
Abstract
Purpose
We assessed the human in vivo metabolic drug interaction profile of Ginkgo biloba extract EGb 761® with respect to the activities of major cytochrome P450 (CYP) enzymes.
Methods
A single-center, open-label, randomized, three-fold crossover, cocktail phenotyping design was applied. In random order, the following treatments were administered to 18 healthy men and women for 8 days each: placebo twice daily, EGb 761® 120 mg twice daily, and EGb 761® 240 mg in the morning and placebo in the evening. In the morning of day 8, administration was performed together with the orally administered phenotyping cocktail (enzyme, metric): 150 mg caffeine (CYP1A2, paraxanthine/caffeine plasma ratio 6-h postdose), 125 mg tolbutamide (CYP2C9, plasma concentration 24-h postdose), 20 mg omeprazole (CYP2C19, omeprazole/5-hydroxy omeprazole plasma ratio 3-h postdose), 30 mg dextromethorphan (CYP2D6, dextromethorphan/dextrorphan plasma ratio 3-h postdose), and 2 mg of midazolam (CYP3A, plasma concentration 6-h postdose). Formally, absence of a relevant interaction was assumed if the 90% confidence intervals (CIs) for EGb 761®/placebo ratios of the metrics were within the 0.70–1.43 range.
Results
EGb 761®/placebo ratios for phenotyping metrics were close to unity for all CYPs. Furthermore, respective CIs were within the specified margins for all ratios except CYP2C19 for EGb 761® 120 mg twice daily (90% CI 0.681–1.122) and for CYP2D6 for EGb 761® 240 mg once daily (90% CI 0.667–1.281). These findings were attributed to the intraindividual variability of the metrics used. All treatments were well tolerated.
Conclusion
EGb 761® has no relevant effect on the in vivo activity of the major CYP enzymes in humans and therefore has no relevant potential to cause respective metabolic drug–drug interactions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ginkgo biloba extract is a popular herbal remedy used for a variety of disorders. EGb 761®Footnote 1 special extract is a dry extract from Ginkgo biloba leaves (drug-extract ratio 35–67:1) that has been adjusted to 22.0–27.0% ginkgo flavonoids and 5.0–7.0% terpene lactones consisting of 2.8–3.4% ginkgolides A, B, C; and 2.6–3.2% bilobalides, with a ginkgolic acid content <5 ppm [1]. EGb 761® interferes with various pathomechanisms relevant to dementing disorders [2–4]. A large number of clinical trials suggest that Ginkgo biloba extract (GBE) has beneficial effects on memory, cognition, and the vascular system [5–9]. For a herbal drug to be taken by elderly people, who often have several chronic diseases, the ability of GBE to cause metabolic drug–drug interactions should be known. In fact, available data for GBE effects on cytochrome P450 activity in vitro and in vivo from animal and human studies is inconsistent. In vitro studies in rat liver microsomes showed inhibitory effects of GBE on some CYPs [10–12], whereas both inhibition [13, 14] and induction [15–17] was reported for in vivo studies. In vitro experiments carried out in human liver microsomes suggested that GBE weakly inhibits human CYP enzymes, e.g., CYP1A2 and CYP3A [18]. Yale and Glurich [19] found a weak inhibition of CYP2D6 activity (20%) of Ginkgo biloba in vitro and moderate inhibition for CYP2C9 and CYP3A. The effect of Ginkgo biloba was also assessed on a panel of recombinant human CYPs (CYP1A2, CYP2C9, CYP2C19, CYP2D6, CYP3A). Constituents of Ginkgo biloba (ginkgolic acids I and II) significantly inhibited CYP1A2 (IC50 = 4.85 μM), CYP2C9 (IC50 = 2.25 μM), and CYP2C19 (IC50 = 4.3 μM) [20]. The extract tested in the study reported here, EGb 761®, was also tested for its ability to inhibit major human CYPs. Except for CYP2D6 (K i > 900 μg/ml), the full extract was observed to strongly inhibit CYP2C9 (K i = 14 ± 4 μg/ml) and, to a lesser extent, CYP1A2 (K i = 106 ± 24 μg/ml), CYP2E1 (K i = 127 ± 42 μg/ml), and CYP3A (K i = 155 ± 43 μg/ml) [21].
Whereas studies using enzymes from laboratory animals and in vitro studies with human material may provide some general information, especially with herbal drugs, it is difficult to predict drug–drug interactions in patients in this way [22]. The interplay of multiple chemical moieties, each of these subject to its own pharmacokinetics, limits the applicability of mechanistic approaches for in vitro/in vivo extrapolations. Available in vivo studies in humans indicate that GBE has no effect on the hepatic microsomal drug oxidation system [23]. In a clinical trial with 12 healthy volunteers, no significant effect on CYP1A2, CYP2D6, CYP2E1, and CYP3A activity for Ginkgo biloba was found [24]. Another clinical study with 12 healthy volunteers assessed the influence of GBE on CYP2D6 and CYP3A activity using the probe substrates dextromethorphan (DEX) and alprazolam, respectively. No differences were observed between baseline and post-GBE treatment [25]. A pharmacokinetic study in healthy volunteers conducted with diazepam as a substrate of CYP2C19 also did not provide evidence for a herb–drug interaction [26]. Izzo and Ernst [27] reviewed the literature (Medline, Cochrane Library and Embase) to determine the possible interactions between seven popular herbal medicines, including ginkgo. They summarized from about 128 case reports and 80 clinical trials that an effect on CYP enzymes by ginkgo seems unlikely.
