
Abstract
Rapid and accurate detection of respiratory syncytial virus (RSV) provides pathogen-specific diagnosis, allows implementation of appropriate infection control measures, and improves patient management. One diagnostic challenge is that respiratory infections, which can be caused by several viral pathogens including RSV, usually present with similar signs and symptoms that are nearly indistinguishable by clinical diagnosis. We have described in the chapter a rapid, high-throughput laboratory technique that can detect a panel of common viral pathogens in one single reaction. With the combination of target-enriched multiplexing PCR amplification and Luminex suspension array identification, 12 common respiratory viruses, including RSV A and B, influenza virus A and B, parainfluenza virus 1, 2, 3, and 4, human metapneumovirus, rhinoviruses, enteroviruses, and SARS coronavirus, are detected and differentiated simultaneously within five hours.
You have full access to this open access chapter, Download protocol PDF
Similar content being viewed by others

Key words
1 Introduction
1.1 Respiratory Syncytial Virus and Related Diseases
Respiratory syncytial virus (RSV) is known to be the leading cause of bronchiolitis and pneumonia in infants and young children (1, 2). Illness begins most frequently with rhinorrhea, sneezing, and cough. Most children experience recovery from illness after 8–15 days. During their first RSV infection, 25–40% of infected infants and young children have signs or symptoms of bronchiolitis or pneumonia, and 0.5–2% require hospitalization. There are high-risk groups prone to severe RSV disease that include premature infants, children with congenital heart and chronic lung diseases, and immunosuppressed patients or those with a congenital immunodeficiency, in which 25% require hospitalization (3–5). Infections with RSV of genotype A or B may result in differing clinical manifestations and outcomes (6, 7). RSV causes hazardous nosocomial infection and produces outbreaks each year with widespread infections in both children and adults, including medical personnel, who may have a mild enough illness that does not cause absences from work. Furthermore, the spread of the virus is facilitated by the number of young infants admitted during an outbreak who tend to shed high titers of virus for prolonged periods (8). Other viruses that can mimic RSV infection include adenoviruses, influenza virus (INF) A and B, parainfluenza viruses (PIV), human metapneumovirus (hMPV), and rhinoviruses. Patients with acute respiratory infections can present with similar signs and symptoms regardless of the viral pathogen, and clinical differential diagnosis of infections caused by these viruses can be difficult.
1.2 Conventional Laboratory Diagnostic Methods
Early and accurate virus-specific laboratory diagnosis significantly enhances patient management. There are currently a variety of laboratory tests available to detect and differentiate respiratory viruses, which have been developed over the last two decades. The use of rapid tests in the diagnosis of RSV infection allows implementation of appropriate infection control measures, thus reducing nosocomial spread (9) and may be useful for consideration of timely treatment with aerosolized ribavirin in severe cases. Direct fluorescent antibody (DFA) tests have good sensitivity for RSV, but are not as good for other respiratory viruses (10, 11). Rapid EIA antigen tests are available for RSV and Influenza A and B; they are easy to perform, and more rapid than DFA, but have slightly lower sensitivity and specificity (12, 13). Among the respiratory viruses mentioned previously, the vast majority will be grown in traditional viral culture cell lines used in clinical virology laboratories with the exception of hMPV, which is not yet widely used in routine diagnostic laboratories (14). Furthermore, cell culture has a slow turnaround time with most viruses showing no detectable cytopathic effects until 3 to 14 days later. However, a shell vial technique incorporated with mixed fresh cells (R-Mix, Diagnostic Hybrids, Inc., Athens, OH) can be performed which speeds up the turnaround time to 2 days and has a sensitivity similar to conventional cell culture (15). The diagnosis of RSV infections using serology has no practical applications in clinical use.
