
Abstract
To develop new Polymerase Chain Reaction (PCR)-based assays for nucleic acid detection for infectious diseases. Development of new assays on demand for emerging infectious diseases. For example, no proper nucleic acid-based tests exist for detection of H1N1 influenza virus. My lab, being the parasitology research unit aims to fill this gap by developing this ability.
You have full access to this open access chapter, Download chapter PDF
5.1 Sub-chapter A: Development and Validation of PCR-Based Diagnostic Test for Rapid Detection of Emergent Pathogens
5.1.1 Specific Aims
-
A.
To develop new Polymerase Chain Reaction (PCR)-based assays for nucleic acid detection for infectious diseases.
-
B.
Development of new assays on demand for emerging infectious diseases. For example, no proper nucleic acid-based tests exist for detection of H1N1 influenza virus. My lab, being the parasitology research unit aims to fill this gap by developing this ability.
-
C.
Extension of this technology for
-
Rapid detection using fast PCR reaction so that the tests can be used as point of care diagnostic tests.
-
Real time PCR tests for detection of virus loads.
-
5.1.2 Background and Significance
The area of molecular diagnostics has developed in a big way following the successful sequencing of the human genome in 2003. This was followed by the sequencing of the genomes of major infectious disease-causing organisms. This allowed the identification of unique sequences of microorganisms that could be used as markers to detect the presence of these microorganisms in the human body. Currently, infectious disease testing accounts for over three-quarters of total molecular diagnostics revenues internationally, most of which is due to increased disease burden of infectious diseases such as influenza, viral hepatitis, tuberculosis and HIV.
This project will develop the assays for Polymerase Chain Reaction (PCR)-based diagnostics in the much-neglected area of infectious disease diagnostics. We plan to systematically develop assays for the common and rare bacterial or viral pathogens with the objective of subsequently out licensing the tests to pathological laboratories. We will also develop rapid assays for detection of emerging infectious diseases. For example, the newly emerging influenza strains can be detected very accurately by PCR-based tests. This will open up a huge business opportunity and help catch up with the emerging international trend of next generation of diagnostics-assisted therapy.
PCR is a simple reaction involving the amplification of the genetic material from specific sources by chemical techniques. As applied to infectious diseases diagnostics, it involves the amplification of the genetic material of the infectious disease-causing microorganism to a detectable level proving the presence of the microorganism in the blood or other bodily fluid. These reactions are easy to perform and are quick and reliable tests to detect virtually all infectious diseases pathogens having either DNA or RNA as genetic material. As opposed to ELISA-based tests that detect the immune response of the body, the PCR-based test will detect the presence of minute amounts of microorganismso that an infection can be detected at a much earlier stage.
Furthermore, as an extension of this technology, live bacteria and viruses can be detected by Reverse Transcription-PCR that is not possible by any other assay. Once the basic assays have been established, a higher level of automation can be set up in the form of a real time PCR where viral loads can be determined. The probes and the primers developed by BioConsort will be used in these assays and will result in methodologies that will be unique.
Advantages of PCR-based diagnostics
-
1.
Reliability: As PCR-based diagnostics are direct tests that detect the presence of infectious microorganisms, if done properly are extremely reliable and gives consistent reproducible results. The positive result is a single band of a specific size at a particular location on agarose gel.
-
2.
Specificity: If the oligonucleotides are designed well, the PCR reaction will give a single band specific for a particular microorganism. In the absence of the microorganism or in the presence of a different microorganism, no such band will be seen.
-
3.
Sensitivity: As a PCR reaction amplifies even minuscule amounts of genetic material. It is this 100–1000 times sensitive than ELISA-based techniques that detects signals once the infection is well established. Furthermore, after the waning of the infection, the PCR signal will drop, but the immune signals will remain giving an erroneous result.
-
4.
Flexibility: Multiple reactions can be run in a single tube giving a result that appears as multiple marker bands for the same microorganism for better cross checking of the results.
