
Abstract
Using a local randomized experiment that arises from the statutory retirement age in Norway, we study the effect of retirement on health across gender and socioeconomic status. We apply data from administrative registers covering the entire population and from survey data of a random sample to investigate the effects of retirement on acute hospital admissions, mortality, and a composite physical health score. Our results show that retirement has a positive effect on physical health, especially for individuals with low socioeconomic status. We find no effects of retirement on acute hospitalizations or mortality in general. However, our results suggest that retirement leads to reduced likelihood of hospitalizations for individuals with low socioeconomic status. Finally, we show that the positive health effects are driven by reduced pain and reduced health limitations in conducting daily activities. Our findings highlight heterogeneity in the health effects across socioeconomic status and across subjective and objective measures of health.

The graphs show the fraction retired by age from the two datasets. The upper graphs are based on the survey data, whereas the two lower graphs are based on administrative data. All graphs depict the fraction retired across the age span of 55–79. The x-axis on the left two graphs depicts age in years, whereas the x-axis in the graphs to the right depicts age in months, relative to the retirement eligibility age in months (805 months)

The graphs present the age-health relationship for physical health, acute hospital admissions, and mortality. The scale for physical health is a point on the SF-12 scale, and the scale for acute hospital admissions and mortality corresponds to the incidence in the population. The x-axis displays age in months relative to the retirement age threshold of 805 months
Similar content being viewed by others


Notes
Early retirement in Norway was introduced at age 65, but later reduced in a stepwise matter to age 62. The authors exploit this stepwise reduction as a source of exogenous variation.
The pension system was reformed in 2011, but none of the new rules were in place throughout our study-period.
One basic amount is the lowest earnings required to accrue pension points.
This was lifted in 2008 for 67-year olds.
DI provides another important channel out of the labor force. However, being granted DI is fundamentally different from retiring, as DI typically follows from a long period of sickness absence and must be certified by a physician and is granted through a thorough process.
The difference between sharp and fuzzy RD is parallel to the difference between a randomized experiment with perfect compliance and a randomized experiment with imperfect compliance, when only the intention to treat is randomized.
Dong (2015) shows that using RD design calls for careful consideration of the unit of measurement when age is the forcing variable, as age in years, as opposed to age in months, might lead to inconsistent results.
The optimal bandwidth suggested by Imbens and Kalyanaraman (2012) varies by SES group. The suggested bandwidth is in the range of 8–12 months for all the groups. For simplicity, we apply a bandwidth of 10 months in all estimations. Choosing different bandwidths within this interval has little influence on the estimated effects. See the robustness checks in the Appendix for more on the sensitivity of the results with respect to the choice of bandwidth.
Due to the small sample size left in the survey data when we apply the 10 months bandwidths, we also ran the entire analysis using a bandwidth of 20 months. This does not change the results from the survey data in any substantial way.
See Slagsvold et al. (2012) for a thorough description.
The reason that the NorLAG survey responses cannot be connected to the administrative health registers applied in this study is that the NorLAG data were anonymized after they were connected to the registers.
The first wave contains 5559 observations (response rate 67%), whereas the second wave contains 15,149 observations (response rate 60%).
All SF-12 components are outlined in Section 5.2.2.
Coded according to NACE Rev.1.1
All admissions are coded in accordance with the International Statistical Classification of Diseases and Related Health Problems, ICD-10 (WHO 1992)).
This is the earliest year in which data on hospitalizations are available.
The results from the sensitivity analysis are shown in the Appendix.
This is also true for the NorLAG data, but the differences in educational attainment is statistically significant in the administrative data due to a large number of observations.
In the graphs, retirement refers only to those who have actually retired, either through the early pension program or at the retirement age of 67. This means that individuals on DI are not considered retired. If we remove all individuals that are currently on DI or who were on DI before they retired, from our sample, the picture looks the same.
Translated from Norwegian by the authors.
