
Abstract
Background
Diabetes prevalence is increasing globally, and Sub-Saharan Africa is no exception. With diverse health challenges, health authorities in Sub-Saharan Africa and international donors need robust data on the epidemiology and impact of diabetes in order to plan and prioritise their health programmes. This paper aims to provide a comprehensive and up-to-date review of the epidemiological trends and public health implications of diabetes in Sub-Saharan Africa.
Methods
We conducted a systematic literature review of papers published on diabetes in Sub-Saharan Africa 1999-March 2011, providing data on diabetes prevalence, outcomes (chronic complications, infections, and mortality), access to diagnosis and care and economic impact.
Results
Type 2 diabetes accounts for well over 90% of diabetes in Sub-Saharan Africa, and population prevalence proportions ranged from 1% in rural Uganda to 12% in urban Kenya. Reported type 1 diabetes prevalence was low and ranged from 4 per 100,000 in Mozambique to 12 per 100,000 in Zambia. Gestational diabetes prevalence varied from 0% in Tanzania to 9% in Ethiopia. Proportions of patients with diabetic complications ranged from 7-63% for retinopathy, 27-66% for neuropathy, and 10-83% for microalbuminuria. Diabetes is likely to increase the risk of several important infections in the region, including tuberculosis, pneumonia and sepsis. Meanwhile, antiviral treatment for HIV increases the risk of obesity and insulin resistance. Five-year mortality proportions of patients with diabetes varied from 4-57%. Screening studies identified high proportions (> 40%) with previously undiagnosed diabetes, and low levels of adequate glucose control among previously diagnosed diabetics. Barriers to accessing diagnosis and treatment included a lack of diagnostic tools and glucose monitoring equipment and high cost of diabetes treatment. The total annual cost of diabetes in the region was estimated at US$67.03 billion, or US$8836 per diabetic patient.
Conclusion
Diabetes exerts a significant burden in the region, and this is expected to increase. Many diabetic patients face significant challenges accessing diagnosis and treatment, which contributes to the high mortality and prevalence of complications observed. The significant interactions between diabetes and important infectious diseases highlight the need and opportunity for health planners to develop integrated responses to communicable and non-communicable diseases.
Similar content being viewed by others


Background
Sub-Saharan Africa, like the rest of the world, is experiencing an increasing prevalence of diabetes alongside other non-communicable diseases [1]. In 2010 12.1 million people were estimated to be living with diabetes in Africa, and this is projected to increase to 23.9 million by 2030 [2]. In Sub-Saharan Africa this trend is emerging in a region grappling with high rates of communicable diseases - including the highest global prevalence of HIV [3], Tuberculosis [4] and Malaria [5]. Diabetes is a component cause of several other important and often lethal diseases, both non-communicable diseases such as cardiovascular disease [6] and renal disease [7], and communicable diseases such as pneumonia [8], bacteraemia [9, 10] and tuberculosis [11], which have considerable impacts on morbidity and mortality in the region [12–17]. With this double burden of disease and limited resources, diabetes must compete for political attention and financial investment. With various regional and international meetings and initiatives [18], including the UN high-level meeting on Non-communicable Diseases scheduled for 19-20 September 2011, diabetes and other non-communicable diseases are beginning to get greater political attention. Policymakers need guidance from strong reviews of current information on trends and public health impact. This review expands on recent reviews of diabetes in the region [19–21], providing greater consideration of the diabetes prevalence, access to diabetes diagnosis and care, clinical outcomes following diabetes (chronic diabetes complications, infections and mortality), and economic costs.
Methods
We conducted a systematic review of all papers published on diabetes in Sub-Saharan Africa between January 1999 and March 2011 and available on PubMed. We defined Sub-Saharan Africa as all mainland African countries south of the Sahara with the addition of the island state of Madagascar. We searched for articles providing data from this region on diabetes prevalence, diabetes outcomes (chronic diabetes complications, infections, and mortality), access to diabetes diagnosis and care, and the economic burden caused by diabetes. A combined keyword search on PubMed identified 1102 papers. See Additional File 1: Annex 1 for a description of the review and Additional File 2: Annex 2 for the keywords used. The references of included articles were scanned to identify additional articles of interest published before January 1999. Grey literature, from sources including the websites of the World Bank, World Health Organisation and International Diabetes Federation was also reviewed.
Results
The prevalence of diabetes in Sub-Saharan Africa
Type 2 diabetes accounts for over 90% of diabetes cases in Sub-Saharan Africa [19], whilst Type 1 diabetes, gestational diabetes, and variant forms such as atypical 'ketosis-prone' diabetes and malnutrition-related diabetes constitute the remainder.
Type 2 diabetes
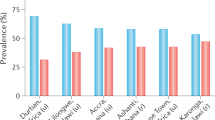
Just nine countries in the region have reported data from type 2 diabetes (T2DM) prevalence surveys in the last decade (see table 1) [22–36]. Two of these countries have conducted population surveys with the assistance of the World Health Organisation's 'STEPwise Approach to Chronic Disease Surveillance Management'. Prevalence in the general population of T2DM recorded in these studies ranged from 0.6% in rural Uganda [35] to 12% in urban Kenya [27]. A low to medium prevalence (0-7%) was recorded in Cameroon, Ghana, Guinea, Kenya, Nigeria, South Africa and Uganda and a very high prevalence (> 10%) was recorded in Zimbabwe (table 1).
Variation in prevalence recorded within countries was common. Prevalence estimates varied considerably between different studies for some countries, with estimates for rural South Africa ranging from 3.9% [31] to 8.8% [33]. Variation between urban and rural populations was frequently observed, with a higher prevalence recorded in urban populations [22, 23, 26, 27, 33, 34]. Prevalence recorded in Christensen's Kenyan survey ranged from 2% in rural areas to 12% in urban areas [27].
One recent study investigated the incidence of type 2 diabetes in Kinshasa among a cohort of 807 people, aged over 40 at baseline [37]. 93 participants developed T2DM during the study period (December 2004 to September 2008), corresponding to an incidence rate of 29 (95% CI 15-43) per 1,000 person-years.
