
Abstract
Most of the current environmental health researches assumes that exposure to the environmental agents occurs either in the residence or workplace, neglecting the mobility of the people due to commuting and daily activities. Mobility of the people varies in terms of spatial and temporal range, that is, from momentary short ones to generation-scale long ones. Focusing on the daily movement of the people, various methods for grasping the mobility, which also range from simple observational methods like time allocation to methods with advanced technology like global navigation satellite systems, will be reviewed. Referring environmental health studies examining the health effects of either air pollution or heat, importance of the mobility of the people is discussed. Assessing the mobility will open a new research avenue for the study of infectious diseases as well as noncommunicable diseases.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
1 When Location Matters?
1.1 Environmental Versus Biological Monitoring
Environmental health concerns the relationship between exposure to various physical, chemical, or biological (often microbiological) factors in environment and health outcome; hence, the evaluation of exposure is the crucial part of it. In addition to these materialistic factors, exposure to certain social environment, like poverty-prone neighborhood, accessible public facilities, etc., has been gaining increasing attention since 1990s, which is now known as “social epidemiology.”
Depending on the media (most of the case, relevant media should be food, water, air, soil, etc.) as well as the agent of concern, a variety of the methods exists to evaluate the exposure, and exposure evaluation has been recognized as an independent research field. The procedure for exposure evaluation can be largely classified into two categories, that is, measuring environment and measuring organism; these are the procedures called as environmental monitoring and biological monitoring. Depending on the media and the agent, one or both of these methods are utilized. For example, both (organic) mercury from fish and cadmium from rice are heavy metals exposed through food consumption. Therefore, by monitoring the concentration of these metals in respective major food source, combined with food consumption data, exposure (ingested amount of mercury/cadmium) could be estimated. Biological monitoring for these metals is also possible by measuring the concentration of mercury in the hair (which reflects the concentration in the blood, and approximates the concentration in the brain) or cadmium in urine (which reflects the concentration in renal cortex). Detailed discussions about these two categories of monitoring are beyond the scope of this book, and interested readers should refer to existing textbooks.
Unlike the case for arsenic in water or mercury in the fish, many of the major “classical” air pollutants like NOx, SOx, CO, PMs (either 2.5 or 10) do not have appropriate biological exposure markers, and we need to rely on the environmental monitoring. This is also true for the exposure to temperature or to noise, both of which are associated with atmospheric exposure. In conventional environmental health study or environmental epidemiology, environmental monitoring of the outdoor atmosphere at the residential area of the participants has been used as surrogates for individual/population exposure to the agents of concern. Implicit assumption here is that people would stay in their residence, and variation of the exposure due to their daily mobility is, if any, negligible. Although this assumption is not realistic at all, this approach has been successful in a sense evidenced by the existence of numerous epidemiological findings in this area in the past.
In fact, exposure to pollutants or physical factors associated with air/atmosphere is heavily influenced by the location of the individual. Assume we would like to estimate an individual’s exposure to nitric oxides, most of the case, individuals would not stay in the home whole day, particularly in urban settings, commuting into city center or business districts for workplace or for schooling, thereby exposing themselves to environments that are different from their own residential neighborhoods. In this sense, Kwan [6] has suggested that research involving geographical components should reconsider conventional methods to estimate the exposure, referring to environmental health/epidemiology (together with the research on segregation or on the issue of accessibility).
Richardson et al. [11] pointed out that due to the accumulation of highly sophisticated spatial and spatiotemporal technology like GIS, GPS, remote sensing, and computer cartography, collectively termed as geographic information science, it becomes possible to model the disease process involving multiple spatiotemporal data obtained in different disciplines. Likewise, the exposure to environmental factors could be evaluated using such spatiotemporal data. Spatial resolution of various types of environmental data becomes so high that heterogeneity within the area of commuting distance could be documented. In addition, recent technical progress in downscaling of the climate models (see [2]) enables the researchers to predict differential impact of climate change within relatively small areas.
1.2 When Mobility of People Matters in Environmental Health?
Apart from the environmental data, to consider the mobility of the people, we need to collect the information on the mobility of people with enough spatiotemporal resolution.