A medical certificate is required for spells of absence of more than 3 days or 8 days, depending on whether the employer has signed the “IA-agreement” or not.
See Jürges (2007) for a more general discussion of subjective versus objective measures of health.
References
Angrist JD, Pischke J-S (2010) The credibility revolution in empirical economics: how better research design is taking the con out of econometrics. J Econ Perspect 24 (2):3–30
Behncke S (2012) Does retirement trigger ill health? Health Econ 21(3):282–300
Blake H, Garrouste C (2013) Killing me softly: work and mortality among French seniors. Technical report HEDG, Department of Economics, University of York
Bloemen H, Hochguertel S, Zweerink J (2017) The causal effect of retirement on mortality: evidence from targeted incentives to retire early. Health Econ 26(12):204–218
Bound J, Waidmann T (2007) Estimating the health effects of retirement. Michigan Retirement Research Center Research Paper No. UM WP 2007-168
Brazier JE, Roberts J (2004) The estimation of a preference-based measure of health from the SF-12. Med Care 42(9):851–859
Case A, Deaton AS (2005) Broken down by work and sex: how our health declines. In: Analyses in the Economics of Aging. University of Chicago Press, pp 185–212
Cattaneo MD, Jansson M, Ma X (2016) Simple local regression distribution estimators with an application to manipulation testing. Unpublished Working Paper, University of Michigan, and University of California Berkeley
Coe NB, Zamarro G (2011) Retirement effects on health in Europe. J Health Econ 30(1):77–86
Dong Y (2015) Regression discontinuity applications with rounding errors in the running variable. J Appl Econom 30(3):422–446
Eibich P (2015) Understanding the effect of retirement on health: mechanisms and heterogeneity. J Health Econ 43:1–12
Godard M (2016) Gaining weight through retirement? Results from the SHARE survey. J Health Econ 45:27–46
Grossman M (1972) On the concept of health capital and the demand for health. J Polit Econ 80(2):223–255
Hahn J, Todd P, Van der Klaauw W (2001) Identification and estimation of treatment effects with a regression-discontinuity design. Econometrica 69(1):201–209
Hallberg D, Johansson P, Josephson M (2015) Is an early retirement offer good for your health? Quasi-experimental evidence from the army. J Health Econ 44:274–285
Heller-Sahlgren G (2017) Retirement blues. J Health Econ 54:66–78
Hernæs E, Markussen S, Piggott J, Vestad OL (2013) Does retirement age impact mortality? J Health Econ 32(3):586–598
Imbens GW, Lemieux T (2008) Regression discontinuity designs: a guide to practice. J Econ 142(2):615–635
Imbens G, Kalyanaraman K (2012) Optimal bandwidth choice for the regression discontinuity estimator. Rev Econ Stud 79(3):933–959
Insler M (2014) The health consequences of retirement. J Hum Resour 49 (1):195–233
Jenkinson C, Layte R (1997) Development and testing of the UK SF-12. J Health Serv Res 2(1):14–18
Jürges H (2007) True health vs response styles: exploring cross-country differences in self-reported health. Health Econ 16(2):163–178
Kudrna G (2017) The Norwegian pension reform: an external perspective. CEPAR Working Paper 2017/07, CEPAR
Kuhn A, Wuellrich J-P, Zweimüller J (2010) Fatal attraction? Access to early retirement and mortality. IZA discussion paper No. 5160
Lee DS, Card D (2008) Regression discontinuity inference with specification error. J Econ 142(2):655–674
Lee DS, Lemieux T (2010) Regression discontinuity designs in economics. J Econ Lit 48(2):281–355
Mazzonna F, Peracchi F (2012) Ageing, cognitive abilities and retirement. Eur Econ Rev 56(4):691–710
Mazzonna F, Peracchi F (2017) Unhealthy retirement? J Hum Resour 52 (1):128–151
McGarry K (2004) Health and retirement do changes in health affect retirement expectations? J Hum Resour 39(3):624–648
Neuman K (2008) Quit your job and get healthier? The effect of retirement on health. J Labor Res 29(2):177–201
Røed K, Haugen F (2003) Early retirement and economic incentives: evidence from a quasi-natural experiment. Labour 17(2):203–228
Rohwedder S, Willis RJ (2010) Mental retirement. J Econ Perspect 24 (1):119–138
Slagsvold B, Veenstra M, Daatland SO, Hagestad G, Hansen T, Herlofson K, Koløen K, Solem PE (2012) Life-course, ageing and generations in Norway: The NorLAG study. Norsk Epidemiol 22(2)
