
Abstract
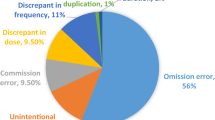
Background Medication discrepancies are common when patients cross organisational boundaries. However, little is known about the frequency of discrepancies within mental health and the efficacy of interventions to reduce discrepancies. Objective To evaluate the impact of a pharmacy-led reconciliation service on medication discrepancies on admissions to a secondary care mental health trust. Setting In-patient mental health services. Methods Prospective evaluation of pharmacy technician led medication reconciliation for admissions to a UK Mental Health NHS Trust. From March to June 2012 information on any unintentional discrepancies (dose, frequency and name of medication); patient demographics; and type and cause of the discrepancy was collected. The potential for harm was assessed based on two scenarios; the discrepancy was continued into primary care, and the discrepancy was corrected during admission. Logistic regression identified factors associated with discrepancies. Main outcome measure Mean number of discrepancies per admission corrected by the pharmacy technician. Results Unintentional medication discrepancies occurred in 212 of 377 admissions (56.2 %). Discrepancies involving 569 medicines (mean 1.5 medicines per admission) were corrected. The most common discrepancy was omission (n = 464). Severity was assessed for 114 discrepancies. If the discrepancy was corrected within 16 days the potential harm was minor in 71 (62.3 %) cases and moderate in 43 (37.7 %) cases whereas if the discrepancy was not corrected the potential harm was minor in 27 (23.7 %) cases and moderate in 87 (76.3 %) cases. Discrepancies were associated with both age and number of medications; the stronger association was age. Conclusions Medication discrepancies are common within mental health services with potentially significant consequences for patients. Trained pharmacy technicians are able to reduce the frequency of discrepancies, improving safety.
Similar content being viewed by others

References
Institute for Healthcare Improvement. Accuracy at every step: the challenge of medication reconciliation. Cambridge, MA: Institute of Healthcare Improvement; 2006. Available on www.ihi.org/knowledge/pages/improvementstories/accuracyateverystep.aspx. Accessed 12 Sept 2013.
National Institute for Clinical Excellence. Technical patient safety solutions for medicines reconciliation on admission of adults to hospital. Alert reference: NICE/NPSA/2007/PSG001. National Institute for Clinical Excellence; 2007. Available on http://www.nice.org.uk/nicemedia/pdf/PSG001Guidance.pdf. Accessed 12 Sept 2013. ISBN 1-84629-563-7.
Lizer MH, Brackbill ML. Medication history reconciliation by pharmacists in an inpatient behavioral health unit. Am J Health Syst Pharm. 2007;64:1087–91.
Maidment ID, Haw C, Stubbs J, Fox C, Katona C, Franklin BD. Medication errors in older people with mental health problems: a review. Int J Geriatr Psychiatry. 2008;23:564–73.
Procyshyn RM, Barr AM, Brickell T, Honer WG. Medication errors in psychiatry: a comprehensive review. CNS Drugs. 2010;24:595–609.
Marvanova M, Roumie CL, Eden SK, Cawthon C, Schnipper JL, Kripalani S, et al. Health literacy and medication understanding among hospitalized adults. J Hosp Med. 2011;6:488–93.
Maidment ID, Parmentier H. Medication error in mental health: implications for primary care. Men Health Fam Med. 2009;6:203–7.
Morcos S, Francis SA, Duggan C. Where are the weakest links? Psychiatr Bull. 2002;26:371–4.
Hellstrom LM, Bondesson A, Hogland P, Eriksson T. Errors in medication history at hospital admission: prevalence and predicting factors. BMC Clin Pharmacol. 2012;12:9.
Mueller SK, Sponsler KC, Kripalani S, Schnipper JL. Hospital-based medication reconciliation practices. Arch Int Med. 2012;172:1057–69.
Michels RD, Meisel SB. Program using pharmacy-technicians to obtain medication histories. Am J Health Syst Pharm. 2003;60:1982–6.
van den Bemt PM, van den Broek S, van Nunen AK, Harbers JB, Lenderink AW. Medication reconciliation performed by pharmacy technicians at the time of preoperative screening. Ann Pharmacother. 2009;43:868–74.