Mobility of people can mean wide variety of phenomenon in terms of time, space, and context as listed in Fig. 2.1. Time scale of the mobility can range from moment to moment as exemplified by the Ecological Momentary Assessment (later in this chapter) to years, even including hundreds of centuries (like Out of Africa, the expansion of our ancestors)! Duration of the sojourn time should be considered as an independent factor and can also range from few seconds to generations; for example, workplace exposure to hazardous substances (including radioactive materials) would be evaluated in terms of minutes, while the effects of regional migration may emerge after several generations. Accordingly, spatial scale could range from a few meters to thousand kilometers. A few meter matters when micro-scale environments such as indoor (including air-conditioning) vs. outdoor, inside and outside of vehicle are considered, for example. At larger scale, proximity to major roads or any combustion facility could exert significant influences on exposure to noise or air pollutants. Far larger scale can change the environment as a whole; an important aspect in today’s environmental health is that people can make a global scale travel within 24 h. Mobility of people also entails the change in the context; by changing the location, the socioeconomic and cultural aspects of the neighborhood would change, which may affect the meaning of material environment and, in turn, health status of the moving individuals. At the same time, change in location means the change in activities of the individuals; for example, individuals working at outside road construction site might have much higher physical activity levels (and increased ventilation rate) and higher exposure to heat, dust, and noise than staying at home.

Schematic classification of various type of human mobility by “relevant” spatial and temporal scales. For example, “Migration’ takes place with relatively long time, ranging from months to multiple generations and traveling relatively long distance, while “outdoor/indoor” discrimination is needed even a couple of meters apart. ‘EMA’ stands for ecological momentary assessment (see text)
While it is fairly difficult to consider all of these potential factors, in case of atmospheric exposure, geographical location of the individual should be the factor to consider in the first place, since it does provide the basis of the air which she or he inhales in every moment. In this chapter, main focus will be on daily mobility of people for commuting and for other daily life activities. Geographical location is crucial for some physicochemical environmental factors other than air pollutants. One such example is heat environment, which consists of temperature, humidity, air flow, and radiation, and varies even with a very small scale, reflecting the variation of land use or land cover, local topography (layout of surrounding buildings, for example), or elevation. In addition, numerous heat sources are found in human-built environment, including exhaust gases, waste heat, etc. As a result of combined effects of these factors, most of the urban centers have warmer environment, compared to the surrounding areas, termed as heat island.
2 How to Grasp the Moving People? (2 Illustrations)
Mobility of individuals has been dealt with in many research areas. In urban planning, grasping mobility of individuals is crucial to create an appropriate layout for transportation, public space/facilities, and private houses. In public health, mobility of individuals sometimes play key role in the spread of diseases (described later). Also, mobility has been one of a classical topic in the area of human ecology since it is associated with the question of how a population utilizes the environment spatially as well as temporally (time allocation studies). Mobility is also associated with energetics (utilization of somatic energy) as a part of physical activities in general. As such, many methods to grasp the mobility of individuals have been developed (Table 2.1), which will be discussed below.
The simplest method is field observation. Time allocation studies observe the individuals in the targeted field and record the location and type of activity for a given period, which is useful to answer some of the basic questions in human ecology or other related fields as noted above. While this method is in a sense “perfect” since the observer can obtain whatever details she or he wants, obvious disadvantages include time-labor intensiveness, biased behavior due to the presence of observing researcher. A simplified variation of the time allocation is the spot-check method, in which researcher will observe the people’s activity in certain fixed location(s) (e.g., see [9]). Despite its simplicity and easiness, spot-check method could provide valuable quantitative information. Activity diary is another classical method, which relies on the self-recorded diary. This would solve the issue of labor-intensiveness for researcher and could cover much larger number of individuals, but like other self-reporting methods, reliability and accuracy of the record are the main problems to be considered. Activity diary is useful when researchers are interested in qualitative aspects of the moving behavior.
Person-trip is another method, which has long been utilized especially urban planning as well as urban studies (e.g., see ([4, 8])). Person-trip uses a predetermined, formatted questionnaire to be either self-recorded or recorded by interviewers, through which location of the individual, purpose of travel (translocation), and method of travel (either walk, bicycle, private car, public transportations) for a given period will be obtained. While this method has problem of bias and/or inaccuracy due to recall, brevity and simplicity made this method popular, particularly when a large population needs to be covered. Many governmental (both national and local levels) surveys utilize this method to quantify the volume of mobility, for example, traffic volume of vehicles.
