
Abstract
The greying of the global population has become a matter of concern for planners, scientists and the common man alike. In simple terms, the greatest challenge ahead is formulating appropriate and customized responses for the ‘needs of the elderly’. It is in this background that a study was commissioned by HelpAge India in 2016 to explore further strategies and pilot initiatives in the state of Kerala, which is much ahead of other states in India. Goal of the study was to develop informed frameworks and models for transforming Kerala to an ‘age-friendly’ state as a pilot age-friendly initiative in India. Kerala’s demographic transition from a state with high mortality and high fertility to one with a low count in both of these outpaces that of the rest of the country by 25 years according to Kerala Development Report of the Planning Commission in as early as 2008. Currently at 14% of the total population of Kerala, the number of those above 60 years is expected to reach 40% by the end of 2061. The declining birth rates and the migration of the young, coupled with the increase in life expectancy to an average of 72 years, Kerala is fast ageing with a greying population and increasing demands on the fiscal, health and social security mechanisms. Institutionalization of state government schemes/projects takes its own time. It may be noted that the age-friendly initiatives will lead to action in grass-roots level for senior citizens through day centres. Ultimately, the day centres will be converted into Agecare Service Centres of Government where all actions related to senior citizens will be coordinated by the people, of the people, for the people (ESHGs in rural and SCAs in urban will lead the action). ‘Age-friendly initiatives’ will do groundbreaking work into making ‘ageing’ a wonderfully productive period of life.
Access this chapter
Tax calculation will be finalised at checkout
Purchases are for personal use only
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Appendices
Annexure I

Annexure II: Study on Age-Friendly Services
(Foundation on which the age-friendly initiatives in Kerala is built-up)
The study on age-friendly services was done in 2016 by HelpAge India in the state of Kerala on the elderly who are living alone or with their equally aged spouses. This study was to understand their needs and concerns and to develop appropriate models that will provide them with age-friendly services, either on payment or otherwise, with relatively better access and ease.
Goal of the Study
Develop informed frameworks and models for transforming to an ‘age-friendly’ state.
Objectives
-
1.
Assess the number of elderly singles or family units in the study area who require assistance to live their lives with dignity and support.
-
2.
Develop a better understanding of the services currently available, the gaps, the issues and the changes required to make it more age-friendly.
-
3.
Develop appropriate models, on payment basis or otherwise, that can help such elderly people living alone to live their lives more comfortably.
Scope and Time Frame
The study was spread across the districts of Ernakulam, Kottayam, Pathanamthitta, Thrissur, Calicut and Kollam. Initially although only four districts of Ernakulam, Kottayam, Thrissur and Pathanamthitta were selected, Calicut was added as there was considerable migration from there also. The study covered about 600 respondents belonging to the upper class, the upper-middle class, the middle class, the lower-middle class and the poor.
While initially the study proposed to have different target groups for Objectives b and c, it was later decided that the Objective c was equally applicable to all categories, only the source of funding being different.
The study was completed in three months. The time frame was extended as establishing contacts in the villages for FGDs took more time than expected.
Methodology and Tools
There were initial discussions held with institutions like IEEE and Kerala Sasthra Sahithya Parishad (KSSP) for the designing of the study. It was based on the outcome of these discussions that Calicut was also added. Kollam was added only for focus group discussions.
As the study team did not have a direct presence in the districts selected, it was decided to work through partner organizations. The organizations that partnered the study team are:
-
1.
Kollam—Nav Jeevan Trust
-
2.
Ernakulam Urban: Magics
-
3.
Ernakulam Rural: Department of Social Work, Sri Sankara University, Kalady
-
4.
Kottayam: Archana Women’s Centre
-
5.
Pathanamthitta: Action for Social Development
-
6.
Thrissur: Department of Social Work, St. Thomas College
-
7.
Calicut: Department of Social Work, Devagiri College
-
8.
All across the state: IEEE Student Chapter.
One-day training programmes were held at each of the centres to orient the field investigators on questionnaire-based data collection as well as the requirements through FGDs. There was a mid-course review as well, and the team was given feedback on the data collected. Revisits were recommended wherever the field data were seen to be insufficient.
This study adopted a three-pronged approach:
-
1.
Questionnaire-based
-
2.
Focus group discussions
-
3.
Discussions with caregivers and institutions providing support.
Five hundred individuals were sampled through the questionnaire-based approach. The questionnaires were largely close-ended. The questionnaires were administered through the field investigators of partner organizations identified in the target districts. Additional 100 were accessed through the students of IEEE Student Chapter.
Ten FGDs were held in all the selected districts, covering more than 200 participants. These FGDs were held in accessible spaces like Anganwadis, community centres, schools and, sometimes, even in their homes. There was a greatly enthusiastic acceptance among the participants, about both the concept and the need for intervention. The meetings were arranged through Pensioners’ Associations, Elderly Clubs, Pakal Veedu and Pensioners’ Union.
Interestingly, the questionnaire-based approach was lesser successful than the personal FGD-based approach. The propensity to accept old age and all its difficulties stoically, and the presence of family members or the tendency to accept such negatives as a natural progression of age kept them from opening up or discussing their problems openly. However, when in a group, these barriers were broken and they spoke freely about the challenges they face in everyday life.
The engagement with the caregivers was also two-pronged—through Web-based questionnaires and direct discussions. The Web-based questionnaire did not have as much response as expected.
Findings from the Study
Profile of the Target Group
A total of 529 people were interviewed using the structured questionnaire, and about 200 people were part of the FGDs. Of the 529 individuals interviewed, 299 were women and 230 men. The age-wise profile is as shown in the graph.