1.3 Molecular Assays for Detection of RSV
As is the case with other respiratory viral pathogens, molecular assays based on in vitro nucleic acid amplification have been implemented gradually in clinical laboratories for RSV detection. These molecular assays, led by PCR, in general, have demonstrated to be superior to routine diagnostic methods in terms of their high sensitivity and specificity (16–18), which are especially useful in adult patients when viral shedding is short and low (19, 20). While cell culture remains the gold standard for RSV diagnosis, the molecular assays have been considered the “platinum” standard to be used as the reference to validate new diagnostic kits for RSV detection (2, 12). However, these organism-specific monoplex assays are resource-intensive; when a respiratory viral infection is considered, the list of possible etiologies is necessarily long. Multiplex RT-PCR-based techniques have widely been reported for simultaneous detection of a panel of respiratory viral pathogens in a single reaction (21–25). Several products, including the Hexaplex assay (Prodesse, Waukesha, WI), the PLx-RVP assay (EraGen Biosciences, Madison, WI), the ID-Tag RVP (TM Biosciences, Toronto, Canada), and the ResPlex II (Qiagen, Valencia, CA), are commercially available (22, 26–30). This chapter describes a complete molecular diagnostic procedure covering common RNA viral pathogens causing respiratory tract infections.
1.4 Simultaneous Detection and Differentiation of 12 Respiratory Viruses Including RSV
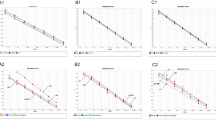
The following procedure consists of three components (Fig. 1). The first, specimen processing and nucleic acid extraction, is done by using an easyMAG automated total nucleic acid extraction instrument (bioMerieux, Durham, NC), based on a magnetic silica particle-based technique (31). The kits are available from bioMerieux and work on a variety of clinical specimens, including nasopharyngeal swabs and aspirates and yields high quantity and quality total nucleic acids (32). The second, nucleic acid amplification, uses a target-enriched multiplexing (TEM)-PCR (33), which contains two nested primer sets for each organism and a set of Super Primers, to simultaneously amplify INF-A, INF-B, PIV-1, PIV-2, PIV-3, PIV-4, RSV-A, RSV-B, hMPV, rhinoviruses (RhV), enteroviruses (EnV), and severe acute respiratory syndrome (SARS) coronavirus (CoV) gene in a single reaction tube (27, 29). The target gene from each of the viruses is listed in Table 1. The third, amplicon detection and identification, is reached by using a microsphere-based liquid array (Luminex, Austin, TX). A median fluorescence intensity (MFI) is reported for each target. A positivity cut-off is used to determine if the sample is positive for a particular target (34, 35). The last amplification and detection components are included in the ResPlex II kit, which is available from Qiagen.

A complete protocol simultaneously detects and differentiates a panel of respiratory RNA viruses. This contains nucleic acid extraction by easyMAG (bioMerieux), nucleic acid amplification by TEM-RT-PCR (Qiagen), and amplification product identification by a liquid chip system (Luminex). The left figure is an illustration of TEM-PCR amplification. (a) Nested gene-specific primers are designed to enrich the targets during initial PCR cycling. Later, universal SuperPrimers are used to amplify all targets. (b) Different primers are involved in the process at each of the three major stages, enrichment, tagging, and amplification. The solid lollipop indicates specific probes, covalently linked with luminex color-coated beads. The gray circles indicate biotin molecules. Modified from (33) with permission.
2 Materials
2.1 Special Instruments
-
1.
easyMAG automated extraction instrument (BioMerieux, Durham, NC).
-
2.
GeneAmp 9700 PCR System (Applied Biosystems) using 9600 emulation mode.
-
3.
LiquiChip 200 Workstation (Luminex, Austin, TX).
-
4.
Vortexer.
-
5.
Microcentrifuge with rotor for 1.5-mL microcentrifuge tubes.
-
6.
Heat Block or thermal cycler set at 52°C.
-
7.
Multichannel pipet.
-
8.
Positive displacement pipets.
2.2 Nucleic Acid Extraction
-
1.
easyMAG reagents – Buffers 1–4, Magnetic Silica (BioMerieux, Durham, NC).
-
2.
RNase-free water.
-
3.
1.5-mL nuclease-free microcentrifuge tubes and racks.
-
4.
Nuclease-free PCR tubes (thin-walled 0.2-mL PCR tubes).
-
5.
RNase-free pipette tips with hydrophobic filters.
2.3 TEM-PCR Amplification
-
1.
ResPlex II Kits (Qiagen).
-
2.
Nucleic acid decontaminating solutions or 10% bleach.
-
3.
RNase-free water.
-
4.
1.5-mL nuclease-free microcentrifuge tubes and racks.
-
5.
Foil to protect reagents from light.
-
6.
RNase-free pipette tips with hydrophobic filters.
2.4 Liquid Chip Detection
-
1.