-
5.
Speed: A PCR reaction is relatively quick to perform and as many as 96 samples can be analysed in a single run. If the whole plate is run, it also is much cheaper than conventional assays.
PCR-based diagnostics: the business potential in India
Market trends also indicate that the current screening tools involving antibody detection by the ELISA method will be replaced by detection based on molecular techniques such as PCR. Furthermore, the current molecular diagnostics products consist mainly of tests designed around a single biomarker associated with a disease state. Next generation molecular diagnostic techniques such as microarrays have been developed for the diagnosis of various infectious diseases, cancer and genetic disorders. This project will do the groundwork for tapping these opportunities.
A symbiotic relationship between pharmaceutical companies and diagnostic laboratories assists in the drug discovery process and in the development of diagnostic tests. Although PCR-based diagnostics services are available in eastern India, it is not well organized and professionally managed for it to become a commercially viable business option. PCR-based diagnostics are still in the novelty stage where certain PCR-based tests are used as a supportive test for the ELISA-based kits. The reasons are as follows:
-
1.
Lack of unified approach and vision: There is a severe lack of personnel with the adequate techno commercial background to make strategic plans for the tests to be pursued, the designing and execution of the tests as well as the business acumen to transform these tests from a highly specialized novelty item to easy-to-do mass service that can be a part of every clinical laboratory and hospital.
-
2.
Lack of hands on technical knowledge among the established pathologists of this region: Partly due to commercial considerations and partly due to lack of adequate molecular biology training in the medical colleges, the pathologists do not have the expertise to carry out these tests as well as interpret these results. As a result, these tests have not gained in popularity.
-
3.
Presence of an organized lobby for the promotion of ELISA-based tests: The manufacturers and the distributors of the diagnostics kits in the city have a strong lobby that opposes the introduction of newer diagnostic tests that will replace the existing tests. This includes Government regulatory authorities that approve the tests.
-
4.
Competition amongst pathological laboratories that cuts into each other: The competition amongst laboratories having the tests and those not having the tests results in sending of the tests to laboratories outside Kolkata to do the simple tests. A simple independent laboratory can tap into this business potential.
-
5.
Lack of validated tests suitable for Indian conditions: All the reagents are imported from abroad and there are no validation studies carried out to see if they will be suitable for conditions here. Hence tests often turn out to be unreliable, as a result of which the medical community cannot trust these.
India promises to be a big market for molecular diagnostics primarily due to increasing health awareness, demand and affordability for quality healthcare. This is further compounded by the fact that the number of insured lives have increased recently and medico-legal implications necessitate conducting such tests. Furthermore, 70% of the decisions of doctors are based on lab reports and such facilities are increasingly becoming available in towns and rural areas.
Roadmap for molecular diagnostics assay development
We plan to proceed on the following lines to develop tests, validate them and subsequently out license it for commercialization.
-
1.
Develop the PCR-based tests and validate them: My lab has the technical ability to develop the PCR-based tests based on technical know-how available in the scientific literature. Once the tests are developed, they can be validated in a sample population of 150–200. The validated tests can then be used in the clinical laboratory.
-
2.
Commercialize the technology by out licensing: Once the tests have been validated, they will be out licensed to pathological labs and hospitals that will then commercialize it.
-
3.
I ntroduce fast PCR-based techniques for rapid detection of infections: A 30 min detection tests will be developed that will have the potential to revolutionize PCR in such a way that it almost becomes a point of care diagnostic test.
-
4.
Introduce new tests and develop tests rapidly to emerging needs: Our lab will introduce one new test every month particularly in the areas where such tests do not exist.
