
Abstract
Background
Numerous factors influence total hip arthroplasty (THA) stability including surgical approach and soft tissue tension, patient compliance, and component position. One long-held tenet regarding component position is that cup inclination and anteversion of 40° ± 10° and 15° ± 10°, respectively, represent a “safe zone” as defined by Lewinnek that minimizes dislocation after primary THA; however, it is clear that components positioned in this zone can and do dislocate.
Questions/purposes
We sought to determine if these classic radiographic targets for cup inclination and anteversion accurately predicted a safe zone limiting dislocation in a contemporary THA practice.
Methods
From a cohort of 9784 primary THAs performed between 2003 and 2012 at one institution, we retrospectively identified 206 THAs (2%) that subsequently dislocated. Radiographic parameters including inclination, anteversion, center of rotation, and limb length discrepancy were analyzed. Mean followup was 27 months (range, 0–133 months).
Results
The majority (58% [120 of 206]) of dislocated THAs had a socket within the Lewinnek safe zone. Mean cup inclination was 44° ± 8° with 84% within the safe zone for inclination. Mean anteversion was 15° ± 9° with 69% within the safe zone for anteversion. Sixty-five percent of dislocated THAs that were performed through a posterior approach had an acetabular component within the combined acetabular safe zones, whereas this was true for only 33% performed through an anterolateral approach. An acetabular component performed through a posterior approach was three times as likely to be within the combined acetabular safe zones (odds ratio [OR], 1.3; 95% confidence interval [CI], 1.1–1.6) than after an anterolateral approach (OR, 0.4; 95% CI, 0.2–0.7; p < 0.0001). In contrast, acetabular components performed through a posterior approach (OR, 1.6; 95% CI, 1.2–1.9) had an increased risk of dislocation compared with those performed through an anterolateral approach (OR, 0.8; 95% CI, 0.7–0.9; p < 0.0001).
Conclusions
The historical target values for cup inclination and anteversion may be useful but should not be considered a safe zone given that the majority of these contemporary THAs that dislocated were within those target values. Stability is likely multifactorial; the ideal cup position for some patients may lie outside the Lewinnek safe zone and more advanced analysis is required to identify the right target in that subgroup.
Level of Evidence
Level III, therapeutic study.
Similar content being viewed by others


Introduction
Dislocation is among the most common complications after primary THA with an estimated range between 0% and 5% [12, 14, 22, 30, 32]. Approximately 50% of dislocations occur within the first 3 months after the index procedure, and more than 75% occur within the first year [7]. Within the first 2 years postoperatively, dislocation is the most common cause for revision surgery [8]. Unfortunately, revision surgery to treat hip instability, ranging from “simple” head and liner exchange to all-component revision or use of constrained devices, has met with variable success [6, 11, 26, 30, 32].
The positioning of implants, restoration of joint biomechanics, and appropriate soft tissue preservation and tensioning are known to play a role in obtaining a stable THA [13, 15, 16]. In addition, head size, cup diameter, and the surgical approach itself may influence hip stability [16, 17, 34]. In an often cited paper, Lewinnek et al. proposed a “safe zone” of cup inclination of 40° ± 10° and anteversion of 15° ± 10° to minimize dislocation risk after primary THA [20]. In their paper, all procedures were completed through a posterolateral approach. However, even if the implants are oriented based on this safe zone, dislocations still occur [1, 17].
The primary goal of this study was to determine if the radiographic target values for cup inclination and anteversion proposed as the Lewinnek et al. safe zone accurately predicted dislocation in a contemporary THA practice. The secondary goal was to determine if the achievement of these radiographic target values varied based on surgical approach.
Patients and Methods
All patients who had a dislocation after a primary THA completed at our institution between 2003 and 2012 were identified. Patients were identified through our total joint registry, which has followed all patients with a THA since 1969. Clinical and radiographic followup was performed at 3 months, 1 year, 2 years, 5 years, and then every 5 years thereafter. Patients who were unable to return for followup were mailed a questionnaire and were asked to return radiographic images. If they did not respond, they were contacted by telephone. Dislocations were defined as any episode that required closed or open reduction or a revision arthroplasty. Two percent of living patients did not have a minimum of 2 years of followup. The study cohort only included primary THAs. As such, all immediate THAs after fracture, hemiarthroplasties and resurfacings, or conversions from a previous resurfacing were excluded. Institutional review board approval was obtained before initiation of the study.
