
Abstract
Background
The International Classification of Functioning, Disability and Health (ICF) model of the consequences of disease identifies three health outcomes, impairment, activity limitations and participation restrictions. However, few orthopaedic health outcome measures were developed with reference to the ICF. This study examined the ability of a valid and frequently used measure of upper limb function, namely the Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH), to operationalise the ICF.
Methods
Twenty-four judges used the method of Discriminant Content Validation to allocate the 38 items of the DASH to the theoretical definition of one or more ICF outcome. One-sample t-tests classified each item as measuring, impairment, activity limitations, participation restrictions, or a combination thereof.
Results
The DASH contains items able to measure each of the three ICF outcomes with discriminant validity. The DASH contains five pure impairment items, 19 pure activity limitations items and three participation restriction items. In addition, seven items measured both activity limitations and participation restrictions.
Conclusion
The DASH can measure the three health outcomes identified by the ICF. Consequently the DASH could be used to examine the impact of trauma and subsequent interventions on each health outcome in the absence of measurement confound.
Similar content being viewed by others

Background
Fracture of the wrist is a common injury and is especially prevalent in older post-menopausal women. Wrist fracture is associated with variable outcome, for example, approximately 50% of cases fail to recover pre-operative function [1] and 20% of patients report moderate to severe pain at 6 month post-fracture [2]. A recent series of Cochrane reviews of the effectiveness of commonly applied interventions for wrist fracture have highlighted the continued unsatisfactory outcome for many patients [3]. Further, there is an association between wrist fracture and long-term disability and increased risk of dependency [4]. Any measure of outcome from wrist fracture needs to be able to index the impact of fracture, not only on the impairment itself but also on the level of associated disability.
The WHO identifies three health outcomes in its International Classification of Functioning Disability and Health (ICF) taxonomy of the consequences of disease, namely, impairments (I), activity limitations (A) and restrictions in social participation (P) [5] (see Table 1 for definitions). In accordance with the ICF, a complete assessment of outcome for any health condition or intervention requires an evaluation of each health outcome domain. Whilst, the reliability and construct validity of six patient self-report instruments for the assessment of the upper extremity following trauma were recently reviewed [6], the review did not examine the content validity of each instrument relative to the outcomes identified in the ICF. This may be an important omission because the application of the ICF to aid rehabilitation requires that each health outcome be measurable. Whilst new measures specifically designed to assess each ICF outcome could be developed, the development and validation of new measures is a time consuming and expensive process. A preferable approach might be to examine the compatibility between the ICF and outcome measures currently in use [7].
The development of core measurement sets for patients with musculoskeletal conditions or for acute hospital and early post-acute rehabilitation are available [8–10], and these may be relevant to patients with wrist fracture. Whilst, the core measurement sets detail the categories within each health outcome that need to be assessed for a given health condition, they do not identify the actual items to be used to measure each category. The ability of existing health outcome measures to operationalise the ICF is an area of active research [11–13] and it is possible that existing wrist fracture outcome measures may contain items that measure each ICF outcome. That said, in order for the ICF to be tested as a model of the outcomes from wrist fracture it is not only necessary to have measures of each ICF outcome but those measures need to show discriminant validity. Such pure measures are necessary to ensure that any observed relationship between the three outcomes is not simply due to measurement confound.
The method of Discriminant Content Validity (DCV) is able to establish the discriminant validity of measurement items [13, 14]. DCV examines the relationship between individual measurement items and all constructs within a theoretical model thereby establishing the content validity of a measurement item against all constructs within a given theory. Rather than judge items against a single theoretical construct, the DCV method establishes whether each theoretical construct can be measured discriminately because the method asks judges to indicate the extent to which an item matches each theoretical construct of interest, in this case the three main outcomes identified by the ICF. This method has been used to establish the content validity of items within existing orthopaedic and chronic pain measures [13, 14]. In this study we used DCV to identify ICF outcomes measured by the Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH) [15].
Method
Design
Participants acted as judges and matched the thirty-eight items from the DASH to the definitions of the impairment, activity limitations and participation restrictions constructs from the ICF model.