Ware JE Jr, Kosinski M, Keller SD (1996) A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care 34(3):220–233
WHO (1992) The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. World Health Organization, Geneva
Acknowledgments
We would like to thank Arild Aakvik, Ragnhild Balsvik, Dorly Deeg, Elisabeth Fevang, Astrid Grasdal, Thomas Hansen, Thomas Hofmarcher, Christian Monden, Matthew Neidell, Viggo Nordvik, Miikka Rokkinen, Ingrid Hoem Sjursen, Eirik Strø mland, Kristin Årland, and seminar participants at Columbia University, Norwegian Social Research, 23rd Nordic Congress of Gerontology, Norwegian School of Economics, University of Bergen, The Frisch Centre, and three anonymous referees for helpful comments and suggestions.
Funding
This study was funded by The Research Council of Norway (NFR), grant number 237011 and grant number 50813, and NordForsk, grant number 74637.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors declare that they have no conflict of interest
Additional information
Responsible editor: Alessandro Cigno
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix - Sensitivity and Robustness
Appendix - Sensitivity and Robustness
1.1 A.1 Disabled individuals: past labor income and self-reported work status
People on DI are mechanically transferred from disability pension to retirement pension at age 805 months. We need to make sure that the positive physical health effects found in the main analysis are not driven by these individuals. Initially, there is no reason to believe that there should be a health effect for people on DI, as they were not working before retirement, and should therefore have no change in circumstances. However, as the physical health measure contains elements of self-assessed health, it is possible that someone who is disabled may need to justify their disability status, consciously or subconsciously, by under-reporting health. In this case, health prior to retirement may be under-reported. Post retirement, when they are no longer in a situation where poor health is defining their labor market status, they might feel healthier, or they no longer have the need to report poor health. Provided this is a plausible scenario; We need to rule out that the results found in Section 5 are driven by justification bias.
The first two rows of Table 8 displays the results on two sub-samples of the survey data (labeled “Working” and “Income”), each aimed at running the analysis only on the sub-sample that was recorded as working until the statutory retirement age. The working sub-samples are defined in Section 4.2. Finding coefficients of the same sign and magnitude, especially for the rule based on self-assessed work status, ensures us that these effects are not driven by the disability justification hypothesis. The estimations based on the income-rule yields large and insignificant coefficients, both a consequence of the small sample sizes. Yet, the direction of the effects is similar to what was found in the main analysis.
For the outcomes from the administrative data, we should expect that individuals who retire formally at 67 but without any actual change in circumstances should water down the effects, as the health measures from this data source are not subject justification bias. We can therefore expect that this assessment can uncover significant effect, not detected in the gross sample. The first rows of Tables 9 and 10 present the estimations restricted to “workers” for acute hospitalizations and mortality, respectively. Here, we find no significant results for any of the sub-groups. The significant result on hospitalizations found for men with low education in the main analysis is no longer present.
1.2 A.2 Robustness checks and validity of the regression discontinuity design
Below we assess the sensitivity of the results for different bandwidth selections; we check for discontinuities in the forcing variable, age, at the cutoff; we test for discontinuities in other outcomes that should not have been affected by the threshold; and, we check for discontinuities in the outcomes of interest at points in the age distribution where there should be no discontinuities. This robustness assessment follows the suggestions in Imbens and Lemieux (2008) closely.