Type 1 diabetes
Four studies estimating the prevalence and/or incidence of type 1 diabetes in the region were published since 1990 [38–41] (see table 2). Observed prevalence ranged from 3.5 per 100,000 persons in Mozambique [40], to 12 per 100,000 persons in Zambia [40]. Recorded incidence ranged from 1.5 per 100,000 persons per year in Tanzania [41] to 2.1 per 100,000 persons per year in Ethiopia [39].
Gestational diabetes mellitus
The literature review identified two studies on the prevalence of gestational diabetes in Sub-Saharan Africa 1999-present, one in Ethiopia [42] and one in South Africa [43] (see table 3). Three other relatively recent studies, published before January 1999, were identified [44–46]. The range of prevalence recorded in these five studies is considerable, from 0% among pregnant women in Tanzania to 9% in Ethiopia.
Other Types of Diabetes
Several reviews describing diabetes trends in Africa report the occurrence of other forms of diabetes, namely 'Atypical African diabetes' or 'Ketosis-prone atypical diabetes mellitus' and 'Malnutrition-related diabetes' or 'Tropical Diabetes' [19, 20, 47]. However, beyond describing their existence and aetiology, no studies investigating the population prevalence of these forms of diabetes in the region were identified.
Outcomes of diabetes
Diabetes mortality
Three studies investigated mortality in patients with diabetes in the region, two of which were conducted almost twenty years ago (Table 4). These studies revealed high mortality proportions, with 5-year mortality ranging from 4% - 57% [48–50]. 41% of individuals with Insulin-Dependent Diabetes Mellitus (IDDM) died within five years in a study in Tanzania, and half of these deaths were attributed to ketoacidosis [50]. Infection was another important cause of mortality, accounting for 48% of deaths in indeterminate diabetes cases, 32% in IDDM and 23% in Non-Insulin Dependent Diabetics (NIDDM) in the Tanzanian survey [50].
The prevalence of chronic diabetes complications among persons with diabetes
Twenty-three studies on the prevalence of chronic complications of diabetes among persons with diabetes published from 1999-2011 were reviewed (see table 5) [51–74]. The recorded prevalence of retinopathy ranged from 7% in Kenya [63], to 63% in South Africa [67], neuropathy ranged from 27% in Cameroon [52] to 66% in Sudan [54], and the prevalence of microalbuminuria ranged from 10% in Tanzania [74] to 83% in Nigeria [73]. Some national variation was suggested, with recorded retinopathy rates ranging from 7% to 22% in Kenya [63, 64].
Important infections and diabetes
Whilst epidemiological studies outside Sub-Saharan Africa have associated diabetes with infectious diseases of great importance in this region (see Discussion section), the literature review identified little epidemiological data on this association in Sub-Saharan Africa. A few smaller case-control studies have suggested that the prevalence of urinary tract infections is increased in diabetic patients in Sub-Saharan Africa, as observed in developed countries [75]. Several reviews have described the frequent occurrence of gangrene, infection and sepsis associated with diabetic foot ulcer disease [76] and with trauma to the hand (tropical diabetic hand syndrome) [77] in Sub-Saharan Africa.
Access to diabetes diagnosis and treatment
All of the type II prevalence surveys which recorded proportions of previously undiagnosed diabetes among participants who attended screening programmes found very high levels (≥40%). Proportions exceeded 50% in five surveys, and reached 100% in rural Guinea [24–27, 29, 33].
Beran et al surveyed the availability of diagnostic testing tools in a sample of healthcare settings in three countries, and found that in Mozambique urine glucose strips were available in just 18% of health facilities surveyed, ketone testing strips in 8% and blood glucose metres in 21%, whilst availability in Mali was 54%, 43% and 13% and in Zambia 61%, 54%, 49% [40, 78].
Low levels of adequate glucose control in diagnosed diabetics were reported in several prevalence studies [24, 68]. Only 27% of diagnosed type 2 diabetics receiving treatment in the Cameroon study had adequately controlled glucose levels [24]. Of 99 type 1 diabetics in the Tanzanian survey, only one person achieved good glucose control [68]. None of the 99 type 1 diabetics had the ability to monitor their glucose levels at home, and hospitals were unable to routinely do this [68]. A regular supply of insulin was unaffordable for many diabetics, with one month's insulin supply costing 19.6 days wages in Malawi [79] and 25% of the minimum wage in Tanzania [80]. One Sudanese study found that 65% of a families' annual household expenditure on health was spent on caring for a diabetic child [81]. Beran and Yudkin found that state interventions affected insulin price, reporting that an annual supply of insulin cost 5% of GDP in Mozambique, where it was subsidised by the government, whereas it cost 25% of GDP in Mali without subsidies [78]. One study investigated Insulin availability and reported that one of five hospitals and none of six health centres surveyed had a regular insulin supply[40].
Economic Costs of Diabetes
Few studies were identified which investigated the cost of diabetes in the region. Kiriga et al (2009) estimated that the total economic cost (direct and indirect) of diabetes in the WHO's Africa region in 2000 was Int$25.51 billion (US$67.03 billion), or Int$3363 (US$8836) per person with diabetes per year [82] (numbers converted from International dollars to their equivalent value in US dollars [83]). Kiriga also estimated that the direct cost of treating diabetes in 2000 ranged from Int$876 (US$2302) to Int$1220.6 (US$3207) per person.
One study into the cost of caring for children with T1DM in Sudan found that the mean annual expenditure on diabetes care was US$283 per diabetic child, 36% of which was spent on insulin [81]. A Tanzanian study estimated that in 1989-1990 the total cost of outpatient care for all diabetic patients was US$2.7 million, of which insulin accounted for two-thirds of the expenditure, and total in-patient cost was US$1.25 million [84]. As diabetes care in Tanzania was provided free of charge to users this total cost of US$4 million was paid from the government health budget and accounted for 8% of the government's total health expenditure 1989-1990. A South African study investigated the cost of hyperglycaemic emergency admissions in South Africa over a two month period in 2005 and reported an average cost R5309, equivalent to US$712, per admission [85].
