
Abstract
Invasive mycoses are a rising problem, not only in traditional categories of patients like hematologic or neutropenic ones, but also in elderly non-neutropenic patients admitted to internal medicine wards. Patients being admitted to medical wards are usually older, have multiple comorbidities, e.g., liver cirrhosis or chronic obstructive respiratory disease, may be malnourished or receive peripheral or total parenteral nutrition, and frequently are undergoing chronic corticosteroid therapy, chemotherapy for cancer or monoclonal antibodies for autoimmune diseases. Such risk factors may be contemporarily present in a single patient increasing the risk for the development of invasive mycoses. Diagnosis of candidemia and invasive aspergillosis is particularly difficult in patients hospitalized on medical wards, since symptoms and signs have low specificity, and most diagnostic tests have been only validated in neutropenic hematologic patients, but not in those without neutropenia. Both candidemia and invasive aspergillosis carry significant morbidity and mortality. The aim of this paper is to provide a simple guide to physicians for a prompt identification and treatment of patients with possible or suspected invasive mycoses.
Similar content being viewed by others


Introduction
Since the early 1980s, fungi have emerged as major causes of human disease [1, 2]. The most important factor that has contributed to the increase in fungal infections is the expansion of the population of immunocompromised patients, due to mucosal or cutaneous barrier disruption, defects in the number and function of neutrophils or in cell-mediated immunity, metabolic dysfunction, and extremes of age. Increasing use of broad-spectrum antibiotics, cytotoxic chemotherapies, and transplantation further increase the risk for both common and uncommon opportunistic fungi.
Invasive candidiasis (IC) and invasive aspergillosis (IA) are the two most common forms of invasive fungal infections. These two clinical syndromes have been traditionally encountered in neutropenic patients with hematologic malignancies or in critically ill patients hospitalized on intensive care units (ICU). However, during the last decade an increasing number of invasive fungal infections have been diagnosed in patients admitted to medical wards, such as elderly patients, patients undergoing chronic corticosteroid therapy, patients with liver cirrhosis or chronic obstructive respiratory disease (COPD), patients malnourished and receiving total parenteral nutrition (TNP), patients receiving chemotherapy for cancer or monoclonal antibodies for autoimmune diseases. Since most of these patients are commonly admitted to internal medicine wards, physicians should be aware of the potential risk of invasive mycoses in patients coming from the community, and presenting with signs and symptoms of infection. The aim of this review is to provide a practical guide for rapid identification and appropriate management of patients admitted to medical wards with possible or suspected invasive mycoses.
Invasive candidiasis
Epidemiologic studies from the last two decades have identified Candida species as the fourth most common cause of nosocomial bloodstream infection (BSI), and the leading cause of invasive fungal infections (IFIs) among hospitalized patients [1, 2]. Despite advances in antifungal therapy, Candidemia and other forms of invasive candidiasis (IC) continue to contribute to an excessive morbidity, greater mortality, prolonged hospitalizations, and increased costs of care [3, 4].
Candidemia is a rising problem due to the changing patterns of patients admitted to the hospital. An increasing number of elderly, critically ill patients with risk factors for invasive candidiasis are nowadays admitted to internal medicine wards (IMWs). As shown in Fig. 1, patients admitted to IMWs have high complexity, are usually older, with multiple comorbidities, various forms of immunosuppression, and frequently carry multiple risk factors for IC. Particular attention has recently been directed at the concept of the ‘‘frail elderly patient’’ [5–7]. Although frailty has been considered synonymous with disability, comorbidity or advanced old age, it is recently recognized as a biological syndrome of decreased reserve and resistance to stressors resulting from a cumulative decline across multiple physiological systems, causing increased vulnerability to an adverse outcome [8]. The immune system alterations observed in frailty include heightened inflammation and alterations in the innate and adaptive immune systems, and are likely responsible for the overall immune functional decline and increased susceptibility to fungal infections in the frail elderly population [9]. Frail patients are typically hospitalized in IMWs.

Clinical features of patients residing in internal medicine wards
Several risk factors for IC have been identified in frail elderly patients (Table 1). The elevated serum glucose levels associated with type 2 diabetes (T2DM) alter host immune responses, predisposing to various infectious processes [10], including IC. Invasive procedures, like urinary catheters, indwelling central venous catheter (CVC), and both peripheral parenteral nutrition (PPN) and total parenteral nutrition (TPN) [11] are significantly associated with IC [12]. Catheters, like other medical devices, can serve as a substrate for Candida biofilm infection, which exhibits a drug-resistant phenotype, necessitating biofilm extirpation for treatment success [3]. The risk of IC is particularly high in patients with cancer and long-term CVC (e.g. port-a-cath) receiving intravenous chemotherapy [13–15]. Of importance, the presence of thrombi in patients with CVC or peripherally inserted central catheter may be a dramatic complication in patients with infection on a device due to Candida. Other risk factors for IC include chronic renal failure, renal transplantation, receipt of immunosuppressive treatment for systemic connective tissue diseases (such as systemic lupus erythematosus, systemic sclerosis, rheumatoid arthritis and polymyositis/dermatomyositis), and treatment with glucocorticoids or multiple antibiotics. All these factors contribute to the dysfunction of immune response and T-, B- and dendritic cells, making them more susceptible to the occurrence of IFIs [16]. Tumor necrosis factor α (TNF-α) antagonists, often used in the treatment of inflammatory rheumatic and autoimmune diseases, have also been associated with IC [17].