In summary, despite limited in vivo data supporting the absence of major effects, it cannot be excluded that EGb 761® may alter the activity of CYP enzymes in patients. The objective of our study was to quantitatively assess the in vivo herbal drug–drug interaction potential of EGb 761® with respect to the five major human drug-metabolizing CYP enzymes.
Materials and methods
Study participants
The study (EudraCT number 2008-005686-63) was approved by the Ethics Committee of the Chamber of Physicians of Northrhine and the pertinent regulatory authorities and conducted as defined in local regulations, International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH-GCP), Directive 2001/20/EC, and in accordance with the Declaration of Helsinki. Eighteen healthy volunteers gave written informed consent to participate in the study. Participants were considered to be in good health on the basis of medical history, physical examination, vital signs measurement, electrocardiogram (ECG), and clinical laboratory tests. Volunteers were required to be Caucasian, of either gender, aged between 18 and 55 years, to have a body mass index (BMI) between 19 and 29 kg/m2, to be a nonsmoker, and (if female) be and stay nonpregnant and nonlactating. Drugs other than the study medication (within 2 weeks prior to study start), usual consumption of >50 g alcohol per day, illicit drugs, and concomitant intake of alcohol, methylxanthines, or grapefruit products (72 h before first study drug administration until 48 h after last study drug administration) was prohibited.
Study design
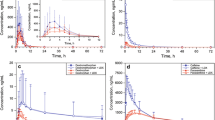
The study had an open-label, single-center, randomized, threefold cross-over design. The following treatments were administered for 8 days each: placebo twice daily (treatment A), EGb 761® 120 mg twice daily (treatment B), and EGb 761® 240 mg in the morning and placebo in the evening (treatment C). In the morning of day 8, administration was performed together with the orally administered phenotyping cocktail: 150 mg caffeine (CAF) (three tablets of Percoffedrinol®, Lindopharm GmbH, Germany), 125 mg of tolbutamide (TOL) (one fourth of a tablet of Tolbutamide 500 mg, Actavis UK Limited, UK), 20 mg omeprazole (OME) (one tablet Omeprazol-ratiopharm® NT 20 mg, ratiopharm GmbH, Germany), 30 mg DEX hydrobromide (one capsule Hustenstiller-ratiopharm®, ratiopharm GmbH, Germany). Administration of 2 mg midazolam (MID) (Dormicum® V Injektionslösung, Roche Pharma AG, Germany) orally with 120 ml of water was administered 1 min thereafter. The three study periods were separated by a washout phase of at least 14 days between cocktail administrations. On each day, drug administration took place between 7:00 and 9:00 a.m. and between 7:00 and 9:00 p.m., with an interval of exactly 12 h between doses. For an individual participant, the same time of study-drug administration was used for all periods. Participants fasted from 2 h before until 2 h after evening dose on day 7 and 8 and at least 9 h before until 6 h after administration in the morning of day 8 and from 2 h before until 2 h after evening dose on day 8. Blood samples to check for exposure/compliance and steady-state conditions (plasma concentrations of the four terpene lactones bilobalide, ginkgolide A, B, and C) were collected approximately 10 min prior to the 9th, 13th, and 15th dose of EGb 761® or placebo. Blood samples for phenotyping agents [to determine CAF, paraxanthine (PAX), TOL, OME, 5-hydroxy OME (5-OH-OME), DEX, dextrorphan (DOR), and MID] were collected via an indwelling catheter into 9-ml Li-Heparin Monovettes® (Sarstedt) on day 8 approximately 10 min prior to dosing of the cocktail and 3, 6, and 24 h thereafter.
Handling of pharmacokinetic samples
Immediately after withdrawal, blood samples for compliance were cooled in ice water, centrifuged for 10 min at 4°C at 2.000 g. To analyze terpene lactones as pharmacokinetic marker constituents of EGb 761®, the supernatant plasma was transferred into two polypropylene tubes, acidified with hydrochloric acid (to stabilize terpene lactones), and stored <−20°C until analysis. Blood samples drawn for phenotyping agents were handled the same way except that no hydrochloric acid was added and storing temperature was <−65°C.
Sample preparation for analysis
After thawing, plasma samples (200 μl) were precipitated with 400 μl acetonitrile (ACN) for the CAF, PAX, and TOL assays. For this method, two internal standards [20 μl CAF-d3 (300 ng/ml) and 20 μl TOL-d9 (300 ng/ml) dissolved in ACN] were added. Precipitation was done the same way without an internal standard for OME, 5-OH-OME, DEX, DOR), and MID assays, respectively. After thorough mixing for 10 s, samples were centrifuged for 10 min at room temperature at 20.800 g. After centrifugation, 200 μl of supernatant were transferred into screw-capped glass vials for liquid chromatography tandem mass spectrometry (LC-MS/MS) analysis.