Discussion
Prevalence of diabetes
Prevalence of type 2 diabetes
The prevalence of T2DM appears to have increased considerably from that recorded in earlier (pre-1985) surveys conducted in the region, which found the prevalence in Sub-Saharan Africa was typically below 1%, with the exception of studies in South Africa (3.6%) [86] and the Ivory Coast (5.7% (Zmirou, D. 1979 thesis, reported in McLarty et al 1990 and Motala et al 2003)) [87, 88]. However, many of these early studies may have underestimated prevalence, due to the use of low sensitivity screening methods and non-standardised diagnostic criteria [33, 89, 90].
Impaired Glucose Tolerance (IGT) and Impaired Fasting Glucose (IFG) are predictors of incident T2DM [91]. Thus, a high IGT prevalence alongside a low T2DM prevalence may indicate the early stage of a diabetes epidemic [92]. IGT prevalence suggests that the T2DM prevalence is likely to increase further in several countries in the region, including Cameroon, Ghana and Guinea (Table 1)...
Preventing obesity and increasing level of physical activity is important for reducing the onset of T2DM. Eight T2DM surveys measured the prevalence of obesity among participants, which ranged from 0.2% among rural males in Tanzania [34] to 21% among females in urban Cameroon [24]. The Ministry of Health study in Cameroon reported that controlling obesity and overweight levels would reduce diabetes by 15% in males and 13% in females [24]. The comparatively higher prevalence of T2DM recorded in urban areas was associated with a higher prevalence of obesity among the urban samples and a lower proportion reporting regular physical activity [23, 34]. The projections that by 2025 70% of Africans will live in cities, with a regional annual urban growth rate of 4.5% [93], suggest that levels of obesity and T2DM diabetes will continue to rise in the region [19].
Prevalence of other types of diabetes
As there is very limited data available on other forms of diabetes in the region it is difficult to describe trends. Given the small number and limitations of existing studies, it is not clear whether the very low incidence rates of T1DM of 1-2 per 100,000 are reliable. All the existing studies based their estimates on previously diagnosed cases rather than population screening, and misdiagnosis and high community mortality may leave many cases unknown [20, 39, 68]. This is supported by the observation that T1DM was often first diagnosed when patients presented at healthcare facilities with acute diabetic complications [48, 85]. Similarly, more studies measuring the prevalence of gestational diabetes are needed to determine whether the observed variation from 0 to 9% among pregnant women reflects true regional variation.
Outcomes of diabetes
Mortality and chronic complications
The three studies investigating mortality following diabetes found high proportions, and these may have been underestimates or overestimates due to sampling only selected diagnosed diabetic patients accessing healthcare. More large-scale population-based studies are needed to explore whether the varying diabetes complication proportions in different countries reflect true variation. Small samples sizes and hospital-based recruitment limit the generalisability of these studies.
The observed high mortality in patients with diabetes and high prevalence of diabetes complications is likely to be a consequence of many late diagnosed and poorly controlled cases. Assessing the public health importance of diabetes demands an appreciation of the impact of diabetes on other diseases and population mortality, and in particular the benefits of well-controlled diabetes for averting costly cardiovascular and microvascular complications [7, 94]. The total cost of these complications is likely to far outweigh the cost of effective primary and secondary prevention.
Infections
Potential associations between diabetes and important communicable diseases in the region, particularly tuberculosis and HIV, further complicate the pattern of increasing diabetes prevalence in Sub-Saharan Africa and the challenges posed on resource-constrained health systems. Newer studies primarily outside Sub-Saharan Africa provide evidence on such associations.
A recent meta-analysis of thirteen studies found that diabetes was associated with a 3.1 times elevated risk of tuberculosis [11], and a systematic review of 9 studies found that this increased risk varied from 1.5 to 7.8 [95]. Studies have suggested that 20% of smear-positive tuberculosis in India and 25% of tuberculosis in Mexico is attributable to diabetes [96, 97]. The increased risk of tuberculosis associated with diabetes may be largely attributed to poor glycemic control [98, 99]. Unfortunately, proper epidemiological studies of the diabetes-tuberculosis association from Africa are to our knowledge missing [100].
Meanwhile, the high prevalence of HIV and the roll-out of ART may increase the prevalence of diabetes risk factors and consequently diabetes incidence. Antiretroviral therapy (ART) for HIV, and to a small extent, HIV itself, is associated with an increased risk of developing the metabolic syndrome, which predisposes individuals to develop type 2 diabetes and cardiovascular disease [101]. A range of metabolic changes have been associated with ART, such as increased central obesity [101], increased insulin resistance [102], lipodystophy [103], and dislipidemia [104]. These changes have also been associated, although to a much lesser extent, with untreated HIV[102]. One review found that prevalence of metabolic syndrome among patients on ART ranged between 18 and 33% [105].
Evidence from other countries of the associations between diabetes and a range of other severe infectious diseases also deserves consideration. Type 2 diabetes is associated with a 25-75% increased risk of pneumonia and pneumococcal bacteremia leading to hospitalisation [106–111], and longer duration of diabetes, diabetes complications, and poor long-term glycemic control increase the risk [108, 112]. Diabetes increases the risk of developing severe sepsis, with one study reporting a 2.5-fold increased risk for hospitalization with sepsis in diabetic individuals compared to the general population [110]. Patients with diabetes mellitus have a two to three fold increased risk of bacteremia and sepsis originating from the urinary tract compared with those without diabetes [113]. Among 11 patients newly admitted with type 1 diabetes at a teaching hospital in Nigeria, 9 (82%) presented with urinary tract infection, malaria, or recurrent boils [114]. Bacteremia risk due to hemolytic streptococci and staphylococci is also increased two to three-fold in patients with diabetes [115–117], and often originates from wound infections, which are an important health problem in the region [20].
Projections of future diabetes trends have not considered the potential impact of these associations which could affect the future diabetes burden. Consideration of the associations between diabetes and the other major communicable diseases in the region has been notably absent from the literature - both peer reviewed and grey literature. It is vital that awareness of these associations is promoted so that complementary and integrated programmes in these disease areas can be planned [118].