On the basis of all the aforementioned, physicians working in IMWs should be aware of the risk for their patients to develop an invasive Candida infection [18]. This assumption is reinforced by the fact that recent studies have shown that more than one-third of all collected candidemia episodes occur in IMWs. Patients with candidemia residing in IMWs usually have a higher mean age (73.2) than hematologic (66.4) or ICU patients (57.2), a prevalence of non-albicans Candida spp. (52.6 %), a high frequency of solid tumors (51.8 %) and CVC in place (81 %), and the highest 30-day crude mortality rate (50.4 %) [19]. The most common non-albicans species are C. parapsilosis and C. glabrata, followed by C. tropicalis and C. Krusei. Another study conducted in a teaching hospital on 145 cases of candidemia occurring during the period January 2008–June 2011 finds that the majority of episodes of candidemia are diagnosed on IMWs (66.4 % of all cases). The duration of PPN and TPN of more than 4 days is found to be the strongest risk factor for candidemia in elderly patients, while additional risk factors are receipt of combinations of antibiotics and CVC [7]. Elderly patients receiving multiple courses of antibiotic therapy may develop C. difficile infection, and prior C. difficile diarrhea has recently been associated with subsequent candidemia in patients hospitalized in IMWs [20].
For these reasons, all clinicians should include candidemia as a possible cause of persistent fever and clinical worsening in hospitalized internal medical patients identifying those who have potential risk factors and predisposing underlying diseases (i.e. solid neoplasia, T2DM, renal insufficiency, steroid or other immunosuppressive therapy). Only the increased awareness of possible candidemia will prompt an immediate diagnostic effort and delivery of antifungal treatment. A practical algorithm for early identification of patients at risk for IC in IMWs is described in Fig. 2.

Proposed clinical approach to patients residing in IMWs with risk factors for candidemia. Signs and symptoms of candidemia may be absent or non-specific in elderly patients residing in internal medicine wards. Studies conducted in this setting have shown multiple factors associated with risk of developing candidemia, including peripheral parenteral nutrition, central venous catheter, broad-spectrum antibiotics and others. The contemporary presence of multiple risk factors as suggested in this figure plus the evidence of Candida spp. colonization, positive (1-3)-Β-d-glucan and low procalcitonin levels should lead clinicians to high clinical suspicion of candidemia. Start of antifungal therapy appears justified in these cases. This algorithm is proposed by the authors as a simple tool for a rapid identification of patients at risk of candidemia in IMWs. Further prospective studies enrolling large number of patients are needed to confirm this approach. IMWs internal medicine wards
The clinical presentation of candidemia may span from the absence of specific symptoms to severe sepsis or septic shock. The early clinical manifestations of sepsis are non-specific, and no clinical sign or symptom has sufficient specificity to be highlighted with the exception of a positive funduscopic examination. Candida endophthalmitis occurs at an incidence of 3.7–25 % in prospective series, and often is a complication unrecognized by clinicians [21]. Funduscopic examination is mandatory in all patients with documented candidemia. Blood cultures (BC) are currently considered the “gold standard” for IC diagnosis, particularly when coupled with clinical symptoms [22]. The number of BC recommended in a single session is 3 (2–4), with a total volume of 40–60 mL for adults. The timing for obtaining the BC is one right after the other from different sites, and venipuncture remains the technique of choice. A BC set comprises 60 mL blood for adults obtained in a single session within a 30-min period and divided in 10-mL aliquots among three aerobic and three anaerobic bottles. When candidemia is suspected the frequency of sampling recommended is daily, and the incubation period must be at least 5-day long. The sensitivity of BC to detect Candida is 50–75 %, although lower sensitivity rates in neutropenic patients and those undergoing antifungal treatment have been reported. So, the performance of BC is not very high, and it is positive only in about the half of the cases of candidemia [23]. In addition, 24–72 h are required for species identification and susceptibility testing, and a recent study finds that there are differences in time to positivity among different Candida species: significantly longer for C. glabrata and shorter for C. tropicalis, when compared with other species [24].
