
Abstract
Background
Food sIgG and sIgG4 are highly individually versatile. We put a hypothesis that one of the responsible factors is the presence of gastrointestinal inflammatory diseases. The objectives were: 1. An analysis of wheat and rice sIgG and sIgG4 in healthy children, children with IgE-mediated wheat allergy (WA), coeliac disease (CD) and Helicobacter pylori infection (HP). 2. Usability of wheat sIgG and sIgG4 in the WA diagnostics.
Methods
We compared 388 each wheat and rice sIgG and sIgG4 in a group of 200 children: 50 WA (diagnosis, diet treatment, tolerance), 50 CD (diagnosis and remission), 50 HP and 50 healthy. SIgE, sIgG, sIgG4 were determined with the FEIA method (Pharmacia CAP System).
Results
In healthy children food sIgG were the lowest; no sIgG4 were found. In the CD diagnosis group wheat and rice sIgG and rice sIgG4 were the most common and their concentrations were the highest (p < .001, p < .05). Wheat sIgG4 were the highest in WA children (diagnosis and tolerance) to fall during the elimination diet (p < .05). Wheat and rice sIgG remained the same in all allergy phases. Rice sIgG also did not differ in the class G4.
Conclusions
1. Serum concentrations of wheat and rice sIgG and sIgG4 are elevated in children with CD, HP and WA. 2. Sub-clinical incidence of some gastrointestinal inflammatory diseases may be responsible for high individual versatility of food sIgG and sIgG4 concentrations in serum. 3. Wheat sIgG and sIgG4 in children do not correlate with WA clinical picture.
Similar content being viewed by others


Background
Along with the recent development of diagnostic techniques it has become increasingly popular to use serum concentration levels of specific IgG (sIgG) and IgG4 (sIgG4) as markers of food hypersensitivity. Vast popularity of these diagnostically incorrect tests provoked EAACI to issue an official statement which was later supported by AAAAI and CSACI [1–3]. Scientific associations do not recommend using sIgG and sIgG4 assays in the food hypersensitivity diagnostics. They point out that many individuals have their elevated levels which do not correspond to clinical symptoms of the disease. The research has shown that in humans the presence of food sIgG and sIgG4 is highly individual. The sIgG appear in half of the population, usually as a response to the most common foods [4]. The sIgG4 is only in the case of some food allergens of cow’s milk and egg protein. It has not been resolved so far why in healthy people the frequency and the titers of food sIgG and sIgG4 show such substantial individual variations. Does it depend merely on the frequency of food consumption and the nature of the antigen? Or are there any additional factors?
In this paper we make a hypothesis that these factors can be gastrointestinal inflammatory diseases. One of them is coeliac disease (CD) which can be asymptomatic [5]. The adults with untreated CD showed higher sIgG activity for gliadin, casein and ovalbumin [6, 7]. There have been no research in this respect into other gastrointestinal diseases, hence the question arises if in their case the titers of food sIgG and sIgG4 are different from normal. Some of these diseases, e.g. the infection with Helicobacter pylori (HP), are very common and can take a non-symptomatic or mildly symptomatic form or its symptoms may be non-specific.
The purpose of this paper is a comparative analysis of the frequency and titers of wheat and rice sIgG and sIgG4 in healthy children and the children with IgE-mediated wheat allergy (WA), with CD and HP. Moreover, we evaluate the usefulness of assays of wheat sIgG and sIgG4 in the WA diagnostics. Although wheat is one of the most common food allergens in children, the presence of food sIgG and sIgG4 in WA has’nt been discussed in the literature.
Methods
We compared 338 assays each of wheat and rice sIgG and sIgG4 antibodies determined in 200 children in four groups: 50 children with WA (50 assays each at the time of diagnosis and during the elimination diet; 38 assays during the tolerance); 50 children with CD (diagnosis – aCD, remission - rCD), 50 children with HP and 50 children from the control group (Table 1). Information was collected about the subjects’ consumption of wheat and rice (a questionnaire). The course of WA in a group of 50 children described in this paper (clinical picture over the years, tolerance development age and its factors, specific IgE and IgE on diagnosis, during diet treatment and tolerance) were specified earlier in References #8.
