
Abstract
Youth violence disproportionately affects inner city, urban minority communities in the USA. This article illustrates the use of surveillance data to inform and evaluate community action directed at this serious problem. Community efforts in response to surveillance data indicating high rates of violence surrounding convenience stores with unrestricted alcohol beverage licenses provided a natural experiment to examine the impact of imposing licensing restrictions on intentional injury rates. Rates of ambulance pickups for intentional injuries in the 15- to 24-year-old population in five census tracts where alcoholic beverage sales were restricted were compared to five census tracts with similar demographic characteristics near stores where restrictions were not instituted. Time periods included an 18-month baseline period, a 6-month period during which restrictions were in effect in the intervention communities, and an 18-month period following lifting of this restriction resulting from legal action by store owners. The monthly average rate of ambulance pickups for violent injuries showed a significantly greater baseline-to-intervention phase decrease in the intervention communities (i.e., from 19.6 to 0 per 1,000) than in the control communities (i.e., 7.4 to 3.3 per 1,000). This rate subsequently increased to 11.4 in the intervention communities after the restriction was removed. This study illustrates the potential value of surveillance data for guiding community mobilization efforts and for evaluating the impact of such efforts. It also demonstrates the potential impact of restricting inexpensive, single-serve alcoholic beverages on rates of violence.
Similar content being viewed by others

Introduction
Intentional injury among youth is a serious public health problem. Homicide is the second leading cause of death among 15- to 24-year olds in the USA (Centers for Disease Control and Prevention 2010). Although mortality represents the most severe outcome of violence, non-fatal injuries are much more common and may have serious consequences. Disability, disruption of social services, health disparities, increased health care cost, and reduction in property values are all associated with violence (Mercy et al. 2002). The frequency of non-fatal injuries also predicts more severe forms of violence such as fatal injuries and disabilities. For each fatal injury, there are approximately 20 to 40 non-fatal violence victims who receive treatment in hospitals (Mercy et al. 2002). The repercussions of youth violence are far reaching and impact many facets of society. Its consequences include increased burden on health and welfare services, a loss of productivity, depreciation of property values, and neighborhood decay (Mercy et al. 2002). The impact of death, injury, and disability among youth affects not only the victims, but extends to their communities, families, and friends (Mercy et al. 2002; US Department of Health and Human Services 2001).
Public health providers and communities often rely on surveillance data to monitor fatal and non-fatal outcomes. Youth violence surveillance entails the analysis of primary and secondary datasets garnered from emergency rooms, hospital discharges, law enforcement, schools, juvenile justice systems, public health surveys, medical examiners, and vital statistics. Reports based on these data may be used to guide, implement, and monitor prevention efforts by community–university partnerships in areas where youth violence is pervasive. This article illustrates this process, based on a study that used local surveillance data to examine the impact of a community-based youth violence prevention effort that restricted the sale of inexpensive, single-serve alcohol beverages at convenience grocery stores.
The relation between alcohol outlet density and violence is well established in the literature. Numerous studies examining this spatial relation have reported significant associations between alcohol outlet density and violence (Alaniz et al. 1998; Branas et al. 2009; Britt et al. 2005; Escobedo and Ortiz 2002; Franklin et al. 2010; Gorman et al. 2001; Gruenewald et al. 2006; Nielsen and Martinez 2003; Reid et al. 2003; Scribner et al. 1995, 1999; Zhu et al. 2004). Researchers have also observed that alcohol outlets are often located within communities that are already at increased risk for violence and other health-related problems. These communities are generally located in inner-city areas with high rates of poverty where the majority of residents represent ethnic minorities (LaVeist and Wallace 2000; Pollack et al. 2005). These communities are often characterized by social disorganization such that crime and violence are highly prevalent and considered normative. This is supported by a recent study that reported a strong positive association between risk for violence and the number and density of alcohol outlets in areas where social disorganization exists (Gruenewald et al. 2006). Areas with high densities of alcohol outlets may also serve as an “attractor” to youth and uninhibited behavior, contributing to a variety of undesirable activities such as illegal drug sales, prostitution, and violence (Alaniz et al. 1998).