Access to diagnosis and treatment
The high rates of undiagnosed and uncontrolled diabetes recorded highlight the presence of significant barriers to accessing diagnosis and treatment. The high rates of undiagnosed diabetes suggest that existing screening practices in the region are not effective. Given the reports that health centres lack the necessary diagnostic tools it is also likely that screening for diabetes is not routinely performed.
Several important challenges to accessing diagnosis and treatment have been identified in the literature: the high financial cost of treatment, particularly insulin; the limited availability of diagnostic tools, treatment and glucose monitoring equipment; and a low awareness of diabetes among healthcare professionals which was reported by some authors[40]. Other important barriers may exist that have not yet been identified, as few studies have focused on this issue, and more information on the comparative importance of these factors is necessary to effectively target any interventions.
Economic Impacts of Diabetes
Diabetes is an expensive disease, especially when the cost of complications, including the many diseases where diabetes is an underlying causal factor, is considered. Kiriga's study highlighted the vast expense of treating diabetes in the WHO's African region; however the cost of complications were excluded from the study, and therefore this is a significant underestimate of total cost of diabetes. Kiriga estimated that the direct cost of treating diabetes in 2000 ranged from Int$876 (US$ 2302) to Int$1220.6 (US$3207) per person. Even at this level of direct cost, there is a significant discrepancy between the cost and available expenditure, as the International Diabetes Federation (IDF) has estimated that in 2010 national funding for the healthcare of diabetics in Africa is just US$111 per person, which already amounts to 7% of national healthcare expenditure [119].
With limited national funding, individual patients and their families may have to spend significant proportions of their income on treatment for diabetes, a level of expenditure that may not be sustainable or affordable. The Sudanese study found that families spend an average of US$283 per year caring for their diabetic child, which amounted to 65% of the family's annual expenditure on health. It is possible that in this scenario other health needs are overlooked in order to devote over 50% of annual health expenditure to the one member of the family with diabetes.
The burden of T2DM is disproportionately borne by people of working age [120], which is also the age-group most profoundly affected by HIV in this region. Reducing the economic activity of this group through disease and disability affects both household and national economies. Diabetes therefore not only imposes considerable costs of treatment on families, it also hinders their ability to pay for this treatment through the loss of income of the diabetic member. At a national level an increasing prevalence of diabetes among the economically active, and the high prevalence of diabetic complications and low survival rates, will negatively impact economic development, and in turn the health budget.
Information on the cost of diabetes, including the cost of the complications, is critical for policymakers to highlight the importance of introducing early and cost effective interventions for both primary and secondary prevention.
Conclusion
With increasing prevalence and interactions with other diseases, including the major communicable diseases of the region, diabetes is becoming a pressing public health problem for Sub-Saharan Africa. If effective interventions are implemented in the near-future it may be possible to avert much of this burden, as primary prevention and treatment can reduce the incidence of both diabetes and a range of related diseases where diabetes is a causal factor. However, establishing timely and effective integrated diabetes programmes in the region requires a shift in current public health priorities, and this requires a much better evidence base - both to highlight the scale of the problem and the areas for intervention. Below are a set of recommendations for necessary action in order to address some of the knowledge gaps identified in this article. As identified in the WHO 2008-2013 Action Plan for the Global Strategy on Noncommunicable Diseases, these tasks require comprehensive efforts from multiple stakeholders, including countries, international organisations, academic institutions, civil society and the private sector.
Recommendations
-
1.
Countries, with the assistance from academic institutions, should ensure that local diabetes prevalence and incidence data are collected, for example through the recurring Demographic and Health Surveys, to increase the availability of good information on current epidemiological trends.
-
2.
Academic institutions should collect regional and country-specific data on mortality, morbidity, costs, and access to diagnosis and care.
-
3.
Under the leadership of intergovernmental agencies such as the World Health Organization and the World Bank, models should be developed to assess the public health impact of diabetes in relation to other important diseases, to enable informed prioritisation of available health funding at country level.
-
4.
International agencies, civil society and the private sector should join forces and use their expertise and network to promote awareness of the interactions between diabetes and key communicable diseases in Sub-Saharan Africa, to inform the development of integrated and complimentary service delivery programmes and health policies.
-
5.
International agencies and civil society should establish peer-learning and experience-sharing discussion forums to promote development of feasible and cost-effective strategies and solutions for management and control of diabetes in Sub-Saharan Africa.
References
WHO: The Global Burden of Disease: 2004 Update. 2004, World Health Organisation: Geneva
Sicree R, Shaw J, Zimmet : The Global Burden: Diabetes and Impaired Glucose Tolerance. Diabetes Atlas, IDF. 2009, International Diabetes Federation: Brussels, 4
UNAIDS: 2010 Report on the global AIDS epidemic. 2010, Geneva: UNAIDS
World Health Organisation: WHO Global Tuberculosis Control Report 2010. 2010, WHO: Geneva
World Health Organisation: World Malaria Report 2010. 2010, WHO: Geneva
Saydah SH, et al: Age and the burden of death attributable to diabetes in the United States. Am J Epidemiol. 2002, 156 (8): 714-9. 10.1093/aje/kwf111.
Brown WV: Microvascular complications of diabetes mellitus: renal protection accompanies cardiovascular protection. Am J Cardiol. 2008, 102 (12A): 10L-13L.
Kornum JB, T R, Riis A, Lervang HH, Schønheyder HC, Sørensen HT: Diabetes, glycemic control, and risk of hospitalization with pneumonia: a population-based case-control study. Diabetes Care. 2008, 31 (8): 1541-5. 10.2337/dc08-0138.
Thomsen RW, H H, Lervang HH, Johnsen SP, Schønheyder HC, Sørensen HT: Risk of community-acquired pneumococcal bacteremia in patients with diabetes: a population-based case-control study. Diabetes Care. 2004, 27 (4): 1143-7.
Thomsen RW, H H, Lervang HH, Johnsen SP, Schønheyder HC, Sørensen HT: Diabetes mellitus as a risk and prognostic factor for community-acquired bacteremia due to enterobacteria: a 10-year, population-based study among adults. Clin Infect Dis. 2005, 40 (4): 628-31. 10.1086/427699.