WA was diagnosed in children with positive food challenge results (double-blind placebo-controlled food challenge, DBPCFC) with symptoms occurring within 2 h after wheat consumption and positive SPT as well as with the levels of wheat sIgE higher than 0.7 kU/L. The first challenge test was performed as the open food challenge (OFC), the second - always as the DBPCFC followed by the OFCs. DBPCFC has been described in detail before [8]. 38 children developed tolerance. The subjects were diagnosed with other food allergies, most frequently to cow’s milk, egg protein and peanuts. During the observation the majority of children were diagnosed with atopic dermatitis (78 %), asthma (48 %) and allergic rhinitis (34 %). The progress of WA has been described in detail in References #8. The sIgG and sIgG4 assays were made at the time of diagnosis (the median age was 13 months: 2–22 months.), after 2 years of treatment with a wheat-free diet (the median age was 36 months: 21–42 months.) and during the period of tolerance - negative OFC with wheat (the median age was 69.5 months: 37–192 months).
CD children were examined at the time of diagnosis – aCD (76.3 months: 33 – 230 month.) and remission – rCD (98.6 months: 57 – 254 months). The aCD was made for children with the malabsorption syndrome (Marsh IIIC) and with antibodies to tissue transglutaminase as well as with endomysial antibodies [5]. The rCD was diagnosed when this antibodies were normal. The sIgG and sIgG4 assays were not made until after 12 monthsnths of remission, usually 2 years after the diagnosis.
HP was diagnosed in children (97.4 months: 58 – 212 mo.) with typical endoscopic (gastritis, positive CLO test) and histological picture (chronic gastritis) [9].
The control group (66.4 months: 12 – 197 months.) was composed of patients in whom lesions in the upper part of the digestive tract were ruled out (endoscopic and histological examination). Children had been admitted due to abdominal pains or dwarfism (suspected malabsorption syndrome). They were diagnosed with functional gastrointestinal disorders or constitutional dwarfism.
The inclusion criteria were: diagnosed WA, CD or HP infection and the consent of participants and their guardians.
The criteria for a child to be excluded from observation were other chronic diseases and decreased concentration of total IgG. For children from the CD group, the HP group and the control group an additional elimination factor was atopy which was diagnosed on the basis of an elevated level of tIgE and/or positive sIgE test results for 8 allergens (milk, egg, peanut, cat, Cladosporium herbarum, Dermathophagoides pteronyssinus, grass, sagebrush) and/or a positive SPT (10 air-borne and 10 food allergens). 56 children were lost to follow-up: 52 children with atopy and from WA group: 1 child with ulcerative colitis and 3 children who visited the clinic only once.
All the patients remained under the care of an attending physician (an allergologist or gastroenterologist) throughout the whole observation period. Children were patients of the outpatient clinic and the gastroenterology department. The study was conducted from January 1990 to May 2012.
The titers of tIgE (accuracy 2–9,1 %, sensitivity <2 kU/L, specificity 100 %), sIgE (accuracy 5–11 %, sensitivity <0,35 kU/L, specificity 100 %), sIgG (accuracy 5–10 %, sensitivity <20ug/L, specificity 100 %) and sIgG4 (accuracy 4–7 %, sensitivity <1,5ug/L, specificity >95 %) to wheat and rice were determined by means the FEIA method using the ImmunoCAP System (UniCAP, CAP 100; Pharmacia & Upjohn Diagnostics AB, Uppsala, Sweden). SPTs were performed by means of commercial solutions manufactured by Allergopharma (Germany). The wheal reactions were read after 15 min. (histamine) - 20 min (allergens). Tests were considered positive when the wheal size was ≥ 3 mm in diameter in comparison with the negative control (control solution).