Essex JSNA. Geography and demographics—chapter. Version 1.4—September 2010. Available on http://www.essexpartnershipportal.org/pages/uploads/JSNA/Demography%20refresh%20chapter%20-%20update%20v1.4.pdf. Accessed 12 Sept 2013.
National Patient Safety Agency. Patient safety incident report form; Healthcare Staff. National Patient Safety Agency; 2009. Available on https://www.eforms.npsa.nhs.uk/staffreport/. Accessed 12 Sept 2013.
Pippins JR, Gandhi TK, Hamann C, Ndumele CD, Labonville SA, Diedrichsen EK, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Int Med. 2008;23:1414–22.
Dean BS, Barber ND. Validated, reliable method of scoring the severity of med errors. Am J Health Syst. 1999;56:57–62.
Grimes TC, Duggan CA, Delaney TP, Graham IM, Conlon KC, Deasy E, et al. Medication details documented on hospital discharge: cross-sectional observational study of factors associated with medication non-reconciliation. Br J Clin Pharmacol. 2011;73:449–57.
Galvin M, Jago-Byrne MC, Fitzsimons F, Grimes T. Clinical pharmacist’s contribution to medication reconciliation on admission to hospital in Ireland. Int J Clin Pharm. 2013;35:14–21.
The Information Centre. Hospital episode statistics 2011–12. The Information Centre; 2012. Available on http://www.hesonline.nhs.uk/Ease/servlet/ContentServer?siteID=1937&categoryID=212. Accessed 14 Sept 2013.
Bishop CM. Pattern recognition and machine learning. Berlin: Springer; 2006.
Mehta R, Onatade R. Auditing medication history-taking can help demonstrate improved pharmacy services. Phar Pract. 2008;18:209–13.
Cornish PL, Knowles SE, Marchesano R, Tam V, Shadowitz S, Juurlink DN, et al. Unintended medication discrepancies at the time of hospital admission. Arch Int Med. 2005;165:424–9.
Gleason KM, McDaniel MR, Feinglass J, Baker DW, Lindquist L, Liss D, et al. Results of the Medications at transitions and clinical handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Int Med. 2010;25:441–7.
Lubowski TJ, Cronin LM, Pavelka RW, Briscoe-Dwyer LA, Briceland LL, Hamilton RA. Effectiveness of a medication reconciliation project conducted by PharmD Students. Am J Pharm Educ. 2007;71:1–7.
McFazdean E, Isles C, Moffat J, Norrie J, Steward DI. Is there a role for a prescribing pharmacist in preventing prescribing errors in the medical admissions ward? Pharm J. 2003;270:896–9.
Campbell F, Karnon J, Czoski-Murray C. A systematic review of the effectiveness and cost effectiveness of interventions aimed at preventing medication error (medicines reconciliation) at hospital admission. The University of Sheffield, School of Health and Related Research (ScHARR); 2007. Available on: http://www.nice.org.uk/nicemedia/live/11897/38591/38591.pdf. Accessed 12 Sept 2013.
Department of Health. Living well with dementia: A national dementia strategy. Department of Health Publications, London; 2009. Available on: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/168220/dh_094051.pdf. Accessed 13 Sept 2013.
Chhabra PT, Rattinger GB, Dutcher SK, Hare ME, Parsons KL, Zuckerman IH. Medication reconciliation during the transition to and from long-term care settings: a systematic review. Res Soc Adm Pharm. 2012;8:60–75.
Richards M, Ashiru-Oredope D, Chee N. What errors can be identified by pharmacy-led medicines reconciliation? A prospective study. Acute Med. 2011;10:18–21.
Greenwald JL, Halasyamani L, Greene J, LaCivita C, Stucky E, Benjamin B, et al. Making inpatient medication reconciliation patient centered, clinically relevant and implementable: a consensus statement on key principles and necessary first steps. J Hosp Med. 2010;5:477–85.
Kaboli PJ, Fernandes O. Medication reconciliation: moving forward. Arch Int Med. 2012;172:1069–70.
Acknowledgments
We acknowledge the support from both ward staff and pharmacy staff (including Hilary Scott, Chief Pharmacist).
Funding
None.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brownlie, K., Schneider, C., Culliford, R. et al. Medication reconciliation by a pharmacy technician in a mental health assessment unit. Int J Clin Pharm 36, 303–309 (2014). https://doi.org/10.1007/s11096-013-9875-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-013-9875-8