Participants
Twenty-four academics (one clinical, five industrial and thirteen health psychologists and five health service researchers) from the Applied Psychology Research Group at the University of Aberdeen took part in the study as part of a seminar on the DCV method. The precise number of judges required for judgement tasks is yet to be established but between 2–20 is regarded as adequate [16–18].
Materials
The definitions of the three ICF constructs, namely: impairment, activity limitations, and participation restrictions were taken from the WHO and are given in Table 1. All 38-measurement items from the DASH were assessed. The DASH is a self-administered region-specific outcome instrument developed as a measure of self-rated upper-extremity disability and symptoms and has been identified as the most validated and easy to use measure of upper extremity function [6]. The DASH consists of 30 core items, and 8 optional items, which generate a disability score, scaled 0 (no disability) to 100.
Procedure
The detailed procedure for a DCV study has been published previously [13, 14, 19]. Briefly, for each DASH item, participants provided a Yes/No judgement of whether the item was a match to the theoretical definition of each ICF construct. Consequently, each participant provided 3 judgements for each of the 38 items, i.e. 114 judgements in total. In addition, participants gave a confidence rating for each judgement on an 11-point scale ranging from 0% to 100%, rising in 10% increments.
Statistical Analysis
Classification of items
Judgements were coded 1 for a match and -1 for a no match. Each judgement was multiplied by its accompanying confidence rating, expressed as a proportion. Consequently, the weighted judgements ranged from -1 to +1. One-sample t-tests were used to classify each item to one of the 7 possible combination of constructs, namely: I, A, P, IA, IP, AP or IAP. An item was classified as being related to a construct if its weighted judgement against that construct was significantly greater than zero. Missing data, either a missing judgement or a missing confidence rating were coded zero. The weighted judgement of that item by that judge, therefore, was zero and was entered as such into the one sample t-test. Hochberg's correction was used to correct for multiple tests [20]. Application of the Hochberg's correction identified statistical significance was achieved with t-values that corresponded to a p value of ≤ 0.001.
Inter-rater reliability
Intraclass correlation coefficients (ICC) and their 95% confidence intervals (95%C.I.), were used to assess agreement between judges across all 38 items and for each construct, i.e. I, A and P judgements. The weighted judgements were used to calculate the ICC using the two-way mixed model with measure of consistency.
Results
Reliability of participant performance
The ICC for all judgements across all 38 items was 0.96 (95% C.I. 0.94–0.97). The ICC for each construct was as follows, 0.96 (95% C.I. 0.96–0.99) for I judgements, 0.96 (95% C.I. 0.94–0.97) for A judgements and 0.94 (95% C.I. 0.86–0.98) for P judgements. Examination of the contribution of each participant to the ICC, for all judgements and for each construct revealed all participants to be performing equally well; therefore, all 24 participants were included in the subsequent analyses.
DCV Analyses
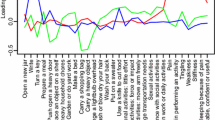
Thirty-four of the 38 items were classified to one or more of the ICF constructs (see Table 2). Twenty-seven items were identified as pure construct measures being related to a single ICF construct only. Five items were uniquely related to the impairment construct; all five items were from the main section of the DASH. Nineteen items were uniquely related to the activity limitations construct; 15 items from the main section of the DASH and two from each optional section. Three items were identified as pure measures of the participation restriction construct; two from the main section, one from the optional work section. Seven items were matched to both the activity limitations and participations constructs; this was the only form of mixed item within the questionnaire; five mixed items were from the main section of the questionnaire and two from the sport/music section. Judges failed to agree on the classification of 4 items; these were items 10, 29 and 30 from the main section of the questionnaire and item three from the optional work module.
Discussion
The DASH contained 27 pure construct measures and can, therefore, be used to measure each ICF construct without measurement confound.