The data were characterized by the median, the minimum and maximum values. The Mann–Whitney test was used to compare sIgG and sIgG4 levels among the patients in the examined groups. The correlation between the selected variables was evaluated with the Spearman rank correlation. A tool used for the statistical analysis was STATA 11, License No 30110532736.
The study was conducted in compliance with the Declaration of Helsinki and following the consent by the Ethical Committee of the Pomeranian Medical University in Szczecin (BN-001/107/90). Sources of funding for the research: State Committee for Scientific Research grant No4 PO5E 086 14 and the clinic in-house research budget.
Results
The children from the control group as well as the ones with WA (diagnosis and tolerance), aCD and HP consumed wheat daily and rice – 1–2 times a week. The children in rCD and the WA children did not consume wheat, but they were given rice at least 4 times a week.
Wheat and rice sIgG4 are not present in children from the control group
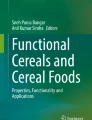
In the children from the control group wheat sIgG was found in 66 % of subjects and rice sIgG – in 30 % (Table 2). No wheat or rice sIgG4 was found in any of those children. The median titer of wheat sIgG was 2850 μg/L (0–7250 μg/L), while that of rice sIgG was 0 (0–4780 μg/L) (Fig. 1).

Serum concentrations and medians of wheat and rice sIgG in children from the control group and in children with IgE mediated wheat allergy. *wheat/rice: p < 0,05; Mann–Whitney test, **control group: children not suffering from atopy and gastrointestinal diseases in the upper part of the digestive tract (endoscopic and histological examination). In the control group the median titer of wheat sIgG was 2850 μg/L (0–7250 μg/L), while that of rice sIgG was 0 (0–4780 μg/L). In each of the wheat allergy phases the titers of sIgG were significantly higher for wheat than for rice (p < .005). They did not differ significantly over the three allergy phases both in the case of wheat and rice
Wheat and rice sIgG and IgG4 are elevated in children over the three wheat allergy phases
At the time of WA diagnosis, diet treatment and WA tolerance, wheat sIgG and sIgG4 and rice sIgG were found in the majority of subjects (88–96 %), while rice sIgG4 – in 46–50 % (Table 2). In each of the WA phases the titers of sIgG and sIgG4 were significantly higher for wheat than for rice (p < .005 and p < .001) (Figs. 1, 2). In the class G they did not differ significantly over the three allergy phases both in the case of wheat and rice (Fig. 1). Rice sIgG4 the titers were also the same over the three allergy phases (Fig. 2). Wheat sIgG4 titers were the same at the time of diagnosis and in the period of tolerance, and decreased during the wheat-free diet (p < .05).

Serum concentrations and medians of wheat and rice sIgG4 in children from the control group and in children with IgE mediated wheat allergy. *wheat/rice: p < 0,05; Mann–Whitney test, **control group: children not suffering from atopy and gastrointestinal diseases in the upper part of the digestive tract (endoscopic and histological examination). In children from the control group wheat or rice sIgG4 were not found. In each of the wheat allergy phases the titers of sIgG4 were significantly higher for wheat than for rice (p < .001). Wheat sIgG4 titers were the same at the time of diagnosis and in the period of tolerance, and decreased during the wheat-free diet (p < .05). Rice sIgG4 the titers were also the same over the three allergy phases
Wheat and rice sIgG and IgG4 are elevated in children with coeliac disease and Helicobacter pylori infection
In the period of aCD wheat and rice sIgG were present in all the subjects, sIgG4 were less common (86 % and 50 %) (Table 2). In the rCD the antibodies were rarer: wheat and rice IgG was found in 84 % of subjects and sIgG4 - in 54 % and 16 %. The titers of wheat and rice sIgG and sIgG4 were always more elevated in aCD than in rCD (p < .001) (Figs. 3, 4). In aCD the serum concentrations of wheat sIgG and sIgG4 were higher than the rice-specific ones (p < .05), to remain the same in rCD.