GPS (Global Positioning System) has been used as if it was a generic term, but actually GPS is a name of a system developed in USA. Generic name for the systems is global navigation satellite systems (GNSS), which is referring to any system that locates specific targets by use of the combination of signal-detecting device and a group of satellites. In this book, the “targets” are basically human individuals, but they could be animals (so-called activity logger) or traffic vehicles. Spatial resolution of contemporary GPS is fine enough to locate individuals for many study fields, and it solves the issues of time-labor intensiveness and false or biased report. Thus, this has been used in various research areas including anthropology, human ecology, and presumably sociology, and urban studies (see [6, 11]). Another advantage is that GPS uses electrical data processing, which also alleviates the risk/errors associated with data transfer. On the other hand, in some area like inside building or underground malls the signal for GPS are generally weak and difficult to detect. Although the GPS could provide very rich and useful information regarding the mobility, individuals rarely own the device, and researchers need to provide and distribute it to the participants. This has been overcome by the recent propagation of GPS-equipped mobile phones and alike.
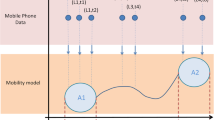
Mobile phone per se can be also utilized as a tool in capturing the location of individuals without using GPS device since every call made by mobile phone is registered by nearby relay station, hence generating a record regarding approximate location of the mobile phone users at the time of the call. By collecting such records of local calls, researcher can trace or reconstruct the translocation of individuals. Major advantage of this method is the fact nowadays a large proportion of populations own the mobile phone even in developing countries and in very remote areas. On the hand, researchers need to negotiate with mobile phone company to obtain such record, and the major barriers for such negotiation are as following: (1) conflict with the protection of privacy information (even when the information is provided in anonymous manner) may arise, (2) often there are two or more mobile phone companies operating in a given area, and (3) since the information is provided in anonymous manner, demographic parameters of the mobile owner are not known to the researcher. Effort has been made to overcome the last point, in which an algorism has been developed to estimate the demographic attributes of a mobile phone owner through the pattern of mobility, although the feasibility as well as the accuracy of estimated attributes needs further investigation (Arai, Shibasaki, in preparation).
Wesolowski et al. [15] compared the mobility data obtained by a person-trip type survey with the one obtained by mobile phone; both conducted in Kenya over the same period. Reflecting the nature of the methods, numbers of the participants were 2650 and 35,000 in the survey and mobile phone analyses, respectively. While the person-trip type survey was cross-sectional in nature, the mobile phone records followed the movement of the people for 3 months. While the resultant two data sets agreed in some aspects of the travels such as (1) most visited areas (in terms of districts) or (2) overall relative frequency of individuals with different number of travels, they disagree other aspects such as the number of mobile phone subscribers in the area as much as ten times.
3 Examples of Dynamic Exposure Evaluation: Air Pollutant and Heat
In this section, a couple of examples will be presented that incorporates the mobility of the individuals/groups in estimating exposure to physicochemical factors in the air. As the physicochemical factors, air pollutant and heat will be discussed. In the final part, a rather classical, different approach to trace individual exposure will be also introduced.
3.1 Dynamic Exposure to Air Pollution
A relatively large spatial scale study has been conducted covering approximately 80 × 200 km area in Belgium [3], which compared regional exposure estimates for two representative air pollutants, NOx and ozone, under two alternative assumptions. First, exposure assumed to occur in the residential place of the participants (static exposure), that is, the mobility of the participants is neglected. Second, mobility of the people was taken into account in estimating exposure (dynamic exposure). Information on mobility was obtained through activity diaries collected from 8800 residents, which is then extrapolated to a synthetic (but reflecting the demographic structure of actual) population of approximately 5 millions. The target geographical region consisted of 1145 zones (327 municipalities) whose average area was 12 km2, and the location of each individual has been predicted for 1 week (7 days) by 1-hr interval. Pollutant concentrations are estimated for NO2 and ozone using air pollution models (i.e., an emission model combined with a dispersion model) for a year by 1 h interval and 1 × 1 km resolution with finer resolution along major roads. Based on the location data and pollution data, time-weighted exposure estimate was calculated under two conditions: with and without taking peoples’ mobility into account. To estimate the municipality-wise health impacts of the exposure to these air pollutants, the time-weighted exposure estimate was converted into the respiratory mortality using the information of existing epidemiological data, which is then converted into years of life lost (YLL) following the burden of diseases framework by WHO.