Future prospects of PCR-based diagnostics in India
As the main advantage of PCR-based diagnostics is reliability and accuracy, newer instruments are being developed to do these tests even faster. Faster PCR tests would mean that these tests can be done as a point of care type diagnostics in the doctor’s chambers. Whereas the traditional PCR run with the gel run will take about three hours to give the results (2 h and 30 min for the PCR run with another 30 min for the gel run) newer PCR systems being developed here will complete the run in 30 min and the results can be obtained within an hour. An improvement to this is also being carried out where the test results can be viewed colourimetrically, where the positive results can be indicated by the appearance of a single colour in a tube.
The ability of a lab having the technical ability and the single-minded focus and determination in the area of PCR-based diagnostics will transform these tests into commercially viable tests that can compete with the other tests already available in the market. My lab hopes to get the first player advantage in this exciting field in the area of diagnostics.
5.1.3 Relevant Conclusions from Published Literature
-
(a)
India studies: Preliminary PCR-based assays have been conducted in India for Indian samples like Mycobacteria, Hepatitis, HIV and other bacterial and viral diseases. These will give us a lead in designing the primers. PCR-based tests have been developed in isolated laboratories working with specific microorganisms, but nowhere has a systematic study of multiple pathogens been carried out for detection of both the DNA and RNA. Furthermore, no studies have been carried out systematically for multiplex PCR.
-
(b)
International studies: Simple PCR-based assays are routinely used in labs abroad. However, since the strains are different in India, such tests need to be redesigned for Indian conditions. Below are a few examples of PCR-based assays done on bacterial cultures:
-
Tuberculosis: Genetic markers specific for Mycobacterium tuberculosis are well established and BioConsort has access to these primers. The positive results will look like the gel below (Fig. 5.1).
Fig. 5.1 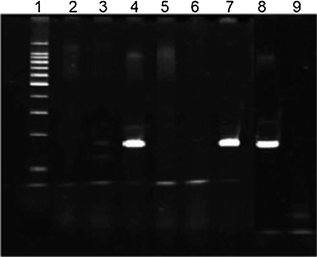
Detection of PCR products of IS6110 in direct BACTEC 12B cultures. Lanes—1 100 bp ladder marker; 2 negative control (water); 3 M. marinum; 4 M. africanum; 5 M. kansasii; 6 M. chelonae; 7 M. bovis; 8 M. tuberculosis H37Ra; 9 negative control (E. coli)
-
Hepatitis: This is the causative agent for Jaundice. It is difficult to distinguish between the B and the C types at an early stage of infection. However, they can be distinguished by PCR-based techniques.
-
Hepatitis B: This is a DNA virus and a straightforward test from the blood of the patient results in a single clean band.
-
Hepatitis C: This is the causative agent for Jaundice. It is an RNA virus, therefore, a Reverse Transcription-PCR needs to be done. A nested PCR might be necessary to get a clean band.
-

5.1.4 Preliminary Results from the Principal Investigator’s (PI) Laboratory
The PI has designed PCR-based assays for detection of M. tuberculosis Phosphate specific transporter gene that can be used to detect M. tuberculosis accurately. Similar assays will be developed for unique proteins of pathogens.
The PI has also designed an RT PCR assay for detection of a drug resistant strain of tuberculosis. The results of the same are illustrated in Fig. 5.2.

a Standardization of the PCR conditions to determine the optimal annealing temperature from degenerate primers for a phosphate specific transporter. Lanes—1 Marker; 2 50 °C; 3 55°C; 4 65 °C; 5 72 °C. b (i) Overexpression of the same gene. Lanes—1 Positive control; 4 Drug susceptible mycobacteria; 5 Drug resistant mycobacteria. (ii) Southern blot with the PCR amplified probe to demonstrate that the same gene is overexpressed
5.1.5 Research Design/Methods
The research methodology to be used is as follows:
-
1.
Designing PCR primers for identification of infectious diseases pathogens: This is the most important step in PCR-based diagnostics. The primers will be developed from unique sequences of the pathogens. As sequences in part or full are available in the gene bank database, primers will be designed from them. For multiplexing, multiple primers need to be designed to be used in a single reaction. Our lab has the expertise to design such primers while making sure that they do not self-anneal. Once the primers are ready, the PCR conditions will be standardized for the assays.