Alternative procedures based on the detection and quantification of fungal biomarkers and metabolites have been developed to improve and anticipate the detection of candidemia. The (1,3)-β-d-glucan detection (BDG) is a technique useful for Candida detection, but is not specific for Candida because it is a non-invasive testing to detect circulating fungal cell wall components [25]. BDG is a polysaccharide located in the cell membrane of most fungal pathogens, including Aspergillus and Candida species. Notable exceptions are Mucor species and Cryptococcus species, which either do not express β-glucan or exhibit only low-level or variable expression. Detection of BDG in blood or other bodily specimens represents a reasonable panfungal marker for IFI, and is included in the EORTC/MSG (European Organization for Research and Treatment of Cancer/Mycosis Study Group) diagnostic criteria for invasive fungal infections in 2008, for all types of patients (any kind of patient). Fungitell Assay (Associates of Cape Cod, Inc., East Falmouth, MA) is commercially available in Europe and can detect β-glucan in serum within 2 h. BDG can be used in monitoring at-risk patients; serial determination (twice a week) are recommended [17]. With a positive cutoff of ≥80 pg/ml, the sensitivity and specificity of the test are respectively 77 and 86 %, with a negative predictive value of 97 % [26, 27]. The main problems of the routine use of BDG are its high cost (~35 euros/sample) and high rate of false-positive results in the presence of hemodialysis, other fungal or bacterial infection, wound gauze, albumin or immunoglobulin infusion. Nonetheless, after weighing the pros and cons, numerous authors support more routine use of β-glucan testing at this time [28].
Another biomarker of Candida infection is mannan, a polysaccharide and polymer of the sugar mannose that is a highly immunogenic component of the Candida cell wall [29, 30]. Both mannan antigens and antibodies can increase in serum from patients with Candida infection. The Platelia Candida antigen and antibody tests are commercially available tools for the detection of serum levels of mannan antigen and antimannan antibodies, respectively [Platelia Candida Antigen Plus (Ag PlusTM) and Antibody Plus (Ab PlusTM; Bio-Rad Laboratories)]. Combined mannan/anti-mannan sensitivity and specificity for invasive candidiasis diagnosis are 83 and 86 %, respectively. Higher sensitivity (100 %) and somewhat lower specificity (74 %) for candidemia are reported when employing combined mannan antigen and antimannan antibody detection with lower cutoffs than those suggested by the manufacturer of the Platelia assays [31]. These assays can help to detect the infection early because they can be positive 6 days on average prior blood cultures. It shows also very high negative predictive value (>85 %) and can be used to rule out infection. The main problem of this test is reduced sensitivity in C. parapsilosis and C. krusei infections [32]. Rapid PCR- and microarray-based assays for a rapid identification of clinically relevant yeasts in blood culture have been proposed [33]. Compared to blood cultures, the performance of methods such Prove-it Sepsis platform is found to be highly accurate when analyzing primary isolates, demonstrating a sensitivity of 99 % and a specificity of 98 % for fungal targets. These results suggest that molecular methods may be incorporated into the tools for clinical patient management, and would allow possibly faster identification and more focused therapies in patients with bloodstream infections. However, further confirmation studies are needed, and due to the high costs, these techniques are not routinely used in the majority of laboratories in the world.
Systemic antifungal agents shown to be effective for the treatment of candidiasis are comprised in three major categories: the echinocandins (anidulafungin, caspofungin, and micafungin), the triazoles (fluconazole, itraconazole, voriconazole, and posaconazole) and lipidic formulations of amphotericin B (liposomal Amphotericin B and lipidic complex amphotericin B). Treatment guidelines [34] recommend an echinocandin as a first-line choice to treat IC. Recommendations included in the last ESCMID guidelines are summarized in Table 2. The recommendation for liposomal amphotericin B or voriconazole is less stringent, and fluconazole is recommended with marginal strength only, except for C. parapsilosis. The use of echinocandins appears mandatory in patients with severe or moderately severe clinical conditions (e.g., hemodynamically unstable or with suspected concomitant organ involvement), in those with prior triazole exposure, and in those infected with less susceptible Candida spp. such as C. glabrata and C. krusei.
Two recent retrospective analyses of data from large prospective trials favor echinocandins over fluconazole. In the first [35], the global response rate is higher for anidulafungin than for fluconazole (71 vs. 54 %, respectively), although the original study was designed to establish non-inferiority; there was also a trend for lower 14-day all-cause mortality, but this advantage was not present at 28 days. In the second [3], treatment with an echinocandin is associated with significantly reduced mortality (27 % for echinocandins vs 36 % for other regimens), compared with the use of a drug from either the triazole or polyene classes, and this superiority is evident for both C. albicans and non-albicans groups, and in patients with a wide range of severity of illness, with exception of those with the highest (>24) Acute Physiology and Chronic Health Evaluation II score. Moreover, in patients with systemic candidiasis caused by fluconazole-susceptible C. albicans anidulafungin is more effective than fluconazole in terms of better global response (OR 2.36; 95 % CI 1.06–5.25), faster clearance of Candida from the bloodstream (log-rank p < 0.05), and fewer persistent infections (2.7 vs. 13.1 %; p < 0.05) [36].