Alcohol outlets in urban areas that are licensed for off-premise sales (i.e., licensed to sell alcohol to be consumed outside of the store) represent a particular problem based on studies showing their relation to elevated rates of violence (Gruenewald et al. 2006; Lipton and Gruenewald 2002; Scribner et al. 1995, 1999). Although the same rationale regarding alcohol outlet density as a causal factor for violence can be applied to single-serve container sales, outlets that primarily sell single-serve containers may have a compounded impact on the prevalence of violence by increasing the affordability of alcoholic beverages (Parker et al. 2011). Although such a relation appears quite plausible, few studies have examined the impact of single-serve alcoholic beverages or malt liquor beverages on violence (Barajas et al. 2011; Chavira et al. 2011; Jones-Webb et al. 2008; Parker et al. 2011). These studies related to single-serve alcoholic beverages had focused on promotion and availability of these beverages as factors for racial disparities in homicide rates (Jones-Webb et al. 2008) and analyzing the consumption of such beverages as a predictor for exposure to violence (Chavira et al. 2011). Unlike the above studies, a more specific evaluation, conducted by Parker et al. (2011), reported a significant association between the availability of refrigerated shelf space dedicated to the sale of single-serve beverages and neighborhood-level violence. However, a recent quasi-experimental study examining the impact of malt liquor sale restrictions on crimes reported a mixed finding (Barajas et al. 2011). Although the study showed a reduction in disorderly conduct in the restricted sales areas, there was an increase in larceny, burglary, and aggravated assault.
Evidently, there is a scant and inconsistent body of scientific literature that has specifically examined the impact of single-serve alcohol sales or alcohol licensing restrictions on violence-related injuries. The limited number of studies addressing this issue may largely reflect the difficulty of assessing the impact of community-wide prevention efforts. The Centers for Disease Control, in its publication, Guide to Community Preventive Services (Campbell et al. 2009), identified a gap in the literature regarding how local decisions are made and emphasized the need to examine policies affecting alcohol outlet density. The Guide acknowledges that, although this type of study may be difficult to conduct, the results could provide a basis for guiding policy decisions concerning alcohol outlets.
The collection of local surveillance data on youth violence-related incidents has been a central focus of the Virginia Commonwealth University Clark-Hill Institute for Positive Youth Development. The Institute operates as a CDC-funded Academic Center of Excellence for the prevention of youth violence. Through its community surveillance system, the Institute has been continuously gathering and analyzing youth violence data from hospital emergency rooms, vital registry, ambulance pickups, schools, police, and juvenile justice systems since 2000. These data are routinely summarized and disseminated to guide prevention interventions and policy actions. In 2003, through the Institute's community outreach efforts, residents were made aware of the increased prevalence of violence surrounding convenience stores that sold inexpensive, single-serve alcoholic beverages. Alarmed by these data, residents held several community forums to discuss issues surrounding the problems associated with these “Mom and Pop” (i.e., nonchain, locally owned) convenience stores. Community members recognized that the availability of these beverages significantly contributed to undesirable activities such as violence, loitering, littering, and overall neighborhood decay. They collaborated with the local civic leagues to push for restrictions on any new Alcoholic Beverage Control (ABC) licenses and to prevent renewal of existing licenses that allowed convenience grocery stores in their communities to sell these beverages. More specifically, they requested that the Virginia ABC board issue restricted licenses to allow only the sale of 6 packs, 12 packs, or cases of beer and not the inexpensive and popular 40- or 22-oz bottles. Although these community efforts were maintained for 6 months, enforcement subsequently declined in response to strong opposition to these restrictions by some convenience grocery store owners and their legal counsel.