Jeon CY, Murray MB: Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Med. 2008, 5 (7): e152-10.1371/journal.pmed.0050152.
Rudan I, et al: Epidemiology and etiology of childhood pneumonia. Bull World Health Organ. 2008, 86 (5): 408-16. 10.2471/BLT.07.048769.
Seale AC, et al: Maternal and early onset neonatal bacterial sepsis: burden and strategies for prevention in sub-Saharan Africa. Lancet Infect Dis. 2009, 9 (7): 428-38. 10.1016/S1473-3099(09)70172-0.
Mayanja BN, et al: Septicaemia in a population-based HIV clinical cohort in rural Uganda, 1996-2007: incidence, aetiology, antimicrobial drug resistance and impact of antiretroviral therapy. Trop Med Int Health. 15 (6): 697-705.
Reddy EA, Shaw AV, Crump JA: Community-acquired bloodstream infections in Africa: a systematic review and meta-analysis. Lancet Infect Dis. 10 (6): 417-32.
Steen TW, Aruwa JE, Hone NM: The epidemiology of adult lung disease in Botswana. Int J Tuberc Lung Dis. 2001, 5 (8): 775-82.
Lonnroth K, et al: Tuberculosis control and elimination 2010-50: cure, care, and social development. Lancet. 375 (9728): 1814-29.
World Health Organisation: 2008-2013 Action Plan for the Global Strategy for the Prevention and Control of Noncommunicable Diseases. 2008, WHO, Geneva
Levitt NS: Diabetes in Africa: epidemiology, management and healthcare challenges. Heart. 2008, 94 (11): 1376-82. 10.1136/hrt.2008.147306.
Gill GV, et al: A sub-Saharan African perspective of diabetes. Diabetologia. 2009, 52 (1): 8-16. 10.1007/s00125-008-1167-9.
Mbanya JC, et al: Diabetes in sub-Saharan Africa. Lancet. 2010, 375 (9733): 2254-66. 10.1016/S0140-6736(10)60550-8.
Mbanya JC, et al: Standardized comparison of glucose intolerance in west African-origin populations of rural and urban Cameroon, Jamaica, and Caribbean migrants to Britain. Diabetes Care. 1999, 22 (3): 434-40. 10.2337/diacare.22.3.434.
Sobngwi E, et al: Physical activity and its relationship with obesity, hypertension and diabetes in urban and rural Cameroon. Int J Obes Relat Metab Disord. 2002, 26 (7): 1009-16.
MOH: Cameroon Burden of Diabetes Project (Cambod): Baseline Survey Report. 2004, Ministry of Health, Cameroon
Amoah AG, Owusu SK, Adjei S: Diabetes in Ghana: a community based prevalence study in Greater Accra. Diabetes Res Clin Pract. 2002, 56 (3): 197-205. 10.1016/S0168-8227(01)00374-6.
Balde NM, et al: Diabetes and impaired fasting glucose in rural and urban populations in Futa Jallon (Guinea): prevalence and associated risk factors. Diabetes Metab. 2007, 33 (2): 114-20. 10.1016/j.diabet.2006.10.001.
Christensen DL, et al: Prevalence of glucose intolerance and associated risk factors in rural and urban populations of different ethnic groups in Kenya. Diabetes Res Clin Pract. 2009, 84 (3): 303-10. 10.1016/j.diabres.2009.03.007.
Mathenge W, Foster A, Kuper H: Urbanization, ethnicity and cardiovascular risk in a population in transition in Nakuru, Kenya: a population-based survey. BMC Public Health. 10: 569-
Nyenwe EA, et al: Type 2 diabetes in adult Nigerians: a study of its prevalence and risk factors in Port Harcourt, Nigeria. Diabetes Res Clin Pract. 2003, 62 (3): 177-85. 10.1016/j.diabres.2003.07.002.
Oladapo OO, et al: A prevalence of cardiometabolic risk factors among a rural Yoruba south-western Nigerian population: a population-based survey. Cardiovasc J Afr. 21 (1): 26-31.
Erasmus RT, et al: Prevalence of diabetes mellitus and impaired glucose tolerance in factory workers from Transkei, South Africa. S Afr Med J. 2001, 91 (2): 157-60.
Alberts M, et al: Prevalence of cardiovascular diseases and associated risk factors in a rural black population of South Africa. Eur J Cardiovasc Prev Rehabil. 2005, 12 (4): 347-54. 10.1097/01.hjr.0000174792.24188.8e.
Motala AA, et al: Diabetes and other disorders of glycemia in a rural South African community: prevalence and associated risk factors. Diabetes Care. 2008, 31 (9): 1783-8. 10.2337/dc08-0212.
Aspray TJ, et al: Rural and urban differences in diabetes prevalence in Tanzania: the role of obesity, physical inactivity and urban living. Trans R Soc Trop Med Hyg. 2000, 94 (6): 637-44. 10.1016/S0035-9203(00)90216-5.
Maher D, et al: Distribution of hyperglycaemia and related cardiovascular disease risk factors in low-income countries: a cross-sectional population-based survey in rural Uganda. Int J Epidemiol. 40 (1): 160-71.
MOH: National Survey: Zimbabwe Non-Communicable Disease Risk Factors (ZiNCoDs). Preliminary Report. 2005, Ministry of Health and Child Welfare, Zimbabwe
Longo-Mbenza B, et al: Metabolic syndrome, aging, physical inactivity, and incidence of type 2 diabetes in general African population. Diab Vasc Dis Res. 7 (1): 28-39.
Elamin A, Eltayeb B, Tuvemo T: High Incidence of Type I Diabetes Mellitus in Sudanese children. Ann Saudi Med. 1997, 17 (4): 478-480.
Alemu S, et al: Insulin-requiring diabetes in rural Ethiopia: should we reopen the case for malnutrition-related diabetes?. Diabetologia. 2009, 52 (9): 1842-5. 10.1007/s00125-009-1433-5.