A recently published study used 4 judges to link the ICF to the DASH items [21]. In this study the ICF coding taxonomy was employed and individual DASH items were assigned one or more ICF code. This strategy enables the identification of I items but does not enable A to be distinguished from P because the ICF coding taxonomy fails to discriminate between these two theoretically distinct constructs. Nonetheless, these findings were consistent with the DCV analysis; with the exception of one item, all items identified as measuring I in the current study were assigned to ICF codes within the body functions category in the linkage study. The exception was item 29 which was not classified in the current study due to a lack of agreement between judges; in the Drummond et al study item 29, which concerns sleeping difficulties, received a body function coding. The I items within the DASH primarily focus on pain and muscle stiffness or weakness, previous studies have identified pain items as measures of the impairment construct [13].
All other items (except item 30) were coded as "activities and participation" by Drummond et al. In the current study these items were also coded as A or P or AP. However, the current data enables A and P items to be distinguished and enables mixed items to be clearly identified. This has the advantage of enabling the discriminant measurement of each type of outcome.
The availability of discriminant outcome measures is especially important in assessing outcomes in intervention studies. Being able to assess the impact of an intervention on I, A and P outcomes, in a manner that is free of measurement confound, provides the means to assess the success of an intervention within each outcome domain. For example, in the case of wrist fracture, x-ray may indicate the fracture (I) to be healed but the patient may not have regained full function (A) and may remain afraid of going outside (P). Measurement of outcome in this patient would be over positive if only the impairment outcome were measured. The DASH produces a single score; consequently it does not distinguish between the three ICF health outcomes as it is currently used. However, its content is capable of producing an impairment score; an activity limitations score and a participation restriction score as well as the standard single score. The standard method of scoring the DASH generates a simple mean score across all items and converts this mean score to a 0–100 scale. The standard method of scoring the questionnaire could be applied to the items measuring each health outcome, such that, a respondent would generate a score between 0–100 for each health outcome [see Additional files 1 and 2]. We do not advocate the standard method of scoring the DASH be replaced. Rather, the availability of the DCV analysis of the DASH for clinicians and researchers enables the instrument to be individualised to the requirements of a given situation, be that the particular needs of an individual patient or the requirements of a specific research question. Consequently, it enables the existing evidence base to be developed cumulatively.
Conclusion
This study adds to previous research in identifying pure measurement items for each of the three ICF outcomes. It provides a means to generate three distinct outcome measures for arm, shoulder and hand trauma, namely impairment, activity limitations and participation restrictions. As a consequence, the impact of interventions, such as surgery, on each health outcome can be identified.
References
De Bruin HP: The Colles' fracture, review of literature. Acta Orthopaedica Scandinavica. 1987, 58: 7-25.
Macdermid JC, Roth JH, Richards RS: Pain and disability reported in the year following a distal radius fracture: a cohort study. BMC Musculoskeletal Disorders. 2003, 4: 24-10.1186/1471-2474-4-24.
Handoll HHG, Madhok R: From evidence to best practice in the management of fractures of the distal radius in adults: working towards a research agenda. BMC Musculoskeletal Disorders. 2003, 4: 27-10.1186/1471-2474-4-27.
Scaf-Klomp W, Van Sonderen E, Sanderman R, Ormel J, Kempen G: Recovery of physical function after limb injuries in independent older people living at home. Age and Ageing. 2001, 30: 213-219. 10.1093/ageing/30.3.213.
World Health Organisation: International classification of functioning, disability and health: ICF. 2001, Geneva: World Health Organisation
Dowrick AS, Gabbe BJ, Williamson OD, Cameron PA: Outcome instruments for the assessment of the upper extremity following trauma: a review. Injury. 2005, 36 (4): 468-476. 10.1016/j.injury.2004.06.014.
Stucki G, Ewert T, Cieza A: Value and application of the ICF in rehabilitation medicine. Disability and Rehabilitation. 2003, 25: 628-634. 10.1080/09638280110070221.
Grill E, Ewert T, Chatterji S, Kostanjsek N, Stucki G: ICF core sets development for the acute hospital and early post-acute rehabilitation facilities. Disability and Rehabilitation. 2005, 27: 361-366. 10.1080/09638280400013974.
