
Abstract
Introduction
Acute liver failure (ALF) is an indication for emergency liver transplantation (LT). Although centers performing only deceased donor liver transplants (DDLT) have shown improved outcomes in this situation, they still have relatively long waiting lists. An alternative would be living donor liver transplantation (LDLT), which has shown equivalent outcomes in the elective situation but there is limited evidence of its results in ALF.
Aim
The purpose of this study was to assess the outcomes in patients with ALF undergoing emergency LDLT in our center in Delhi, India.
Methods
We prospectively collected data on 479 patients who underwent LT in our hospital between January 2009 and December 2015 to evaluate the outcomes of those with ALF. The ALF patients were listed for transplantation after they met the Kings’ College criteria and rapid evaluation was done following a protocol consisting of three phases. Patients with grade III/IV encephalopathy were put on mechanical ventilation. Data regarding their postoperative course, morbidity, and mortality were analyzed.
Results
Thirty-six (7.5%) out of the 479 patients underwent emergency LT for ALF. Their mean age was 27.5 years (range 4–59 years) and the male to female ratio of 2:3. Preoperative intubation was required in 15 of 25 patients who had encephalopathy. Wilson’s disease was the most common cause of ALF in children while in adults, it was acute viral hepatitis. The time interval between listing and transplantation was a mean of 36 ± 12.4 h. The mean graft to recipient weight ratio (GRWR) was 1.06 ± 0.3. The recipients were extubated postoperatively after a mean period of 2.6 days and their mean ICU stay was 6.3 days. Postoperative infection was the most common complication and required upgradation of antifungal and antibiotic treatments. Neurological complications occurred in five patients. Thirty-one of 36 (86.1%) patients survived and progressive cerebral edema and sepsis were the most common causes of mortality. Patients who died had higher model for end-stage liver disease scores, longer cold ischemia time (CIT), and higher grades of encephalopathy (though 80% patients with encephalopathy survived). There was no donor mortality. At long-term follow up of a median of 56 months, 29 (80.5%) of 36 patients were still alive.
Conclusions
In our experience, LDLT is an alternative procedure to DDLT in patients with ALF and is associated with good outcomes even in patients with high grades of encephalopathy.
Similar content being viewed by others


Introduction
Acute liver failure (ALF) is a grade I indication of listing for liver transplantation. In the pretransplant era, the outlook in patients with ALF was very poor with the Mayo Clinic reporting only 6% survival [1] but after the introduction of liver transplantation for this near fatal disease, the survival rate has improved and Bismuth et al. reported a 1-year survival of 68% after liver transplants [2]. However, most of the data on liver transplantation for ALF has come from centers doing deceased donor transplants (DDLT). A living donor liver transplant (LDLT) has certain advantages—it avoids the recipient being on a waiting list, reduces the shortage of organs and, most important, is the only option available in many countries where deceased donors are still not available. In our institution, we have been performing LDLT for patients in acute liver failure and herein present our experience.
Methods
We retrospectively analyzed, from a prospectively collected database, the details of all patients who had undergone LDLT for ALF between January 2009 and December 2015. The data was compiled from an electronically collected database, the patient’s files, and our hospital information system.
Inclusion criteria
All the patients underwent liver transplant for ALF in accordance with the King’s College criteria.
Evaluation and management
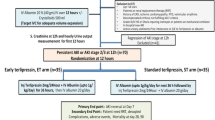
The patients with a diagnosis of ALF were managed according to the American Association for the Study of Liver Disease (AASLD) guidelines. The recipient evaluation was started soon after admission and the family counseled about the prognosis and possible need for a liver transplant. Patients with hepatic encephalopathy were managed in the intensive care unit (ICU) for monitoring and patients with grade III–IV encephalopathy were electively intubated for airway protection (we do not routinely perform invasive intra-cerebral pressure monitoring). All the patients were evaluated and listed for liver transplantation if they met King’s College criteria. Urgent donor work up was done according to a set protocol (Fig. 1). The donor was first explained all the details regarding the procedure and complications associated with liver transplantation, at the time of family counseling. The donor was again counseled by different doctors at the time of clearance in a five-step manner. A psychiatric consultation was obtained for this very purpose. The donor then appeared in front of an authorization committee where there was no doctor from the treating team and assessed for coercion. After several such discussions, the written informed consent was obtained. All the patients with encephalopathy underwent a CT scan of the brain and clearance by a neurologist before undergoing a liver transplant. Donors with a body mass index (BMI) > 30 kg/m2 and/or liver attenuation index (LAI) < 0 were rejected. A government nominated authorization committee was summoned urgently with the help of hospital administration, which cleared all the procedures and also evaluated the donors for willingness to undergo the operation. A porto-caval shunt was routinely created in all the patients after the explant procedure.

