
Abstract
Summary
This study explored the distribution of vertebral fractures in hip fracture patients. Unlike patients with intertrochanteric fractures, those with subcapital fractures were less likely to have vertebral fractures in the T4-T10 region of the spine. The dissimilar distribution of vertebral fractures among patients with intertrochanteric and subcapital fractures may indicate different underlying etiologies.
Introduction
There are two main types of hip fractures: intertrochanteric and subcapital. Both types can have associated vertebral fractures. In this study, we explored the distribution of vertebral fractures in the two hip fracture populations.
Methods
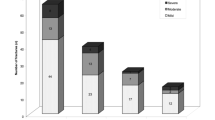
This was a retrospective analysis of a convenience sample of 120 patients: 40 with subcapital fractures and vertebral fractures, 40 with intertrochanteric fractures and vertebral fractures, and 40 with vertebral fractures only. Based on Genant’s semiquantitative assessment method of radiographic images, the distribution and severity of each patient’s vertebral fractures were explored [1].
Results
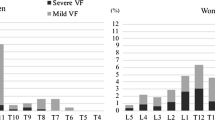
Patients with subcapital fractures had significantly fewer total vertebral fractures (93 vs. 144, p = 0.005; 93 vs. 127, p = 0.019), vertebral fractures from T4 to T10 (41 vs. 81, p = 0.005; 41 vs. 64, p = 0.042), and vertebral fractures at the T7-T8 peak (11 vs. 31, p = 0.002; 11 vs. 30, p = 0.003) than patients with intertrochanteric fractures and those with vertebral fractures alone, respectively, and they were more likely to have only one vertebral fracture (15 vs. 3, p < 0.001; 15 vs. 2, p < 0.001). The number of vertebral fractures from T11 to L4 and at the T12-L1 peak did not differ among the groups. The numbers of fractures at each vertebral level was significantly correlated only between those with intertrochanteric fractures and those with vertebral fractures alone (r = 0.65, p = 0.009).
Conclusion
The distribution of vertebral fractures among patients with subcapital fractures differed from the other fracture groups, which may indicate that subcapital fractures and some lumbar fractures have a different underlying etiology than intertrochanteric fractures and thoracic (T4-T10) fractures.

Similar content being viewed by others

References
Genant HK, Jergas M, Palermo L, Nevitt M, Valentin RS, Black D, Cummings SR (1996) Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis. J Bone Miner Res 11:984–96
Siris ES, Chen Y, Abbott TA, Barrett-Connor E, Miller PD, Wehren LE, Berger ML (2004) Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch Intern Med 164:1108–12
Cooper C, Atkinson EJ, O’Fallon WM, Melton LJ (1992) Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985–1989. J Bone Miner Res 7:221–7
Nevitt MC, Ross PD, Palermo L, Musliner T, Genant HK, Thompson DE (1999) Association of prevalent vertebral fractures, bone density, and alendronate treatment with incident vertebral fractures: effect of number and spinal location of fractures. Bone 25:613–9
Waterloo S, Ahmed LA, Center JR, Eisman JA, Morseth B, Nguyen ND, Nguyen T, Sogaard AJ, Emaus N (2012) Prevalence of vertebral fractures in women and men in the population-based Tromso Study. BMC Musculoskelet Disord 13:3–11
Fox KM, Cummings SR, Williams E, Stone K (2000) Femoral neck and intertrochanteric fractures have different risk factors: a prospective study. Osteoporos Int 11:1018–23
Partanen J, Jamsa T, Jalovaara P (2001) Influence of the upper femur and pelvic geometry on the risk and type of hip fractures. J Bone Miner Res 16:1540–6
Gonnelli S, Caffarelli C, Maggi S, Rossi S, Siviero P, Gandolini G, Cisari C, Rossini M, Iolascon G, Letizia Mauro G, Crepaldi G, Nuti R (2013) The assessment of vertebral fractures in elderly women with recent hip fractures: the BREAK Study. Osteoporos Int 24:1151–9
Greenspan SL, Myers ER, Maitland LA, Kido TH, Krasnow MB, Hayes WC (1994) Trochanteric bone mineral density is associated with type of hip fracture in the elderly. J Bone Miner Res 9:1889–94
Szulc P, Duboeuf F, Schott AM, Dargent-Molina P, Meunier PJ, Delmas PD (2006) Structural determinants of hip fracture in elderly women: a re-analysis of the data from the EPIDOS study. Osteoporos Int 17:231–6
Gallagher JC, Melton LJ, Riggs BL, Bergstrath E (1980) Epidemiology of fractures of the proximal femur in Rochester, Minnesota. Clin Orthop Relat Res 150:163–71
Lips P, Taconis WK, Van Ginkel FC, Netelenbos JC (1984) Radiologic morphometry in patients with femoral neck fractures and elderly control subjects: comparison with histomorphometric parameters. Clin Orthop 183:64–9
Vega E, Mautalen C, Gomez H, Garrido A, Melo L, Sahores AO (1991) Bone mineral density in patients with cervical and trochanteric fractures of the proximal femur. Osteoporos Int 1:81–6
Pulkkinen P, Gluer CC, Jamsa T (2011) Investigation of differences between hip fracture types: a worthy strategy for improved risk assessment and fracture prevention. Bone 49:600–4
Nakamura N, Kyou T, Takaoka K, Ohzono K, Ono K (1992) Bone mineral density in the proximal femur and hip fracture type in the elderly. J Bone Miner Res 7:755–9
Crilly RG, Cox L (2013) A comparison of bone density and bone morphology between patients presenting with hip fractures, spinal fractures or a combination of the two. BMC Musculoskelet Disord 14:68–76
Riggs BL, Wahner HW, Seeman E, Offord KP, Dunn WL, Mazess RB, Johnson KA, Melton LJ (1982) Changes in bone mineral density of the proximal femur and spine with aging: differnces between the postmenopausal and senile osteoporosis syndromes. J Clin Investig 70:716–23
Eastell R, Mosekile L, Hodgson SF, Riggs BL (1990) Proportion of human vertebral body bone that is cancellous. J Bone Miner Res 5:1237–41
Lotz JC, Hayes WC (1990) Estimates of hip fracture risk from falls using quantative computed tomography. J Bone Joint Surg 72:689–700
Cummings SR, Nevitt MC, for the Study of Osteoporotic Fractures Research Group (1994) Non-skeletal determinants of fractures: the potential importance of the mechanics of fall. Osteoporos Int 4:83–91
Hayes WC, Myers ER, Morris JN, Gerhart TN, Yett HS, Lipsitz LA (1993) Impact near the hip dominates fracture risk in elderly nursing home residents who fall. Calcif Tissue Int 52:192–8
Tanner DA, Kloseck M, Crilly RG, Chesworth B, Gilliland J (2010) Hip fracture types in men and women change differently with age. BMC Geriatr 10:12–15
Melton LJI, Chao EYS, Lane J (1988) Biomechanical aspects of fractures. In: Riggs BL, Melton LJI (eds) Osteoporosis: Etiology, Diagnosis and Management. Raven Press, New York, pp 111–131
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Watt, J., Cox, L. & Crilly, R.G. Distribution of vertebral fractures varies among patients according to hip fracture type. Osteoporos Int 26, 885–890 (2015). https://doi.org/10.1007/s00198-014-2887-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-014-2887-y