An analysis of the current place of stay of the interviewees showed that close to 50% of them stayed with their married children. But, 35% men and 26% women came in the most vulnerable category where they were either living alone or with their equally aged spouse. Additionally, 19% of the women were staying with relatives and 1% in old age homes.

As this was not a purely random selection of samples, it may not be theoretically correct to say that this is a true reflection of the picture at the field level. Even so, the current estimation of 46% of the elderly women and 35% of the elderly men staying without strong or reliable support systems is a matter of concern.
An age-wise break-up of the men and women living on their own is as shown:

Fifty-three percentage of the 32 women staying alone were above 70 years of age. This was 5% of the universal sample of women interviewed. They are the most vulnerable and require focused attention.
The next most vulnerable group are those who are living with only their spouse who may be also equally aged. Thirty-one percentage of the total women interviewed and 65% of the total men interviewed stayed with just their spouse. Of this, 37% of the men and 24% of the women were above 70 years of age.

These numbers are a matter of concern to the state, as this will have an impact on the policies that impact social welfare and security, health and even livelihoods.
Availability and Accessibility of Services
Health Services
There are many justifications for devoting public resources to improving the health of older populations. The first is the human right that older people have to the highest attainable standard of health. Yet, people often experience stigma and discrimination, and violations of their rights at individual, community and institutional levels simply as a result of their age. Under the right to health, states are obligated to deliver, without discrimination of any kind, health facilities, goods and services that are available, accessible and acceptable and of good quality.
The interviewees were asked a range of questions based on their health status, health-seeking behaviour, current ailments, issues and concerns and finally their recommendations. These questions were also discussed during the FGDs.
-
1.
Current Practices: About 50% of the men and the women stated that they visited hospitals regularly on a monthly basis, and 20% each stated that they have had to visit hospitals regularly on a semi-annual basis. Six percentage of the women and 5% of the men had to visit on a weekly basis.

-
2.
Reasons for the Hospital Visits: Forty-two percentage of the women and 46% of the men stated that they visited the hospital for controlling diabetes, 24% of women and 21% of men for treating hypertension and about 14% each for treating cardiac ailments. Thus, about 80% of the elders visiting the hospital were going for lifestyle diseases which required routine tests but needed consultations only if the tests showed abnormalities.
In the normal course of events, these routine tests, like testing of blood for sugar levels and cholesterol, and checking of BP, could be partially or fully done from home. There is modern medical equipment that can do all these tests and display results immediately. However, almost 80% of the elderly have to visit hospitals every month for these tests.