-
2.
Collection of blood and extraction of the genetic material: The genetic material will be extracted from 0.5 ml of the blood. Briefly, it will be spun down to pellet the cells and the plasma will be treated with chemicals to lyse the cells and free the genetic material. It will then be passed through a Qiagen QIAamp column (or a similar column procured from an Indian manufacturer and washed with the supplied buffer and precipitated with alcohol to get the DNA. PCR reaction will be set up using this DNA.
For RNA viruses, an additional step will be required. The RNA will be extracted in the same way as DNA and a reverse transcription reaction will be carried out. This will convert the RNA into cDNA and the PCR reaction will be carried out using this cDNA.
-
3.
PCR reaction: The PCR reaction will be carried out with either the DNA or the cDNA. The assay conditions will be standardized for the following conditions:
-
Annealing temperatures: A range of 55–72 °C will be used and the highest temperature giving a single band will be chosen. For multiplex PCR the conditions will be standardized again. However, it is assumed that since the primers will be exact matches of the DNA sequences, a temperature above 65 °C will give optimum results.
-
No of cycles: So as to reduce the number of cycles and time for the reaction, a 15 cycle, a 20 cycle, a 25 cycle and a 30 cycle reaction will be tried.
-
-
4.
Analyzing the results on an agarose gel: The results will be analysed on an agarose gel. The band size will be compared to a positive control kept for this purpose. A blank lane for the negative control will indicate a clean PCR reaction with no contamination. The composition of the gel and gel running conditions will be standardized so as to minimize the time and costs for the reaction.
-
5.
Validation of the assays: The assays will be validated against ELISA-based tests already available in the market. A sample size of 100 will be used for validation to test the reliability of the assay. Once the assays are validated, the know-how and the methodology for conducting the study will be out licensed.
We will develop and validate the following assays in a phase wise manner.
In Phase 1, the commercially important assays will be developed. They will be the following:
-
M. tuberculosis
-
Hepatitis B
-
Hepatitis C
Out of the three, the first two are DNA viruses and the third one is an RNA virus. So, both PCR and Reverse Transcriptase assays will be developed. As there is an urgent need for these assays they will be first assays to be developed. First simple PCR assays will be developed followed by multiplex PCR and nested PCRs if necessary.
Time and budget permitting, the following assays will also be attempted and the promising ones will be taken forward.
-
Hepatitis C virus (RNA)
-
Hepatitis E virus (RNA)
-
Plasmodium falciparum
-
Plasmodium vivax
-
Salmonella typhi
-
Vibrio cholerae.
Phase 2: As soon as the first phase of tests has been developed, we will introduce a new upcoming technology, a Rapid PCR for quick diagnostics of the infectious disease pathogens that can be used almost as a POC medicine. This will use the same reagents developed during the earlier assays with slight modifications. Phase 3: After the second year, newer rarer assays will be developed as per the needs of the industry in consultation with the physicians. Our lab will develop assays for the detection of a few of the following infectious agents:
-
Chlamydia pneumoniae
-
Clostridium botulinum
-
Mycoplasma pneumoniae
-
Neisseria gonorrhoeae
-
Dengue virus (RNA)
-
Japanese encephalitis virus (RNA)
-
Poliovirus (RNA)
-
Mumps virus (RNA)
-
Rabies virus (RNA)
-
Enteric adenovirus
-
Measles virus
-
Avian influenza virus (H5N1)
-
SARS coronavirus
-
Influenza virus (various forms)
-
Rotavirus (RNA)
-
5.1.6 Time Table for the Proposed Work
Year | Proposed plan |
|---|---|
Year 1 | 1. Setting up of the PCR lab and establishing collaborations with pathological labs for the supply of blood samples |
2. Developing PCR assays for Mycobacterium tuberculosis, Hepatitis B and Hepatitis C | |
3. Developing multiplex PCR assays for the above three pathogens to detect multiple markers for the same pathogen | |