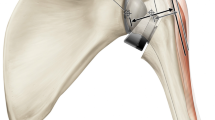
Radiographic analysis included inclination and anteversion of the acetabular component based on a pelvic AP radiograph (Fig. 1) on the most recent radiographs before dislocation as described earlier [2, 29]. This method was selected given it is the most clinically applicable method in contemporary practice used by surgeons on a day-to-day basis. In the current study the term “combined safe zone” describes the fact that both acetabular safe zones, anteversion and inclination, were reached. Additional radiographic analysis included femoral offset, acetabular offset, horizontal and vertical change of the center of rotation, and limb length discrepancy as previously described (Fig. 2) [27, 28]. All radiographs were reviewed by two of the authors (PvR, MTJ) and was completed twice by each of the reviewers at least 2 weeks apart. For all radiographic parameters, the mean correlation coefficient of the interobserver reliability was 0.89 (range, 0.84–0.94), and the mean correlation coefficient of the intraobserver reliability was 0.89 (range, 0.75–0.97). Eighty-five percent of patients had complete preoperative and postoperative radiographs for analysis (ie, AP pelvis, AP hip, and crosstable lateral). The remaining 15% had preoperative and postoperative radiographs available for review, but not the complete complement.

AP radiograph depicting the method used to measure anteversion (AV) as previously described [2]. The long (A to B, AB) and short (C to D, CD) axes of the ellipse of the acetabular component are drawn, which intersect each other at a right angle. The angle of anteversion is calculated through the formula AV = sin−1 (CD/AB). The inclination is the angle between the teardrop line and the long axis of the ellipse.

AP radiograph showing the measured parameters (femoral offset, blue lines; former center of rotation, green lines; leg length, yellow lines). The red line depicts the teardrop line as a baseline for all measurements.
The study cohort consisted of 206 hips in 206 patients. Demographic analysis included the mean age at the time of primary THA, the distribution of sex, time to dislocation, mean body mass index, and mean followup (Table 1). Diagnoses included degenerative joint disease, posttraumatic arthritis, avascular necrosis, inflammatory arthritis, and neuropathic arthritis (Table 1). During the study period, 9784 primary THAs were completed at our institution with 5765 having a posterior approach, 3384 having an anterolateral approach, and 71 having an extended trochanteric osteotomy. The approach used depended on surgeon preference. A repair of the capsule was performed in all cases with a posterior approach.
A total of eight acetabular component designs were used in this series, but all had uncemented fixation. Similarly, 16 femoral component designs were used with 152 of 206 stems (74%) being inserted in an uncemented fashion.
Statistical Methods
Data are presented as mean values with ranges or 95% confidence interval (CI). Log-rank test was applied to test for significant differences [18]. Differences in the survival of subgroups were tested with the log-rank test [18]. Statistical analysis was performed with use of SPSS software (IBM, Armonk, NY, USA).
Results
Proportion of Cups in the Safe Zone
The mean cup inclination was 44° ± 8° (95% CI, 42°–45°) and anteversion was 15° ± 9° (95% CI, 13°–16°). The cup inclination was within the safe zone in 84% (174 of 206) of hips. The anteversion was within the safe zone in 69% (143 of 206) of hips. In 58% (120 of 206) of hips, both safe zones were achieved (Fig. 3). The mean femoral offset was 38 ± 7 mm (95% CI, 37–39 mm). The mean acetabular offset was 32 ± 4 mm (95% CI, 31–33 mm). The mean lateralization of the center of rotation was +6 ± 4 mm (95% CI, +5–+6 mm) from the native center of rotation, and the mean limb length difference was 4 ± 7 mm (95% CI, 3–5 mm) longer.

Diagram depicting number of patients who dislocated that were within the Lewinnek safe zones.
Relationship Between Surgical Approach and Safe Zone
When analyzing based on approach, cup inclination was within the safe zone in 92% (190 of 206) of cases for the posterior approach and 62% of cases for the anterolateral approach. Similarly, anteversion was within the safe zone in 73% of cases after a posterior approach and 49% of cases with an anterolateral approach. As such, the combined safe zone was achieved in 65% of cases with the posterior approach (Fig. 4) and 33% of cases with the anterolateral approach (Fig. 5). An acetabular component performed through a posterior approach was three times as likely to be within the combined safe zone (odds ratio [OR], 1.3; 95% CI, 1.1–1.6) than after an anterolateral approach (OR, 0.4; 95% CI, 0.2–0.7; p < 0.0001). In contrast, acetabular components performed through a posterior approach (OR, 1.6; 95% CI, 1.2–1.9) had an increased risk of dislocation compared with those performed through an anterolateral approach (OR, 0.8; 95% CI, 0.7–0.9; p < 0.0001).

