibility: Unadjusted model, Model I (covariates including age, PIR (Poverty Income Ratio), BMI (Body Mass Index), race, dietary calcium intake and alcohol consumption were adjusted), and Model II (covariates including age, PIR, BMI, race, dietary calcium intake, serum or plasma cholesterol, educational status, marital status and alcohol consumption were adjusted). Odds ratio of Trichomonas vaginalis infection was deemed as the major endpoint, which was calculated via the comparison between the infected and the uninfected groups, reflecting the various profiles of the infection rate along with the changing of the exposure. To refrain from arbitrary categorization, smooth fitting curves and generalized additive models were conducted for both overall regression analyses and subgroup analyses, validating the association between continuous overall RBC folate and T. vaginalis infection ratio. All P values were calculated, and we regarded P < 0.05 as the criterion to indicate statistical significance.
Results
Characteristics of enrolled participants
The baseline characteristics of 1274 participants subclassified by T. vaginalis infection status are shown in Table 1, among which, by analyzing the P value, specific characteristics that showed significant differences in the prevalence of the disease were summarized, including RBC folate, BMI, age, PIR, marital status, education status and alcohol consumption (P < 0.05 for each). On average, participants were 33.93 years of age and 27.87 kg/m2 for BMI, Compared with the uninfected group, the infected ones tended to be lower income, less calcium intake, more labile marital status, less educational, and consume more alcoholic beverages. Sex was excluded from the table because the participants stretched from the dataset from 2001 to 2004 were all women.
Association between RBC folate and Trichomonas vaginalis infection
To indicate the association between RBC folate and T. vaginalis infection, multivariate regression analyses and subgroup analyses stratified by BMI and age were performed. The results are shown in Tables 2 and 3.
Judging from the multivariate regression analyses, we found a weak correlation between the exposure and outcome variables whether the confounders were adjusted or not (Unadjusted: OR = 0.99 (95% CI 0.99, 1.00) P value < 0.0001, Model I: OR = 0.99 (95% CI 0.99, 1.00) P value = 0.0003, Model II: OR = 0.99 (95% CI 0.99, 1.00) P value = 0.0019). RBC folic acid was converted into quartiles: Q1 (70–203 ng/ml), Q2 (204–257 ng/ml), Q3 (258–328 ng/ml), and Q4 (329–1022 ng/ml). A significantly lower odds ratio of T. vaginalis infection was found in Q3 and Q4 in all confounding variables adjusted model (Model II) when compared with Q1, the reference quantile, which reveals a significant negative association between RBC folate and T. vaginalis infection (Q2: OR = 0.68 (95% CI 0.36, 1.28), P value = 0.2289, Q3: OR = 0.20 (95% CI 0.07, 0.55) P value = 0.0018, Q4: OR = 0.39 (95% CI 0.17, 0.92) P value = 0.0305). As shown in Fig. 2, smooth curve fitting and generalized additive models focusing on overall RBC folate and T. vaginalis infection ratio confirmed the linear negative association (Plinearity = 0.0007). Judging from the graph, a more significant negative correlation was found in participants with relatively lower RBC folic acid concentrations. With increasing RBC folate concentration, the negative relevance became weaker.

Correlation between RBC folate and T. vaginalis infection. The natural spline curve indicates the linear association between RBC folate and the T. vaginalis infection ratio (Plinearity = 0.0007). The area between the dotted blue lines is regarded as a 95% confidential interval. Each red point reveals the concentration of RBC folate, forming a continuous fitting curve. Ratios are based on model II in multivariate logistic regression models, with all confounders (age, PIR, BMI, race, dietary calcium intake, serum or plasma cholesterol, education status, alcohol consumption and marital status) adjusted
Subgroup analyses and smooth curve fitting models stratified by age and BMI were conducted to further address the modifying effect of potential confounders. Reference as Q1, significant negative correlations between RBC folate and T. vaginalis infection were also observed Q3 and Q4 in elder group (age > 35 years old, Q2: OR = 0.74 (95% CI 0.31, 1.72) P value = 0.4789, Q3: OR = 0.05 (95% CI 0.01, 0.44) P value = 0.0068, Q4: OR = 0.31 (95% CI 0.10, 0.93) P value = 0.0363) and high BMI group (BMI > 26.505 kg/m2, Q2: OR = 0.64 (95% CI 0.30, 1.39) P value = 0.2635, Q3: OR = 0.20 (95% CI 0.06, 0.64) P value = 0.0065, Q4: OR = 0.30 (95% CI 0.11, 0.83) P value = 0.0199), while weak evidence sustains a significant correlation in youngsters group (age ≤ 35) and low BMI group (BMI ≤ 26.505 kg/m2), as detailed in Table 3. Intuitive graphs of curve fittings are shown in Figs. 3 and 4, in accordance with the subgroup results with RBC folate in quartiles (Plinearity for age ≤ 35 = 0.1929, Plinearity for age > 35 = 0.0039, Plinearity for BMI ≤ 26.505 = 0.1689 and Plinearity for BMI ≤ 26.505 = 0.0022).