Year 2 | 1. Development of the next set of assays for Plasmodium falciparum, Plasmodium vivax, Salmonella typhi and Vibrio cholera. The pathogens will be chosen based on the needs of the local market |
2. Development of multiplex assays to detect the presence of multiple pathogens in the same test | |
3. Out licensing of the assays to pathological labs if possible for commercialization | |
Year 3 | 1. Development of a fast PCR reaction to detect the presence of these pathogens in a fast reaction using the know-how gathered from the previous test. This test can be used for a point of care test |
2. Two additional tests for influenza viruses to be developed depending on the need. All tests developed will be multiplexed and put into the fast PCR format |
5.2 Sub-chapter B: Identification of Biomarkers for Differential Diagnosis of Allergic and Non-allergic Respiratory Diseases from Exhaled Breath Condensate
5.2.1 Introduction
Exhaled breath condensate (EBC) is the condensate of exhaled breath collected using a refrigerated device [1,2,3,4]. Various volatile molecules and water diffuse out of the cells lining the airspaces in the lung, the airways and the mouth. Analysis of exhaled breath also revealed the presence of non-volatile particles [4]. These droplets may be formed due to turbulence in the airways, changes in surface tension in the alveoli and airways or from the airway lining fluid (ALF). A collection of these gases in the exhaled air forms the EBC. EBC comprises of water vapour and a variety of volatile such as nitric oxide, carbon monoxide, and hydrocarbons and non-volatile (such as urea, GSH, leukotrienes, prostanoids, and cytokines) [1, 3] components. The composition of EBC is not completely understood.
Exhaled breath condensate (EBC) is increasingly gaining popularity in the field of lung diseases due to its non-invasive nature. Various oxidative stress markers and inflammatory mediators such as inflammatory cytokines, reactive oxygen/nitrogen species and oxidized glutathione may be estimated using EBC. Therefore it may be useful for detecting and discovering novel markers for different lung diseases. However, the small amount of EBC obtained from each patient poses a hurdle in its application for detection of various lung ailments. Moreover, its ability to replicate the ALF still remains to be tested. Standardization of use of EBC for diagnosis and comparison needs further optimization of the dilution factors to be used for different patients.
Lung ailments such as asthma and chronic obstructive pulmonary disease (COPD) involve inflammation of the airways and the lung [5]. Inflammation is currently assessed using invasive techniques such as bronchoscopy, bronchial biopsies, bronchoalveolar lavage (BAL) fluid analysis and sputum induction [6] or through serum and urine biomarkers which may reflect a systemic inflammation. This assessment assists in designing pharmacological therapy for patients and management of the disease. As mentioned previously, exhaled breath comprises of both volatile (e.g. nitric oxide, carbon monoxide and hydrocarbons) and non-volatile components [7, 8]. Nitric oxide (NO) measurement is a standardized method for assessing airway inflammation currently in asthma patients, not on glucocorticoids treatment. This measurement is useful for monitoring patient health and compliance to pharmacotherapy [9]. Use of EBC for such estimations will prove its clinical utility.
5.2.2 Experimental Setup
EBC collection can be performed using home-made or commercially available apparatus. The apparatus generally consists of a double walled glass container which is cooled on the inside using ice, liquid nitrogen or jacketed tubing. The collecting system consists of tubing connected to the glass container at one end and to the mouth piece at the other end. The patient is required to breathe out of their mouth, with a nose-clip on, through a mouth piece for 15 min. The EBC is collected in the double walled glass container in the outer container [7]. Depending on respiratory parameters, condenser surfaces, temperature and turbulence of airflow, 1–2.5 ml of EBC may be collected.