-
3.
Issues Faced: Medical health is the most important service frequently accessed by the elders, and they face a lot of problems in accessing this service.
-
(a)
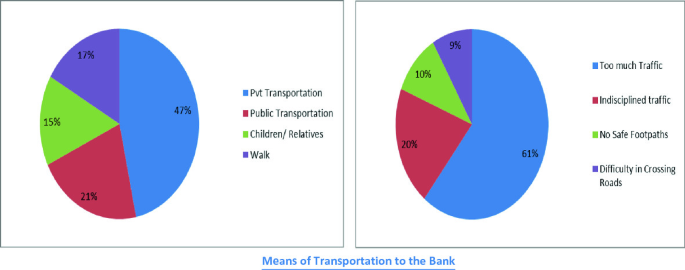
Transportation to Hospital: Of the 529, 26% used own vehicles as transportation for their trips to the hospital, 42% used private transportation facilities and 22% used public transportation facilities. Only about 10% walked. Of the 37 people staying on their own, 6 (16%) used own vehicles, 17 (46%) used private transportation, 10 (27%) used public transportation and 4 walked.
During the FGDs, the participants clarified saying that they found it very difficult to use the public transportation system and that is why most of them depended on auto rickshaws to take them to the hospital. The frequently increasing auto fare was a matter of concern to most of them. If the quality of the services of the public transportation improved, it would benefit 73% of those living alone and 64% of the universal sample.
-
(b)
Long Queues: Although only 141 (27%) responded with a clear ‘no’ when asked about being satisfied with the services provided at the hospital, many more responded to the reasons for dissatisfaction. Of the universal sample, 5% said that the doctors were too busy and not as responsive to them as desired, 20% said that the waiting time was too long and they had to wait in long queues, and about 2% spoke about the procedures being too complicated requiring external support to navigate.
However, there was a 100% dissatisfaction stated during the FGDs. The long wait and the unsympathetic response of the hospital staff were very vociferously conveyed during the FGDs. Although there were boards in some hospitals saying the elderly patients need not wait in the queue, there were many anecdotes of how rudely they were asked to get out when they jumped the queue. They spoke about the nurses telling them sarcastically that the board only meant that they need not ‘stand’ in a queue. They could mark their place and sit on the chairs till their turn came. However, there were never enough chairs also available, especially in the government hospitals.
-
(c)
Complex Procedures: The procedures followed in the hospital for registration, follow-up visits, payments, laboratory tests, etc., were difficult, and the elderly wanted some staff to guide them on it. Apart from the complexity of the procedures, they also felt that they were made to walk to too many windows for the different processes. New registrations, retrieving old registrations, making payments, going to the laboratory, then back to wait for the consultation with the doctors, all these involved a lot of moving up and down corridors or even floors. This tired them out as well as adding to the stress.
-
(d)
Scans and Invasive Testing Procedures: The participants also spoke about the increase in the number of tests that the hospitals insisted on. Most of them felt panicked at the thought of scans. They wanted to minimize the need for scans and invasive testing processes. Most of them demanded an age-friendly atmosphere in the hospital that minimized stress and helped them feel relaxed and cared for.
-
(f)
Not Getting Services of Senior Doctors: The elders felt that their cases were being passed on to house surgeons or senior medical students as they were just routine check-ups. But the students fumbled with injections, etc., making the process more painful. They also did not get adequate reassurance or advice from the students as they were not experienced enough. They felt they were being ignored in the larger scheme of things.
-
(g)
Queues at the Pharmacy: As most of them purchased their monthly requirement of medication after the visit to the hospital, they found even this difficult due to the long queues and crowds in the pharmacy section of the hospital.
-
(a)
-
4.
Coping Mechanisms
There were quite a few participants who spoke about voluntarily reducing the number of hospital visits, from once a month to once in two months or even once a quarter, because they did not want to face the long queues. This was specially the case with elders who were dependent on their children to accompany them to the hospitals. The care provider had to take a day or more off from work to take them to the hospital. This coping mechanism was mainly practised by the respondents who generally went for routine check-ups for diabetes and hypertension.
Although Kerala Government does have palliative care facilities in some Panchayats, they are more focused on patients who are totally bedridden like terminal stage patients, accident victims, etc. The elderly, who cannot walk to the clinic, do not fall under this category.
Some Panchayats also have doctors visiting the Panchayat once or twice a week. However, they do not do home visits and the participants said that they are not on call on the other days and hence unavailable for emergencies.
Employment and Income