96-well, flat-bottomed, microtiter plates with lids.
-
2.
1.5-mL nuclease-free microcentrifuge tubes and racks.
-
3.
Foil to protect reagents from light.
-
4.
RNase-free pipette tips with hydrophobic filters.
3 Methods
3.1 Nucleic Acid Extraction by EasyMAG
NOTE: Additional information can be obtained from the Generic Protocol provided with the easyMAG instrument.
NOTE: Samples for testing include nasopharyngeal aspirates, nasopharyngeal swabs, and other respiratory secretions and swabs.
-
1.
Press the Daily Use Icon.
-
2.
Begin the extraction request by entering the sample type. With each sample entry, confirm the type of sample. These should be set to “other” and “primary.”
-
3.
Define the sample volume and elution volume. For extraction on nasal collections, program a 0.2 mL sample volume with a 55 μL elution volume.
-
4.
Ensure the protocol is Generic.
-
5.
Press the enter button when finished.
-
6.
After all samples are entered, press the Organize Runs icon (opposing arrows).
-
7.
Create a new run by pressing the New Run icon (sun).
-
8.
Enter a run name, and then press OK.
-
9.
Create the run layout using the arrow icons to arrange the sample list in the correct order for your run.
-
10.
Press the Load Run (instrument with bottles) icon.
-
11.
Place the sample tray and pipette tips in the correct positions.
-
12.
Using the barcode scanner, scan in the position and the sample tray for each position.
-
13.
Press the Printer Icon to print the run. Press OK on the print window when it appears.
-
14.
Pull the sample tubes from the instrument and place them in the metal sample rack.
-
15.
Pipette 200 μL of sample into each sample tube. Use the printout as a guide.
-
16.
When finished, place the sample tray back into the instrument. The position and sample tray will have to be scanned into the instrument. Close the lid of the sample module.
-
17.
Press the Add Lysis icon. The lysis buffer will be added by the instrument and incubated for approximately 10 min.
-
18.
While the sample is lysing on the instrument, prepare the magnetic silica.
-
19.
Prepare the magnetic silica, using the multichannel pipette, choose program 1 (Press the Select button until P1 is displayed and then press Enter.). Place one 1-mL BioHit tip on the pipettor. The pipettor program is set up as:
-
Program 1
-
Fill 550 μL
-
Dispense 550 μL
-
-
-
20.
Pipette 550 μL of RNase-free water into a 1.5-mL tube.
-
21.
Vortex the silica well and pipette 550 μL of silica into the tube containing the water. Vortex this mixture well.
-
22.
Select an empty ELISA plate. Using the multichannel pipette, choose program 2 (Press the Select button until P2 is displayed, and then press Enter.). Place one 1-mL BioHit tip on the pipettor. The pipettor program 2 is set up as:
-
Program 2
-
Fill ≈1,000 μL
-
Dispense ≈100 μL back into source tube
-
Dispense 125 μL, ×8
-
Purge
-
-
-
23.
Aspirate volume and dispense the first “shot” back into the original tube.
-
24.
Pipette the subsequent eight dispenses into eight wells of the ELISA plate strip. Be sure to purge at the end of the pipetting step.
-
25.
When the lysing step has been completed, an alarm will sound. Open the lid of the sample module. Using multichannel pipettor program 3, place eight 1 mL BioHit tips on the pipettor (Press the Select button until P3 is displayed, then press Enter.). Pipettor program 3 is set up as:
-
Program 3
-
Fill and mix 100 μL
-
Fill and mix, ×4 (800 μL, 900 μL, then three, 1,000 μL mixes)
-
-
-
26.
Beginning with the ELISA plate, aspirate all eight wells on the ELISA plate.
-
27.
Place the tips into the sample tube tray just about where the tubes bend; then dispense and mix in the sample tube tray.
-
28.
When all silica has been dispensed into the sample tube trays, press the Start icon.
NOTE: Do not open the easyMAG sample module lid during testing phases! Doing so will abort the run.
-
29.
The run will continue until all samples are completed. “Finished” will display on the bar at the bottom of the screen. While the run is in progress, label a 1.5-mL tube for each sample and control for long-term storage.
-
30.
Complete the run by pressing the View Results Icon (Magnifying Glass).
-
31.
Press the Printer Icon and press OK.