Serum concentrations and medians of wheat and rice sIgG in children from the control group and in children with coeliac diseases and Helicobacter pylori infection. wheat/rice: *p < 0,05, **ns; Mann–Whitney test, ***control group: children not suffering from atopy and gastrointestinal diseases in the upper part of the digestive tract (endoscopic and histological examination). The titers of wheat and rice sIgG were always more elevated in children with active celiac disease than in remission of celiac disease (p < .001). In active celiac disease the serum concentrations of wheat sIgG were higher than the rice-specific ones (p < .05), to remain the same in remission of celiac disease. In the children with Helicobacter infection the median wheat sIgG were higher than that for rice (p < .05). Their serum concentrations of wheat sIgG were the same as in children with the remission of celiac disease

Serum concentrations and medians of wheat and rice sIgG4 in children from the control group and in children with coeliac diseases and Helicobacter pylori infection. *wheat/rice: p < 0,05; Mann–Whitney test, **control group: children not suffering from atopy and gastrointestinal diseases in the upper part of the digestive tract (endoscopic and histological examination). The titers of wheat and rice sIgG4 were always more elevated in children with active celiac disease than in children with remission of celiac disease (p < .001). In children with active celiac disease the serum concentrations of wheat sIgG4 were higher than the rice-specific ones (p < .05), to remain the same in children with remission of celiac disease. In the children with the Helicobacter pylori infection the median wheat of sIgG4 were higher than that for rice (p < .05). Their serum concentrations of wheat sIgG4 were the same as in children with the remission of celiac disease
In the HP children wheat sIgG and sIgG4 were found in 78 % and 76 % respectively, while rice sIgG and sIgG4 were less common (56 % and 12 %). The median wheat sIgG and sIgG4 were higher than that for rice (p < .05) (Figs. 3, 4).
In children in aCD wheat and rice sIgG and rice sIgG4 were the most elevated (p < .001, p < .001 and p < .05) (Figs. 3, 4). In the sIgG4 subclass the highest titers for wheat were observed in WA children in the phase of diagnosis and tolerance, while in the period of wheat-free diet they were identical as in aCD (Fig. 2).
Discussion
In our study we examined the frequency and titers of wheat and rice IgG and IgG4. We compared a group children not suffering from atopy and gastrointestinal diseases in the upper part of the digestive tract (control group) to a group of children with WA and with CD and HP, two common and usually mildly symptomatic gastrointestinal diseases. Atopy had been excluded from the study since it is known to predispose to developing food sIgG and sIgG4 [7, 10, 11].
Wheat and rice sIgG are not present in all healthy children (control group) but are more common in children with wheat allergy, coeliac disease and Helicobacter pylori infection
The results confirm other authors’ observation that food sIgG do not develop in all healthy children. In addition to that, their incidence and titers vary depending on the food [4]. In this study we detected double as much wheat sIgG as rice IgG (66 % and 30 %) (Table 2). Our research has also shown that wheat sIgG reach higher titers than the ones that are rice specific. In children with WA, CD and HP not only did we observe more common wheat and rice sIgG, but they also reached higher concentration levels in serum (Figs. 1, 3). We did not find the wheat and rice sIgG4 fraction in children from the control group who suffered neither from atopy nor from any gastrointestinal disease (Table 2). The fraction was present in children from the remaining groups: WA, CD and HP (Figs. 2, 4).
The highest concentrations and frequency of wheat and rice sIgG were observed in aCD, while in rCD their frequency was lower and their titer values were smaller (Fig. 2).