Of the 529 interviewed, one man and 112 women (21%) were unemployed even prior the generally accepted retirement age. Currently, this has increased to 143 men and 255 women (75%). Of the unemployed, 336 are solely dependent on pensions of some kind, own job-related pension, husband’s pension, old age pension, disability pension or widow pension. Seven, of the 529, were continuing with their MGNREGA employment.
This has serious implications on the fiscal outflow from the government exchequer. With increasing number of people coming into the pensioners’ bracket coupled with the increase in the payout period per person due to the increase in life expectancy, the dependents on state-based incomes will increase exponentially, adding to the fiscal burden of the state. The government will have to seriously consider alternate methods of payments rather than making provisions for it in their normal budgetary allocations. Tax-funded minimum pensions may be an alternative to ensure the financial security of the older populations. This is particularly important for people who have been part of the informal workforce (e.g. women who have played a caregiving role throughout their life or agricultural workers) and who have not had the opportunity to accrue benefits such as pensions or health insurance.
From the respondents’ point of view, their current incomes are insufficient to ensure their continued well-being. Increasing costs of health care, transportation, basic necessities, etc., are not in keeping with the paltry amounts they are getting, especially through the social welfare-based pensions, like the old age pension or the widow pension. While the study did not look at change in lifestyles due to reduced incomes, the participants of the FGDs were concerned about this. They requested the study team to explore possibilities of introducing and promoting age-friendly livelihood skills so that they could either ensure or augment their incomes, especially when they were incapable of physical labour.
Age-Friendly Banking—Financial Transactions and Bank Services
As almost all payments are now being routed through the banks, 437 (83%) of the respondents had bank accounts. However, the visits to the banks varied from monthly visits (48%) to annual (8.5%).

Despite the large number of respondents holding bank accounts, they did not deem it to be ‘age-friendly’. Thirty-two percentage of the respondents had problems with banking. Their concerns ranged from the complex procedures to the difficulties in reaching the bank.

-
1.
Complex Procedures: The procedures changed frequently and confused the respondents. They required support to understand and comply with the bank requirements. Although most banks have a very prominent help desk, it was either never staffed or the person was too busy to provide the respondents the time and hand holding help required.
Even the paperwork required was not age-friendly with the font size being too small to read. The respondents had to invariably ask help to fill in these forms.
-
2.
Lack of Instructions/Information: Given the frequently changing procedures and processes involved in banking, the interest rates and the lack of staff who can guide them through their requirements, the respondents felt that this could have been ameliorated if the information/instructions were displayed prominently. Even what was displayed was usually in an A4 size sheet with small fonts, making it difficult for them to read.
-
3.
Time Taken: The procedures took too much time, and the spaces were not age-friendly. Issues such as lack of adequate priority seating facilities, lack of easy access to drinking water or toilets, and crowds at the counters were not conducive for age-friendly banking practices.
During FGDs, the participants very matter-of-factly stated that most of them had high blood sugar and it is a known fact that such people experience the need for frequent urination. However, no bank had toilet facilities that the public could access.
-
4.
Travel: Sixty-eight percentage of the respondents used either private or public transportation to reach the banks. Fifteen percentage depended on their children or other relatives to accompany them to the bank. Given that most of their children are working and banks can be accessed only during working days, the children have to take a day’s leave to accompany their parent to the bank. This has been stated as a problem by both the respondents and the caregivers. With the rising rates of crime, the FGD participants were fearful of being seen as coming out of a bank or even taking autos that they were not familiar with.