Quantification of phenotyping cocktail substances
Plasma concentrations of CAF, PAX, and TOL were quantified on an API 5000 with QJet™ Ion Guide (Applied Biosystems, Foster City, CA, USA) LC-MS/MS. The effluent of LC system (300 ml/min; 1200 series; Agilent, Waldbronn, Germany) was delivered through a reversed-phase column (125 x 2 mm, 3 μm; Nucleodur C18 Isis, Macherey-Nagel, Dueren, Germany) eluted with a gradient solvent system consisting of water (A) and methanol (B) (0 → 0.75 min A:B 80:20 → A:B 30:70, 0.75 → 4.00 min A:B 30:70, 4.00 → 5.00 min A:B 30:70 → A:B 80:20) to the mass spectrometer. Plasma concentrations of OME, 5-OH-OME, DEX, DOR, and MID were determined on the same system with the following modifications. The effluent (300 ml/min) was delivered through a different reversed-phase column (50 x 2.1 mm, 5 μm; Hypersil Gold, Thermo Electron, Runcorn, UK) eluted with a gradient solvent system consisting of 0.1% formic acid (A) and methanol (B) (0 → 1.5 min A:B 95:5, 1.5 → 1.51 min A:B 95:5 → A:B 10:90, 1.51 → 6 min A:B 10:90 → 6 → 6.5 min A:B 10:90 → A:B 95:5, 6.5 → 10 min A:B 95:5) to the mass spectrometer. Caffeine, CAF-d3, PAX, TOL, and TOL-d9 were detected by positive electrospray ionization (ESI+) in the positive multiple reaction monitoring mode (MRM+) with the following ion transitions [m/z]: 195.1 → 138.0 for CAF, 198.0 → 138.0 for CAF-d3, 181.1 → 124.0 for PAX, 271.3 → 91.1 for TOL, and 280.2 → 90.8 for TOL-d9. CAF, CAF-d3, and PAX were eluted after 2.17 and 1.99 min, respectively. TOL and its internal standard were eluted after 2.55 min. The lower limits of quantification (LLOQ) for CAF and PAX were 100 ng/ml and for TOL 300 ng/ml. Instrument control and data acquisition were performed with the Analyst 1.4.2 software (Applied Biosystems). Peak area ratios (analyte/internal standard) were used for quantification, and calibration functions were calculated via a weighted (1/x) least squares linear regression. CAF and PAX concentrations ranged from 0.2 to 2.5 μg/ml. Interday precision was between 1.8% and 8.2% and 1.5% and 14.5%, respectively, and interday accuracy was between −1.8% and 0.3 % and −5.3% and −0.8 %, respectively. TOL concentrations ranged from 0.6 to 7.5 μg/ml. Interday precision was between 7.3% and 12.5%, and interday accuracy was between −4.7% and 5.4%.
OME, 5-OH-OME, DEX, DOR, and MID were also detected by ESI+ in the MRM+ mode, with the following ion transitions [m/z]: 346.2 → 197.9 for OME, 362.2 → 214.1 for 5-OH-OME, 272.2 → 171.2 for DEX, 258.2 → 157.0 for DOR, and 326.1 → 291.0 for MID. Under these conditions, OME and 5-OH-OME were eluted after 2.87 and 2.82 min, respectively. DEX, DOR, and MID were eluted after 2.80, 2.74, and 2.84 min, respectively. LLOQ for OME and 5-OH-OME was 3.3 ng/ml, for DEX and DOR 0.17 ng/ml, and for MID 0.4 ng/ml. OME and 5-OH-OME concentrations ranged from 3.3 to 360 ng/ml. Interday precision was between 3.0% and 11.7% and 3.7% and 12.2%, respectively, whereas interday accuracy was between −7.4% and 8.4% and −5.4% and 7.0%, respectively. DEX and DOR concentrations ranged from 0.17 to 18.36 ng/ml. The interday precision was between 5.4% and 13.2% and 1.7% and 12.0%, respectively, whereas interday accuracy was between −4.2% and 5.1% and −4.9% and 2.4%, respectively. Concentration ranges for MID were from 0.4 to 43.2 ng/ml. The interday precision was between 4.4% and 7.0%, whereas interday accuracy was between −7.1% and 6.2%.