The analyses revealed the pollutant-specific regional difference in the pollutant concentration; that is, for NO2, urban zones had higher concentrations than rural zones regardless the age and gender, and for ozone, it was vice versa. As expected, urban and industrial zones have much larger population in daytime, which was in contrast with the surrounding zones. As the results, dynamic exposure for NO2 for the whole population was slightly higher than static exposure, while for ozone it was vice versa. While the difference between static and dynamic exposure were statistically significant, the difference was small and reached only up to 3%. In terms of health impact, again the difference between the two methods was statistically significant but small (1.2% increase for NO2 and 0.8% decrease for ozone). At the municipality level, the maximum difference between the two approaches reached as large as 12%, where dynamic was higher than static, and larger differences were usually observed in rural areas. For ozone, maximum difference was only 4% (dynamic was lower than static).
While the extent of impacts shown in this study might not be so remarkable, the results demonstrated that mobility of people could have significant impact on the estimate of health impact by air pollution and that such an impact could be more remarkable at smaller scale. As pointed out by the authors, considering the mobility of people in air pollution issue inevitably connects the issue of transportation (and urban planning) with health issues, which is also commended from the viewpoint of eco-health. Similar dynamic-vs-static comparison was conducted with much smaller sample size in western New York, and as naturally expected the difference between the two approaches depended on the pattern of spatiotemporal pattern of air pollutants, PM2.5, as well as on that of behaviors [17].
The Human Early-life Exposome (HELIX) is a multi-country (eight countries), multi-cohort project in Europe to characterize early life exposure to various chemical and physical environmental factors and to associate them with health consequences in early life ([13] project URL: http://www.projecthelix.eu/en). Involving 28,000 mother-child pairs, the project would try to grasp the whole picture about the exposure as much as possible, and the use of time-space activity information is planned, which will be utilized to estimate the participants’ exposure to not only air pollutants but also noise, UV radiation, temperature, and built environment/green space etc. Basically, the environmental data is collected from (ground) monitoring stations and/or remote sensing. In addition, smartphone-based “personal exposure monitoring kit” has been developed that enables to capture not only the location of mothers and children but also their physical activities and air pollution by built-in accelerometer and sensors for UV and PM2.5. Recent progress of this project can be found at the following URL: https://www.isglobal.org/en/web/guest/healthisglobal/-/custom-blog-portlet/prova/5620053/7201.
HELIX is an ambitious attempt, which needs large amount of budget (8.6 M euro, according to the web page), time, and manpower. Considering the nature of current “environmental exposure,” that is, long term, multiple species, and mild to moderate (rather than severe) level, probably such an extensive effort is required to elucidate the relationship between environmental agents and health consequences.
3.2 Dynamic Exposure to Heat
Heat is another environmental factor, which might have some relevance to the mobility issue, since urban heat, or heat island, is a ubiquitous phenomena common to most of the big urban areas, which would pose additional heat burden to urban dwellers as well urban commuters under the influence of climate change (global warming). Usually, effects of heat are considered to be immediate or short, which is different from those of air pollutants, whose effects can be both short term and long term.
Although not involving mobility assessment, Laaidi et al.’s study on the heat-mortality relationship [7] is worth to be discussed here. This study analyzes the relationship between all-cause mortality among the elderlies living in Paris, France, or nearby area and land-surface temperature captured by satellites for a period of a heat wave occurred in August 2003. Based on a case-control study of 241 pairs of mortal-alive elderly people (age > 65), they found elevated odds ratio of mortality with increased land surface temperature (LST) of the residence area. Of noteworthy, the elevated odds ratio was associated with minimum (night time) LST averaged over either 13 days (whole observation period) or 6 days preceding the reported deaths but not with any LSTs averaged over 2 days preceding deaths or the day of death. This result suggested that the effect of heat might not be limited to immediate effects but might be “cumulative” to some extent. Also, approximately 0.37 °C of increase in temperature was associated with a significantly elevated odds ratio more than two, showing relatively potent effect of temperature on mortality. In this study, spatial resolution of the LST was 1 km2, and the case and control are matched, in addition to age and sex, for residential area, which contains 24–150 pixels, allowing the temperature comparison between the case and control. Targeting the elderlies, mobility would be less important than in younger generations.
We have conducted a study in which mobility of the people is considered in heat exposure issue in a subtropical urban area. This particular issue will be discussed in the next chapter.