This rather unique situation provided a natural experiment to examine the impact of restricting licenses for alcohol beverage sales on intentional injury-related ambulance pickups. It also provides an illustration of methods used to translate surveillance data into community action.
Methods
An ecological panel study was used to examine the impact of restricted licenses for alcohol beverage sales on intentional injury-related ambulance pickups. Rates of ambulance pickups for violent intentional injuries in census tracts where convenience grocery stores were restricted from selling inexpensive, single-serve alcoholic beverages were compared to rates in control census tracts across three phases. The baseline phase represented the 18-month period prior to imposing restrictions in the intervention community. The intervention phase represented the 6 months during which the restriction was in effect. The reversal phase represented the 18 months following removal of the restriction.
Setting and Design
This study was conducted in Richmond, Virginia. Approximately 52 % of the city's overall population was African American, and 60 % of youth aged 10–24 were African American (US Census Bureau 2009). The 2008 homicide rate in Richmond was 15.5 homicides per 100,000, nearly three times the national average of 5.4 per 100,000 (US Department of Justice and Federal Bureau of Investigation 2009). The majority of homicides were among youth 15 to 24 years of age. The city harbors a disproportionately high density of public housings and convenience grocery stores that sell alcoholic beverages and goods (Masho and Bishop 2005).
Convenience grocery stores where community action had led to license restrictions between January and June of 2003 were identified from the ABC licensure database, and their locations were geocoded. These 18 stores were located within five separate census tracts. The five tracts containing these stores were selected to represent the intervention communities. We then selected five demographically similar census tracts (see Table 1). These comparison communities contained 18 ABC-licensed stores where restrictions had not been imposed. To prevent bias due to diffusion effects of the intervention, the comparison communities were selected from a separate part of the city where youth violence activity is also historically high. Whereas the intervention tracts were located in the central and northern areas of the city, the selected controls were located in the city's south side (Fig. 1).

Intervention and control areas and distribution of convenience grocery stores
Data Source and Analysis
Demographic data for each census tract were obtained from the US Census Bureau (US Census Bureau 2002). Indicators examined included proportions of residents between 15 and 24 years, educational attainment of residents 25 years and older, female-headed households with children 18 years of age or younger, race and ethnic groups, and poverty ratio (ratio of income to poverty level). The proportions were computed for each census tract, and means were compared across conditions (i.e., intervention versus control). Data on ambulance pickups for intentional injury between July 2001 and December 2004 were obtained from the Richmond Ambulance Authority (RAA). The RAA has the franchise to provide emergency medical services to the city. Although there are other transport companies that are volunteer rescue squads or “concierge” services, the RAA is the main service provider in the city. The type of intentional injury was coded based on the paramedics' assessments and patients' reports. Events where an assault occurred, including rape, fight/brawl, shooting, or stabbing, were categorized as a violent injury-related event and included in the analysis. Because violent injuries disproportionately affect the youth population, this analysis was conducted for youth 15 to 24 years of age. The RAA data also included information on longitude and latitude to indicate the location of the incidents for geocoding. Spatial analysis using Geographic Information System software (ArcGIS Desktop version 9.1) was conducted to examine data by census tracts.
The rate of intentional injury-related ambulance pickups was calculated using the average number of RAA pickups per month for each census tract per 1,000 populations in the specified time period. Rates were calculated for the 18 months preceding restrictions (baseline phase), the 6 months during which restrictions were in place (intervention phase), and the 18 months following removal of the restrictions (reversal phase).
Analyses of changes in ambulance pickups for intentional injuries across the three phases were conducted using SAS Proc Mixed. Analyses were based on a multilevel modeling approach in which observations during each of the three phases of the study (i.e., baseline, intervention, and reversal) were considered nested within census tracts. Phase was treated as a random effect using dummy coding of the intervention and reversal phases with baseline phase as the reference. This allowed us to model changes in the rate of ambulance pickups within census tracts across the three phases. We considered this preferable to a more typical growth curve approach to modeling changes across phases because we anticipated non-linear change across the baseline, intervention, and reversal phases in census tracts where ABC license restrictions were imposed and then withdrawn. We concluded that modeling intervention effects on changes relative to baseline would provide a more easily interpretable and direct test than examining intervention effects on growth parameters within a non-linear change model. These effects were readily incorporated into a mixed effects analysis as reflected in the following equations for the level 1 and level 2 models.