Wheat and rice IgG4 don’t present in healthy children (control group) but are more common in children with wheat allergy, coeliac disease and Helicobacter pylori infection (Table 2)
The results confirm other authors’ observation that food IgG4 do not develop in healthy children as a reaction to all kinds of food. As a prevailing subclass they are synthesized for some food allergens only, mainly to chicken egg protein and cow’s milk. They are most common and reach the highest titers for the chicken egg protein ovomucoid, while in the case of cow’s milk casein, gliadin and gluten the system first of all synthesizes subclasses 1 and 3 of immunoglobulin G [6].
Wheat sIgG and sIgG4 do not correlate with the wheat allergy clinical picture
In the majority of children with WA and CD the humoral response to wheat in the class sIgG and sIgG4 was persistent – specific antibodies were present in serum even after wheat had been eliminated from the diet. In WA they were still found in most of the subjects, sIgG titer did not change and sIgG4 decreased (p < .05). In rCD their concentration fell considerably. Persisting long-term highly stable sIgE and sIgG4 epitope-binding patterns were also observed among patients with peanut allergy who were avoiding the allergen [12, 13].
In contrast to children with WA, the elimination of a food from healthy children’s diet results in decreased sIgG titers [14]. Also in milk allergic small children being on a milk-free diet a considerable fall in sIgG serum concentration was observed, which had taken place before their tolerance to milk was developed [15, 16]. Infants with longstanding presence of milk or hen’s egg sIgG suffered from a persistent allergy to those foods [17].
We also found out that the frequency and titers of wheat sIgG and sIgG4 did not correlate to the WA clinical picture. They were developed by the majority of children, but not in all of them, and their frequency was the same in all the disease phases (Table 2). Rice sIgG was observed in the majority of children in all the WA phases, while rice sIgG4 - in a half of the subjects. This indicates that in WA the immune response is changed. It refers not only to food allergens, but also to tolerated foods.
However, several opposite findings have been published that the sIgG and sIgG4 titers do not differ between healthy individuals and patients with atopy or with food allergy to cow’s milk, chicken’s egg and kiwi [16, 18, 19]. Tay et al. found that serum concentration of ovalbumin sIgG and sIgG4 is identical in healthy, allergic and tolerant individuals, but in the case of peanut sIgG and sIgG4 the titers are higher in allergic and atopic patients than in healthy subjects [10].
It is generally assumed that in children with food allergy the elevated titers of food sIgG are the effect of their increased intestinal permeability. When an allergen is eliminated from a diet, intestinal permeability normalizes [20]. In our study group, most of the WA children (78 %) suffered from atopic dermatitis as well. As Majamaa and Isolauri have found out, in such patients the transport of food macromolecules is seven times larger than in healthy individuals and it includes 20 % of the absorbed proteins [21, 22].
The development of food tolerance, both natural and in oral immunotherapy, is associated with the increase in food sIgG4 [23–26]. The maintenance of tolerance to cow’s milk in atopic individuals is characterized by the fall in sIgE titers and high levels of sIgG4 [27]. Children with egg allergy who have developed tolerance to baked egg also experience lowered sIgE and elevated sIgG4 concentrations [28]. Low titers of sIgG4 in young children with food allergy indicate its longstanding character. High serum concentrations of sIgG4 is characteristic to these food allergic children who develop their tolerance early [29, 30]. Sletten et al. claimed opposite findings that in children with milk allergy high titers of sIgG4 for milk allergens decrease during the tolerance period [31].
In conclusion, the incidence and titers of sIgG and sIgG4 are determined not only by the type of food, but also by the type and the activity of a gastrointestinal disease. Higher incidence and titers of food sIgG and sIgG4 were observed in all the diseases under study, i.e. in WA, CD and HP. This indicates that gastrointestinal diseases, due to its commonness and mildly-symptomatic nature, can be one of the factors responsible for high individual versatility of food sIgG and sIgG4.