3.3 Personal Monitoring Device
In the area of industrial health, exposures of the factory workers to air-borne chemicals peculiar to the factory are monitored with device, which is “worn” by each worker. Many types of such devices have been developed for various solvents or gaseous pollutants, among which the γ-radiation monitor is the best known. Cumulative exposure of each individual to the target chemical/radiation is quantified by analyzing the amount of chemical collected/absorbed by the device. Such personal device has been used for appropriate control of worker’s exposure to hazardous chemicals, but which could be extended into surveys in general population. While this method provides the estimate of individual exposure, if used in general population, distribution and retrieval of the device could be labor taking, and the quantified results would not give any hint of the potential sources of the exposure, since it only provides the cumulative exposure rather than temporally tracing the individual exposure.
4 Development and Potential Use of Mobility Information in Environmental Health
Potential use of mobility information would not be confined to the issues that have been discussed in this chapter so far. These examples will be discussed in this section.
4.1 Infectious Diseases
Many infectious diseases are transmitted through direct or indirect human-to-human contact. Mobility information has been utilized in the development of the models for propagation of some of the infectious diseases like influenza (direct) or malaria (indirect). In developing models, however, most of the attempts have based on simulations under plausible assumptions about the parameters, and not so much have been done using actual mobility data.
Malaria is one of the diseases that will be propagated by mosquitoes (indirect human contact). Propagation of the Malaria agent (Plasmodium) occurs when a mosquito (Anopheles) sucked blood from an infected human individual and then bites an intact individual. Since the range of area that traveled by a mosquito is relatively limited (approximately 3–12 km/day for Anopheles) [5], mobility of infected human individuals should play some roles in the propagation of the agent, particularly for long distance propagation. Wesolowski [14] tried to elucidate the role of human mobility in the propagation of Malaria in Kenya. Based on mobile phone records (either call or text) of about 15 million people for 1 year, they reconstructed the mobility patterns of the people and combined this information with spatial prevalence data of Malaria cases.
Location of the people (mobile users) is followed based on approximately 12,000 cell towers located in 692 settlements in Kenya. Travels (change of the location) beyond the border of each participant’s “primary settlement” (presumably where the residence is located) was counted and used for data analyses. A malaria prevalence map with 1 km2 resolution for 2009 has been used to classify the settlements according to their prevalence, then, combining the two types of information, that is, travels and prevalence observed in various settlements, they have estimated the proportion of the infected travels, which actually transported the malaria from one settlement to another. In this way, they could identify the source areas and the sink areas; the former supply the malaria, while the latter accept it. With such an analyses, they could show there were several distinct sources and sinks for Malaria in Kenya. Nairobi, the capital, and the area around the Victoria Lake were serving as the most remarkable sink and the source, respectively. Also, they observed that travel of people reflected the regional population density and regular travel, which is different from the travel of the parasites, where the lake regions serve as the primary source of the parasites, which flew into its surrounding areas and the capital area. Based on these observations, the authors suggested that the elimination program must take the imported case into account for the program to be successful. In addition, they demonstrated that this method could identify the “hot spot” (settlement), which shows distinct export and import of malaria incidence compared to adjacent settlements and that it can also provide useful information for elucidating the mechanisms of smaller scale transmission. Such an analysis provides a good example demonstrating the huge potential of using spatial analyses in the area of disease propagation.
They applied the same approach to model and predict the Dengue epidemics in Pakistan [16]. Mobility of approximately 40 million subscribers was followed for 6 months in 2013 across 356 tehsils (small politically defined areas in Pakistan), and analyzed with more than 15,000 reported cases observed in 82 tehsils over 7 months in 2013. Focus of the analyses was the spread of the disease from Southern region, where the warm climate supports the existence of vector mosquito throughout the year, to the northern regions with greater seasonality that limits the transmission. The authors calculated the “dengue suitability” of each region mainly based on daily temperature, which was combined with the probability of importing the infection by travelers from epidemic area to estimate the regional (spatiotemporal) risk of dengue epidemic. The results considering the mobile phone data are compared with those obtained from conventional “gravity” model, in which the travel volume of the people depends on the population sizes of and distance between the two regions (beginning and end of the travel). The results of the two models sometimes differ widely; among the two regions that experienced real dengue epidemics in 2013, import of infection could not be predicted by the gravity model, while the model with mobile phone information could. Also, the risk map generated for entire Pakistan showed substantially different pictures between the two models. Part of the reason of such differences is related with the observation that contrary to conventional mobility model, the mobile phone data showed no decay of travel volume with increasing distance of the regions. Overall, this research demonstrated the importance of grasping mobility based on real observational data to understand the spread of infectious disease at the level of a country.