All three echinocandins are well tolerated and appear very safe. Both caspofungin and micafungin undergo minimal hepatic metabolism, whereas anidulafungin has no hepatic metabolism and undergoes intravascular chemical degradation [37]. The echinocandins are neither substrates nor modulators of the cytochrome P450 [38], thus ensuring minimal potential for drug–drug pharmacokinetic interactions during polytherapy. Caspofungin is an echinocandin in which dosage reduction is recommended for patients with moderate hepatic dysfunction (Child-Pugh score 7–9, class B). Anidulafungin is licensed to be used in patients with severe hepatic impairment (Child-Pugh score > 9, class C). Coadministering caspofungin with rifampin lowers caspofungin exposure, and it has been recommended to increase the dose of caspofungin in the rare cases, where both drugs need to be administered concomitantly [39]. Recent studies show that lower caspofungin area-under-the-concentration (AUC) time curves are achieved in obese persons than thinner ones [40]. This suggests that dose optimization in heavier patients is needed, and an increased caspofungin dosage (e.g. 70 mg/daily) may be considered. Further studies also suggest the potential for higher doses of micafungin in obese patients [41].
Triazoles are the only drugs with oral availability. Fluconazole is favored over the three available echinocandins only for treatment of candidemia due to C. parapsilosis on the basis of the decreased in vitro activity of echinocandins against C. parapsilosis [42] and reports of echinocandin resistance among selected isolates [43]. For uncomplicated candidemia, antifungal therapy should be continued for 14 days after the end of candidemia and resolution of symptoms attributable to invasive infection. To determine the end of candidemia, at least one blood culture per day should be taken until culture results come back negative. In patients who improve clinically and clear Candida from the bloodstream, treatment can probably be simplified by stepping down to oral fluconazole after 10 days of intravenous treatment. In patients with candidemia and a prosthetic intravascular device, a prolonged follow-up is recommended after resolution of candidemia due to the risk of late-onset infective endocarditis [44]; in these latter cases, transesophageal echocardiography is recommended in all cases. In disseminated infection, a prolonged treatment is necessary (more than 4 weeks and up to lifelong suppressive therapy).
There are reports of emerging resistance of Candida spp. to various antifungals including echinocandins. Most recent data of SENTRY Antimicrobial Surveillance Program find that Candida spp. resistance to the echinocandins is low (0.0–1.7 %); Candida albicans and Candida glabrata that were resistant to anidulafungin, caspofungin, or micafungin were shown to have fks mutations. Among echinocandin-resistant C. glabrata isolates from 2011, 38 % were fluconazole resistant. Voriconazole is active against all Candida spp. except C. glabrata (10.5 % non-susceptibility), whereas posaconazole shows decreased activity against C. albicans (4.4 %) and Candida krusei (15.2 %) [45]. Since use of echinocandins is increasing, a strict monitoring of susceptibility patterns to these drugs is mandatory, as well as a judicious and rationale use of these drugs to avoid selection of resistant mutants.
Invasive aspergillosis
Invasive pulmonary aspergillosis (IPA) is one of the major causes of morbidity and mortality in patients severely immunocompromised, especially among patients with prolonged neutropenia or undergoing hematopoietic stem cell transplantation [46]. More recently, several authors report the occurrence of IPA in liver cirrhosis, chronic obstructive pulmonary disease (COPD), and other clinical syndromes requiring steroid treatment, with a very high mortality rate [47–49].
An early diagnosis therefore seems crucial to improve prognosis in patients [50] presenting to the hospital with pneumonia, but simple isolation of Aspergillus spp. from respiratory specimens may be difficult or misleading since this organism may colonize the airways without generating an infection. Thus it is very important to recognize IPA, in particular in these new categories of patients at risk [51, 52]. To this end, unfortunately clinical and radiological signs are frequently lacking and usually not specific. In such a complex contest, definite diagnosis is rarely established before death or before overwhelming fungal proliferation.
The incidence of IPA is probably underestimated, owing to the poor sensitivity of clinical and radiological investigations and diagnostic tests. In addition, large surveillance programs mainly focus on hematology and oncology patients: IPA has been traditionally regarded as an infection mainly occurring in patients with well-established risk factors, such as neutropenia, hematologic malignancies, organ transplantation, or HIV1. However, an increasing number of reports underline the susceptibility of some categories of non-neutropenic patients to invasive fungal infections [53–56]. Recent studies underscore the increasingly important role that Aspergillus species plays in recipients of low doses of corticosteroids, patients with COPD, liver cirrhosis, transfusion-associated hemosiderosis, and diabetes mellitus [3–5]. The pathogenesis of IPA in non-neutropenic patients, e.g. those with steroid-associated immunosuppression, differs greatly from those being neutropenic. While angioinvasive lesions are often widespread, and death is related to a high fungal burden in neutropenic animals, the pathogenesis in non-neutropenic, steroid-treated animals is driven by an adverse inflammatory host response, with a low fungal burden in the lung parenchyma and less frequent dissemination of infection [57]. Low steroid doses (15 mg of prednisone per day or equivalent) are sufficient to develop IPA when the medication is administered continuously, as confirmed in a report by Rello et al. [58]. In these moderately immunosuppressed patients, Aspergillus colonization may contribute to the onset of IPA, particularly in patients with chronic pulmonary disease. Of interest, there is a report of a concomitant H1N1 infection suggesting that Influenza A virus may predispose the respiratory tract to IPA, particularly in patients affected by worsening COPD treated with chronic steroid therapy requiring hospitalization in intensive care units. This association may identify a particular high-risk patient population with poor prognosis even if rapidly and aggressively treated [59]. Thus, it is possible to speculate that such a remarkable immunologic impairment might contribute to triggering IPA in patients colonized with Aspergillus.