Various other commercially available EBC collection systems are available [10]. One such example is EcoScreen® (JaegerTonnies, Hoechberg, Germany). The design of the equipment is similar to a home-made device, apart from the ability to collect samples in a frozen state. This may be very useful when collecting volatile substance in EBC. However, if the temperature of the cooling apparatus fluctuates, it leads to collection of EBC in a mixed liquid–solid form. Such inconsistencies in EBC collection result in differences in concentrations reported in different studies. For analysis of multiple analytes, the collection vial needs to be replaced with smaller vials. For scaling-up operations, the cost of a condenser should also be considered. The EcoScreen® II can be used to assess respiratory parameters during collection or may be connected to a pneumotachograph and a computer to enable recording of respiratory parameters online [10]. Additionally, EcoScreen II is capable of collecting EBC from the airways or the alveoli in separate compartments/bags. This enables comparison of the EBC between the two in normal and diseased state. The surface of the collecting system (plastics vs. Teflon-coated metal) may also be more appropriate for the collection of compounds such as lipids. However, no published studies are available with this condenser.
The RTube® (Respiratory Research, Inc., Charlottesville, VA) is another commercially available portable condenser [11]. RTube® comprises a disposable polypropylene collecting system and an aluminium sleeve around it for refrigeration [11]. The temperature for cooling may be chosen by the user. Due to its portable nature, RTube® can be easily used in longitudinal studies where the measurement is required multiple times a day. Further, the polypropylene collecting bag can easily be stored in the refrigerator at home. However, the temperature in a home refrigerator (−20 °C) may differ from a laboratory freezer (−80 °C) which may result in loss of some volatile compounds. Its design also prevents salivary contamination [11]. It can also be used for determining pH of EBC using pHTube® (Respiratory Research, Inc., Charlottesville, VA) [11]. For pH measurement, sufficient volume may be collected in about a minute [11]. The collected EBC still needs to be taken to the laboratory for biochemical tests. Comparison of EBC collected from RTube and EcoScreen reported higher volumes of the condensate and detection of lipid and protein mediators in EBC collected from EcoScreen. Further studies to address this issue are required. Standardization of the sterilization protocol for EBC equipment is necessary to reduce cross contamination. Currently, the equipment is sterilized using an antibacterial solution such as sodium hypochlorite for 1 h followed by rinses with water. The effect of different collection material on the components of EBC is unknown. In EcoScreen the condenser is coated with Teflon® (E.I. du Pont de Nemours & Company, Inc., Washington, DE) to avoid loss of molecules by adhering to the service. Borosilicate glass coating was found to be better than silicone, aluminium, polypropylene and Teflon for albumin detection. These results suggest that the condenser material needs to be according to the molecules/compounds to be detected. Further use of separate sensors for simultaneous collection of different compounds such as hydrogen peroxide [12] and inflammatory mediators may be developed. Further effect of the antiseptic solutions used for cleaning and optimization of collection protocol to enable simultaneous collection of material is required (Figs. 5.3 and 5.4).

Overview of collection of exhaled breath condensate (EBC)

a Method for the collection of EBC. b Tube for the collection of EBC
5.2.3 Measurements of Mediators in EBC
EBC consists of both volatile and non-volatile compounds. Collection of EBC is performed according to standard guidelines which also assists in the development of new techniques for collection. Some issues which need to be considered include:
-
(1)
Temperature of the collection system which determines the collection of volatile compounds.
-
(2)
Volatile compounds may be lost due to sublimation.
-
(3)
Proper analysis of all the components to be analysed should be performed to optimize the duration of EBC collection, storage conditions and assay methods to be used for each.
-
(4)
Multiple assays should be performed for different compounds.
-
(5)
Due to lower concentrations of various compounds, attempts to increase concentration by lyophilization, freeze drying or dehydration may help in improving sensitivity.
-
(6)
Appropriate assay controls should be used to estimate the low concentrations of different compounds.