This level 1 equation (see Eq. 1) represents Y ti, the rate of ambulance pickups during phase t for census tract i, as a function of the rate during the baseline phase (β 0i ), the change from the baseline to the intervention phase (β 1i , where P I is coded 1 for the intervention phase and 0 otherwise), the change from the baseline to the reversal phase (β 2i , where P R is coded 1 for the reversal phase and 0 otherwise), and a residual term (ε ti ).
The level 2 equations (see Eqs. 2, 3, and 4 above) included intercepts γ 00, γ 10, and γ 20 that represent the grand means for census tracts in the control condition for the parameters in Eq. 1, and γ 01, γ 11, and γ 21 that represent the intervention effects on these parameters, respectively. INT is the dummy-coded intervention condition (1 for intervention condition and 0 for control). This provided a basis for testing differences between tracts in the intervention and control conditions (a) in rates at baseline, γ 01; (b) in change in rates from the baseline to intervention phase, γ 11; and (c) in change in rates from the baseline to reversal phase, γ 21. Follow-up tests were also conducted to examine effects within each condition using procedures in Proc Mixed that allow for focused tests on parameter estimates. For example, testing the significance of γ 10 + γ 11 indicates whether the change across the baseline and intervention phases is significant for tracts in the intervention condition. An unstructured model of the covariance structure was used as it fit the data significantly better than models with more restrictive assumptions (e.g., symmetric, compound symmetry) based on differences in the deviance (−2 log likelihood) for the various models.
Results
Demographic characteristics of the intervention and control communities during the study period (3.5 years) are reported in Table 1. Intervention and comparison communities did not significantly differ at p < 0.05 in the proportion of residents who were African Americans, were married, were living in female-headed households with children, were between 15 and 24 years old, were at or below the poverty level, or who had less than a high school education. The average rate of ambulance pickups per month for intentional injuries during the baseline phase was higher in the intervention community than in the control community (19.6 versus 7.4 per 1,000 15- to 24-year-old population, respectively), but this difference was not statistically significant at p < 0.05.
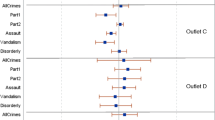
Parameter estimates for the mixed effects models are reported in Tables 2 and 3. Monthly rates of ambulance pickups for intentional injury per 1,000 in the 15- to 24-year-old population across the three phases by condition are reported in Fig. 2 along with 95 % confidence intervals. Ambulance pickup rates for intentional injuries were not significantly different for tracts in the intervention and control conditions at baseline (see γ 01 in Table 2). There was, however, a significant difference between tracts in the intervention and control conditions in their degree of change across the baseline and intervention phases (see γ 11 in Table 2). For tracts within the control condition, rates per 1,000 15 to 24-year olds during the intervention and reversal phases did not significantly differ from rates during the baseline phase (see Fig. 2 and γ 10 and γ 20 in Table 2). In contrast, the average rate of ambulance pickups in the intervention tracts sharply declined between the baseline and intervention phases, decreasing from 19.6 per 1,000 15- to 24-year olds at baseline to 0 during the intervention phase (γ 10 + γ 11 = −19.55, t(16) = −5.16, p < 0.001), and subsequently increased to 11.4 during the reversal phase (i.e., [γ 20 + γ 21] − [γ10 + γ11] = 11.44, t(16) = 4.52, p = 0.022). This pattern of findings was consistent with our hypothesis that rates would decline following imposition of restricted ABC licensing in tracts in the experimental condition, but would increase when this policy was reversed.