As the social welfare/security pensions are not deposited regularly on a monthly basis, sometimes they have to make multiple visits to the banks to enquire about it. This was proving to be problematic, and the current move of the state government in reaching the social welfare pensions to their homes has been welcomed by the participants.
-
5.
ATMs and Their Utility: Two hundred and seven (47%) of the respondents who had bank accounts had ATM facilities. Of those who did have ATM cards, 132 (64%) used it often or very often and 57 (28%) rarely. If this is analysed over the total number of respondents, only 39% had ATM facilities and only 25% used it frequently. Hence, this facility, although increasingly available and accessible, is not useful for the ageing population. The reasons given are:
-
(a)
Forgetting the pin or the operating instructions 30%
-
(b)
Did not apply due to the additional charges levied 5.5%
-
(c)
Unable to see the instructions 2.5%.
-
(a)
This is a matter of concern as the card is normally given to their children/relatives to withdraw money, and the elders may be unaware of misappropriations. With some modifications, like enabling a fingerprint recognition system instead of pin numbers, increase in the font size of the instructions or enabling audio facility, this can be made more age-friendly so that the senior citizens can carry out their financial transactions with safety and dignity.
Outdoor Environment and Neighbourhoods
Good neighbourhood enables older people to feel safe when going out for basic necessities such as shops and health services and for social and leisure purposes. It encourages exercise through walking, which benefits health (Traynor et al. 2013).
However, reality, as based on responses that came in through the questionnaires as well as the FGDs, showed that the current conditions of neighbourhoods and roads inhibited free movement and often led to enforced seclusion of the elderly.
Seventy-nine percentage of those interviewed said that they found the roads unsafe. Hundred percentage of those who attended the FGDs were very vocal in decrying the condition of the roads and the traffic. Heavy traffic not slowing at zebra crossings, pavements not usable due to vehicle parking, petty traders or extended shops were the often heard complaints.

Crossing the road is a nightmare for most of the participants. Unaccompanied outings are few due to these reasons, and they are dependent on their children or other well-wishers to take them out. As a result, they restrict their movement outside their homes as much as possible.
Lack of safe roads coupled with lack of safe transportation is resulting in a voluntary withdrawal from the external world. Two hundred and thirty-four said that physical mobility is a problem, and 145 stated that their mobility was restricted due to this. This enforced seclusion is detrimental to the well-being of the elderly.

There are no public spaces that are available for a quiet outing or even a walk. The participants expressed the need for such green spaces where they could take walks and feel refreshed. Currently, they are house-bound most of their time and feel excluded from the outside world.
Transportation
In developing countries, the basic minimum standards would at least be:

-
Public transportation is available and affordable.
-
They are accessible with low floors and disabled—friendly features.
-
They have priority seating which is respected.
-
Staff are courteous and considerate.
The study showed that close to 50% of the women and 40% of the men depended on private transportation or their children for their visits. The people who preferred to walk outnumbered the people who used public transport.
The reasons for not using public transportation facilities were:
-
1.
Difficulty in boarding the bus due to the height of the steps.
-
2.
The impatience of the drivers and the conductors.
-
3.
Crowded busses with no special features to help the elderly to maintain their balance.
-
4.
Although priority seating is available, it is often not respected and the elderly are forced to stand.
-
5.
Rash driving.
-
6.
Long-distance travel by public transportation is completely ruled out due to lack of toilet facilities and very brief breaks that are not in keeping with their reduced mobility.
-
7.
Even trains are not age-friendly as the steps are vertical. Climbing up is not a problem, but climbing down is a major problem, even for those without arthritis.
-
8.
Railway stations do not have escalators or ramps. Climbing up and down the overhead bridge is difficult.
-
9.
The train stops only for a brief time in the smaller stations. They have to fight the crowds to even get into the train. There is no priority seating in the train. Finding the right compartment, getting into the train at their slow pace, non-availability of sitting spaces are all deterrents to accessing this form of transportation.
-
10.
Despite reservation rules that are age-friendly, more often than not, the participants say they have been allotted middle or upper berths. As they have to frequently visit the toilet, these berths pose a problem.
Coping Mechanisms
Reduce frequency of trips requiring transportation facilities. Only the unavoidable trips, mainly for health care and bank transactions, are usually undertaken. Increasingly, there is the tendency to reduce the hospital visits due to these reasons as they do not want to burden their children each time they have to visit the hospital.
Respect and Inclusion
The most pressing matter of concern as expressed in the FGDs was the feeling of not being respected or of having lost one’s individuality and identity.
Once the initial barriers were down, the participants of the FGDs became more open and emotional. Their outpourings were centred around their feelings of being excluded from daily life. They felt they were not being ‘respected’ and ‘valued’. According to them, there was a serious erosion of the value systems prevailing in the state. The fast changing technologies, globalization, impact of cellular phones and mobile technology, easy access to Internet, both parents being employed, all these according to them contributed to the deteriorating value systems. While this advent cannot be stemmed, the participants felt that it was time we accept it and find alternate ways of dealing with the possible fallouts and adverse impacts. They felt that an attempt has to be made right from school levels to inculcate respect for their elders.
Retirement also led to a loss of their individual identity, and they feel unimportant, lost, invisible. Even the participants staying with their children felt lonely and cut away from the mainstream. The intergenerational dependencies that had earlier made them a cohesive unit no longer held true.
Ageism, prejudice or discrimination on the grounds of a person’s age is seen in different forms in different walks of life even in a state like Kerala, which revered its seniors. The doctors say, ‘well, you are old, what more do you expect?’, the children say, ‘you are old, why don’t you just relax at home and leave the rest to us?’, the community says, ‘you are old, now its time for you to relax and take things easy at home…’, the prospective employers say, ‘you are old, do you think you will be able to deliver?’ This finally becomes the mantra that the seniors internalize.
Some of the women participants had developed this into a ‘martyr complex’ saying ‘we should understand we are old and have to bravely face all the discomforts that come with it without complaining. Physical ailments, aches and pains are part of this’. One man gave the study team a small write-up which ended with the despondency of the dispirited, ‘….now all we do is wait for death…that is all we have to look forward to….’
Seniors are a valuable resource, and they can meaningfully contribute to the development of the society. They have workplace knowledge, skills, the wisdom of experience, the spirit of voluntarism and the time to spare. They can be effectively utilized, provided the society recognizes their capabilities, respects their inputs and gives them a chance to contribute. In short, healthy ageing requires an enabling environment that promotes intergenerational synergy.
Social Life and Entertainment

Kerala has made great strides in recognizing the need for age-friendly social life and has introduced the concept of Pakal Veedu or daytime home for enabling the seniors to spend quality time with their peers. In some Panchayats, they have also been provided with a building through the MP funds or donations. However, the recurring costs for the maintenance of these buildings have not been taken into account and most of such buildings are left locked. One of the participants pointed out very sarcastically that they have provided a maternity home for the street dogs. Wherever NGOs have taken up this concept, it is running well with well planned activities. However, they are not sustainable due to the heavy dependence on grants.
Hobbies
According to the study, watching TV and periodic visits to the temples or the houses of the relatives seem to be the most common social activities indulged in.