Diagram depicting the number of patients with a posterior approach who dislocated and were within the Lewinnek safe zones.

Diagram depicting the number of patients with an anterolateral approach who dislocated and were within the Lewinnek safe zones.
Discussion
Instability is one of the most common complications after primary THA, occurring in 0.3% to 10% of cases [9, 25]. Prior studies distinguish between patient-related factors such as abductor weakness or neurologic deficits and technique-related risk factors [9, 32, 39]. Technical factors under the surgeon’s direction include approach, soft tissue management, implant design choice, and component position [9]. In 1978, Lewinnek et al. [20] defined their safe zone for the acetabular component to avoid dislocation. Although the concept of a safe zone is widely accepted and used in clinical practice, dislocations still occur. As such, the primary goal of this study was to determine if the radiographic target values for cup inclination and anteversion proposed by Lewinnek et al. accurately predict dislocation in a contemporary THA practice.
There are numerous limitations to the current study. First, the study was based on AP radiographs: femoral version, and thus combined femoral and acetabular anteversion, was not evaluated. In the future, more advanced analyses (eg, cross-sectional and dynamic imaging) will be required. However, the focus of this investigation was on the concept of an acetabular safe zone with the information the practicing clinician typically has available. In addition, all procedures were completed at a high-volume tertiary care institution. As such, the findings may not be widely expandable. Third, multiple surgeons and implants were involved. Although some may see this is a drawback, it actually represents a contemporary cohort of patients with multiple femoral head size options and multiple liner options available.
Although the vast majority of our cups were within the safe zone for both inclination and anteversion, dislocations still occurred. Reize et al. [36] similarly found that 58% of their cups were within both safe zones (ie, cup inclination and anteversion) for those who dislocated. However, they did not report on the proportion of patients who dislocated. Esposito et al. [13] also noted that 57% of their cups were within both safe zones for those who dislocated. The mean cup inclination (44°) and anteversion (15°) of dislocated hips reported in the current study reflect the standard values noted for the native hip [35]. In addition, the mean values of both inclination and anteversion were nearly identical to the recommended targets by Lewinnek et al. [20].
In the current study, there was an increased risk of dislocation with the posterior approach although acetabular components positioned through this approach were nearly twice as likely to be within the proposed combined safe zone of anteversion and inclination. However, this difference was smaller than prior reports [5]. This reinforces the fact that for the posterior approach, the safe zone is not an accurate predictor of dislocation. More importantly, it highlights that for the posterior approach, there is no “sweet spot” and thus no benefit in reorienting the safe zone. There continues to be debate surrounding the risk of dislocation based on approach [9, 14]. Masonis and Bourne [24] reported that 1% and 3% of THAs dislocated after use of the transtrochanteric and posterior approaches, respectively. However, that was reduced to 2% with a posterior capsular repair [24]. Similarly, other studies have shown that a capsular repair and an increased femoral head diameter after the posterior approach decrease the likelihood of dislocation [5, 32]. Conversely, an analysis of the dislocations in the anterolateral group reveals that accepting less acetabular anteversion through this approach also is not protective against dislocation. As exemplified in graphic format (Fig. 5), those with less anteversion had more dislocations. Although reorienting the safe zone may have no clinical benefit for the posterior approach, it may have a role in the anterolateral approach. However, this requires further investigation.
In our series of THAs implanted by high-volume surgeons, we found that 2% dislocated when followed for a mean of > 2 years. Recently, Esposito et al. [13] described their frequency of dislocation to be 2% as well. However, their study period was only the first 6 months from the surgical intervention. This is important because the frequency of dislocation varies based on length of followup [4, 10]. In addition, Esposito et al. [13] identified dislocations through patient self-reporting and mailed surveys as opposed to confirmation through clinical followup. Finally, the posterior approach was used in 98% of their patients, limiting analysis with other approaches such as anterolateral.
Because restoration of the native anatomy also plays a crucial role in preventing instability after THA [21, 31], we sought to assess femoral offset, acetabular offset, combined lateralization, and limb length discrepancy. The femoral offset in the current study was 38 mm. According to Preininger et al. [35], the offset of the native hip ranges from 39 to 43 mm. Therefore, the offset in our study cohort was reconstructed accurately. Next, acetabular offset was evaluated and found to be 32 mm. Kurtz et al. [19] reported on the acetabular offset before (40 mm) and after THA (33 mm) and found comparable values. Moreover, the measured limb length difference in our study was < 5 mm. Discrepancies within 1 cm are well tolerated by patients [23, 38]. Finally, the center of rotation was lateralized by 6 mm. Baghdadi et al. [3] used the same technique to assess the change of the center of rotation and found a mean of 11 mm.