The highest concentration of wheat and rice sIgG are in children with coeliac disease
High concentrations of food sIgG in serum are characteristic of CD (Fig. 3). They are elevated also at the time of remission when they reach slightly higher titers than in HP infection. Elevated sIgG4 is not a distinctive feature of CD as it is secondary to the rise in sIgG. Still, in CD these antibodies reach top values that are just slightly lower than in WA where the wheat sIgG4 synthesis is preferential (Figs. 2, 4). What is more, it is worth noting that in WA and CD the enhanced synthesis of sIgG and sIgG4 includes not only the symptom-inducing food (wheat), but also the food which is tolerated (rice). This confirms that in WA, CD and HP the immune response to various foods is changed.
Wheat sIgG and sIgG4 are useless in the wheat allergy diagnostics
The findings of our study also point to the fact that the assays of wheat sIgG and sIgG4 are useless in the WA diagnostics. In WA the concentration of these antibodies increases as a response to not only wheat, but to other foods as well, hence it is impossible to determine the actual allergen. The elevated titers persist throughout all the disease phases, so patients recently diagnosed for allergy cannot be distinguished from those who are being treated with elimination diet or have entered the period of tolerance.
The above findings are burdened by a small size of the sample (50 children in each of the groups). Therefore, it is necessary to confirm the findings in a larger group of patients.
Conclusions
-
1.
Serum concentrations of wheat and rice sIgG and sIgG4 are elevated in children with coeliac disease, Helicobacter pylori infection and IgE-mediated wheat allergy.
-
2.
Sub-clinical incidence of some gastrointestinal inflammatory diseases may be responsible for high individual versatility of food sIgG and sIgG4 concentrations in serum.
-
3.
Wheat sIgG and sIgG4 in children do not correlate with IgE-mediated wheat allergy clinical picture.
Abbreviations
- AAAAI:
-
American Academy of Allergy, Asthma & Immunology
- aCD:
-
coeliac disease diagnosis
- CD:
-
coeliac disease
- CLO test:
-
test for Helicobacter pylori diagnosis in tissue
- CSACI:
-
Canadian Society of Allergy and Clinical Immunology
- DBPCFC:
-
double-blind placebo-controlled food challenge
- EAACI:
-
The European Academy of Allergy and Clinical Immunology Organisation
- FEIA method:
-
fluoro-immuno-enzymatic method
- HP:
-
helicobacter pylori infection
- M:
-
male
- mo.:
-
months
- OFC:
-
open food challenge
- rCD:
-
remission of coeliac disease
- sIgE:
-
specific immunoglobulin E
- sIgG:
-
specific immunoglobulin G
- sIgG4:
-
specific immunoglobulin G4
- SPT:
-
skin prick test
- tIgE:
-
total immunoglobulin E
- WA:
-
IgE-mediated wheat allergy
References
Stapel SO, Asero R, Ballmer-Weber BK, Knol EF, Strobel S, Vieths S, et al. EAACI Task Force. Testig for IgG4 against food is not recommended as a diagnostic tool: EAACI Task Force report. Allergy. 2008;63:793–6.
Bock SA. AAAAI support of the EAACI Position Paper on IgG4. J Allergy Clin Immunol. 2010;125:1410.
Carr S, Chan E, Lavine E, Moote W. CSACI Position statement on the testing of foo-specific IgG. Allergy, Asthma Clin Immunol. 2012;8:12. doi:10.1186/1710-1492-8-12.
Volpi N, Maccari F. Serum IgG Responsens to Food Antigens in the Italian Population Evaluated by Highly Sensitive and Specific ELISA Test. J Immunoass Immunochem. 2009;30:51–69.
Husby S, Koletzko S, Korponay-Szabó IR, Mearin ML, Phillips A, Shamir R, et al. ESPGHAN Working Group on Coeliac Disease Diagnosis; ESPGHAN Gastroenterology Committee; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54:136–60.
Hvatum M, Scott H, Brandtzaeg P. Serum IgG subclass antibodies to a variety food antigens in patients with coeliac disease. Gut. 1992;33:632–8.