For the diseases that are propagated through direct human-to-human contact, mobility of individuals among the population at stake should be much more crucial than the case of Malaria as described above. For example, in the outbreaks of SARS and MERS, identifying the “index case” would be important. Many quantitative models have been proposed to explain the spread of disease, but many of them have not taken the spatial information into account. As explained in this section, modeling with peoples’ mobility for infectious diseases has not been explored so much, while it is a promising field for the future.
At a larger spatial scale, spread of infectious diseases is associated with international travels. Using the data for international airline travelers, potentially “hot” areas for the spread of Zika virus have been identified. Potential threat of importation of the virus from Americas to Africa and Asian countries was demonstrated [1].
4.2 Activity and Noncommunicable Diseases
Relative importance of noncommunicable diseases (NCDs) has been increasing both in developed and developing countries; to name a few, ischemic heart diseases, stroke, diabetes mellitus, and various types of cancer are the big ones in this category. It has been quite well established that obesity and hypertension are associated with higher risk of these diseases, which in turn are associated with imbalance in the energetics. Numerous reports have been published regarding metabolic aspects of individuals at high risks for the NCDs. In these reports, activities are mainly evaluated with activity diary, pedometer, or accelerometer wore by the subjects. While these lines of information would provide valuable data to demonstrate the association between inactivity and risk factors of NCDs, a major defect is that it would not easily identify where in the daily life of the individual potential problem lies (i.e., leverage point). GPS information or mobile phone call record might be useful in reconstructing daily activity of individuals, since they can provide the information regarding the speed of the translocation, by which researcher can make a reasonable guess if the individual moved actively (i.e., walking or bicycling) or passively (i.e., driving a car, using public transportations). This is a relatively unexplored area, which might bear potential public health importance both in developed and developing countries.
4.3 Combining with “Ecological Momentary Assessment”
Ecological momentary assessment (EMA) refers to the methods of collecting data from individuals, who are in their daily lives (thus, ecological), providing real-time data (thus, momentary) repeatedly [12]. This is often enabled by using ICT devices that can prompt a series of questions to participating individuals to report their physical and/or mental conditions to the researchers. The devices can be also connected with sensors for physiological or clinical information like heart rate, blood pressure, or body temperature, blood glucose, or blood oxygenation [10], thereby health “events” like arrhythmia, asthma attack, and panic episodes can be recorded. In addition, EMA device has been connected with physical sensors to air pollution.
With this kind of device, chronological data, which can be associated with special health events, can be collected, accumulated, and later be related with physiological and environmental conditions (like air pollution) where the individual was in, revealing hidden association between the health event and certain patterns of preceding environmental and/or behavioral conditions. This methodology has been successful in clinical settings, particularly highlighted in clinical psychology, and its application to environmental health may generate a unique opportunity to grasp individual’s “dose” and “response” simultaneously. By combining with environmental monitoring information provided by satellites as well as ground monitoring stations, potential of using EMA will be greatly enhanced in the area of environmental health.
5 Conclusion and Beyond: What Is Real Exposure?
As noted in the beginning of this chapter, environmental health concerns the relationship between environmental condition and health consequences, spatial information is an indispensable component of this field. Conventional environmental health studies have dealt with the spatial aspects as represented by administrative units, which is basically a qualitative variable and black box so to speak, in nature. More quantitative aspect of the spatial distribution is worth to be focused in environmental health, and recent progress in information and communication technology including data processing enables us to develop a new type of research. In this way, spatial information becomes much more manipulative in the analyses with its implication being much clearer.
Refining spatial information is only a method to improve the accuracy of exposure estimate, hence, associated with other progresses in this field. For example, conventional environmental health study only focused on a very limited number of environmental factors, most often only a single factor, and the dose-response relationship was evolved around this single factor. This is most likely due to the fact that problems in the past were mostly associated with a single environmental agent like one chemical species. Contemporary issues, however, involve multiple factors that are converged on a single endpoint. In such a case, approach adopted in the HELIX study might be useful, although we yet to know what can be obtained with this approach. Refining exposure estimate should be considered in such a context to characterize comprehensive exposure.
While potential of this field is enormous, especially to be combined with other relevant techniques like EMA, there are a couple of issues that needs constant attention. First, as the technology (both hard and soft) advances, more attention should be paid for the importance of the issue of privacy. This is not only saying that full attention should be paid to protection of privacy, but also (1) considering the benefit for the people obtained through such information and (2) letting people know both aspects (goods and bads) of mobility information, thereby enabling them to choose appropriate reaction towards such investigation.