-
32.
The report will print. A window will pop up reading “The run results are being printed. Mark this run ASSESSED?” Press Yes.
-
33.
Quickly check the report for any errors. If an error was signaled, repeat the extraction and refer to troubleshooting.
3.2 RT-PCR Amplification by TEM-PCR
-
1.
Before using AmpCheck reagent for the first time, make a 1/50 dilution by adding 245 μL RNase-free water into the tube containing the 5 μL AmpCheck and mix.
-
2.
Make sure the thermal cycler is preheated to 50°C before placing samples into the unit.
-
3.
Thaw the template RNA, dNTP Mix, 5× QIAGEN OneStep RT-PCR Buffer, and RNase-free water, and place them on ice.
-
4.
Mix the ResPlex II SuperPrimers by vortexing briefly.
NOTE: It is important to mix the solutions completely before use to avoid localized differences in salt concentration.
-
5.
Prepare a master mix according to Table 2. The master mix typically contains all the components required for RT-PCR except the template RNA. Prepare a volume of master mix 10% greater than that required for the total number of reactions to be performed. A negative control (without template RNA) should be included in every experiment. An additional reaction for amplification of AmpCheck should be included as an amplification check.
Table 2 Composition of reaction mix for QIAplex RT-PCR amplification reaction -
6.
Mix the master mix thoroughly and dispense appropriate volumes into PCR tubes.
-
7.
Mix gently, for example, by pipetting the master mix up and down a few times.
-
8.
Add template RNA to the individual PCR tubes. Include a negative control by substituting RNase-free water for the RNA sample volume. Include an amplification check with 5 μL AmpCheck (diluted 1/50) instead of template RNA.
-
9.
Program the thermal cycler according to the program outlined in Table 3.
Table 3 Optimized cycling protocol using the GeneAmp 9700 PCR system running in 9600 emulation mode -
10.
Start the RT-PCR program while the PCR tubes are still on ice. Wait until the thermal cycler has reached 50°C. Then, place the PCR tubes in the thermal cycler.
3.3 Amplicon Detection and Differentiation by Luminex
-
1.
Before use, Detection Buffer and Stopping Buffer should be brought to room temperature (15–25°C).
NOTE: These buffers can be stored at room temperature so that they are ready to use.
-
2.
Heat a heating block or thermal cycler to 52°C.
-
3.
Heat Stopping Buffer to 52°C, and keep it at 52°C until use.
-
4.
Mix the ResPlex II Bead Mix by vortexing for at least 15 s.
NOTE: Protect the ResPlex II Bead Mix and reaction mix from light. Foil should be used to cover the tubes and 96-well plate.
-
5.
Prepare the detection mix according to Table 4.
Table 4 Composition of detection mix -
6.
The detection mix contains all of the components needed for the reaction except for the PCR products and the diluted Streptavidin–PE. Prepare a volume of detection mix 10% greater than what is required for the total number of assays to be performed.
-
7.
Vortex the reaction mix thoroughly. Dispense 45 μL into each well of a 96-well, flat-bottom plate.
-
8.
For each assay, add 5 μL of the RT-PCR reaction (from the previous section) into a sample well. Mix thoroughly by pipetting up and down.
-
9.
Incubate samples at 52°C in the dark for 10 min.
NOTE: Keep samples at 52°C until the detection reaction is completed.
-
10.
While the samples are incubating, proceed with step 11.
-
11.
Make a fresh 1:1 mixture of Detection Buffer: Streptavidin–PE at room temperature. Make enough to use 10 μL of the mixture per assay. For example, add 50 μL Streptavidin–PE to 50 μL Detection Buffer. Prepare a volume 10% greater than what is required for the total number of detection assays to be performed.
-
12.
Cover with foil or keep in a dark place to protect from light.
-
13.
After incubation (step 9), add 10 μL Detection Buffer:Streptavidin–PE to each sample. Keep the samples at 52°C, and mix briefly by pipetting up and down.
-
14.
Incubate at 52°C in the dark for 5 min.
-
15.
Keep the samples at 52°C, add 120 μL Stopping Buffer (prewarmed to 52°C) to each reaction.
-
16.
Keep the samples at 52°C and protect them from light until analysis.