1.3 A.2.1 Bandwidth selection
The worry in an RD application is that using a bandwidth that is too wide, allows for other things than the intervention of interest to drive differences in outcomes for those right above compared to those right below the threshold. In Table 8 we display the results using bandwidths of 7 and 15 months for physical health. Using a bandwidth of 7 months does not alter the results, whereas increasing the bandwidths to 15 months somewhat reduces the effects. This is not surprising given the downward slope of the health trajectory across age and the upward shift in this trajectory at the retirement eligibility threshold.
The results for hospitalizations and mortality are displayed in Tables 9 and 10. For acute hospital admissions, we find that increasing the bandwidth to 15 months yields significant, negative effects. The effects are still small ranging from 0.7 to 1 percentage points. As the incidence is 14%, this entails a 5–7% reduction in the likelihood of acute hospitalization. Increasing the bandwidth increases the likelihood of factors, other than retirement, affecting acute hospital admissions. Another explanation can be that it takes some time for retirement to take effect on health issues such as stroke and acute heart conditions, thus including more post-retirement months increase the likelihood of finding significant effects. As in the main analysis, we find no effects of retirement on mortality at any of these bandwidths.

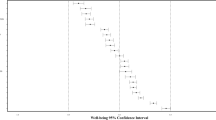
The graph displays point estimates and confidence intervals of the effect of retirement on physical health using different bandwidths. Bandwidth is measured as age in months from the retirement threshold
Graphical Display of Different Bandwidths
1.4 A.2.2 Continuity of the forcing variable
Vital to any RD application is the individual’s incapability of manipulating the forcing variable. In this case, the forcing variable is age (reported by public registers), which individuals cannot manipulate in any way. It could, however, be the case that retired individuals are more likely to respond to the survey due to the reduced opportunity cost of time. Figure 4 shows two histograms of age in months assessing potential bunching at the threshold. There is no evidence of any discontinuity in the forcing variable at the threshold. We also performed a more formal test proposed by Cattaneo et al. (2016). This implies testing the null of the continuous density of the forcing variable at the threshold using a local polynomial density estimator. The p-value under this test is 0.3251. For the population level data, this holds by construction, as people cannot manipulate their age and as all individuals in the population are represented in the data.

Note: The histograms show the distribution of age in months for the age range of 56-79 using the bin-width suggested by STATA (left histogram) and using one bin for each age in months (right histogram)
Discontinuity of the Forcing Variable
1.5 A.2.3 Placebo tests
The placebo tests entail testing for discontinuities in the three health outcomes at points in the age distribution where there should be no discontinuities. A common practice is to conduct placebo tests at the median age of the two sub-samples below and above the actual cut-off. In this case, the median age below the threshold is age 62. However, some individuals can retire at this age, thus making is an unsuited placebo threshold. Consequently, we use age 61 for the lower placebo. For the upper placebo, we use age 73. No discontinuities or significant effects were found at these placebo thresholds for physical health (Table 8). For acute hospital admissions (Table 9), we find significant effects for both the upper and lower placebo. For the lower placebo, this could be due to some occupations having special age-limits for retirement at 61. However, we find no explanations for why the upper placebo yields significant, and even positive effects. This finding reduces the credibility of the effects found in the main analysis for this outcome. The placebo results for mortality is presented in Table 10. There are no significant effects and the coefficients are close to zero for all sub-group at both placebo thresholds.
1.6 A.2.4 Discontinuity in Other Outcomes
Finally, we look for discontinuities in an outcome that should not be affected by retirement, at least not in the short-term. Here, we assess the likelihood of living with a partner or spouse (NorLAG) or being married (administrative data). The regression results shown in Tables 8 and 11 confirm that there are no retirement effect on these outcomes.
Rights and permissions
About this article

Cite this article
Grøtting, M.W., Lillebø, O.S. Health effects of retirement: evidence from survey and register data. J Popul Econ 33, 671–704 (2020). https://doi.org/10.1007/s00148-019-00742-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00148-019-00742-9