Beran D, Yudkin JS, de Courten M: Access to care for patients with insulin-requiring diabetes in developing countries: case studies of Mozambique and Zambia. Diabetes Care. 2005, 28 (9): 2136-40. 10.2337/diacare.28.9.2136.
Swai AB, Lutale JL, McLarty DG: Prospective study of incidence of juvenile diabetes mellitus over 10 years in Dar es Salaam, Tanzania. BMJ. 1993, 306 (6892): 1570-2. 10.1136/bmj.306.6892.1570.
Seyoum B, et al: Prevalence of gestational diabetes mellitus in rural pregnant mothers in northern Ethiopia. Diabetes Res Clin Pract. 1999, 46 (3): 247-51. 10.1016/S0168-8227(99)00101-1.
Mamabolo RL, et al: Prevalence of gestational diabetes mellitus and the effect of weight on measures of insulin secretion and insulin resistance in third-trimester pregnant rural women residing in the Central Region of Limpopo Province, South Africa. Diabet Med. 2007, 24 (3): 233-9. 10.1111/j.1464-5491.2006.02073.x.
Hailu A, Kebede D: High-risk pregnancies in urban and rural communities in central part of Ethiopia. East Afr Med J. 1994, 71 (10): 661-6.
Swai AB, et al: No deterioration of oral glucose tolerance during pregnancy in rural Tanzania. Diabet Med. 1991, 8 (3): 254-7. 10.1111/j.1464-5491.1991.tb01581.x.
Ranchod HA, Vaughan JE, Jarvis P: Incidence of gestational diabetes at Northdale Hospital, Pietermaritzburg. S Afr Med J. 1991, 80 (1): 14-6.
Sobngwi E, Mauvais-Jarvis F, Vexiau P, Mbanya JC, Gautier JF: Diabetes in Africans. Part 1: Epidemiology and clinical specificities. Diabetes and Metabolism. 2001, 628-634. 27
Gill GV, Huddle KR, Monkoe G: Long-term (20 years) outcome and mortality of Type 1 diabetic patients in Soweto, South Africa. Diabet Med. 2005, 22 (12): 1642-6. 10.1111/j.1464-5491.2005.01712.x.
Lester FT: Clinical features, complications and mortality in type 1 (insulin-dependent) diabetic patients in Addis Ababa, Ethiopia, 1976-1990. Q J Med. 1992, 83 (301): 389-99.
McLarty DG, Kinabo L, Swai AB: Diabetes in tropical Africa: a prospective study, 1981-7. II. Course and prognosis. BMJ. 1990, 300 (6732): 1107-10. 10.1136/bmj.300.6732.1107.
Wanjohi FW, et al: Nephropathy in patients with recently diagnosed type 2 diabetes mellitus in black Africans. East Afr Med J. 2002, 79 (8): 399-404.
Ndip EA, Tchakonte B, Mbanya JC: A study of the prevalence and risk factors of foot problems in a population of diabetic patients in cameroon. Int J Low Extrem Wounds. 2006, 5 (2): 83-8. 10.1177/1534734606288413.
Odusan O, Familoni OB, Raimi TH: Correlates of cardiac autonomic neuropathy in Nigerian patients with type 2 diabetes mellitus. Afr J Med Med Sci. 2008, 37 (4): 315-20.
Ahmed AM, Hussein A, Ahmed NH: Diabetic autonomic neuropathy. Saudi Med J. 2000, 21 (11): 1034-7.
Kengne AP, et al: Admission trends over 8 years for diabetic foot ulceration in a specialized diabetes unit in cameroon. Int J Low Extrem Wounds. 2009, 8 (4): 180-6. 10.1177/1534734609349704.
Ogbera AO, et al: An assessment of the disease burden of foot ulcers in patients with diabetes mellitus attending a teaching hospital in Lagos, Nigeria. Int J Low Extrem Wounds. 2006, 5 (4): 244-9. 10.1177/1534734606294538.
Gulam-Abbas Z, et al: Clinical outcome of diabetes patients hospitalized with foot ulcers, Dar es Salaam, Tanzania. Diabet Med. 2002, 19 (7): 575-9. 10.1046/j.1464-5491.2002.00740.x.
Mengesha AY: Spectrum of eye disorders among diabetes mellitus patients in Gaborone, Botswana. Trop Doct. 2006, 36 (2): 109-11. 10.1258/004947506776593576.
Sobngwi E, et al: Microalbuminuria and retinopathy in a diabetic population of Cameroon. Diabetes Res Clin Pract. 1999, 44 (3): 191-6. 10.1016/S0168-8227(99)00052-2.
Seyoum B, et al: Retinopathy in patients of Tikur Anbessa Hospital diabetic clinic. Ethiop Med J. 2001, 39 (2): 123-31.
Rotimi C, et al: Prevalence and determinants of diabetic retinopathy and cataracts in West African type 2 diabetes patients. Ethn Dis. 2003, 13 (2 Suppl 2): S110-7.
Omolase CO, et al: Diabetic retinopathy in a Nigerian community. Singapore Med J. 51 (1): 56-9.
Mwendwa FM, et al: Risk factor profile and the occurrence of microvascular complications in short-term type 2 diabetes mellitus at Kenyatta National Hospital, Nairobi. East Afr Med J. 2005, 82 (12 Suppl): S163-72.
Mwale C, Karimurio J, Njuguna M: Refractive errors in type 2 diabetic patients. East Afr Med J. 2007, 84 (6): 259-63.
Motala AA, et al: Microvascular complications in South African patients with long-duration diabetes mellitus. S Afr Med J. 2001, 91 (11): 987-92.
Read O, Cook C: Retinopathy in diabetic patients evaluated at a primary care clinic in Cape Town. S Afr Med J. 2007, 97 (10): 941-2. 944
Mash B, et al: Screening for diabetic retinopathy in primary care with a mobile fundal camera--evaluation of a South African pilot project. S Afr Med J. 2007, 97 (12): 1284-8.
Majaliwa ES, et al: Survey on acute and chronic complications in children and adolescents with type 1 diabetes at Muhimbili National Hospital in Dar es Salaam, Tanzania. Diabetes Care. 2007, 30 (9): 2187-92. 10.2337/dc07-0594.