Monthly rates of intentional injury ambulance pickups for 15–24-year olds by phase and condition. Error bars represent 95 % confidence intervals
Discussion
This study revealed an association between the restriction of single-serve alcoholic beverages at convenience stores within the intervention communities and a decline in the rate of intentional injury-related ambulance pickups among youth 15 to 24 years old. The study also showed a gradual increase in injury-related ambulance pickup rates after the restriction was reversed. Although numerous studies have examined the association between alcohol outlet density and violence (Alaniz et al. 1998; Branas, et al. 2009; Britt et al. 2005; Escobedo and Ortiz 2002; Franklin et al. 2010; Gorman et al. 2001; Gruenewald et al. 2006; Lipton and Gruenewald 2002; Nielsen and Martinez 2003; Reid et al. 2003; Scribner et al. 1995, 1999; Zhu et al. 2004), we are not aware of any studies that have evaluated the impact of restricting sales of these inexpensive, single-serve alcoholic beverages on the rate of intentional injury ambulance pickups or community-level violence-related outcomes. The results of our study are, however, consistent with few related studies. A recent quasi-experimental study that utilized a pre-post design examined the impact of malt liquor sales restrictions on crimes, at three stores, in a large midwestern city in the USA (Barajas et al. 2011). The study reported a reduction in disorderly conduct in the restricted sales areas, although an increase in other forms of crimes was observed. Another study, by Parker et al. (2011), that examined refrigerated shelf space dedicated to single-serve containers as a proxy for single-serve alcohol sale, also reported a positive association between single-serve sales availability (i.e., shelf space) and rates of violence.
This pattern of findings is consistent with a recent review by Campbell et al. (2009) who noted a relation between violent crime and off-premise outlets. Their review also calculated mean elasticities. They reported a high mean elasticity of 0.48; which meant that for every 1 % increase in outlet density, there was a 0.48 % increase in violent crime. A related cross-sectional study by Branas et al. (2009) that examined alcohol outlets and assaults involving firearms also reported a twofold increased risk of firearm-related assaults in high-density off-site alcohol venues compared to areas with low density area (OR = 2.00, 95 % CI = 1.05–3.75). Few longitudinal studies have examined the relation between violence and off-site alcohol venues. In 2006, the sentinel longitudinal study conducted by Gruenewald and Remer (2006) reported a 1.7 % increase in violence, for every 10 % increase in off-site alcohol outlets. Another longitudinal study, conducted in Australia, also found a positive relation between three types of alcohol premises (general, on premise, and packaged) and violence; however, these types of outlets may not be comparable to those found in the USA (Livingston 2008).
More generally, this study illustrated the utility of using youth violence surveillance data to promote community mobilization and community-led action (Meyer et al. 2008). It also highlighted the use of surveillance data for community-based participatory research to promote community–academic partnerships. Routine collection and geo-mapping of surveillance data suggested elevated violence-related incidents in areas served by convenience stores with unrestricted licenses. Outreach workers presented these data to community groups to document the magnitude of the problem. Unlike many academic-initiated studies where researchers impose predetermined objectives on the community, the presentation of the surveillance data mobilized the communities to convene and pursue policy actions. This approach allowed the implementation of community-based participatory research, by “equitably involving all partners in the research process” with the “aim of combining knowledge with action” (Community Health Scholars Program website, as cited in Katz 2004). These types of strategies not only serve to inform and educate stakeholders, but also assist in engaging the community in their own health (Masho et al. 2010). Such efforts are consistent with emerging environmental efforts to promote and evaluate change at the community level (Fagan et al. 2010).