Meersseman et al. report the findings of a retrospective study of 69 cases of IPA in patients without malignancies who were hospitalized in a medical ICU with a mortality rate exceeding 50 % [60]. Maris et al. [61] conducted a retrospective study to examine the correlation between the clinical diagnosis and autopsy findings in adult patients who died in an intensive care unit (ICU). In their analysis infection due to Aspergillus spp. is the first cause of missed diagnosis that could change patient management and outcome, accounting for 33.3 % of the cases in this setting. Russo et al. [62] confirm IPA as a frequently undiagnosed complication of non-neutropenic patients; furthermore, it seems to extend this observation to non-ICU patients: as shown in Fig. 3 the 70 % of non-neutropenic patients with IPA were observed IMWs.

Distribution of cases of IPA in non-neutropenic patients in a teaching hospital [62]. ICU intensive care unit
During a 6-year study, first retrospectively and then prospectively, Cornillet et al. [63] show that the distribution of proven and probable invasive aspergillosis is similar for neutropenic and non-neutropenic patients, and the overall mortality rate is 71.5 %, being significantly higher in non-neutropenic patients than in neutropenic ones (89 vs. 60 %). Furthermore, compared to the latter, non-neutropenic patients are significantly less likely to have symptoms of invasive aspergillosis, and are more likely to be misdiagnosed as having a bacterial pneumonia. In the study of Cornillet, most patients were initially considered to have a bacterial pneumonia, with delay in diagnosis and treatment of IPA. Changes in antifungal treatment policies (deoxycholate amphotericin B during 1998–2001 and voriconazole during 2001–2003) did not affect the mortality rates by year during the study period. All these observations seem to suggest that unawareness of clinicians for the risk of IPA in non-neutropenic patients might have resulted in a delay of clinical diagnosis and treatment, leading to remarkably high mortality rates.
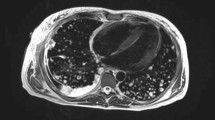
Cultures of Aspergillus species from respiratory secretions have a low diagnostic sensitivity and do not prove the presence of invasive infection. This was clearly demonstrated by Meersseman and coworkers, who find a positivity of bronchoalveolar lavage (BAL) culture of only 60 % in cases of histologically proven pulmonary aspergillosis [60]. In addition, unlike in neutropenic patients, as reported recently by Nucci et al. [64], and confirmed by other studies [36, 65], lung CT has limited value due to the absence of characteristic abnormalities, such as cavitation, air crescent sign, or halo sign. Moreover, Aspergillus infection may develop over preexisting atelectasis or in the acute respiratory distress syndrome [66]. The detection of galactomannan (GM) is a new valuable test for diagnosing IPA. GM is a polysaccharide fungal cell wall component that is released during tissue invasion by Aspergillus hyphae, which can be detected in body fluids. Data on the performance of GM detection in serum are sparse in non-neutropenic patients and suggest that serum GM is probably not a good marker for IPA in these patients [67]. As reported by Meersseman and colleagues, GM in the BAL fluid is very useful to diagnose probable or proven IPA with a sensitivity of 85–90 % using a cutoff index of 0.5, with a lower possibility of false positive in the BAL of patients treated with piperacillin/tazobactam [60]. All these data suggest that GM detection in the BAL fluid can be considered as a useful test in non-neutropenic patients with risk factor for IPA and evidence of pneumonia not responding to initial broad-spectrum antibiotic therapy. If bronchoscopy be contraindicated, GM detection in the sputum can be useful. A recent study shows the sputum to be equivalent to BAL fluid for GM detection, at least in patients with hematologic malignancies [68]. Russo et al. [62] seem to confirm the usefulness of GM detection in the sputum: all cases with a positive culture had a positive GM test. However, available data suggest using a higher cutoff (1–1.2 OD) for GM detection in sputum; 18 patients had a value >1 OD, which would be therefore considered positive. An additional factor that seemed to corroborate the diagnosis of IPA in most of patients, enrolled in this study, was prompt clinical improvement only after initiation of antifungal therapy, which progressed to cure even after antibiotic discontinuation. Report on combined use of GM in BAL and BDG on serum evidenced an improved sensitivity and specificity in diagnosis of invasive aspergillosis in the intensive care unit [69]. Figure 4 describes a proposal of clinical approach to patients admitted to IMWs with suspected invasive aspergillosis. Figure 5 summarizes the diagnostic work-up for patients with suspected invasive fungal infections.

Clinical management of patients residing in IMWs and risk factors for invasive pulmonary aspergillosis (IPA). GM galactomannan, BAL bronchoalveolar lavage, HRCT high-resolution computed tomography

Diagnostic flow chart for diagnosis of invasive fungal infections
As reported in Table 3, voriconazole is the drug of choice in the treatment of IPA and is proven to be effective in this type of patient [70]. The alternative options are represented by lipid formulations of AMB, which are less nephrotoxic than AMB deoxycholate, and more recent options represented by antifungal agents of the echinocandin class, including caspofungin, anidulafungin and micafungin: these agents are active in vitro against Aspergillus species. Anidulafungin achieves apparently adequate concentrations at least in alveolar macrophages [71], but clinical data on the use of echinocandins in cases of IPA are still limited.