Work up protocol of the recipient and donor NCCT non-contrast computerized tomography; MRCP magnetic resonance cholangio-pancreatography
The donors were kept for a day and the recipients were kept in the ICU till they were deemed fit to be transferred. All the recipients were managed with triple immunosuppression drugs with corticosteroids starting on day 1 and tacrolimus and mycophenolate were introduced depending on the patient’s condition and laboratory values.
Follow up
Patients were followed up regularly after discharge from hospital through out patient visits, emails, and telephonic conversations.
Data analysis
The data collected included the patient’s demographics, intervals between jaundice and encephalopathy and encephalopathy to liver transplant as well as intraoperative factors such as cold ischemia time (CIT), warm ischemia time (WIT), blood loss, and graft weight. Postoperative stay, morbidity including neurological complications and mortality were also recorded to assess outcomes. The factors associated with mortality were analyzed. We also studied the patients with high-grade encephalopathy as a separate group to assess their differences from patients without high-grade encephalopathy.
Statistical analysis
The continuous variables were expressed as means and medians. Categorical variables were represented as percentages. The Mann-Whitney U test was used to test the statistical difference between the groups for various factors affecting mortality. A “p” value less than 0.05 was taken to be significant. The calculations were performed using the SPSS statistical software, version 17.0.
Results
During the study period, out of 479 patients who underwent liver transplantation, 36 (7.5%) were done for ALF. The mean age of the adults in this study group was 35.8 years (19–59) and 12 of the transplants were done in children who had a mean age of 9.1 years (4–17). The male:female ratio was 2:3.
Wilson’s disease was the most common cause of ALF in children (Fig. 2) while hepatitis A and E (HAV and HEV) were also responsible in one each. In adults, viral hepatitis in the form of HEV, HAV, and hepatitis B (HBV) were the leading causes of liver failure (Fig. 3). Antitubercular drugs (ATT) were the cause in four patients.

Etiology of acute liver failure in children. HAV hepatitis A virus; HEV hepatitis E virus

Etiology of acute liver failure in adults. ATT anti-tubercular toxicity; HEV, HAV, and HBV hepatitis E, A, and B viruses, respectively
Most of the patients (23 [64%]) required ICU care preoperatively and 15 (42%) were intubated for high-grade encephalopathy. The median period between the onset of jaundice and encephalopathy was 9 days (3–20 days). The mean period from listing for transplant to surgery was 36 ± 12.4 h (6–70 h). The mean model for end-stage liver disease (MELD) score of the patients at the time of transplant was 30.2 ± 9.7 (21–40) and the mean pediatric end-stage liver disease (PELD) score was 33.2±5.6 (27–40). Two patients had deranged renal function without having been on dialysis or having a previous history of renal dysfunction or any evidence of systemic infection.
All the adults received a right lobe graft. Among the children, the left lobe was implanted in 9, right lobe in 2, and the left lateral lobe in 1. The mean CIT was 81.7 ± 30.2 (35–160) minutes and mean WIT was 54.4 ± 21.1 (25–144) minutes. The mean graft to recipient weight ratio (GRWR) was 1.06 ± 0.3 (0.76–1.7). The mean operative time was 618 ± 149 (390–1070) minutes and mean blood transfusion requirement was 3.5 ± 2.9 (1–11) units.
Siblings (brothers and sisters) were the most common donors in 14 and mothers in 11 patients. Aunts, uncles, and nieces were the donors in the other 11 patients. All the transplants were ABO compatible. Of these donors, 19 were females and 17 were males. Their mean age was 40 years (28–55) and mean BMI was 23.6 ± 3.6 (20.7–29.2). None of the donors had steatosis of more than 15%.
Postoperatively, the recipients were extubated after a mean period of 2.6 ± 1.8 (0–9 days) and their mean ICU stay was 6.29 ± 2.7 (3–15 days). Three patients had fungal infections in the postoperative period and in five patients, antibiotics were upgraded because of increasing total leukocyte counts. Two patients required bronchoscopy for mucus plugs with lung collapse and three required psychiatric consultation in the postoperative period. One patient had convulsions and another had quadriparesis following transplantation which were managed conservatively. The quadriparesis improved 3 months after the transplant. Rejection during the postoperative period occurred in only two patients. Clavien’s grade II complications were most commonly seen in 12 patients, 4 patients had grade III complications and 6 had grade I complications. There was no vascular complication noted in the postoperative period. The recipients were discharged after mean period of 15.5 ± 4.6 (8–27 days).