Unuigbe EI, et al: Microalbuminuria and associated factors in newly diagnosed diabetics. Niger Postgrad Med J. 2001, 8 (4): 187-92.
Kalk WJ, Joffe BI: Differences in coronary heart disease prevalence and risk factors in African and White patients with type 2 diabetes. Diabetes Res Clin Pract. 2007, 77 (1): 107-12. 10.1016/j.diabres.2006.10.014.
Eghan BA, Frempong MT, Adjei-Poku M: Prevalence and predictors of microalbuminuria in patients with diabetes mellitus: a cross-sectional observational study in Kumasi, Ghana. Ethn Dis. 2007, 17 (4): 726-30.
Agaba EI, Agaba PA, Puepet FH: Prevalence of microalbuminuria in newly diagnosed type 2 diabetic patients in Jos Nigeria. Afr J Med Med Sci. 2004, 33 (1): 19-22.
Adetunji OR, et al: Microalbuminuria and clinical correlates in black African patients with type 2 diabetes. West Afr J Med. 2006, 25 (4): 279-83.
Lutale JJ, et al: Microalbuminuria among Type 1 and Type 2 diabetic patients of African origin in Dar Es Salaam, Tanzania. BMC Nephrol. 2007, 8: 2-10.1186/1471-2369-8-2.
Makuyana D, et al: Asymptomatic bacteriuria among outpatients with diabetes mellitus in an urban black population. Cent Afr J Med. 2002, 48 (7-8): 78-82.
Abbas ZG, Archibald LK: Challenges for management of the diabetic foot in Africa: doing more with less. Int Wound J. 2007, 4 (4): 305-13.
Abbas ZG, Gill GV, Archibald LK: The epidemiology of diabetic limb sepsis: an African perspective. Diabet Med. 2002, 19 (11): 895-9. 10.1046/j.1464-5491.2002.00825.x.
Beran D, Yudkin JS: Looking beyond the issue of access to insulin: What is needed for propoer Diabetes care in resource-poor settings. Diabetes Atlas, IDF. 2009, International Diabetes Federation: Brussels, 4
Mendis S, et al: The availability and affordability of selected essential medicines for chronic diseases in six low- and middle-income countries. Bull World Health Organ. 2007, 85 (4): 279-88. 10.2471/BLT.06.033647.
Neuhann HF, et al: Diabetes care in Kilimanjaro region: clinical presentation and problems of patients of the diabetes clinic at the regional referral hospital-an inventory before structured intervention. Diabet Med. 2002, 19 (6): 509-13. 10.1046/j.1464-5491.2002.00673.x.
Elrayah H, et al: Economic burden on families of childhood type 1 diabetes in urban Sudan. Diabetes Res Clin Pract. 2005, 70 (2): 159-65. 10.1016/j.diabres.2005.03.034.
Kirigia JM, et al: Economic burden of diabetes mellitus in the WHO African region. BMC Int Health Hum Rights. 2009, 9: 6-10.1186/1472-698X-9-6.
International Monetary Fund: World Economic Outlook Database, April. 2009, [cited 2011 06/04/2011]
Chale SS, S A, Mujinja PGM, McLarty DG: Must diabetes be a fatal disease in Africa? Study of costs of treatment. BMJ. 1992, 1215-18. 304
Pepper DJ, et al: Hyperglycaemic emergency admissions to a secondary-level hospital - an unnecessary financial burden. S Afr Med J. 2007, 97 (10): 963-7.
Marine N, et al: Diabetes, hyperglycemia and glycosuria among Indians, Malays and Africans (Bantu) in Cape Town, South Africa. Diabetes. 1969, 18 (12): 840-57.
Motala AA, Omar MA, Pirie FJ: Diabetes in Africa. Epidemiology of type 1 and type 2 diabetes in Africa. J Cardiovasc Risk. 2003, 10 (2): 77-83. 10.1097/00043798-200304000-00002.
McLarty DG, Pollitt C, Swai AB: Diabetes in Africa. Diabet Med. 1990, 7 (8): 670-84. 10.1111/j.1464-5491.1990.tb01470.x.
Faeh D, et al: Prevalence, awareness and control of diabetes in the Seychelles and relationship with excess body weight. BMC Public Health. 2007, 7: 163-10.1186/1471-2458-7-163.
Levitt NS, et al: Application of the new ADA criteria for the diagnosis of diabetes to population studies in sub-Saharan Africa. American diabetes association. Diabet Med. 2000, 17 (5): 381-5. 10.1046/j.1464-5491.2000.00264.x.
Shaw JE, et al: Impaired fasting glucose or impaired glucose tolerance. What best predicts future diabetes in Mauritius?. Diabetes Care. 1999, 22 (3): 399-402. 10.2337/diacare.22.3.399.
Motala AA: Diabetes trends in Africa. Diabetes Metab Res Rev. 2002, 18 (Suppl 3): S14-20.
UN-HABITAT: State of the World's Cities: Trends in Sub-Saharan Africa. 2004, UN-HABITAT: Nairobi
Holman RR, et al: 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. N Engl J Med. 2008, 359 (15): 1577-1589. 10.1056/NEJMoa0806470.
Stevenson CR, et al: Diabetes and the risk of tuberculosis: a neglected threat to public health?. Chronic Illn. 2007, 3 (3): 228-45. 10.1177/1742395307081502.
Stevenson CR, et al: Diabetes and tuberculosis: the impact of the diabetes epidemic on tuberculosis incidence. BMC Public Health. 2007, 7: 234-10.1186/1471-2458-7-234.
Ponce-De-Leon A, et al: Tuberculosis and diabetes in southern Mexico. Diabetes Care. 2004, 27 (7): 1584-90. 10.2337/diacare.27.7.1584.
Leung CC, et al: Diabetic control and risk of tuberculosis: a cohort study. Am J Epidemiol. 2008, 167 (12): 1486-94. 10.1093/aje/kwn075.