Finally, it should be emphasized that mobility information obtained in the ways described in this chapter might evoke a new discussion about what “true” exposure is and to what extent we need to know about the exposure. As partially discussed before, if you would like to quantify the exposure of an individual as much as possible, you need to actually chase this individual to see how the individual and the environment at a given moment is faced with each other. For example, merely wearing a fine-pore mask would substantially change the exposure to certain air pollutants, which could not be picked up by the approaches discussed in this chapter. After all, required fineness of the quantitative evaluation totally depends on the objectives of the specific research.
References
Bogoch II, Brady OJ, Kraemer MUG, German M, Creatore MI, Brent S, Watts AG, Hay SI, Kulkarni MA, Brownstein JS, Khan K (2016) Potential for Zika virus introduction and transmission in resource-limited countries in Africa and the Asia-Pacific region: a modelling study. Lancet 16(11):1237–1245. https://doi.org/10.1016/S1473-3099(16)30270-5
Cooney C (2012) Downscaling climate models. Environ Health Perspect 120:A22–A28
Dhondt S, Beckx C, Degraeuwe B, Lefebvre W, Kochan B, Bellemans T, Panis LI, Macharis C, Putman K (2012) Health impact assessment of air pollution using a dynamic exposure profile: implications for exposure and health impact estimates. Environ Impact Assess Rev 36:42–51
Doi K, Kii M, Lidason H (2000) Issues of commuter transport in developing countres. IATSS 25:37–44 [in Japanese]
Kaufmann C, Briegel H (2004) Flight performance of the malaria vectors Anopheles gambiae and Anopheles atroparvus. J Vector Ecol 29:140–153
Kwan M (2013) Beyond space (as we knew it): toward temporally integrated geographies of segregation, health, and accessibility. Ann Assoc Am Geogr 103:1078–1086
Laaidi K (2011) The impact of Heat Islands on mortality in Paris during the August 2003 heat wave. Environ Health Perspect 120:254–259
Muniz I, Galindo A (2005) Urban form and the ecological footprint of commuting. The case of Barcelona. Ecol Econ 55:499–514
Ohtsuka R, Sudo N, Sekiyama M, Watanabe C, Inaoka T, Kadono T (2003) Gender difference in daily time and space use among Bangladeshi villagers under arsenic hazard: application of the compact spot-check method. J Biosoc Sci 36:317–322
Patrick K, Griswold W, Raab F, Intille S (2008) Health and the mobile phone. Am J Prev Med 35:177–181
Richardson DB, Volkow ND, Kwan M-P, Kaplan RM, Goodchild MF, Croyle RT (2013) Spatial turn in health research. Science 339:1390–1392
Shiffman S, Stone AA, MR H (2008) Ecological momentary assessment. Annu Rev Clin Psychol 4:1–32
Vrijheid M, Slama R, Robinson O (2014) The Human Early-Life Exposome (HELIX): project rationale and design. Environ Health Perspect 122:535–544
Wesolowski A (2012) Quantifying the impact of human mobility on Malaria. Scientice 338:267–270
Wesolowski A, Stresman G, Eagle N, Stevenson J, Owaga C, Marube E, Bousema T, Drakeley C, Cox J, Buckee CO (2014) Quantifying travel behavior for infectious disease research: a comparison of data from surveys and mobile phones. Sci Rep 4:5678
Wesolowski A, Qureshic T, Boni MF, Sundsøyc PR, Johanssonb MA, Rasheedg SB, Kenth E-M, Buckeea CO (2015) Impact of human mobility on the emergence of dengue epidemics in Pakistan. PNAS 112:11887–11892
Yoo E, Glasgow R, Mu L (2015) Geospatial estimation of individual exposure ot air pollutants: moving form stati monitoing to activity-based dynamic exposure assessment. Ann Assoc Am Geogr 105:915–926
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Watanabe, C. (2019). Health Impact of Urban Physicochemical Environment Considering the Mobility of the People. In: Watanabe, T., Watanabe, C. (eds) Health in Ecological Perspectives in the Anthropocene. Springer, Singapore. https://doi.org/10.1007/978-981-13-2526-7_2
Download citation
DOI: https://doi.org/10.1007/978-981-13-2526-7_2
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-2525-0
Online ISBN: 978-981-13-2526-7
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)