Apart from women also spending time in prayers, there does not seem to be much difference in the way men and women respondents spend their free time. Men also spend relatively less time in housework, which is understandable. Group activities are meeting friends and going for meetings, and solitary activities are reading and listening to music. More men than women seem to prefer to spend their time in such solitary pastimes.
There does not seem to be any significant difference in this pattern among the people who are staying on their own or with just their spouse. There is a marginal shift seen in the pastimes of the respondents staying with married children from watching TV to housework. The category under ‘nothing/watching TV’ has reduced to 57% from 62%, and the category under ‘housework’ has increased to 17%.
What is a matter of concern is the large percentage of respondents spending their time ‘doing nothing, just watching TV’, especially in the age group of 50–60, when they could have been extremely useful human resources for the community.
Outings
The responses to the question of ‘where all do you visit’, 22% said that they do not go anywhere. This is a fairly large number and a matter of concern. The reasons stated were lack of mobility, problems with transportation, lack of company, lack of finances and fear of going out into the roads. Interestingly, of the respondents who were staying with their married children, only 2% said that they do not go anywhere and they were all males. This seems more a matter of choice than lack of opportunity. However, respondents living with their married children had more chances of going out of their homes at least occasionally.
This only proves that seclusion is not a matter of choice but of circumstances, which, if corrected, would result in a much more active life for the senior citizens.
This was validated during the FGDs when all of them showed great interest in visiting places. The physical weaknesses did not seem to matter as much as their need for some diversion. Two hundred and seventeen (41%) of the respondents indicated that they would have liked to travel, go on pilgrimages, visit parks, go on picnics or even just visit relatives but were unable to do so due to reasons like: lack of companionship and finances. Sixteen percentage of the respondents above 80 also showed an interest in travelling.


Churches and NGOs have been active in arranging for day outings for the senior citizens.
Companionship
Loneliness was a major problem faced by most of the participants. Even those staying with their children faced this problem as everyone was too busy with their own schedules to spend much time talking to them. The grandchildren were too busy with their computers and mobiles to spare anytime for the grandparents. According to the participants, ‘the present generation did not even have time for their own parents; then how will grandparents come into their thoughts’.
Meeting and spending time with peers, who understood their problems, are of great help, and the respondents were very keen to start networks of senior citizens to create such platforms. Although the Pakal Veedu concept was based on this, this need is not being met as the day houses are not functional. The respondents feel that the Panchayats are not giving their needs any priority. There is no stigma attached to the Pakal Veedu concept unlike the old age homes. Some of the participants did mention that they were teased in their own homes when they attended Pakal Veedu or attended any meetings of the senior citizens.
During the FGDs, wherever such platforms were not available, the participants started making plans to meet somewhere, even in houses on a rotation basis, on a periodical basis. Wherever such platforms do exist, there is great enthusiasm in planning outings, competitions, community lunches during festivals and just getting together, even if it is only once a month.
Communication and Information
While the study did not go into great detail on their channels of communication and sources of information, it did look into their access to and ease of operating computers and cell phones.
Cell Phone Utilization
Two hundred and eighty three (53%) of the total respondents used the cell phone frequently. Of those who used it frequently, 261 (92%) used it only for making and receiving calls. Five were also comfortable in sending and receiving messages, and 17 were even conversant with WhatsApp. Of those who were conversant with WhatsApp, 6 were women and the remaining men. An age break-up showed that 6 were from 50 to 60 age bracket, 8 were from 60 to 70 age group and 3 were from 70 to 80 age group.

The respondents who were uncomfortable with using cell phones said that it was because they were scared of pressing the wrong keys, found it too complicated, the keys and/or the screen were too small or that they preferred the landlines for communication. Interestingly, the respondents also spoke of finding the touchscreen models difficult to use as the screens were too sensitive and their fingers were not agile enough or steady enough to swipe correctly. Some also spoke about the audio level not in keeping with their diminished hearing capabilities.
Computers and Internet
Forty-six percentage (8.7%) respondents stated that they used the computer frequently, of which 19 were women and 27 were men. Among women, 2 were from the ‘above 80’ age group. Eighty-one (15%) said that they would like to learn to use the computer. Here again, 4 are from the ‘above 80’ age group. Fifty (9.5%) respondents said they use the Internet frequently. Seventy-five (14%) said they would like to learn to use the Internet. Of those who showed interest to learn, 7 were in the ‘above 80’ age group.
HelpAge India is giving trainings for seniors to use computers and smartphones. A digital literacy training centre has been started for elderly at Vayojana Sevana Kendram. Through Senior Citizen Associations, HelpAge India implements the digital literacy programme all over Kerala and successfully completed hundreds of training sessions
-
Routine Requirements
Respondents were asked about their routine practices of purchasing groceries, provisions, accessing their supplies from the PDS, cooking, washing and ironing. As expected, the role of children increases in keeping with the increase in age of the respondents.