Correlation between RBC folate and T. vaginalis infection stratified by age. Fitting curve of the association between RBC folate and T. vaginalis infection, stratified by age, with age = 35 taken as the dividing criterion. Age, PIR, BMI, race, dietary calcium intake, serum or plasma cholesterol, education status, alcohol consumption and marital status were adjusted

Correlation between RBC folate and T. vaginalis infection stratified by BMI. The fitting curve of the association between RBC folate and T. vaginalis infection, stratified by BMI, with BMI = 26.505 taken as the dividing criterion. Age, PIR, BMI, race, dietary calcium intake, serum or plasma cholesterol, education status, alcohol consumption and marital status were adjusted
Discussion
In the cross-sectional analysis of two merged datasets from 2001 to 2004 NHANES surveys, our study found a significant negative correlation between RBC folate concentrations and Trichomonas vaginalis infection, based on the outcomes of multivariate regression models, with folic acid converted. Subgroup analyses stratified by potential confounders were conducted to better meet the STROBE statement requirements [14]. It was observed that the increase of RBC folic acid concentration was related to the decrease of the possibility of parasitism with Trichomoniasis vaginalis. Recently, Naderi, et al. systematically demonstrated that supplementary folate is nutritionally essential for the support of optimal human health and development [15]. In previous studies, low folate was associated with impaired T cells, and folate deficiency was associated with an increased risk of bacteriuria in pregnancy [16, 17]. Nevertheless, it can be challenging to further verify our conclusions with previous analyses because few studies have focused on the latent association between RBC folate and T. vaginalis infection. Based on the in vivo folate status of 308 female participants, Janet et al. demonstrated that folate concentration is significantly and independently associated with HR-HPV infection [18]. Another cross-sectional study also showed a synergistic effect of low serum folate with HR-HPV infection in the process of cervical carcinogenesis [19]. Other published studies explored the association between folic acid and gynecological diseases20,21,22,23,24 . It ought to be noted that there exist studies supporting folate work as a protective factor in B. vaginosis, which is another kind of vaginosis. One population-based study found that increased dietary folate may reduce the risk of severe B. vaginosis [25], while another study examining women enrolled in the Nashville Birth Cohort (2003–2006) reported a significant atrichossociation between folate deficiencies and B. vaginosis [26]. Thus, addressing health problems of women’s folate status may provide the rationale to decrease the infectious ratio of Trichomonas vaginalis infection, the homogeneous vaginosis.
The research analyzed representative data from the NHANES database, which employed standardized protocols. According to the current research status, our study is a pioneering observational study examining the relationship between RBC folic acid and Trichomonas vaginalis infection. This also has limitations. First, our study is observational and cross-sectional. We cannot validate whether higher RBC folate levels influence changes in Trichomonas vaginalis over time. The casual relationship between them is not clear. Therefore, carefully prospective studies with large samples are needed to verify the concrete mechanism of the association between RBC folate concentration and T. vaginalis Additionally, due to the possibility of causing the gastrointestinal side effects of anti-parasite drugs, it is potential that participants may alter their B-vitamin status through nutritional supplements [27]. Third, there was concern that there were also male patients infected with T .vaginalis, and more complete data are demanded to broaden the study [28]. Last, we did not adjust for other variables, and the participants in the dataset were limited to 2001–2004 due to the subsequent circles recorded by NHANES did not include T .vaginalis infection status, the independent variable. Therefore, other potential confounding factors and biases caused by the passage of time cannot be excluded.
Conclusions
The authors demonstrated a negative association between RBC folate and Trichomonas vaginalis infection among representative women of the US. Meanwhile, the benefits of supplementary folate intake might be more significantly reported in older adults and ones equipped with higher body mass indexes. Apart from the general treatment for patients infected with Trichomonas vaginalis, a high-folic diet can be recommended additionally by clinicians (e.g. ascended proportion of green leafy vegetables, fruits, and bean products).