Quantification of terpene lactones
Plasma concentrations of the four terpene lactones bilobalide and ginkgolide A, B, and C were quantified using LC-MS with electrospray in the negative ionization mode (UltiMate 3000 with detector MSQ+, Dionex, Sunnyvale, CA, USA). Mobile phase was isocratic (0.9 ml/min) methanol/water/formic acid (500/500/0.25 v/v) on a reversed-phase column [250 x 4.6 mm, 5 μm; Luna C18(2), Phenomenex, Torrance, CA, USA] with postcolumn addition of methanol/ammonium hydroxide solution 30% (98/2 v/v) with 0.1 ml/min. Bilobalide and ginkgolide A, B, and C were detected by negative ESI (ESI−) in the selected ion monitoring (SIM) mode with the following ion transitions [m/z]: 324.9 for bilobalide, 406.9 for ginkgolide A, 422.9 for ginkgolide B, and 439.0 for ginkgolide C. Bilobalide and ginkgolide A, B, and C were eluted after 5.4, 7.4, 8.0, and 5.1 min, respectively. LLOQ for ginkgolide A was 1.2 ng/ml and for bilobalide and ginkgolide B and C 0.6 ng/ml. Instrument control and data acquisition were performed with Chromeleon software (Dionex). Peak areas were used for quantification, and calibration functions were calculated via a least square linear regression. Concentrations of bilobalide and ginkgolide A, B, and C ranged from 0.7 to 7.9 ng/ml, 1.3 to 10.2 ng/ml, 1.0 to 6.2 ng/ml, and 0.6 to 1.1 ng/ml, respectively; interday precision was between 1.0% and 10.2%, 0.6% and 12.2%, 1.1% and 10.0%, and 0.3% and 13.9%, respectively, with interday accuracy between −4.9% and 8.0%, –6.9% and 0.0%, –11.7% and 7.7%, and −9.8% and 6.4%, respectively.
CYP phenotyping metrics
Estimation of individual CYP enzyme activity for each enzyme was based on established phenotyping metrics. To establish CYP1A2 activity, the molar PAX over CAF plasma concentration ratio at 6 h postdose was determined. CYP2C9 activity was estimated using the 24-h postdose TOL plasma concentration. In vivo CYP2C19 activity was measured using the molar plasma OME over 5-OH-OME concentration ratio 3 h after OME administration. The 3 h molar plasma concentration ratio of DEX over DOR was used as an index of CYP2D6 activity. Cytochrome P450 3A activity was estimated using the MID plasma concentration 6 h after oral administration.
Statistical methods
Evaluation of phenotyping metrics followed the standard bioequivalence approach, with adjusted margins. Absence of a clinically relevant interaction was concluded if the 90% confidence interval (CI) for estimated ratio μtest/μplacebo did not exceed a range of 0.70–1.43 for a phenotyping metric. For an anticipated intrasubject multiplicative coefficient of variation (CV) of ≤25%, a sample size of n = 14 would have allowed rejection of each null hypothesis “relevant interaction present” with α = 0.05 (two-sided) and a power of at least 90%. Four additional participants were included to account for potential dropouts, resulting in a sample size of n = 18. There was no adjustment for multiple comparisons because all assessments were considered as separate tests. Genotyping was done to identify individuals with two nonfunctional alleles of CYP2C19 and/or CYP2D6, and such individuals were excluded from analyses for the respective metric because any interaction with regard to a specific enzyme cannot occur in its absence.
Results
Demographic data
Eighteen (eight men, ten women) healthy volunteers were included in this study. Mean age [± standard deviation (SD)] was 32.6 ± 9.8 years, mean height 172 ± 8.8 cm, mean body weight 67.4 ± 9.8 kg, and mean body mass index (BMI) 22.7 ± 2.3 kg/m2. All participants completed the three planned study periods. Four participants were poor metabolizers for CYP2D6 and were excluded from analysis of EGb 761® effects on this enzyme; no participant carried two alleles coding for nonfunctional CYP2C19. One participant was also excluded from CYP3A analysis because the concentration was below the LLOQ.
EGb 761® terpene lactone concentrations
Concentrations of terpene lactones from EGb 761® were measured from all 18 participants who received active treatment and completed the study. Between days 5 and 8, geometric mean plasma concentrations for the four terpene lactones showed only small variations: mean values (± SD) varied for ginkgolide A between 2.78 ± 1.64 ng/ml (day 5) and 2.92 ± 1.78 ng/ml (day 7), ginkgolide B between 2.25 ± 0.90 ng/ml (day 5) and 2.34 ± 1.06 ng/ml (day 8), ginkgolide C between 0.75 ± 0.08–0.13 ng/ml (days 8 and 7) and 0.76 ± 0.14 ng/ml (day 5), and bilobalide between 1.87 ± 1.25 ng/ml (day 7) and 1.92 ± 1.37 ng/ml (day 5), indicating that steady state was reached.
Evaluation of CYP activity
Based on data from all 18 participants, the geometric mean ratios for the CYP1A2, CYP2C9, and CYP3A metric were similar for all three treatments (Table 1), with 90% CIs for ratios of the respective metrics being within the predefined acceptance range (Table 2). Thus, EGb 761® showed neither inhibition nor induction of these enzymes.