Scheuringer M, Stucki G, Huber EO, Brach M, Schwarzkopf SR, Kostanjsek N, Stoll T: ICF core set for patients with musculoskeletal conditions in early post-acute rehabilitation facilities. Disability and Rehabilitation. 2005, 27: 405-410. 10.1080/09638280400014006.
Stoll T, Brach M, Huber EO, Scheuringer M, Schwarzkopf SR, Konstanjsek N, Stucki G: ICF core set for patients with musculoskeletal conditions in the acute hospital. Disability and Rehabilitation. 2005, 27: 381-387. 10.1080/09638280400013990.
Cieza A, Brockow T, Ewart T, Amman E, Kolleritis B, Chatterji S, Ustun TB, Stucki G: Linking health-status measurements to the international classification of functioning, disability and health. Journal of Rehabilitation Medicine. 2002, 34: 205-210. 10.1080/165019702760279189.
Brockow T, Cieza A, Kuhlow H, Sigl T, Franke T, Harder M, Stucki G: Identifying the concepts contained in outcome measures of clinical trials on musculoskeletal disorders and chronic widespread pain using the international classification of functioning, disability and health as a reference. Journal of Rehabilitation Medicine. 2004, 36: 30-36. 10.1080/16501960410015371.
Pollard B, Johnston M, Dieppe P: What do osteoarthritis heath outcome instruments measure? Impairment, activity limitation or participation restriction?. Journal of Rheumatology. 2006, 33: 757-763.
Dixon D, Pollard B, Johnston M: What does the chronic pain grade questionnaire measure?. Pain. 2007, 130: 249-253. 10.1016/j.pain.2006.12.004.
Hudak PL, Amadio PC, Bombardier C: Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder, and hand). American Journal of Industrial Medicine. 1996, 29: 602-608. 10.1002/(SICI)1097-0274(199606)29:6<602::AID-AJIM4>3.0.CO;2-L.
Waltz CW, Strickland OL, Lenz ER: Measurement in nursing research. 1991, Philadelphia: F.A. Davis Co
Lynn MR: Determination and quantification of content validity. Nursing Research. 1986, 35: 382-385. 10.1097/00006199-198611000-00017.
Rubio DM, Berg-Weber M, Tebb SS, Lee ES, Rauch S: Objectifying content validity: conducting a content validity study in social work research. Social Work Research. 2003, 27: 94-104.
Pollard B, Johnston M: Operationalisation of constructs within theoretical models using existing measures: a method to establish content validity of health status measures [abstract]. Proceedings of the British Psychological Society. 2005, 13: 87-
Hochberg Y: A sharper Bonferroni procedure for multiple tests of significance. Biometrika. 1988, 75: 800-803. 10.1093/biomet/75.4.800.
Drummond AS, Sampaio RF, Mancini MC, Kirkwood RN, Stamm TA: Linking the disabilities of arm, shoulder, and hand to the international classification of functioning, disability, and health. Journal of Hand Therapy. 2007, 20: 336-343.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2474/9/114/prepub
Acknowledgements
The Medical Research Council Health Services Research Collaboration funded this work.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
DD collected and analysed the data and is the principle author of the paper. MJ, MMcQ and CC-B provided a critical review of the manuscript. All authors read and approved the final manuscript.
Electronic supplementary material
12891_2008_520_MOESM1_ESM.pdf
Additional file 1: DASH ICF SYNTAX. Syntax for use with SPSS analysis software. This syntax will calculate pure I, A and P scores and a mixed AP score from the DASH questionnaire, measured at up to two time points. The syntax should be applied to an SPSS data file formatted as described in additional file 2. (PDF 14 KB)
12891_2008_520_MOESM2_ESM.pdf
Additional file 2: DASH ICF SPSS datafile. An empty SPSS data file formatted to support the syntax provided in additional file 1. (PDF 15 KB)
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Dixon, D., Johnston, M., McQueen, M. et al. The Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH) can measure the impairment, activity limitations and participation restriction constructs from the International Classification of Functioning, Disability and Health (ICF). BMC Musculoskelet Disord 9, 114 (2008). https://doi.org/10.1186/1471-2474-9-114
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2474-9-114