3.4 Result Output and Interpretation
Samples are analyzed on the LiquiChip 200 Workstation using QIAplex MDD Software. (Alternatively, the Luminex 100 IS System or Luminex 200 System with QIAplex MDD Software can be used). A mean fluorescence intensity (MFI) is reported for each target. Table 5 provides an example of data, from a ResPlex II run. The positivity cutoff is dependent on the instrument and software used for analysis. The cutoff value for each target is determined as the sum of the mean plus four times the standard deviations of the negative controls.
4 Notes
-
1.
HotStar Taq DNA Polymerase (contained in the Qiagen OneStep RT-PCR Enzyme Mix) requires initial activation by incubation at 95°C for 15 min before amplification can take place. This incubation also partially inactivates the reverse transcriptase. The thermal cycling program includes steps for both reverse transcription and PCR. Do not activate HotStarTaq DNA Polymerase until the reverse-transcription reaction is finished.
-
2.
It is important to maintain an RNase-free environment during extraction and RT-PCR setup steps. Set up all reaction steps in an area separate from the other areas (extraction, amplification, and detection). Dead air boxes can be used for each step/area to avoid contamination between areas.
-
3.
Set up all RT-PCR reactions on ice. RNA is the target, which is fragile. Keeping the reaction mixes cold will reduce RNA degradation.
-
4.
Use disposable, RNase-free tips containing hydrophobic filters to minimize cross-contamination.
-
5.
Use of the GeneAmp 9700 PCR System (Applied Biosystems) running in the 9600 emulation mode for the amplification step is recommended. Performance of this protocol using other equipment has not been verified yet.
-
6.
From the beginning of the hybridization procedure in the detection step, the detection reaction must be kept at 52°C until analysis on the LiquiChip 200 Workstation.
-
7.
Protect the ResPlex II Bead Mix and reaction mix from light. Foil should be used to cover the tubes and 96-well plate.
-
8.
In a clinical validation study on 360 archived frozen nasopharyngeal swabs and aspirates, the sensitivity and specificity for RSV detection were 73.3 and 100%, when compared to a standard combined from cell culture and monoplex real-time TaqMan PCR. Sensitivities and specificities were 72.2–90% and 99.7–100%, respectively, for other respiratory viruses. When a full panel (96 tests) was run, the hands-on time and the test turnaround time were estimated as 55 min and 6 h, respectively (27).
-
9.
There is no validation data on PIV-2, PIV-4, enterovirus, and rhinovirus. There is some cross-reactivity between PIV-1 and PIV-3 in the ResPlex assay; of 27 samples testing positive for parainfluenza, eight samples (29.6%) had IMF values higher than the cutoff values for PIV-1 and PIV-3 (27).
-
10.
The assay was useful to detect and recognize viral coinfections, which are usually related to more severe clinical manifestations (30).
-
11.
Respiratory DNA viruses, such as bocavirus (36), adenovirus, and a recently reported respiratory polyomavirus (37), were not covered in the ResPlex II kits evaluated in the study. A new version of the ResPlex II kit, which covers bocavirus and adenovirus in addition to those described in the chapter, has been available from Qiagen since July 2008.
-
12.
We thank Melinda McCormac, Shufang Meng, and Wray Estes for their excellent technical support. This project was partially supported by a research and development grant from Qiagen. The protocol contains partial information in product inserts of the easyMAG and the ResPlex II kits and the Standard Operating Manual of the Molecular Infectious Disease Laboratory, Vanderbilt University Hospital.
References
Domachowske, J.B. and Rosenberg, H.F. (1999) Respiratory syncytial virus infection: immune response, immunopathogenesis, and treatment. Clin Microbiol Rev 12, 298–309.
Tang, Y.W. and Crowe, J.W. Jr. (2007) Respiratory syncytial virus and human metapneumovirus. In: Murray, P.R., Baron, E.J., Jorgensen, J.H., Landry, M.L., Pfaller, M.A., Eds. Manual of Clinical Microbiology. 9th Edn. American Society for Microbiology Press, Washington, D.C., pp. 1361–1377.
Arnold, S.R., Wang, E.E., Law, B.J., et al. (1999) Variable morbidity of respiratory syncytial virus infection in patients with underlying lung disease: a review of the PICNIC RSV database. Pediatric Investigators Collaborative Network on Infections in Canada. Pediatr Infect Dis J 18, 866–869.