For CYP2C19, the lower limit of the 90% CI for its OME-based metric ratio exceeded the predefined range (0.681 < 0.70, see Table 2) in the 120-mg b.i.d. group. In contrast, the 90% CI for the other dosing schedule of 240 mg EGb 761® q.d. was completely within the predefined limits. Geometric mean ratios of CYP2D6 for all three treatments were similar (Table 1) based on data from 14 of 18 participants (four were poor metabolizers). Although the point estimator (0.925) of the ratio for CYP2D6 in the 240-mg q.d. group was close to unity, the lower limit of the 90% CI exceeded the predefined range (0.667 < 0.70, see Table 2), whereas for the 120-mg EGb 761® b.i.d. group, the 90% CI for the ratios was within the limits.
Safety results
All 18 randomized participants received all three kinds of study medication and were included in the safety analysis set. Administration of EGb 761® 120 mg b.i.d. and EGb 761® 240 mg q.d. was well tolerated when given alone and together with the phenotyping cocktail. Overall, 19 adverse events (AE) occurred during the study, out of which 11 were considered as unlikely to be related to study medication, with headache being the most frequent event, for which a causal drug relationship could not be excluded. Laboratory tests, 12-lead ECGs, physical examinations, and vital signs did not evince any risk of EGb 761® in any of the three treatment groups.
Discussion
The aim of the study was to evaluate a possible effect of EGb 761® intake on the activity of five major human CYP enzymes using the cocktail-phenotyping approach. We provide evidence that EGb 761® has no clinically relevant inhibitory or inducing effects toward the major human CYP enzymes when administered at chronic therapeutic doses in vivo. Phenotyping for drug-metabolizing enzymes is defined as measuring its actual in vivo activity in an individual and is performed by administering a selective substrate for this enzyme and subsequently determining appropriate pharmacokinetic parameters closely reflecting enzyme activity [28]. Drugs within a cocktail should not interfere with metabolism of other drugs in the cocktail [29]. Usually, a crossover design is used, with administration of the respective phenotyping agents in both periods, combined with coadministration of the drug to be tested on one period [28].
This study was designed to combine a state-of-the-art drug–drug-interaction cocktail [28, 30] with a minimal sampling strategy. Based on estimation of the samples size required, the number of participants was essentially sufficient, although intraindividual variability was higher than expected (Table 2). As far as is known, the substrates are specific for individual CYPs, there are no interactions between these substrates, and the probe drugs in the coctail are among those that may be considered as best validated [31–34]. Exposure to EGb 761® has been monitored, and steady-state conditions with regard to plasma concentrations of the four terpene lactones were achieved. A maximum exposure was realized with a 240-mg EGb 761® daily dose, and exposure duration was sufficient to eventually induce CYPs, as steady state for EGb 761® components was reached, and 1 week is typically sufficient to achieve full induction [35]. As to whether phenotyping metrics used were optimal, the most recent European Medicines Agency draft guidelines on the investigation of drug interactions (CPMP/EWP/560/95/Rev. 1 – Corr.), published after completion of this study, asks for determination of complete area under the concentration-time-curve (AUC) values of phenotyping substrates and discourages the use of single concentrations and metabolic ratios. For simplicity, however, it is desirable to use metrics that need single samples [28], as done in our study. For either approach, it is decisive to what extent the metric indeed reflects enzyme activity. The metrics used for CYP1A2 and CYP2C9 may be considered as fully validated [28]. For CYP2C19, based on OME hydroxylation; and for CYP2D6, based on DEX demethylation, validation of plasma clearance or AUC of the substrates is not superior to single-point measurements [28]. Single-point assessment for CYP3A based on MID hydroxylation is still considered appropriate [31, 32]. For CYPs1A2, 2C9, and 3A, 90% CIs were within the predefined acceptance range, indicating the absence of herbal drug–drug interactions. This holds true for both dosing schedules. For CYP2C19, the lower limit of the 90% CI for its metric ratio was outside the predefined range (Table 2) in the 120-mg group. Assuming this to be a real effect of EGb 761® on CYP2C19 activity would arouse suspicion that EGb 761® might induce CYP2C19 at the 120-mg b.i.d. dose only. Conspicuously, data of this study obviously demonstrate that EGb 761® is free on any inhibitory effect directed toward CYP2C19, because the upper limit of the 90% CI for its metric ratio is clearly positioned within the predefined range (for both dosing schedules). Some induction of OME metabolism by GBE was reported by Yin et al. [36]; as volunteers with genes coding for inactive CYP2C19 had the highest effect, this change cannot be explained by CYP2C19 induction [37]. A pharmacokinetic study in healthy volunteers conducted with diazepam as a substrate of CYP2C19 presented no herb–drug interaction between GBE and diazepam [26]. Also, another clinical study examined the possible effects of Ginkgo biloba on single-dose pharmacokinetics of voriconazole in healthy volunteers. There was also no evidence of induction of CYP2C19 activity because of Ginkgo biloba treatment [38]. The study reported here suggests that the observed variability is the main reason for the lower CI range being outside the predefined limits, as the intraindividual CV of the CYP2C19 metric was the second highest of all CYPs considered (45.4%, Table 2). This is supported by the fact that the inability to formally exclude an interaction was observed for only one of the two dosing schedules. As a consequence, we concluded that there is no clinical relevance of CYP2C19-related findings of the cocktail study under consideration. A daily dose of 120 mg EGb 761® b.i.d. does not affect CYP2C19 activity when administered over an 8-day period.