In conclusion, IPA is a potentially fatal complication in non-neutropenic patients with specific risk factors. The studies reported in the literature, using recently recommended diagnostic criteria, seem to suggest an emerging role even in these patients who may have a higher mortality rate than their neutropenic peers, and provide preliminary evidence that early diagnosis and prompt initiation of antifungal therapy may improve the ultimate outcome of their IPA.
References
Becksague CM, Jarvis WR (1993) Secular trends in the epidemiology of nosocomial fungal-infections in the United States, 1980–1990. J Infect Dis 167:1247–1251
Edmond MB, Wallace SE, McClish DK et al (1999) Nosocomial bloodstream infections in United States hospitals: a three-year analysis. Clin Infect Dis 29:239–244
Andes DR, Safdar N, Baddley JW et al (2012) Impact of treatment strategy on outcomes in patients with candidemia and other forms of invasive candidiasis: a patient-level quantitative review of randomized trials. Clin Infect Dis 54:1110–1122
Mazzone A, Concia E, Falcone M, Pea F, Rossolini G (2012) Invasive fungal infections in the setting of internal medicine: an emergent challenge. Ital J Med 6(2 Suppl):19–35
Rockwood K, Hogan DB, MacKnight C (2000) Conceptualisation and measurement of frailty in elderly people. Drugs Aging 17:295–302
Gobbens RJ, Luijkx KG, Wijnen-Sponselee MT, Schols JM (2010) Towards an integral conceptual model of frailty. J Nutr Health Aging 14:175–181
Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G (2004) Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci 59:255–263
Falcone M, Blasi F, Menichetti F, Pea F, Violi F (2012) Pneumonia in older frail patients: an up to date. Intern Emerg Med 7:415–424
Gavazzi G, Krause KH (2002) Ageing and infection. Lancet Infect Dis 2:659–666
Rajagopalan S (2005) Serious infections in elderly patients with diabetes mellitus. Clin Infect Dis 40:990–996
Luzzati R, Cavinato S, Giangreco M et al (2013) Peripheral and total parenteral nutrition as the strongest risk factors for nosocomial Candidemia in elderly patients: a matched case–control study. Mycoses 56:664–671
Caccese R, Carfagna P, Pistilli N et al (2012) Candida thrombophlebitis of central veins: case report and review. Med Mycol 50:299–304
Falcone M, Accarpio F, Venditti M et al (2010) Septic bilateral pulmonary candidiasis successfully treated with anidulafungin therapy in two patients with peritoneal carcinomatosis. J Antimicrob Chemother 65:2266–2267
Falcone M, Russo A, De Rosa FG et al (2010) Clinical experience of anidulafungin for the treatment of patients with documented candidemia. J Chemother 22:397–401
Raad I, Hanna H, Boktour M et al (2004) Management of central venous catheters in patients with cancer and candidemia with cancer and candidemia. Clin Infect Dis 38:1119–1127
Alarcón GS (2006) Infections in systemic connective tissue diseases: systemic lupus erythematosus, scleroderma, and polymyositis/dermatomyositis. Infect Dis Clin North Am 20:849–875
Rychly DJ, Di Piro JT (2005) Infections associated with tumor necrosis factor-a antagonists. Pharmacotherapy 25:1181–1192
Cei M, Pardelli R, Sani S, Mumoli N (2014) Local resistance patterns to antimicrobials in internal medicine: a focused report from the REGIMEN (REGistro Infezioni in MEdicina INterna) study. Clin Exp Med 14:77–82
Bassetti M, Taramasso L, Nicco E et al (2011) Epidemiology, species distribution, antifungal susceptibility and outcome of nosocomial candidemia in a tertiary care hospital in Italy. PLoS One 6:e24198
Guastalegname M, Russo A, Falcone M, Giuliano S, Venditti M (2013) Candidemia subsequent to severe infection due to Clostridium difficile: is there a link? Clin Infect Dis 57:772–774
Donahue SP, Greven CM et al (1994) Intraocular candidiasis in patients with candidemia. Clinical implications derived from a prospective multicenter study. Ophthalmology 101:1302–1309
Cuenca-Estrella M, Verweij PE et al (2012) ESCMID* guideline for the diagnosis and management of Candida diseases 2012: diagnostic procedures. Clin Microbiol Infect 18(Suppl. 7):9–18
Horvath LL, Hospenthal DR, Murray CK, Dooley DP (2003) Detection of simulated candidemia by the BACTEC 9240 system with plus aerobic/F and anaerobic/F blood culture bottles. J Clin Microbiol 41:4714–4717
Lai CC, Wang CY, Liu WL, Huang YT, Hsueh PR (2012) Time to blood culture positivity of different Candida species causing fungemia. J Med Microbiol 61:701–704
Posteraro B, De Pascale M, Tumbarello M et al (2011) Early diagnosis of candidemia in intensive care unit patients with sepsis: a prospective comparison of (1®3)-b-d-glucan assay, Candida score, and colonization index. Crit Care 15:R249