Oxygen and Nitrogen Reactive Species and Redox-Relevant Molecules in EBC
Reactive oxygen species (ROS) and reactive nitrogen species (RNS) are among the few biomarkers that can be detected by EBC. These are used in many lung disease studies. The formation of several RNS starts with nitric oxide (NO), which is a volatile component of EBC. NO is synthesized by nitric oxide synthase (NOS) from the amino acid arginine. The respiratory tract contains several different types of cells (airway epithelial cells, alveolar epithelial cells, macrophages, eosinophils, neutrophils, smooth muscle cells and mast cells) which contain NOS. A ROS, superoxide anion (\( {{\text{O}}_{2}}^{ - } \)), reacts with NO and forms the unstable and highly reactive peroxynitrite (ONOO–). The peroxynitrite anion aids in the nitrosation of tyrosine, or its residues, and forms 3-nitrotyrosine (3-NT), which can be measured by HPLC or MS. NO also reacts with thiols, like glutathione, cysteine, and protein thiol residues, to form S-nitrothioles (RS-NO). RS-Nos can be measured colourimetrically. NO is finally metabolized to nitrite (\( {{\text{NO}}_{2}}^{ - } \)) and nitrate (\( {{\text{NO}}_{3}}^{ - } \)).
Patients with asthma, be it adults [13] or children [14], have been found to have high levels of nitrites and nitrates in their EBC. One study showed that asthmatic adults treated with glucocorticoids had lower levels of nitrite/nitrates in their EBC as compared to patients not treated with steroids [13]. Nitrite concentrations in the EBC increase when asthma exacerbates [15] and in severe cases [16], nitrite and nitrate concentrations in EBC can be measured by assays (colourimetric, chemiluminescent, fluorimetric) or by chromatography (ion, gas or liquid).
Hydrogen peroxide (H2O2) is another volatile molecule in EBC. In several cell types, H2O2 can be produced by superoxide dismutase (SOD) through conversion of the superoxide anion. H2O2 can be released from both inflammatory and structural cells including neutrophils, eosinophils, macrophages, and epithelial cells. H2O2 can be detected in EBC but is probably more unstable than other oxidative stress markers like isoprostanes. Like the RNS, H2O2 is found to increase in people affected with asthma, COPD and ARDS. Treatment with montelukast did not have any effect on the H2O2 content in EBC of mildly asthmatic patients, whereas treatment with triamcinolone acetonide reduced the H2O2 content.
A limitation in the assessment of H2O2 in the EBC is its instability, which means that samples have to be collected fresh, and frozen for later assays. H2O2 is measured by assays (colourimetric, chemiluminescent and fluorimetric assays). Another biomarker of oxidative stress is malondialdehyde (MDA), which is formed from the degradation of polyunsaturated lipids by ROS. MDA present in EBC can be measured, in the range of 10 nM, by HPLC. Oxidative stress or inflammation in the respiratory tract leads to increase in ROS and RNS, which are used as indicators. Patients with asthma, COPD, cystic fibrosis or idiopathic pulmonary fibrosis (IPF) have high levels of H2O2, RS-NO, \( {{\text{NO}}_{2}}^{ - } \), \( {{\text{NO}}_{3}}^{ - } \), 3-NT and MDA in the EBC. Apart from these, the airway lining fluid (ALF) also has antioxidant compounds like cysteine (Cys) and Glutathione (GSH). EBC contains GSH in the magnitude of nM, as compared to bronchoalveolar lavage fluid (BALF) which contains GSH in the magnitude of µM.