Similar considerations also apply for CYP2D6, where the lower limit of the 90% CI for its metric ratio exceeded the predefined range (Table 2), in this case only for the 240-mg q.d. group. Assuming this to be a real effect of EGb 761® would arouse suspicion that EGb 761® might affect CYP2D6 activity in the direction of induction, whereas there is clearly no inhibitory effect directed toward CYPD6. Again, most probably, the variability observed is of key relevance for the inability to formally reject the possibility of an interaction, as the intraindividual CV of the CYP2D6 metric was the highest of all the CYPs considered (51.9%, Table 2). Published data regarding a potential induction of CYP2D6 by GBE has not been found. In principle, CYP2D6 is not inducible in humans [39, 40]. A previous clinical study of 12 healthy volunteers assessed the influence of EGb 761® on CYP2D6 and 3A activity. For probe substrates DEX (CYP2D6 activity) and alprazolam (CYP3A activity), no statistically significant differences were observed between baseline and post-GBE treatment, indicating a lack of effect on CYP2D6 and CYP3A [25]. Taking these findings together, we conclude that there is no clinical relevance of CYP2D6-related findings of the drug-cocktail study under consideration.
In general, in vitro and in vivo studies produced conflicting results [10–17]. In vitro studies with human enzymes showed that Ginkgo biloba may inhibit CYPs [18–21]. Such inhibition has been associated with ginkgolic acids [20]. Variability in ginkgolic acid content of tested extracts might therefore explain some of the observed variabilities. EGb 761® contains <5 ppm ginkgolic acids. Taking all these contradictory data into account, however, in humans, we could not confirm any of these findings for the effect of EGb 761® on CYP activity following chronic administration, whereas results of the study reported are in accordance with published data from clinical studies assessed in human participants with this, and other, Ginkgo biloba preparation [23–26].
In summary, our data indicate that there is no inhibitory effect of EGb 761® on any of the five human CYPs. Furthermore, our results suggest that EGb 761® does not induce CYP1A2, 2C9, and 3A activity. For the noninducible CYP2D6, 90% CIs exceeding the acceptance range for one dosing schedule is meaningless. For CYP2C19, 90% CIs exceeding the acceptance range toward an induction effect was not attended by corresponding results of clinical drug–drug-interaction studies. Thus, from a clinical point of view, a relevant effect on activity of the CYPs tested could be ruled out for both treatment regimens. Our results eliminate the need for further in vitro or in vivo evaluation of particular CYP-related drug–drug interaction studies with EGb 761®.
Notes
EGb 761® is the active substance of Tebonin® (Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany)
References
Diamond BJ, Shiflett SC, Feiwel N, Matheis RJ, Noskin O, Richards JA, Schoenberger NE (2000) Ginkgo biloba extract: mechanisms and clinical indications. Arch Phys Med Rehabil 81(5):668–678
Abdel-Kader R, Hauptmann S, Keil U, Scherping I, Leuner K, Eckert A, Muller WE (2007) Stabilization of mitochondrial function by Ginkgo biloba extract (EGb 761). Pharmacol Res 56(6):493–502. doi:10.1016/j.ph.2007.09.011
Tchantchou F, Xu Y, Wu Y, Christen Y, Luo Y (2007) EGb 761 enhances adult hippocampal neurogenesis and phosphorylation of CREB in transgenic mouse model of Alzheimer's disease. Faseb J 21(10):2400–2408. doi:10.1096/fj.06-7649com
Tchantchou F, Lacor PN, Cao Z, Lao L, Hou Y, Cui C, Klein WL, Luo Y (2009) Stimulation of neurogenesis and synaptogenesis by bilobalide and quercetin via common final pathway in hippocampal neurons. J Alzheimers Dis 18(4):787–798. doi:10.3233/JAD-2009-1189
Elovic EP, Zafonte RD (2001) Ginkgo biloba: applications in traumatic brain injury. J Head Trauma Rehabil 16(6):603–607
Cohen-Salmon C, Venault P, Martin B, Raffalli-Sebille MJ, Barkats M, Clostre F, Pardon MC, Christen Y, Chapouthier G (1997) Effects of Ginkgo biloba extract (EGb 761) on learning and possible actions on aging. J Physiol Paris 91(6):291–300