MacDonald, N.E., Hall, C.B., Suffin, S.C., et al. (1982) Respiratory syncytial viral infection in infants with congenital heart disease. N Engl J Med 307, 397–400.
Nachman, S.A., Navaie-Waliser, M., and Qureshi, M.Z. (1997) Rehospitalization with respiratory syncytial virus after neonatal intensive care unit discharge: a 3-year follow-up. Pediatrics 100, E8.
Martinello, R.A., Chen, M.D., Weibel, C., and Kahn, J.S. (2002) Correlation between respiratory syncytial virus genotype and severity of illness. J Infect Dis 186, 839–842.
Walsh, E.E., McConnochie, K.M., Long, C.E., and Hall, C.B. (1997) Severity of respiratory syncytial virus infection is related to virus strain. J Infect Dis 175, 814–820.
Halasa, N.B., Williams, J.V., Wilson, G.J., et al. (2005) Medical and economic impact of a respiratory syncytial virus outbreak in a neonatal intensive care unit. Pediatr Infect Dis J 24, 1040–1044.
Macartney, K.K., Gorelick, M.H., Manning, M.L., Hodinka, R.L., and Bell, L.M. (2000) Nosocomial respiratory syncytial virus infections: the cost-effectiveness and cost-benefit of infection control. Pediatrics 106, 520–526.
Barenfanger, J., Drake, C., Leon, N., Mueller, T., and Troutt, T. (2000) Clinical and financial benefits of rapid detection of respiratory viruses: an outcomes study. J Clin Microbiol 38, 2824–2828.
Landry, M.L. and Ferguson, D. (2000) SimulFluor respiratory screen for rapid detection of multiple respiratory viruses in clinical specimens by immunofluorescence staining. J Clin Microbiol 38, 708–711.
Aslanzadeh, J., Zheng, X., Li, H., et al. (2008) Prospective evaluation of rapid antigen tests for diagnosis of respiratory syncytial virus and human metapneumovirus infections. J Clin Microbiol 46, 1682–1685.
Zheng, X., Quianzon, S., Mu, Y., and Katz, B.Z. (2004) Comparison of two new rapid antigen detection assays for respiratory syncytial virus with another assay and shell vial culture. J Clin Virol 31, 130–133.
Deffrasnes, C., Cote, S., and Boivin, G. (2005) Analysis of replication kinetics of the human metapneumovirus in different cell lines by real-time PCR. J Clin Microbiol 43, 488–490.
Barenfanger, J., Drake, C., Mueller, T., et al. (2001) R-Mix cells are faster, at least as sensitive and marginally more costly than conventional cell lines for the detection of respiratory viruses. J Clin Virol 22, 101–110.
Freymuth, F., Eugene, G., Vabret, A., et al. (1995) Detection of respiratory syncytial virus by reverse transcription-PCR and hybridization with a DNA enzyme immunoassay. J Clin Microbiol 33, 3352–3355.
Henkel, J.H., Aberle, S.W., Kundi, M., and Popow-Kraupp, T. (1997) Improved detection of respiratory syncytial virus in nasal aspirates by seminested RT-PCR. J Med Virol 53, 366–371.
Tang, Y.W., Heimgartner, P.J., Tollefson, S.J., et al. (1999) A colorimetric microtiter plate PCR system detects respiratory syncytial virus in nasal aspirates and discriminates subtypes A and B. Diagn Microbiol Infect Dis 34, 333–337.
Falsey, A.R., Formica, M.A., Treanor, J.J., and Walsh, E.E. (2003) Comparison of quantitative reverse transcription-PCR to viral culture for assessment of respiratory syncytial virus shedding. J Clin Microbiol 41, 4160–4165.
Weinberg, A., Zamora, M.R., Li, S., Torres, F., and Hodges, T.N. (2002) The value of polymerase chain reaction for the diagnosis of viral respiratory tract infections in lung transplant recipients. J Clin Virol 25, 171–175.
Boivin, G., Cote, S., Dery, P., De Serres, G., and Bergeron, M.G. (2004) Multiplex real-time PCR assay for detection of influenza and human respiratory syncytial viruses. J Clin Microbiol 42, 45–51.