Abbreviations
- RBC:
-
Red Blood Cell
- T. vaginalis :
-
Trichomonas vaginalis
- NHANES:
-
National Health and Nutrition Examination Survey
- IQR:
-
Interquartile range
- SD:
-
Standard deviation
- PIR:
-
Poverty Income Ratio
- BMI:
-
Body Mass Index
- CI:
-
Confidence interval
- B. vaginosis :
-
Bacterial vaginosis
References
Secor WE. Trichomonas vaginalis: treatment questions and challenges. Expert Rev Anti Infect Ther. 2012;10(2):107–9. https://doi.org/10.1586/eri.11.159.
Yang S, Zhao W, Wang H, Wang Y, Li J, Wu X. Trichomonas vaginalis infection-associated risk of cervical cancer: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2018;228:166–73. https://doi.org/10.1016/j.ejogrb.2018.06.031.
Rowley J, Vander Hoorn S, Korenromp E, et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ. 2019;97(8):548-562P. https://doi.org/10.2471/BLT.18.228486.
Mirzadeh M, Olfatifar M, Eslahi AV, et al. Global prevalence of Trichomonas vaginalis among female sex workers: a systematic review and meta-analysis. Parasitol Res. 2021;120(7):2311–22. https://doi.org/10.1007/s00436-021-07216-6.
Tompkins EL, Beltran TA, Gelner EJ, Farmer AR. Prevalence and risk factors for Trichomonas vaginalis infection among adults in the US, 2013–2014. PLoS ONE. 2020;15(6): e0234704. https://doi.org/10.1371/journal.pone.0234704.
Mercer F, Johnson PJ. Trichomonas vaginalis: pathogenesis, symbiont interactions, and host cell immune responses. Trends Parasitol. 2018;34(8):683–93. https://doi.org/10.1016/j.pt.2018.05.006.
Kissinger P, Adamski A. Trichomoniasis and HIV interactions: a review. Sex Transm Infect. 2013;89(6):426–33. https://doi.org/10.1136/sextrans-2012-051005.
Davis A, Dasgupta A, Goddard-Eckrich D, El-Bassel N. Trichomonas vaginalis and human immunodeficiency virus coinfection among women under community supervision: a call for expanded T. vaginalis screening. Sex Transm Dis. 2016;43(10):617–22. https://doi.org/10.1097/OLQ.0000000000000503.
Salawu OT, Esume CN. Frequency of human immunodeficiency virus (HIV) in Trichomonas vaginalis infected women in Badagry, Lagos, Nigeria. J Reprod Infertil. 2016;17(1):61–3.
Chan YM, Bailey R, O’Connor DL. Folate. Adv Nutr. 2013;4(1):123–5. https://doi.org/10.3945/an.112.003392.
McClelland RS. Trichomonas vaginalis infection: can we afford to do nothing? J Infect Dis. 2008;197(4):487–9. https://doi.org/10.1086/526498.
Curtin LR, Mohadjer LK, Dohrmann SM, et al. The national health and nutrition examination survey: sample design, 1999–2006. Vital and health statistics. Series 2, Data evaluation and methods research. 2012;(155):1–39.
Rattan P, Penrice DD, Ahn JC, et al. Inverse association of telomere length with liver disease and mortality in the US population. Hepatol Commun. 2022;6(2):399–410. https://doi.org/10.1002/hep4.1803.
von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–7. https://doi.org/10.1016/S0140-6736(07)61602-X.
Naderi N, House JD. Recent developments in folate nutrition. Adv Food Nutr Res. 2018;83:195–213. https://doi.org/10.1016/bs.afnr.2017.12.006.
Dhur A, Galan P, Hercberg S. Folate status and the immune system. Prog Food Nutr Sci. 1991;15(1–2):43–60.
Courtemanche C, Elson-Schwab I, Mashiyama ST, Kerry N, Ames BN. Folate deficiency inhibits the proliferation of primary human CD8+ T lymphocytes in vitro. J Immunol. 2004;173(5):3186–92. https://doi.org/10.4049/jimmunol.173.5.3186.
Flatley JE, McNeir K, Balasubramani L, et al. Folate status and aberrant DNA methylation are associated with HPV infection and cervical pathogenesis. Cancer Epidemiol Biomark Prev. 2009;18(10):2782–9. https://doi.org/10.1158/1055-9965.EPI-09-0493.