Thiagarajan G, Chandani S, Harinarayana Rao S, Samuni AM, Chandrasekaran K, Balasubramanian D (2002) Molecular and cellular assessment of ginkgo biloba extract as a possible ophthalmic drug. Exp Eye Res 75(4):421–430
Rioufol G, Pietri S, Culcasi M, Loufoua J, Staat P, Pop C, Drieu K, Ovize M (2003) Ginkgo biloba extract EGb 761 attenuates myocardial stunning in the pig heart. Basic Res Cardiol 98(1):59–68. doi:10.1007/s00395-003-0380-4
DeFeudis FV (2003) A brief history of EGb 761 and its therapeutic uses. Pharmacopsychiatry 36(Suppl 1):S2–S7. doi:10.1055/s-2003-40450
Sugiyama T, Shinozuka K, Sano A, Yamada S, Endoh K, Yamada K, Umegaki K (2004) Effects of various ginkgo biloba extracts and proanthocyanidin on hepatic cytochrome P450 activity in rats. Shokuhin Eiseigaku Zasshi 45(6):295–301
Umegaki K, Saito K, Kubota Y, Sanada H, Yamada K, Shinozuka K (2002) Ginkgo biloba extract markedly induces pentoxyresorufin O-dealkylase activity in rats. Jpn J Pharmacol 90(4):345–351
Sugiyama T, Kubota Y, Shinozuka K, Yamada S, Wu J, Umegaki K (2004) Ginkgo biloba extract modifies hypoglycemic action of tolbutamide via hepatic cytochrome P450 mediated mechanism in aged rats. Life Sci 75(9):1113–1122. doi:10.1016/j.lfs.2004.02.020
Yoshioka M, Ohnishi N, Sone N, Egami S, Takara K, Yokoyama T, Kuroda K (2004) Studies on interactions between functional foods or dietary supplements and medicines. III. Effects of ginkgo biloba leaf extract on the pharmacokinetics of nifedipine in rats. Biol Pharm Bull 27(12):2042–2045
Ohnishi N, Kusuhara M, Yoshioka M, Kuroda K, Soga A, Nishikawa F, Koishi T, Nakagawa M, Hori S, Matsumoto T, Yamashita M, Ohta S, Takara K, Yokoyama T (2003) Studies on interactions between functional foods or dietary supplements and medicines. I. Effects of Ginkgo biloba leaf extract on the pharmacokinetics of diltiazem in rats. Biol Pharm Bull 26(9):1315–1320
Yang XF, Wang NP, Lu WH, Zeng FD (2003) Effects of Ginkgo biloba extract and tanshinone on cytochrome P-450 isozymes and glutathione transferase in rats. Acta Pharmacol Sin 24(10):1033–1038
Sugiyama T, Kubota Y, Shinozuka K, Yamada S, Yamada K, Umegaki K (2004) Induction and recovery of hepatic drug metabolizing enzymes in rats treated with Ginkgo biloba extract. Food Chem Toxicol 42(6):953–957. doi:10.1016/j.fct.2004.02.007
Deng Y, Bi HC, Zhao LZ, He F, Liu YQ, Yu JJ, Ou ZM, Ding L, Chen X, Huang ZY, Huang M, Zhou SF (2008) Induction of cytochrome P450s by terpene trilactones and flavonoids of the Ginkgo biloba extract EGb 761 in rats. Xenobiotica 38(5):465–481. doi:10.1080/00498250701883233
von Moltke LL, Weemhoff JL, Bedir E, Khan IA, Harmatz JS, Goldman P, Greenblatt DJ (2004) Inhibition of human cytochromes P450 by components of Ginkgo biloba. J Pharm Pharmacol 56(8):1039–1044. doi:10.1211/0022357044021
Yale SH, Glurich I (2005) Analysis of the inhibitory potential of Ginkgo biloba, Echinacea purpurea, and Serenoa repens on the metabolic activity of cytochrome P450 3A4, 2D6, and 2 C9. J Altern Complement Med 11(3):433–439. doi:10.1089/acm.2005.11.433
Zou L, Harkey MR, Henderson GL (2002) Effects of herbal components on cDNA-expressed cytochrome P450 enzyme catalytic activity. Life Sci 71(13):1579–1589
Gaudineau C, Beckerman R, Welbourn S, Auclair K (2004) Inhibition of human P450 enzymes by multiple constituents of the Ginkgo biloba extract. Biochem Biophys Res Commun 318(4):1072–1078. doi:10.1016/j.bbrc.2004.04.139
Chatterjee SS, Doelman CJ, Noldner M, Biber A, Koch E (2005) Influence of the Ginkgo extract EGb 761 on rat liver cytochrome P450 and steroid metabolism and excretion in rats and man. J Pharm Pharmacol 57(5):641–650. doi:10.1211/0022357056046
Duche JC, Barre J, Guinot P, Duchier J, Cournot A, Tillement JP (1989) Effect of Ginkgo biloba extract on microsomal enzyme induction. Int J Clin Pharmacol Res 9(3):165–168
Gurley BJ, Gardner SF, Hubbard MA, Williams DK, Gentry WB, Cui Y, Ang CY (2002) Cytochrome P450 phenotypic ratios for predicting herb-drug interactions in humans. Clin Pharmacol Ther 72(3):276–287. doi:10.1067/mcp.2002.126913
Markowitz JS, Donovan JL, Lindsay DeVane C, Sipkes L, Chavin KD (2003) Multiple-dose administration of Ginkgo biloba did not affect cytochrome P-450 2D6 or 3A4 activity in normal volunteers. J Clin Psychopharmacol 23(6):576–581. doi:10.1097/01.jcp.0000095340.32154.c6