Pablos-Mendez A, Blustein J, Knirsch CA: The role of diabetes mellitus in the higher prevalence of tuberculosis among Hispanics. Am J Public Health. 1997, 87 (4): 574-9. 10.2105/AJPH.87.4.574.
Dooley KE, Chaisson RE: Tuberculosis and diabetes mellitus: convergence of two epidemics. Lancet Infect Dis. 2009, 9 (12): 737-46. 10.1016/S1473-3099(09)70282-8.
Young FCJ, Johnstone LK, Unwin NC: A review of co-morbifity between infectious and chronic disease in Sub Saharan Africa: TB and Diabetes Mellitus, HIV and Metabolic Syndrome. Globalization and Health. 2009, 5 (9):
Grinspoon SK: Metabolic syndrome and cardiovascular disease in patients with human immunodeficiency virus. Am J Med. 2005, 118 (Suppl 2): 23S-28S.
Mallon PW, Cooper DA, Carr A: HIV-associated lipodystrophy. HIV Med. 2001, 2 (3): 166-73. 10.1046/j.1468-1293.2001.00071.x.
Lichtenstein KA, et al: Clinical assessment of HIV-associated lipodystrophy in an ambulatory population. AIDS. 2001, 15 (11): 1389-98. 10.1097/00002030-200107270-00008.
Jevtovic DJ, et al: The metabolic syndrome, an epidemic among HIV-infected patients on HAART. Biomed Pharmacother. 2009, 63 (5): 337-42. 10.1016/j.biopha.2008.09.011.
Benfield T, Jensen JS, Nordestgaard BG: Influence of diabetes and hyperglycaemia on infectious disease hospitalisation and outcome. Diabetologia. 2007, 50 (3): 549-54. 10.1007/s00125-006-0570-3.
Muller LM, et al: Increased risk of common infections in patients with type 1 and type 2 diabetes mellitus. Clin Infect Dis. 2005, 41 (3): 281-8. 10.1086/431587.
Kornum JB, et al: Diabetes, glycemic control, and risk of hospitalization with pneumonia: a population-based case-control study. Diabetes Care. 2008, 31 (8): 1541-5. 10.2337/dc08-0138.
Jackson ML, et al: The burden of community-acquired pneumonia in seniors: results of a population-based study. Clin Infect Dis. 2004, 39 (11): 1642-50. 10.1086/425615.
Shah BR, Hux JE: Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care. 2003, 26 (2): 510-3. 10.2337/diacare.26.2.510.
O'Meara ES, et al: Hospitalization for pneumonia in the Cardiovascular Health Study: incidence, mortality, and influence on longer-term survival. J Am Geriatr Soc. 2005, 53 (7): 1108-16. 10.1111/j.1532-5415.2005.53352.x.
Thomsen RW, et al: Risk of community-acquired pneumococcal bacteremia in patients with diabetes: a population-based case-control study. Diabetes Care. 2004, 27 (5): 1143-7. 10.2337/diacare.27.5.1143.
Thomsen RW, et al: Diabetes mellitus as a risk and prognostic factor for community-acquired bacteremia due to enterobacteria: a 10-year, population-based study among adults. Clin Infect Dis. 2005, 40 (4): 628-31. 10.1086/427699.
Adeleke SI, et al: Childhood diabetes mellitus in Kano, North West, Nigeria. Niger J Med. 2010, 19 (2): 145-7.
Factor SH, et al: Invasive group A streptococcal disease: risk factors for adults. Emerg Infect Dis. 2003, 9 (8): 970-7.
Jackson LA, et al: Risk factors for group B streptococcal disease in adults. Ann Intern Med. 1995, 123 (6): 415-20.
Laupland KB, Ross T, Gregson DB: Staphylococcus aureus bloodstream infections: risk factors, outcomes, and the influence of methicillin resistance in Calgary, Canada, 2000-2006. J Infect Dis. 2008, 198 (3): 336-43. 10.1086/589717.
Maher D, Smeeth L, Sekajugo J: Health transition in Africa: practical policy proposals for primary care. Bull World Health Organ. 88 (12): 943-8.
Zhang PZX, Brown JB, Vistisen D, Sicree RA, Shaw J, Nichols GA: Economic Impact of Diabetes. Diabetes Atlas, IDF. 2009, International Diabetes Federation: Brussels, 4
Bradshaw D, et al: Estimating the burden of disease attributable to diabetes in South Africa in 2000. S Afr Med J. 2007, 97 (8 Pt 2): 700-6.
Okesina AB, et al: Prevalence of some risk factors of coronary heart disease in a rural Nigerian population. East Afr Med J. 1999, 76 (4): 212-6.
Erasmus RT, et al: Assessment of glycaemic control in stable type 2 black South African diabetics attending a peri-urban clinic. Postgrad Med J. 1999, 75 (888): 603-6.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/11/564/prepub
Acknowledgements and Financial support
Department of Clinical Epidemiology is a member of the Danish Centre for Strategic Research in Type 2 Diabetes (the Danish Research Council, grant no. 09-075724 and 10-079102).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
VH undertook this review as a consultant for Novo Nordisk A/S. NL and OH are both employees of Novo Nordisk A/S.
Authors' contributions
NL and OH conceived the study and wrote the analysis plan. VH conducted the literature review and analysis and wrote the first draft manuscript. NL, RWT and OH reviewed the draft manuscript, provided critical comments and suggested additional analyses. VH finalised the manuscript which was subsequently approved by all authors.
Electronic supplementary material
12889_2010_3359_MOESM1_ESM.DOC
Additional file 1: Annex 1: Flow Diagram of Studies Reviewed. This is a flow diagram of the studies reviewed in this systematic review. (DOC 45 KB)
12889_2010_3359_MOESM2_ESM.DOC
Additional file 2: Annex 2: Keyword search terms. This describes the keywords used to perform the literature search. (DOC 30 KB)
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Hall, V., Thomsen, R.W., Henriksen, O. et al. Diabetes in Sub Saharan Africa 1999-2011: Epidemiology and public health implications. a systematic review. BMC Public Health 11, 564 (2011). https://doi.org/10.1186/1471-2458-11-564
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-11-564