Although this community effort allowed us to take advantage of a “natural” experiment to examine the effect of restricted sale of inexpensive, single-serve alcoholic beverages on youth violence, the quasi-experimental nature of this study, covering a relatively small geographic area, has several clear limitations. The use of surveillance data led to community mobilization to pursue policy changes to address this problem. Once initiated, these efforts could not be easily subverted by suggesting that the participating communities be subjected to random assignment to intervention and control conditions. This hampers our ability to draw clear causal inferences regarding the impact of policy changes versus other changes that may have occurred within the intervention and comparison communities. The unfortunate and unexpected reversal of policy resulted in a fairly short intervention phase. More generally, the limited number of communities in each condition and fairly low base rate of violence-related ambulance pickups resulting from aggregating data within fairly short windows of time within communities provided limited statistical power to detect differences. A longer intervention phase and replication across communities would have provided a clearer basis for drawing a connection between the intervention and observed outcomes (Biglan et al. 2000). Another limitation was the small number of tracts included in this analysis (N = 10). Additionally, this study was unable to examine other moderating factors such as illegal drug sales and loitering. Finally, these data did not examine other less serious intentional injuries that did not require emergency services, which may have been more common than the serious injuries.
Although this study lacked the rigor of a large-scale experimental study, we believe it illustrates the potential value of using surveillance data to inform community mobilization efforts and to evaluate the impact of such efforts. In particular, it demonstrates the potential impact of policies restricting sale of inexpensive, single-serve alcoholic beverages on the rates of intentional injury-related ambulance pickups. It also provides relevant pilot information to emerging large-scale youth violence prevention efforts. Furthermore, this study demonstrated the utility of surveillance data to assess policy changes and community efforts in making significant impacts in communities. It highlights the use of surveillance data to promote and enhance community–academia partnerships in conducting community-based participatory research.
Public health professional and community advocates should be aware of the potential impacts of inexpensive, single-serve alcoholic beverages on violence. Future studies should be conducted using large-scale community-wide data to confirm the finding of this study.
References
Alaniz, M. L., Cartmill, R. S., & Parker, R. N. (1998). Immigrants and violence: The importance of neighborhood context. Hispanic Journal of Behavioral Sciences, 20, 155–175. doi:10.1177/07399863980202002.
Barajas, E., McKee, P., Hannan, P. J., Nelson, T. F., & Jones-Webb, R. (2011). Effects of policies to restrict malt liquor sales on neighborhood crime. Substance Use and Misuse, 46, 1234–1243. doi:10.3109/10826084.2011.567367.
Branas, C. C., Elliott, M. R., Richmond, T. S., Culhane, D. P., & Wiebe, D. J. (2009). Alcohol consumption, alcohol outlets, and the risk of being assaulted with a gun. Alcoholism, Clinical and Experimental Research, 33, 906–915. doi:10.1111/j.1530-0277.2009.00912.x.
Biglan, A., Ary, D., & Wagenaar, A. C. (2000). The value of interrupted time-series experiments for community intervention research. Prevention Science, 1, 31–49. doi:10.1023/A:1010024016308.
Britt, H. R., Carlin, B. P., Toomey, T. L., & Wagenaar, A. C. (2005). Neighborhood level spatial analysis of the relationship between alcohol outlet density and criminal violence. Environmental and Ecological Statistics, 12, 411–426. doi:10.1007/s10651-005-1518-3.
Campbell, A. C., Han, R. A., Elder, R., Brewer, R., Chattopadhyay, S., Fielding, J., & Task Force on Community Preventive Services. (2009). The effectiveness of limiting alcohol outlet density as a means of reducing excessive alcohol consumption and alcohol-related harms. American Journal of Preventative Medicine, 37, 556–568. doi:10.1016/j.amepre.2009.09.028.
Centers for Disease Control and Prevention. (2010). MMWR weekly: Youth risk behavioral surveillance—United States, 2009. http://www.cdc.gov/mmwr/pdf/ss/ss5905.pdf. Accessed 10 Jan 2013.
Chavira, C., Bazargan-Hejazi, S., Lin, J., del Pino, H. E., & Bazargan, M. (2011). Type of alcohol drink and exposure to violence: An emergency department study. Journal of Community Health, 36, 597–604. doi:10.1007/s10900-010-9347-1.