Zuo XC, Zhang BK, Jia SJ, Liu SK, Zhou LY, Li J, Zhang J, Dai LL, Chen BM, Yang GP, Yuan H (2010) Effects of Ginkgo biloba extracts on diazepam metabolism: a pharmacokinetic study in healthy Chinese male subjects. Eur J Clin Pharmacol 66(5):503–509. doi:10.1007/s00228-010-0795-4
Izzo AA, Ernst E (2009) Interactions between herbal medicines and prescribed drugs: an updated systematic review. Drugs 69(13):1777–1798. doi:10.2165/11317010-000000000-00000
Fuhr U, Jetter A, Kirchheiner J (2007) Appropriate phenotyping procedures for drug metabolizing enzymes and transporters in humans and their simultaneous use in the "cocktail" approach. Clin Pharmacol Ther 81(2):270–283. doi:10.1038/sj.clpt.6100050
Turpault S, Brian W, Van Horn R, Santoni A, Poitiers F, Donazzolo Y, Boulenc X (2009) Pharmacokinetic assessment of a five-probe cocktail for CYPs 1A2, 2 C9, 2 C19, 2D6 and 3A. Br J Clin Pharmacol 68(6):928–935. doi:10.1111/j.1365-2125.2009.03548.x
Tucker GT, Houston JB, Huang SM (2001) Optimizing drug development: strategies to assess drug metabolism/transporter interaction potential–towards a consensus. Br J Clin Pharmacol 52(1):107–117
Fuhr U, Rost KL, Engelhardt R, Sachs M, Liermann D, Belloc C, Beaune P, Janezic S, Grant D, Meyer UA, Staib AH (1996) Evaluation of caffeine as a test drug for CYP1A2, NAT2 and CYP2E1 phenotyping in man by in vivo versus in vitro correlations. Pharmacogenetics 6(2):159–176
Jetter A, Kinzig-Schippers M, Skott A, Lazar A, Tomalik-Scharte D, Kirchheiner J, Walchner-Bonjean M, Hering U, Jakob V, Rodamer M, Jabrane W, Kasel D, Brockmoller J, Fuhr U, Sorgel F (2004) Cytochrome P450 2C9 phenotyping using low-dose tolbutamide. Eur J Clin Pharmacol 60(3):165–171. doi:10.1007/s00228-004-0754-z
Frank D, Jaehde U, Fuhr U (2007) Evaluation of probe drugs and pharmacokinetic metrics for CYP2D6 phenotyping. Eur J Clin Pharmacol 63(4):321–333. doi:10.1007/s00228-006-0250-8
Chaobal HN, Kharasch ED (2005) Single-point sampling for assessment of constitutive, induced, and inhibited cytochrome P450 3A activity with alfentanil or midazolam. Clin Pharmacol Ther 78(5):529–539. doi:10.1016/j.clpt.2005.08.004
Yang J, Liao M, Shou M, Jamei M, Yeo KR, Tucker GT, Rostami-Hodjegan A (2008) Cytochrome p450 turnover: regulation of synthesis and degradation, methods for determining rates, and implications for the prediction of drug interactions. Curr Drug Metab 9(5):384–394
Yin OQ, Tomlinson B, Waye MM, Chow AH, Chow MS (2004) Pharmacogenetics and herb-drug interactions: experience with Ginkgo biloba and omeprazole. Pharmacogenetics 14(12):841–850
Zhou HH, Anthony LB, Wood AJ, Wilkinson GR (1990) Induction of polymorphic 4′-hydroxylation of S-mephenytoin by rifampicin. Br J Clin Pharmacol 30(3):471–475
Lei HP, Wang G, Wang LS, Ou-yang DS, Chen H, Li Q, Zhang W, Tan ZR, Fan L, He YJ, Zhou HH (2009) Lack of effect of Ginkgo biloba on voriconazole pharmacokinetics in Chinese volunteers identified as CYP2C19 poor and extensive metabolizers. Ann Pharmacother 43(4):726–731. doi:10.1345/aph.1L537
Eichelbaum M, Mineshita S, Ohnhaus EE, Zekorn C (1986) The influence of enzyme induction on polymorphic sparteine oxidation. Br J Clin Pharmacol 22(1):49–53
Schellens JH, van der Wart JH, Brugman M, Breimer DD (1989) Influence of enzyme induction and inhibition on the oxidation of nifedipine, sparteine, mephenytoin and antipyrine in humans as assessed by a “cocktail” study design. J Pharmacol Exp Ther 249(2):638–645
Acknowledgements
In adherence to the guidelines of the International Committee of Medical Journal Editors, it is declared that this study is work for hire supported by Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany (sponsor). SK, AD, and RH are employees of Dr. Willmar Schwabe GmbH & Co. KG, and TG received honoraria from Schwabe. No further conflict of interest is declared.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Zadoyan, G., Rokitta, D., Klement, S. et al. Effect of Ginkgo biloba special extract EGb 761® on human cytochrome P450 activity: a cocktail interaction study in healthy volunteers. Eur J Clin Pharmacol 68, 553–560 (2012). https://doi.org/10.1007/s00228-011-1174-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-011-1174-5