Zhao W, Hao M, Wang Y, et al. Association between folate status and cervical intraepithelial neoplasia. Eur J Clin Nutr. 2016;70(7):837–42. https://doi.org/10.1038/ejcn.2016.35.
Hernandez BY, McDuffie K, Wilkens LR, Kamemoto L, Goodman MT. Diet and premalignant lesions of the cervix: evidence of a protective role for folate, riboflavin, thiamin, and vitamin B12. Cancer Causes Control. 2003;14(9):859–70. https://doi.org/10.1023/b:caco.0000003841.54413.98.
Zhou X, Meng Y. Association between serum folate level and cervical cancer: a meta-analysis. Arch Gynecol Obstet. 2016;293(4):871–7. https://doi.org/10.1007/s00404-015-3852-5.
Bai LX, Wang JT, Ding L, et al. Folate deficiency and FHIT hypermethylation and HPV 16 infection promote cervical cancerization. Asian Pac J Cancer Prev. 2014;15(21):9313–7. https://doi.org/10.7314/apjcp.2014.15.21.9313.
Wang Z, Wang W, Zhao W, et al. Folate inhibits miR-27a-3p expression during cervical carcinoma progression and oncogenic activity in human cervical cancer cells [published correction appears in Biomed Pharmacother. 2020 May;125:109981]. Biomed Pharmacother. 2020;122: 109654. https://doi.org/10.1016/j.biopha.2019.109654.
Wang W, Yang A, Zhang H, et al. Associations of RBC and serum folate concentrations with cervical intraepithelial neoplasia and high-risk human papillomavirus genotypes in female Chinese adults. J Nutr. 2022;152(2):466–74. https://doi.org/10.1093/jn/nxab396.
Neggers YH, Nansel TR, Andrews WW, et al. Dietary intake of selected nutrients affects bacterial vaginosis in women. J Nutr. 2007;137(9):2128–33. https://doi.org/10.1093/jn/137.9.2128.
Dunlop AL, Taylor RN, Tangpricha V, Fortunato S, Menon R. Maternal vitamin D, folate, and polyunsaturated fatty acid status and bacterial vaginosis during pregnancy. Infect Dis Obstet Gynecol. 2011;2011: 216217. https://doi.org/10.1155/2011/216217.
Ponziani FR, Cazzato IA, Danese S, et al. Folate in gastrointestinal health and disease. Eur Rev Med Pharmacol Sci. 2012;16(3):376–85.
Edwards T, Burke P, Smalley H, Hobbs G. Trichomonas vaginalis: clinical relevance, pathogenicity and diagnosis. Crit Rev Microbiol. 2016;42(3):406–17. https://doi.org/10.3109/1040841X.2014.958050.
Acknowledgements
The authors appreciate the time and effort given by participants during the data collection phase of the NHANES project. Thanks to Zhang Jing (Shanghai Tongren Hospital) for his work on the NHANES database. His outstanding work, nhanesR package and webpage, makes it easier for us to explore NHANES database.
Funding
The study did not receive any funding.
Author information
Authors and Affiliations
Contributions
LWZ contributed to data collection, analysis, study design, and manuscript writing. ZZY, MJH, WZX, HYM, LYF, and ZQR contributed to the writing of the manuscript, and GXG contributed to the project design and administration. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The ethical review committee of the National Centre for Health Statistics approved all NHANES protocols and written informed consent was obtained from all participants. All the additional materials, including protocol numbers, are available to be found here https://www.cdc.gov/nchs/nhanes/about_nhanes.htm. The authors confirmed that the whole procedure of the study was conducted under Protocol #98-12, which is available at https://www.cdc.gov/nchs/nhanes/irba98.htm.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Raw data of all recruited participants from NHANES 2001–2004. Data stretched from NHANES 2001–2004 datasets, containing all the needed variables for subsequent analyses from the participants recruited.
Additional file 2.
Filtered data of the participants enrolled in the study. Data after excluding missing or uninterpreted data from the raw data for variables required for subsequent analyses.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liao, WZ., Zhou, ZY., Mao, JH. et al. Association between red blood cell folate and Trichomonas vaginalis infection among women. BMC Infect Dis 23, 48 (2023). https://doi.org/10.1186/s12879-022-07950-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-022-07950-x