Thirty-one of 36 (86.1%) patients survived. The deaths were due to progressive cerebral edema even after transplant in three and sepsis in two patients. There was no death in the pediatric age group. On long-term follow up, one patient died after 12 months with a fungal infection of the chest and one after 15 months because of chronic rejection. On long-term follow up of 56 months (median), 29 (80.5%) of 36 patients are still alive. There was no mortality among the donors who were discharged after a mean period of 6±1.2 days. They also had no major Clavien’s grade III/IV morbidity.
On further analysis (Table 1), preoperative factors like older age, male gender, higher MELD score, and higher grade of encephalopathy and operative factors like a longer CIT and WIT were associated with higher mortality.
Patients with higher grades of encephalopathy did not differ from other patients in their demographic characteristics and preoperative and operative parameters; however, they did have a significantly higher mortality (p = 0.009). Twenty of 25 (80%) patients with encephalopathy survived.
Discussion
Our experience demonstrates that LDLT for ALF is a life saving procedure in most patients. With advances in surgical techniques, anesthesia, and critical care management, the survival in patients undergoing liver transplant has improved with data European Liver Transplant Registry (ELTR) of 20 years reporting 1-and 5-year survivals of 74% and 68% and 1-and 5-year survivals in the last 5 years of 79% and 72% [3]. DDLT still has a high waiting list mortality because of a shortage of donors. LDLT helps to reduce waiting list mortality [4] and has shown results comparable to DDLT. A Chinese study [5] reported 1- and 3-year survivals of 65% while a Japanese report [6] on 212 patients with ALF reported 1-and 5-year survivals of 79% and 74%, respectively. A study from Pittsburgh [7] comparing LDLT and DDLT showed a similar 5-year survival of 71%. However, a significantly higher survival for LDLT in pediatric patients was shown by a study from Chicago [8] with a longer CIT and waiting time with DDLT. Though the number of patients in LDLT/DDLT groups in these studies was not comparable, it does support LDLT to be an acceptable alternative. In the present study, the 1-year survival of the patients was 86.1% and 80.5% of patients are alive after a median follow up of 56 months. The word “improving” has been used to show the better results obtained from LDLT in ALF than those seen previously and when the procedure was not considered to be an option in this grave situation. The results are more encouraging when we see the number of these patients with severe encephalopathy. The study highlights the comparability and the trend towards better results than quoted in the discussion to suggest that LDLT may be an effective option for patients even in western world.
Hepatic encephalopathy has been shown to affect outcomes in patients with ALF. In our study, the measures for decreasing cerebral edema initiated before LT were continued into the postoperative period. Some studies have quoted cerebral edema to be a poor prognostic factor with Chan et al. [9] reported 64% peri-operative mortality in these patients. We did not perform invasive cerebral monitoring routinely as it is still controversial and carries an increased risk of infection and bleeding [10, 11]. Patients with high-grade encephalopathy had a higher mortality compared to other patients, though both the groups were not different on subgroup analysis. The long-term data from the King’s College [12] have shown better survival in patients with cerebral edema and similarly in our study, 20 of 25 patients with encephalopathy survived.
Various studies have shown a prolonged CIT to be associated with delayed graft functioning and primary nonfunction (PNF) mainly in DDLT and has also been found to correlate with adverse outcomes in LDLT [13]. The plausible explanation of this in LDLT has been the combined effect of the partial graft with longer CIT leading to slower resolution of cerebral edema. In ALF, early graft functioning leads to a faster resolution of cerebral edema and better survival. In the present study, a prolonged CIT was associated with a higher mortality. Studies from the western literature [9, 14] have raised concern about the quality of graft accepted in DDLT centers with extended criteria grafts and ABO incompatible grafts being used and reported PNF as a cause of mortality. A large study from Japan also quoted incompatible blood group to be associated with higher short-term mortality [6]. Extended criteria grafts may not function well after implantation and do not decrease cerebral edema rapidly and may hence be responsible for an increased mortality. In our study, most of the donors were young (the oldest being 55 years) and all the grafts were ABO compatible and this may be the reason for our good results.
