
Abstract
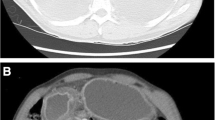
We report a case of esophageal perforation (Boerhaave syndrome) caused by vomiting related to a duodenal ulcer with pyloric stenosis. A 45-year-old male presented with left chest pain and dyspnea after forceful vomiting. Chest radiography and computed tomography (CT) revealed a massive left pleural effusion and left tension pneumothorax. Abdominal CT revealed pyloric stenosis with a remarkably dilated stomach. Tube thoracostomy and nasogastric suction were immediately performed and we selected conservative treatment based on the following factors—a stable general condition without sepsis, early diagnosis, and good drainage. Esophagogastroduodenoscopy on hospital day 9 demonstrated a healing ulcer in the lower esophagus and pyloric stenosis. We performed distal gastrectomy as elective surgery for pyloric stenosis due to a duodenal ulcer on hospital day 30. In summary, an esophageal perforation with contamination spreading to the thoracic cavity was successfully treated with conservative treatment.




Similar content being viewed by others


References
Biancari F, D’Andrea V, Paone R, et al. Current treatment and outcome of esophageal perforation in adults: systematic review and meta-analysis of 75 studies. World J Surg. 2013;37:1051–9.
Soreide JA, Konradsson A, Sandvik OM, et al. Esophageal perforation: clinical patterns and outcomes from a patient cohort of Western Norway. Dig Surg. 2012;29:494–502.
Teh E, Edwards J, Duffy J, et al. Boerrhaave’s syndrome: a review of management and outcome. Interact CardioVasc Thorac Surg. 2007;6:640–3.
Cameron JL, Kieffer RF, Hendrix TR, et al. Selective nonoperative management of contained intrathoracic esophageal disruptions. Ann Thorac Surg. 1979;27:404–8.
Mizutani K, Makuuchi H, Tajima T, et al. The diagnosis and treatment of esophageal perforations resulting from nonmalignant causes. Surg Today. 1997;27:793–800.
Altorjay A, Kiss J, Voros A, et al. Nonoperative management of esophageal perforations. Is it justified? Ann Surg. 1997;225:415–21.
Okten I, Cangir AK, Ozdemir N, et al. Management of esophageal perforation. Surg Today. 2001;31:36–9.
Shaker H, Elsayed H, Whittle I, et al. The influence of the ‘golden 24-h rule’ on the prognosis of oesophageal perforation in the modern era. Eur J Cardiothorac Surg. 2010;38:216–22.
Okonta KE, Kesieme EB. Is oesophagectomy or conservative treatment for delayed benign oesophageal perforation the better option? Interact CardioVasc Thorac Surg. 2012;15:509–11.
Seki H, Ueda T, Shibata Y. Spontaneous esophageal perforation related to a duodenal ulcer with pyloric stenosis: report of a case. Surg Today. 2001;31:1082–6.
Yoshida R, Shimoda M, Hida S, et al. Spontaneous esophageal perforation due to duodenal ulcer; report of a case. Operation. 2006;60:249–53 (Japanese).
Ootuski T, Miyanaga T, Endo N, et al. A case of esophageal perforation caused by pyloric stenosis with duodenal ulcer. J Jpn Surg Accoc. 2012;73:827–31 (Japanese).
Disclosures
Conflict of Interest:
Ryo Tanaka, Shin-ichi Kosugi, Daisuke Sato, Hiroshi Hirukawa, Tetsuya Tada, Hiroshi Ichikawa, Takaaki Hanyu, Takashi Ishikawa, Takashi Kobayashi and Toshifumi Wakai declare no conflict of interest.
Human/Animal Rights:
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008(5).
Informed Consent:
Informed consent was obtained from all patients for being included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tanaka, R., Kosugi, Si., Sato, D. et al. Conservative treatment of esophageal perforation related to a peptic ulcer with pyloric stenosis. Clin J Gastroenterol 7, 295–298 (2014). https://doi.org/10.1007/s12328-014-0493-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12328-014-0493-3