Kemeny DM, Urbanek R, Amlot PL, Ciclitira PJ, Richards D, Lessof MH. Sub-class of IgG in allergic disease. I. IgG sub-class antibodies in immediate and non-immediate food allergy. Clin Allergy. 1986;16:571–81.
Czaja-Bulsa G, Bulsa M. The natural history of IgE mediated wheat allergy in children with dominant gastrointestinal symptoms. Allergy, Asthma Clin Immunol. 2014;10:12. doi:10.1186/1710-1492-10-12.
Koletzko S, Jones NL, Goodman KJ, Gold B, Rowland M, Cadranel S, et al. H pylori Working Groups of ESPGHAN and NASPGHAN. Evidence-based guidelines from ESPGHAN and NASPGHAN for Helicobacter pylori infection in children. J Pediatr Gastroenterol Nutr. 2011;53:230–43.
Tay SS, Clark AT, Deighton J, King Y, Ewan PW. Patterns of immunoglobulin G responses to egg and peanut allergens are distinct: Ovalbumin-specific immunoglobulin responses are ubiquitous, but peanut-specific immunoglobulin responses are upregulated in peanut allergy. Clin Exp Allergy. 2007;37:1512–8.
Shek LP, Bardina L, Castro R, Sampson HA, Beyer K. Humoral and cellular responses to cow milk proteins in patients with milk-induced IgE-mediated and non-IgE-mediated disorders. Allergy. 2005;60:912–9.
Flinterman AE, Knol EF, Lencer DA, Bardina L, den Hartog Jager CF, Lin J, et al. Peanut epitopes for IgE and IgG4 in peanut-sensitized children in relation to severity of peanut allergy. J Allergy Clin Immunol. 2008;121:737–43.
Vickery BP, Lin J, Kulis M, Fu Z, Steele PH, Jones SM, et al. Peanut oral immunotherapy modifies IgE and IgG4 responses to major peanut allergens. J Allergy Clin Immunol. 2013;131:128–34.
Vance GH, Grimshaw KE, Briggs R, Lewis SA, Mullee MA, Thornton CA, Warner JO. Serum ovalbumin – specific immunoglobulin G responses during pregnancy reflect maternal intake of dietary egg and relate to the development of allergy in early infancy. Clin Exp Allergy. 2004;34:1855–61.
Orivuori L, Mustonen K, Roduit C, Braun-Fahrländer C, Dalphin JC, Genuneit C, et al. PASTURE Study Group. Immunoglobulin A and immunoglobulin G antibodies against β-lactoglobulin and gliadin at age 1 associate with immunoglobulin E sensitization at age 6. Pediatr Allergy Immunol. 2014;25:329–37.
Hidvegi E, Cserhati E, Kereki E, Savilahti E, Arato A. Serum immunoglobulin E, IgA, and IgG antibodies to different cow’s milk proteins in children with cow’s milk allergy: association with prognosis and clinical manifestations. Pediatr Allergy Immunol. 2002;13:255–61.
Vance GH, Thornton CA, Bryant TN, Warner JA, Warner JO. Ovalbumin-specific immunoglobulin G and subclass responses through the first 5 years of life in relation to duration of egg sensitization and the development of asthma. Clin Exp Allergy. 2004;34:1542–9.
Bublin M, Dennstedt S, Buchegger M, Antonietta Ciardiello M, Bernardi ML, Tuppo L. The performance of a component-based allergen microarray for the diagnosis of kiwifruit allergy. Clin Exp Allergy. 2011;41:129–36.
Ahrens B, de Oliveira LC L, Schulz G, Borres MP, Niggemann B, Wahn U, Beyer K. The role of hen’s egg-specific IgE, IgG and IgG4 in the diagnostic procedure of hen’s egg allergy. Allergy. 2010;65:1554–7.
Yu LC. Intestinal Epithelial Barrier Dysfunction in Food Hypersensitivity. J Allergy (Cairo). 2012;2012:96081. doi:10.1155/2012/596081.