The period from jaundice to encephalopathy was only 9 days and some studies showed that the shorter the period between jaundice and encephalopathy the better the survival. Most of our patients were extubated early within a mean period of 2.6 days. In spite of preoperative intubation in 40% of the patients, the mean ICU stay of patients with encephalopathy was only 6.3 days and 80% of these patients survived. Neurological complications are known to occur in these patients. In the west, psychiatric consultation is common as paracetamol overdose is the main etiology and patients have committed suicide even after transplant leading to a drop in survival rates [3]. In the present study, most of the patients were young and not previously suffering from any disease but still required psychiatric consultation to help them accept the disease and the outcome of liver transplantation. The family structure in India is helpful in this regard but with increasing urbanization, psychiatric consultation may become a regular part of post-transplant protocol.
We found that the majority of deaths occurred soon after transplantation in keeping with the ELTR data which also points to maximum risk of death soon after transplant [3]. Farmer et al. also showed that deaths due to sepsis and multi-organ failure were the most common causes of graft loss [15]. The MELD score and preoperative ventilatory requirement were both indirect indicators of the severity of sickness and were associated with a significantly higher mortality in our patients. Perhaps the prolonged ICU stay and multiple invasive lines predispose them to a higher risk for infection. These patients have usually been on broad spectrum antibiotics for long periods (both for prophylaxis and diagnosed infections) and have a high incidence of fungal and other opportunistic infections which have been reported from many centers [3, 8]. In our study, three patients died from sepsis and one died after 1 year with a fungal infection of the chest. Two patients were diagnosed with fungal infections in early postoperative period but recovered after appropriate treatment. Early decision-making and rapid work up with good critical care, which avoids prolonged and inappropriate antibiotic use helps in decreasing the resistance, incidence of opportunistic infections, cost and thereby mortality. The short period from listing to surgery in this study possibly helped us to avoid prolonged preoperative stay and antibiotic use.
Paracetamol has been quoted to be the most common etiology of ALF in the studies from US [15] and ELTR [3] data though its incidence is coming down because of legislation restricting its sales. Acharya et al. [16] and Pandit et al. [17] have identified hepatitis A and E to be the most common causes of ALF in India compared to other Asian countries where hepatitis B is the most common cause [18]. Immunization has helped to decrease incidence of hepatitis A in the west. Kumar et al. have reported ATT as the most common cause of drug-induced ALF in this region [19]. ATT-induced liver injury is a diagnosis of exclusion and viral hepatitis must be ruled out before making this diagnosis. ATT was reintroduced in these patients at a lower dose with close monitoring. Few studies have shown better outcomes with drug-induced hepatitis but in these, acetaminophen was the cause.
Kumar et al. proposed a dynamic model “ALF early dynamic (ALFED) model”and shown it to be a better model than King’s College criteria in their study [20]. The ALF study group (ALFSG) also proposed a model which was shown to be better than King’s College criteria. However, none of these have been validated sufficiently to be used in routine clinical practice. The King’s College criteria have been validated in a number of studies [21] and have shown a high positive predictive value (80% in paracetamol-induced ALF and 70–> 90% in non-paracetamol ALF) but lower negative predictive value especially in non-paracetamol-induced liver failure. Thus, King’s College criteria were chosen in the present study to allow comparability.
The donor evaluation period was short with counseling done by transplant coordinators, psychiatrists, and doctors at different stages to reduce any element of coercion. Most of the donors were siblings and emotional attachment was present but the option of withdrawal was always offered at different levels of evaluation by us as well as by other members of the authorization committee who are not a part of our institution. We were pleased that there was no donor mortality and no major Clavien’s grade III or IV morbidity in this study.
The major limitation of this study is the unavailability of data on all the patients who presented with ALF, as most of these patients were referred only after they met King’s College criteria. The study is also a single center experience and may not represent the wider Indian experience.
Hence, we can conclude from our study that LDLT is associated with good outcomes in patients with ALF. Partial grafts from healthy donors, with short CIT, ensure good results even in patients with high grades of encephalopathy.