We found that the historical target values for cup inclination and anteversion defined by Lewinnek et al. may be useful but should not be considered a safe zone, in the sense that positioning the acetabular component within these parameters does not preclude dislocation. The majority of our THAs that dislocated were, in fact, within those target values. Although multiple authors proposed to keep the safe zones described by Lewinnek [33, 37], Esposito et al. [13] found no distinct safe zone. It is likely that the ideal cup position for some patients lies outside the Lewinnek zone and that more-advanced analysis is required to identify the right target in that subgroup. Creating a stable THA remains a balancing act among appropriate component positioning taking into account individual patient bony and muscular anatomy in both the static and dynamic state, soft tissue balance and tensioning, and appropriate aftercare and rehabilitative efforts.
References
Amlie E, Hovik O, Reikeras O. Dislocation after total hip arthroplasty with 28 and 32-mm femoral head. J Orthop Traumatol. 2010;11:111–115.
Bachhal V, Jindal N, Saini G, Sament R, Kumar V, Chouhan D, Dhillon M. A new method of measuring acetabular cup anteversion on simulated radiographs. Int Orthop. 2012;36:1813–1818.
Baghdadi YM, Larson AN, Sierra RJ. Restoration of the hip center during THA performed for protrusio acetabuli is associated with better implant survival. Clin Orthop Relat Res. 2013;471:3251–3259.
Berry DJ. Unstable total hip arthroplasty: detailed overview. Instr Course Lect. 2001;50:265–274.
Berry DJ, von Knoch M, Schleck CD, Harmsen WS. Effect of femoral head diameter and operative approach on risk of dislocation after primary total hip arthroplasty. J Bone Joint Surg Am. 2005;87:2456–2463.
Biedermann R, Tonin A, Krismer M, Rachbauer F, Eibl G, Stockl B. Reducing the risk of dislocation after total hip arthroplasty: the effect of orientation of the acetabular component. Bone Joint J. 2005;87:762–769.
Bolland BJ, Whitehouse SL, Timperley AJ. Indications for early hip revision surgery in the UK–a re-analysis of NJR data. Hip Int.. 2012;22:145–152.
Bozic KJ, Ong K, Lau E, Kurtz SM, Vail TP, Rubash HE, Berry DJ. Risk of complication and revision total hip arthroplasty among Medicare patients with different bearing surfaces. Clin Orthop Relat Res. 2010;468:2357–2362.
Brooks PJ. Dislocation following total hip replacement: causes and cures. Bone Joint J. 2013;95:67–69.
D’Angelo F, Murena L, Zatti G, Cherubino P. The unstable total hip replacement. Indian J Orthop. 2008;42:252–259.
Daly PJ, Morrey BF. Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am. 1992;74:1334–1343.
Delaunay C, Hamadouche M, Girard J, Duhamel A. What are the causes for failures of primary hip arthroplasties in France? Clin Orthop Relat Res. 2013;471:3863–3869.
Esposito CI, Gladnick BP, Lee YY, Lyman S, Wright TM, Mayman DJ, Padgett DE. Cup position alone does not predict risk of dislocation after hip arthroplasty. J Arthroplasty. 2015;30:109–113.
Hailer NP, Weiss RJ, Stark A, Karrholm J. The risk of revision due to dislocation after total hip arthroplasty depends on surgical approach, femoral head size, sex, and primary diagnosis. An analysis of 78,098 operations in the Swedish Hip Arthroplasty Register. Acta Orthop. 2012;83:442–448.
Harrison CL, Thomson AI, Cutts S, Rowe PJ, Riches PE. Research synthesis of recommended acetabular cup orientations for total hip arthroplasty. J Arthroplasty. 2014;29:377-382.
Higgins BT, Barlow DR, Heagerty NE, Lin TJ. Anterior vs. posterior approach for total hip arthroplasty, a systematic review and meta-analysis. J Arthroplasty. 2015;30:419–434.
Howie DW, Holubowycz OT, Middleton R. Large femoral heads decrease the incidence of dislocation after total hip arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2012;94:1095–1102.
Kaplan E, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–481.