As is seen, the major procurers are either self or the children. There are no other local support systems available. This is a matter of concern for those who are living on their own. Twenty-five of the respondents had to travel more than 4 kms to buy their rations, and of them, 7 were in the ‘70-80’ age group and 4 were in the ‘above 80’ age group. To make matters worse, they were using the public transportation system to make these purchases on a monthly basis, sometimes even more. This same group had to also travel more than 4 kms to also access health facilities and the bank. Of the 4, in the ‘above 80 group’, two are staying on their own. Given the fact that they are only about 6% of the respondents above 80 and 0.7% of the total sample size, they may tend to get missed out in the final reckoning, due to the costs involved in reaching out to small pockets of vulnerable populations.
To make matters worse for the elderly, they have to visit the ration shops more than once as about 20% state that all materials were not sold to them at one go, either due to shortage or due to non-receipt of the material.
Sixteen percentage of the respondents stated that they have problems accessing goods from the ration shop. Apart from the long wait and the rude behaviour of some of the shop keepers, they also spoke about physical weakness, forgetfulness and poor transportation facilities.
Ensuring timely information on the arrival of goods, age priority and providing basic amenities at the ration shops would greatly benefit the senior ration cardholders.
The fierce independence of the respondents is further evidenced in 74% of them washing their own clothes (self or spouse) and 51% doing the ironing themselves. Interestingly, 23% do not iron their clothes. The questionnaire did not look at earlier practices, and hence it is not clear if this is a change in practice due to age-related issues.
Services They Are Willing to Pay for
Interestingly, apart from 95, all other respondents wanted services at home. The help ranged from cleaning premises and washing clothes to supporting in purchases, financial transactions and even routine blood tests. However, only 27% said that they would be willing to pay for the services. Forty-two percentage of those willing to pay required routine tests at home or health care. The amounts they were willing to pay ranged from 87 willing to pay up to 1500, 25 willing to pay up to Rs. 5000 and 3 willing to pay even up to Rs. 10,000/- for the services. About 50% preferred a package deal, whereas the rest preferred to pay based on services rendered.
Business Model for Age-Friendly Care
Wherever the study team had an opportunity to interact with groups of senior citizens, they have been surprised by the vitality and positive energy created by the participants. The participants used the meeting itself to formalize their association and, in Pathanamthitta, would not let the team leave till they had helped them chalk out a plan of action.
Plan of Action as described by Pathanamthitta Groups
-
1.
The groups are willing to take over the responsibility of the Pakal Veedu, wherever available. They will charge nominal registration and membership fees. They are also willing to approach local business houses for monthly donations to keep the club operational.
-
2.
They will conduct a survey along with the Panchayat and the local Kudumbashree groups to map the senior citizens and understand their current status. They will take special care to map those living on their own, those who are immobile or incapacitated to reach the centre.
-
3.
They will identify interested educated youngsters to be trained as paramedicals and provide services on a paid basis. They will cross-subsidize those who cannot pay.
-
4.
They will procure necessary tools like sphygmomanometer, blood drawing implements, adult diapers, walking sticks or other assistive devices based on the services they will be offering.
-
5.
They will draw up a list of medical practitioners who are willing to provide their services on a periodical basis.
-
6.
They will also explore possibilities of linking up with Kudumbashree to provide home-based support like meals, washing, etc., on a paid basis.
Rights and permissions
Copyright information
© 2020 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Mathew, B. (2020). Age-Friendly Initiatives. In: Shankardass, M. (eds) Ageing Issues and Responses in India. Springer, Singapore. https://doi.org/10.1007/978-981-15-5187-1_4
Download citation
DOI: https://doi.org/10.1007/978-981-15-5187-1_4
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-15-5186-4
Online ISBN: 978-981-15-5187-1
eBook Packages: Social SciencesSocial Sciences (R0)