Escobedo, L. G., & Ortiz, M. (2002). The relationship between liquor outlet density and injury and violence in New Mexico. Accident Analysis and Prevention, 34, 689–94. doi:10.1016/S0001-4575(01)S000/S0001-4575%2801%2900068-9.
Fagan, A. A., Hanson, K., Hawkins, J. D., & Arthur, M. W. (2010). Translational research in action: Implementation of the communities that care prevention system in 12 communities. Journal of Community Psychology, 37, 809–829. doi:10.1002/jcop.20332.
Franklin, F. A., Laveist, T. A., Webster, D. W., & Pan, W. K. (2010). Alcohol outlets and violent crime in Washington D.C. Western Journal of Emergency Medicine, 11, 283–290. Retrieved from http://escholarship.org/uc/item/36j311xv. Accessed 10 Jan 2013.
Gorman, D. M., Speer, P. W., Gruenewald, P. J., & Labouvie, E. W. (2001). Spatial dynamics of alcohol availability, neighborhood structure and violent crime. Journal of Studies on Alcohol and Drugs, 62, 628–637. Retrieved from http://www.jsad.com/jsad/downloadarticle/Spatial_Dynamics_of_Alcohol_Availability_Neighborhood_Structure_and_Violen/1486.pdf. Accessed 10 Jan 2013.
Gruenewald, P. J., Freisthler, B., Remer, L., LaScala, E. A., & Treno, A. (2006). Ecological models of alcohol outlets and violent assaults: Crime potentials and geospatial analysis. Addiction, 101, 666–677. doi:10.1111/j.1360-0443.2006.01405.x.
Gruenewald, P. J., & Remer, L. (2006). Changes in outlet densities affect violence rates. Alcoholism: Clinical and Experimental Research, 30, 1184–1193. doi:10.1111/j.1530-0277.2006.00141.x.
Jones-Webb, R., Mckee, P., Hannann, P., Wall, M., Pham, L., Erickson, D., & Wagenaar, A. (2008). Alcohol and malt liquor availability and promotion and homicide in inner cities. Substance Use & Misuse, 43, 159–177. doi:10.1080/10826080701690557.
Katz, D. (2004). Representing your community in community-based participatory research: Differences made and measured. Preventing Chronic Disease: Public Health Research, Practice and Policy, 1, 1–4. Retrieved from http://www.cdc.gov/pcd/issues/2004/jan/03_0024.htm. Accessed 10 Jan 2013.
LaVeist, T. A., & Wallace, J. M. (2000). Health risk and inequitable distribution of liquor stores in African American neighborhoods. Social Science and Medicine, 51, 613–617. doi:10.1016/S0277-9536(00)00004-6.
Lipton, R., & Gruenewald, P. (2002). The spatial dynamics of violence and alcohol outlets. Journal of Studies on Alcohol, 63, 187–195. Retrieved from http://www.jsad.com/jsad/downloadarticle/The_Spatial_Dynamics_of_Violence_and_Alcohol_Outlets/1426.pdf. Accessed 10 Jan 2013.
Livingston, M. (2008). A longitudinal analysis of alcohol outlet density and assault. Alcoholism; Clinical and Experimental Research, 32, 1074–1079. doi:10.1111/j.1530-0277.2008.00669.x.
Masho, S.W. & Bishop, D.L. (2005). Spatial distribution of public housing and convenience grocery stores. http://www.clarkhill.vcu.edu/research.html. Accessed 10 Jan 2013.
Masho, S. W., Keyser-Marcus, L., Varner, S., Singleton-Seth, R., Bradford, J., Chapman, D., & Svikis, D. (2010). Addressing perinatal disparities using community based participatory research. Journal of Community Psychology, 39, 292–302. doi:10.1002/jcop.20432.