Odabasi Z, Mattiuzzi G, Estey E et al (2004) β-d-glucan as a diagnostic adjunct for invasive fungal infections: validation, cutoff development, and performance in patients with acute myelogenous leukemia and myelodysplastic syndrome. Clin Infect Dis 39:199–205
Onishi A, Sugiyama D, Kogata Y, Saegusa J et al (2012) Diagnostic accuracy of serum 1,3-β-d-glucan for pneumocystis jiroveci pneumonia, invasive candidiasis, and invasive aspergillosis: systematic review and meta-analysis. J Clin Microbiol 50:7–15
Ostrosky-Zeichner L (2012) Invasive mycoses: diagnostic challenges. Am J Med 125(1A):S14–S24
Hsu JL, Ruoss SJ, Bower ND et al (2011) Diagnosing invasive fungal disease in critically ill patients. Crit Rev Microbiol 37:277–312
Mikulska M, Calandra T, Sanguinetti M, Poulain D, Viscoli C (2010) The use of mannan antigen and anti-mannan antibodies in the diagnosis of invasive candidiasis: recommendations from the Third European Conference on Infections in Leukemia. Crit Care 14: R222
Arendrup MC, Bergmann OJ, Larsson L et al (2010) Detection of candidaemia in patients with and without underlying haematological disease. Clin Microbiol Infect 16:855–862
Sendid B, Poirot JL, Tabouret M et al (2002) Combined detection of mannanaemia and antimannan antibodies as a strategy for the diagnosis of systemic infection caused by pathogenic Candida species. J Med Microbiol 51:433–442
Aittakorpi A, Kuusela P, Koukila-Kähkölä P et al (2012) Accurate and rapid identification of Candida spp. frequently associated with fungemia by using PCR and the microarray-based prove-it sepsis assay. J Clin Microbiol 50:3635–3640
Cornely OA, Bassetti M, Calandra T et al (2012) ESCMID* guideline for the diagnosis and management of Candida diseases 2012: non-neutropenic adult patients. Clin Microbiol Infect 18(Suppl. 7):19–37
Kett DH, Shorr AF, Reboli AC et al (2011) Anidulafungin compared with fluconazole in severely ill patients with candidemia and other forms of invasive candidiasis: support for the 2009 IDSA treatment guidelines for candidiasis. Crit Care 15:R253
Reboli AC, Shorr AF, Rotstein C et al (2011) Anidulafungin compared with fluconazole for treatment of candidemia and other forms of invasive candidiasis caused by Candida albicans: a multivariate analysis of factors associated with improved outcome. BMC Infect Dis 11:261
Vazquez JA, Sobel JD (2006) Anidulafungin: a novel echinocandin. Clin Infect Dis 43:215–222
Chandrasekar PH, Sobel JD (2006) Micafungin: a new echinocandin. Clin Infect Dis 42:1171–1178
Deresinski SC, Stevens DA (2003) Caspofungin. Clin Infect Dis 36:1445–1457
Hall RG, Swancutt MA, Meek C, Leff R, Gumbo T (2013) Weight drives caspofungin pharmacokinetic variability in overweight and obese people: fractal power signatures beyond two-thirds or three-fourths. Antimicrob Agents Chemother 57:2259–2264
Hall RG, Swancutt MA, Gumbo T (2011) Fractal geometry and the pharmacometrics of micafungin in overweight, obese, and extremely obese people. Antimicrob Agents Chemother 55:5107–5112
Bennett JE (2006) Echinocandins for candidemia in adults without neutropenia. N Engl J Med 355:1154–1159
Wiederhold NP, Lewis RE (2003) The echinocandin antifungals: an overview of the pharmacology, spectrum and clinical efficacy. Expert Opin Investig Drugs 12:1313–1333
Falcone M, Barzaghi N, Carosi G et al (2009) Italian study on endocarditis. Candida infective endocarditis: report of 15 cases from a prospective multicenter study. Medicine (Baltimore) 88:160–168
Pfaller MA, Messer SA, Woosley LN, Jones RN, Castanheira M (2013) Echinocandin and triazole antifungal susceptibility profiles for clinical opportunistic yeast and mold isolates collected from 2010 to 2011: application of new CLSI clinical breakpoints and epidemiological cutoff values for characterization of geographic and temporal trends of antifungal resistance. J Clin Microbiol 51:2571–2581
Segal BH, Walsh TJ (2006) Current approaches to diagnosis and treatment of invasive aspergillosis. Am J Respir Crit Care Med 173:707–717
Vandecasteele SJ, Meersseman W, Wilmer A et al (2004) Invasive aspergillosis in critically ill patients without malignancy. Am J Respir Crit Care Med 170:621–625
Ader F, Nseir S, Le Berre R et al (2005) Invasive pulmonary aspergillosis in chronic obstructive pulmonary disease: an emerging fungal pathogen. Clin Microbiol Infect 11:427–429
Falcone M, Massetti AP, Russo A, Vullo V, Venditti M (2011) Invasive aspergillosis in patients with liver disease. Med Mycol 49:406–413
Falcone M, Shindo Y, Venditti M, Kollef MH (2011) Healthcare-associated pneumonia: diagnostic criteria and distinction from community-acquired pneumonia. Int J Infect Dis 15:e545–e550