Kurtz WB, Ecker TM, Reichmann WM, Murphy SB. Factors affecting bony impingement in hip arthroplasty. J Arthroplasty. 2010;25:624–634.e621–622.
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60:217–220.
Liebs TR, Nasser L, Herzberg W, Ruther W, Hassenpflug J. The influence of femoral offset on health-related quality of life after total hip replacement. Bone Joint J. 2014;96:36–42.
Mahoney CR, Pellicci PM. Complications in primary total hip arthroplasty: avoidance and management of dislocations. Instr Course Lect. 2003;52:247–255.
Maloney WJ, Keeney JA. Leg length discrepancy after total hip arthroplasty. J Arthroplasty. 2004;19:108–110.
Masonis JL, Bourne RB. Surgical approach, abductor function, and total hip arthroplasty dislocation. Clin Orthop Relat Res. 2002;405:46–53.
Melvin JS, Karthikeyan T, Cope R, Fehring TK. Early failures in total hip arthroplasty–a changing paradigm. J Arthroplasty. 2014;29:1285–1288.
Morrey BF. Instability after total hip arthroplasty. Orthop Clin North Am. 1992;23:237–248.
Mulcahy H, Chew FS. Current concepts of hip arthroplasty for radiologists: part 1, features and radiographic assessment. AJR Am J Roentgenol. 2012;199:559–569.
Mulcahy H, Chew FS. Current concepts of hip arthroplasty for radiologists: part 2, revisions and complications. AJR Am J Roentgenol. 2012;199:570–580.
Murray DW. The definition and measurement of acetabular orientation. Bone Joint J. 1993;75:228–232.
Padgett DE, Warashina H. The unstable total hip replacement. Clin Orthop Relat Res. 2004;420:72–79.
Patel AB, Wagle RR, Usrey MM, Thompson MT, Incavo SJ, Noble PC. Guidelines for implant placement to minimize impingement during activities of daily living after total hip arthroplasty. J Arthroplasty. 2010;25:1275–1281 e1271.
Patel PD, Potts A, Froimson MI. The dislocating hip arthroplasty: prevention and treatment. J Arthroplasty. 2007;22:86–90.
Paterno SA, Lachiewicz PF, Kelley SS. The influence of patient-related factors and the position of the acetabular component on the rate of dislocation after total hip replacement. J Bone Joint Surg Am. 1997;79:1202–1210.
Peter R, Lubbeke A, Stern R, Hoffmeyer P. Cup size and risk of dislocation after primary total hip arthroplasty. J Arthroplasty. 2011;26:1305–1309.
Preininger B, Schmorl K, von Roth P, Winkler T, Matziolis G, Perka C, Tohtz S. Femoral offset (3D) in patients without osteoarthritis–index values from 200 hip joints. Open Orthop J. 2012;6:578–581.
Reize P, Geiger EV, Suckel A, Rudert M, Wulker N. Influence of surgical experience on accuracy of acetabular cup positioning in total hip arthroplasty. Am J Orthop (Belle Mead NJ). 2008;37:360–363.
Robinson M, Bornstein L, Mennear B, Bostrom M, Nestor B, Padgett D, Westrich G. Effect of restoration of combined offset on stability of large head THA. Hip Int. 2012;22:248–253.
Sobiech M, Jablonski M, Gorzelak M, Turzanska K, Posturzynska A, Drelich M. Postoperative limb lengthening following total hip arthroplasty (THA) through a posterior approach–a challenge for the orthopaedist or physiotherapist? Ortop Traumatol Rehabil. 2010;12:420–429.
Wetters NG, Murray TG, Moric M, Sporer SM, Paprosky WG, Della Valle CJ. Risk factors for dislocation after revision total hip arthroplasty. Clin Orthop Relat Res. 2013;471:410–416.
Author information
Authors and Affiliations
Corresponding author
Additional information
One or more of the authors (ADH, MWP) has received personal fees from Stryker (Mahwah, NJ) outside the submitted work. One of the authors (MWP) has received personal fees from DePuy (Warsaw, IN, USA) outside the submitted work.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at the Mayo Clinic, Rochester, MN, USA.
About this article

Cite this article
Abdel, M.P., von Roth, P., Jennings, M.T. et al. What Safe Zone? The Vast Majority of Dislocated THAs Are Within the Lewinnek Safe Zone for Acetabular Component Position. Clin Orthop Relat Res 474, 386–391 (2016). https://doi.org/10.1007/s11999-015-4432-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-015-4432-5