Mercy, J. A., Butchart, A., Farrington, D., & Cerdá, M. (2002). Youth violence. In E. G. Krug, L. L. Dahlberg, J. A. Mercy, A. B. Zwi, & R. Lozano (Eds.), The world report on violence and health. Geneva: World Health Organization. Retrieved from http://www.who.int/violence_injury_prevention/violence/global_campaign/en/chap2.pdf. Accessed 10 Jan 2013.
Meyer, A., Cohen, B., Edmond, T., & Masho, S. W. (2008). Developing a comprehensive approach to youth violence prevention in a small city. American Journal of Preventive Medicine, 34, s13–s20. doi:10.1016/j.amepre.2007.12.006.
Nielsen, A. L., & Martinez, R. (2003). Reassessing the alcohol-violence linkage: Results from a multiethnic city. Justice Quarterly, 20, 445–469. doi:10.1080/07418820300095581.
Parker, R. N., McCaffree, K. J., & Skiles, D. (2011). The impact of retail practices on violence: The case of single serve alcohol beverage containers. Drug and Alcohol Review, 30, 496–504. doi:10.1111/j.1465-3362.2011.00318.x.
Pollack, C. E., Cubbin, C., Ahn, D., & Winkleby, M. (2005). Neighbourhood deprivation and alcohol consumption: Does the availability of alcohol play a role? International Journal of Epidemiology, 34, 772–780. doi:10.1093/ije/dyi026.
Reid, R. J., Hughey, J., & Peterson, N. A. (2003). Generalizing the alcohol outlet assaultive violence link: Evidence from a U.S. midwestern city. Substance Use and Misuse, 38, 1971–1982. doi:10.1081/JA-120025122.
Scribner, R. A., MacKinnon, D. P., & Dwyer, J. H. (1995). The risk of assaultive violence and alcohol availability in Los Angeles county. American Journal of Public Health, 85, 335–340. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1614881. Accessed 10 Jan 2013.
Scribner, R. A., Cohen, D. A., Kaplan, S., & Allen, S. H. (1999). Alcohol availability and homicide in New Orleans: Conceptual considerations for small area analysis of the effect of alcohol outlet density. Journal of Studies on Alcohol and Drugs, 60, 310–316. Retrieved from http://www.jsad.com/jsad/downloadarticle/Alcohol_Availability_and_Homicide_in_New_Orleans_Conceptual_Considerations/671.pdf. Accessed 10 Jan 2013.
US Department of Health and Human Services. (2001). Youth violence: A report of the surgeon general. Washington, DC: United States Department of Justice. Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK44294. Accessed 10 Jan 2013.
US Department of Justice, Federal Bureau of Investigation. (2009). Crime in the United States, 2008. http://www.fbi.gov/ucr/cius2008/data/table_01.html. Accessed 10 Jan 2013.
US Census Bureau (2009). State and county quick facts. http://quickfacts.census.gov/pdf/states/51/51760.html. Accessed 10 Jan 2013.
US Census Bureau. (2002). Census 2000, summary file 3 (Virginia). http://www.census.gov/census2000/states/va.html. Accessed 10 Jan 2013.
Zhu, L., Gorman, D. M., & Horel, S. (2004). Alcohol outlet density and violence: A geospatial analysis. Alcohol, 39, 369–375. doi:10.1093/alcalc/agh062.
Author information
Authors and Affiliations
Corresponding author
Additional information
This research was supported by cooperative agreement U49/CE000730 from the Centers for Disease Control and Prevention (CDC). The research and interpretations reported are the sole responsibility of the authors and are not necessarily endorsed by CDC or represent the views, opinions, or policies of the CDC or their staff.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Masho, S.W., Bishop, D.L., Edmonds, T. et al. Using Surveillance Data to Inform Community Action: The Effect of Alcohol Sale Restrictions on Intentional Injury-related Ambulance Pickups. Prev Sci 15, 22–30 (2014). https://doi.org/10.1007/s11121-013-0373-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-013-0373-y