Bulpa P, Dive A, Sibille Y (2007) Invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary disease. Eur Respir J 30:782–800
De Pauw B, Walsh TJ, Donnelly JP et al (2008) Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 46:1813–1821
Cornet M, Mallat H, Somme D et al (2003) Fulminant invasive pulmonary aspergillosis in immunocompetent patients—a two-case report. Clin Microbiol Infect 9:1224–1227
Denning DW (2004) Aspergillosis in “nonimmunocompromised” critically ill patients. Am J Respir Crit Care Med 170:580–581
Petri MG, Konig J, Moecke HP et al (1997) Epidemiology of invasive mycosis in ICU patients: a prospective multicenter study in 435 non-neutropenic patients. Paul-Ehrlich Society for Chemotherapy, Divisions of Mycology and Pneumonia Research. Intens Care Med 23:317–325
Peter E, Bakri F, Ball DM, Cheney RT, Segal BH (2002) Invasive pulmonary filamentous fungal infection in a patient receiving inhaled corticosteroid therapy. Clin Infect Dis 35:e54–e56
Balloy V, Huerre M, Latge JP, Chignard M (2005) Differences in patterns of infection and inflammation for corticosteroid treatment and chemotherapy in experimental invasive pulmonary aspergillosis. Infect Immun 73:494–503
Rello J, Esandi ME, Mariscal D et al (1998) Invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary disease: report of eight cases and review. Clin Infect Dis 26:1473–1475
Carfagna P, Brandimarte F, Caccese R et al (2011) Fatal invasive pulmonary aspergillosis complicating influenza A (H1N1)v infection. Mycoses 54:549–551
Meersseman W, Lagrou K, Maertens J et al (2008) Galactomannan in bronchoalveolar lavage fluid: a tool for diagnosing aspergillosis in intensive care unit patients. Am J Respir Crit Care Med 177:27–34
Maris C, Martin B, Creteur J et al (2007) Comparison of clinical and post-mortem findings in intensive care unit patients. Virchows Arch 450:329–333
Russo A, Falcone M, Vena A et al (2011) Invasive pulmonary aspergillosis in non-neutropenic patients: analysis of a 14-month prospective clinical experience. J Chemother 23:290–294
Cornillet A, Camus C, Nimubona S et al (2006) Comparison of epidemiological, clinical, and biological features of invasive aspergillosis in neutropenic and non-neutropenic patients: a 6-year survey. Clin Infect Dis 43:577–584
Nucci M, Nouér SA, Grazziutti M et al (2010) Probable invasive probable invasive aspergillosis without prespecified radiologic findings: proposal for inclusion of a new category of aspergillosis and implications for studying novel therapies. Clin Infect Dis 51:1273–1280
Guinea J, Torres-Narbona M, Gijòn P et al (2010) Pulmonary aspergillosis in patients with chronic obstructive pulmonary disease: incidence, risk factors, and outcome. Clin Microbiol Infect 16:870–877
Meersseman W, Lagrou K, Maertens J, Van Wijngaerden E (2007) Invasive aspergillosis in the intensive care unit. Clin Infect Dis 45:205–216
Kwak EJ, Husain S, Obman A et al (2004) Efficacy of galactomannan antigen in the Platelia Aspergillus enzyme immunoassay for diagnosis of invasive aspergillosis in liver transplant recipients. J Clin Microbiol 42:435–438
Kimura SI, Odawara J, Aoki T et al (2009) Detection of sputum Aspergillus galactomannan for diagnosis of invasive pulmonary aspergillosis in haematological patients. Int J Hematol 90:463–470
Acosta J, Catalan M, del Palacio-Peréz-Medel A et al (2011) A prospective comparison of galactomannan in bronchoalveolar lavage fluid for the diagnosis of pulmonary invasive aspergillosis in medical patients under intensive care: comparison with the diagnostic performance of galactomannan and of (1 → 3)-β-d-glucan chromogenic assay in serum samples. Clin Microbiol Infect 17:1053–1060
Walsh TJ, Anaissie EJ, Denning DW et al (2008) Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis 46:327–360
Crandon JL, Banevicius MA, Fang AF et al (2009) Bronchopulmonary disposition of intravenous voriconazole and anidulafungin given in combination to healthy adults. Antimicrob Agents Chemother 53:5102–5107
Acknowledgments
The authors have served as members of an advisory board on infections in Internal Medicine funded by an unrestricted grant by Pfizer. Dr. A.M. ARUC provided assistance in the preparation of manuscript.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Falcone, M., Concia, E., Iori, I. et al. Identification and management of invasive mycoses in internal medicine: a road-map for physicians. Intern Emerg Med 9, 501–511 (2014). https://doi.org/10.1007/s11739-014-1077-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-014-1077-4