Majamaa H, Isolauri E. Evaluation of the gut mucosal barrier. Evidence for increased antigen transfer in children with atopic eczema. J Allergy Clin Immunol. 1996;97:985–90.
Caffarelli C, Cavagni G, Menzies IS, Bertolini P, Atherton DJ. Elimination diet and intestinal permeability in atopic eczema: a preliminary study. Clin Exp Allergy. 1993;23:28–31.
Akdis M, Akdis CA. Mechanisms of allergen-specific immunotherapy: multiple suppressor factors at work in immune tolerance to allergens. J Allergy Clin Immunol. 2014;133:621–31.
Lee JH, Kim WS, Kim H, Hahn YS. Increased cow's milk protein-specific IgG4 levels after oral desensitization in 7- to 12-month-old infants. Ann Allergy Asthma Immunol. 2013;111:523–8.
Savilahti EM, Savilahti E. Development of natural tolerance and induced desensitization in cow's milk allergy. Pediatr Allergy Immunol. 2013;24:114–21.
Hofmaier S, Comberiati P, Matricardi PM. Immunoglobulin G in IgE-mediated allergy and allergen-specific immunotherapy. Eur Ann Allergy Clin Immunol. 2014;46:6–11.
Merras-Salmio L, Kolho KL, Pelkonen AS, Kuitunen M, Mäkelä MJ, Savilahti E. Markers of gut mucosal inflammation and cow’s milk specific immunoglobulins in non-IgE cow’s milk allergy. Clin Transl Allergy. 2014;4:8. doi:10.1186/2045-7022-4-8.
Leonard SA, Sampson HA, Sicherer SH, Noone S, Moshier EL, Godbold J, Nowak-Węgrzyn A. Dietary baked egg accelerates resolution of egg allergy in children. J Allergy Clin Immunol. 2012;130:473–80.
Tomicić S, Norrman G, Fälth-Magnusson K, Jenmalm MC, Devenney I, Böttcher MF. High levels of IgG4 antibodies to foods during infancy are associated with tolerance to corresponding foods later in life. Pediatric Allergy Clin Immunol. 2009;20:35–41.
Jenmalm MC, Björkstén B. Cord blood levels of immunoglobulin G subclass antibodies to food and inhalant allergens in relation to maternal atopy and the development of atopic disease during the first 8 years of life. Clin Exp Allergy. 2000;30:34–40.
Sletten GB, Halvorsen R, Egaas E, Halstensen TS. Changes in humoral responses to beta-lactoglobulin in tolerant patients suggest a particular role for IgG4 in delayed, non –IgE-medated cow’s milk allergy. Pediatr Allergy Immunol. 2006;17:435–43.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
All the authors have no financial relationships relevant to this article to disclose.
Authors’ contributions
GC-B conceptualized and designed the study, designed the data collection instruments, coordinated and supervised data collection, drafted the initial manuscript, and approved the final manuscript as submitted. MB conceptualized the study, supervised data collection, carried out the analyses, drafted the initial manuscript and approved the final manuscript as submitted. AG conceptualized the study, data collection, carried out the analyses, drafted the initial manuscript and approved the final manuscript as submitted.
Authors’ information
Grażyna Czaja-Bulsa – Prof Pomeranian Medical University in Szczecin, Poland
- paediatrician, allergologist, gastroenterologist
- head of Pediatrics and Pediatric Nursery Unit of The Pomeranian Medical University
- head of Division of Paediatrics, Gastroenterology and Rheumatology of The „Zdroje” Hospital
Michał Bulsa – MD
Aneta Gębala – MD, PhD, paediatrician, gastroenterologist
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Czaja-Bulsa, G., Bulsa, M. & Gębala, A. Food IgG4 antibodies are elevated not only in children with wheat allergy but also in children with gastrointestinal diseases. BMC Gastroenterol 16, 39 (2016). https://doi.org/10.1186/s12876-016-0450-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-016-0450-3