Fan, J., Henrickson, K.J., and Savatski, L.L. (1998) Rapid simultaneous diagnosis of infections with respiratory syncytial viruses A and B, influenza viruses A and B, and human parainfluenza virus types 1, 2, and 3 by multiplex quantitative reverse transcription-polymerase chain reaction-enzyme hybridization assay (Hexaplex). Clin Infect Dis 26, 1397–1402.
Grondahl, B., Puppe, W., Hoppe, A., et al. (1999) Rapid identification of nine microorganisms causing acute respiratory tract infections by single-tube multiplex reverse transcription-PCR: feasibility study. J Clin Microbiol 37, 1–7.
Liolios, L., Jenney, A., Spelman, D., et al. (2001) Comparison of a multiplex reverse transcription-PCR-enzyme hybridization assay with conventional viral culture and immunofluorescence techniques for the detection of seven viral respiratory pathogens. J Clin Microbiol 39, 2779–2783.
Osiowy, C. (1998) Direct detection of respiratory syncytial virus, parainfluenza virus, and adenovirus in clinical respiratory specimens by a multiplex reverse transcription-PCR assay. J Clin Microbiol 36, 3149–3154.
Lee, W.M., Grindle, K., Pappas, T., et al. (2007) High-throughput, sensitive, and accurate multiplex PCR-microsphere flow cytometry system for large-scale comprehensive detection of respiratory viruses. J Clin Microbiol 45, 2626–2634.
Li, H., McCormac, M.A., Estes, R.W., et al. (2007) Simultaneous detection and high-throughput identification of a panel of RNA viruses causing respiratory tract infections. J Clin Microbiol 45, 2105–2109.
Mahony, J., Chong, S., Merante, F., et al. (2007) Development of a respiratory virus panel test for detection of twenty human respiratory viruses by use of multiplex PCR and a fluid microbead-based assay. J Clin Microbiol 45, 2965–2970.
Brunstein, J. and Thomas, E. (2006) Direct screening of clinical specimens for multiple respiratory pathogens using the Genaco Respiratory Panels 1 and 2. Diagn Mol Pathol 15, 169–173.
Brunstein, J.D., Cline, C.L., McKinney, S., and Thomas, E. (2008) Evidence from multiplex molecular assays for complex multipathogen interactions in acute respiratory infections. J Clin Microbiol 46, 97–102.
Boom, R., Sol, C.J., Salimans, M.M., et al. (1990) Rapid and simple method for purification of nucleic acids. J Clin Microbiol 28, 495–503.
Tang, Y.W., Sefers, S.E., Li, H., Kohn, D.J., and Procop, G.W. (2005) Comparative evaluation of three commercial systems for nucleic acid extraction from urine specimens. J Clin Microbiol 43, 4830–4833.
Han, J., Swan, D.C., Smith, S.J., et al. (2006) Simultaneous amplification and identification of 25 human papillomavirus types with Templex technology. J Clin Microbiol 44, 4157–4162.
Dunbar, S.A., Vander Zee, C.A., Oliver, K.G., Karem, K.L., and Jacobson, J.W. (2003) Quantitative, multiplexed detection of bacterial pathogens: DNA and protein applications of the Luminex LabMAP system. J Microbiol Methods 53, 245–252.
Fulton, R.J., McDade, R.L., Smith, P.L., Kienker, L.J., and Kettman, J.R. Jr. (1997) Advanced multiplexed analysis with the FlowMetrix system. Clin Chem 43, 1749–1756.
Allander, T., Tammi, M.T., Eriksson, M., et al. (2005) Cloning of a human parvovirus by molecular screening of respiratory tract samples. Proc Natl Acad Sci USA 102, 12891–12896.
Allander, T., Andreasson, K., Gupta, S., et al. (2007) Identification of a third human polyomavirus. J Virol 81, 4130–4136.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer Science+Business Media, LLC
About this protocol
Cite this protocol
Sefers, S.E., Li, H., Tang, YW. (2010). Simultaneous Detection and Differentiation of Respiratory Syncytial Virus and Other Respiratory Viral Pathogens. In: Stephenson, J., Warnes, A. (eds) Diagnostic Virology Protocols. Methods in Molecular Biology, vol 665. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-60761-817-1_17
Download citation
DOI: https://doi.org/10.1007/978-1-60761-817-1_17
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-60761-816-4
Online ISBN: 978-1-60761-817-1
eBook Packages: Springer Protocols