References
Rakela J, Lange SM, Ludwig J, Baldus WP. Fulminant hepatitis: Mayo Clinic experience with 34 cases. Mayo Clin Proc. 1985;60:289–92
Bismuth H, Samuel D, Castaing D, et al. Liver transplantation in fulminant and subfulminant hepatitis. Ann Surg. 1995;222:109–19
Germani G, Theocharidou E, Burroughs AK, et al. Liver transplantation for acute liver failure in Europe: outcomes over 20 years from the ELTR database. J Hepatol. 2012;57:288–96
Russo MW, LaPointe-Rudow D, Kinkhabwala M, Emond J, Brown RS Jr. Impact of adult living donor liver transplantation on waiting time survival in candidates listed for liver transplantation. Am J Transplant. 2004;4:427–31
Yuan D, Liu F, Chen KF, et al. Adult-to-adult living donor liver transplantation for acute liver failure in China. World J Gastroenterol. 2012;18:7234–41
Yamashiki N, Sugawara Y, Kokudo N, et al. Outcomes after living donor livertransplantation for acute liver failure in Japan: results of a nationwide survey. Liver Transpl. 2012;18:1069–77
Urrunaga NH, Rachakonda VP, Magder LS, Mindikoglu AL. Outcomes of living versus deceased donor liver transplantation for acute liver failure in the United States. Transplant Proc. 2014;46:219–24
Mack CL, Ferrario M, Abecassis M, Whitington PF, Superina RA, Alonso EM. Living donor liver transplantation for children with liver failure and concurrent multiple organ system failure. Liver Transpl. 2001;7:890–5
Chan G, Taqi A, Marotta P, et al. Long-term outcomes of emergency liver transplantation for acute liver failure. Liver Transpl. 2009;15:1696–702
Vaquero J, Fontana RJ, Blei AT, et al. Complications and use of intracranial pressure monitoring in patients with acute liver failure and severe encephalopathy. Liver Transpl. 2005;11:1581–9
Gasco J, Rangel-Castilla L, Franklin B, Thomas PG, Patterson JT. State-of-the-art management and monitoring of brain edema and intracranial hypertension in fulminant hepatic failure. A proposed algorithm. Acta Neurochir Suppl. 2010;106:311–4
Bernal W, Hyyrylainen A, Gera A, et al. Lessons from look-back in acute liver failure? A single centre experience of 3300 patients. J Hepatol. 2013;59:74–80
Olthoff KM, Merion RM, Emond JC, et al. A2ALL Study Group. Outcomes of 385 adult-to-adult living donor liver transplant recipients. Ann Surg. 2005;242:314–25.
Detry O, De Roover A, Honoré P, et al. Cadaveric liver transplantation for non-acetaminophen fulminant hepatic failure: a 20-year experience. World J Gastroenterol. 2007;13:1427–30
Farmer DG, Anselmo DM, Busuttil RW, et al. Liver transplantation for fulminant hepatic failure. Ann Surg. 2003;237:666–76
Acharya SK, Batra Y, Hazari S, Choudhury V, Panda SK, Dattagupta S. Aeopathogenesis of acute hepatic failure: eastern versus western countries. J Gastroenterol Hepatol. 2002;17:S268–73
Pandit A, Mathew LG, Bavdekar A, et al. Hepatotropic viruses as etiological agents of acute liver failure and related-outcomes among children in India: a retrospective hospital-based study. BMC Res Notes. 2015;8:381
Park SJ, Lim YS, Lee SG, et al. Emergency adult-to-adult living-donor liver transplantation for acute liver failure in a hepatitis B virus endemic area. Hepatology. 2010;51:903–11
Kumar R, Shalimar, Bhatia V, et al. Antituberculosis therapy-induced acute liver failure: magnitude, profile, prognosis, and predictors of outcome. Hepatology. 2010;51:1665–74
Kumar R, Shalimar, Sharma H, et al. Prospective derivation and validation of early dynamic model for predicting outcome in patients with acute liver failure. Gut. 2012;61:1068–75
McPhail MJ, Wendon JA, Bernal W. Meta-analysis of performance of Kings’s College Hospital Criteria in prediction of outcome in non-paracetamol-induced acute liver failure. J Hepatol. 2010;53:492–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
SM, NM, PSR, SL, VM, and SN declare that they have no conflict of interest.
Ethics statement
The study was performed conforming to the Helsinki Declaration of 1975, as revised in 2000 and 2008 concerning human and animal rights, and the authors followed the policy concerning informed consent as shown on Springer.com.
Rights and permissions
About this article

Cite this article
Mehrotra, S., Mehta, N., Rao, P.S. et al. Live donor liver transplantation for acute liver failure: A single center experience. Indian J Gastroenterol 37, 25–30 (2018). https://doi.org/10.1007/s12664-017-0812-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12664-017-0812-y