5.2.4 Use of EBC in Inflammatory Diseases of the Lung
Assessment of EBC is a non-invasive technique used to sample the lower airways. Collection of EBC involves tidal breathing (inhalation & exhalation during restful breathing) into a collection device, which is chilled. The chilled collection device allows the water vapour in the EBC to condense and be collected. Quantitation of different mediators and factors can be done from the collected condensate. The mediators that are quantified originate from the epithelial lining fluid (ELF) that gets mobilized during expiration [17]. Different inflammatory mediators, from simple pro-oxidant molecules to larger proteins, are found in the EBC of patients with diseases like COPD, asthma and acute respiratory distress syndrome (ARDS). Despite being a promising and non-invasive technique, several questions have been raised regarding its methodologies that have delayed its adoption as a clinical technique. There is no standardized method for the collection of EBC, and different investigators have used collection devices ranging from Teflon tubing, convection cylinders and ice baths. Thus, before the use of EBC is mainstreamed, a standard method for collection must be determined. Nowadays, EBC collection devices, like RTubeTM from Respiratory Research, Inc., USA, and EcoScreen, from Viasys, are commercially available [10]. There is also the problem of dilution of EBC. The respiratory droplets get diluted, often as much as 10,000 folds, when they are collected in the water-saturated exhaled breath [17]. This poses a problem because mediators and soluble factors are already present at very low concentrations which can be detected by only few, very-sensitive tests. Detection is especially a problem in case of proteins, as they may not get aerosolized. This dilution may differ among test subjects, making it difficult to standardize the test. The American Thoracic Society, as well as the European Respiratory Society, have issued guidelines for the collection of EBC which have attempted to address the above-mentioned issues [18]. It has been suggested that standardization of the EBC mediators may be done by measuring the quantities of non-volatile cations in the EBC [17]. This is considered to give an idea about the degree of dilution, as cation levels in the ELF remain somewhat constant. However, for this method to work, the EBC has to be lyophilized and ammonia removed from it, which may lead to changes in the levels of the biomarkers. Regardless of these issues, EBC analysis has the potential to be a powerful technique for assessing the lung diseases.
5.2.5 Use of EBC in COPD
It has been seen in several studies that the EBC of patients with COPD is different from normal people, and the EBC profile changes with treatment. This shows that assessment of EBC can help in the diagnosis and treatment of lung diseases [10]. Mediators present in the EBC of COPD patients include hydrogen peroxide, hydrocarbons (like isoprostanes) and cytokines, of which H2O2 is the most studied.
-
Hydrogen peroxide (H 2 O 2 ): H2O2 is derived from the superoxide radical that is produced by neutrophils in the airways, and is a marker for oxidative stress and underlying inflammation of the airway. EBC of COPD patients have higher levels of H2O2 compared to healthy controls, and the levels further rise with exacerbation of the disease [19]. The H2O2 levels, measured by EBC, can be correlated with the severity of the disease measured by the FEV1/FVC ratio [19]. H2O2 levels in the EBC of COPD patients can be reduced by n-acetylcysteine, an antioxidant. Further studies are needed to determine the effects of H2O2 in COPD. H2O2 can be used as a biomarker for the diagnosis of COPD, as an indicator of neutrophilic inflammation, since neutrophils are predominant in the airways in COPD [19]. Also, measurement of H2O2 in EBC can be done easily using inexpensive chemicals.
-
Isoprostanes: Isoprostanes are prostaglandin-like compounds that are formed by the free radical-catalyzed peroxidation of essential fatty acids, like arachidonic acid, without the action of the enzyme cyclooxygenase (COX). Chemically stable, and formed in vivo, they are considered to be markers of lipid peroxidation and oxidative stress in humans. Of the isoprostanes, 8-isoprostane has been thoroughly studied as a marker for oxidative stress in human lung diseases. It may be important in the development of COPD. Several studies have shown that the levels of 8-isoprostane are higher in the EBC of COPD patients than in normal healthy controls [10, 19]. Its levels have been found to increase with exacerbation of the disease. However, measurement of pulmonary function with FEV1/FVC showed no correlation between pulmonary function and 8-isoprostane [10, 19]. COPD patients who are also smokers have higher levels of 8-isoprostane than non-smoking COPD patients [10]. Thus, it can be used as a marker for underlying inflammation of the airways. Isoprostane can be measured using a commercial immunoassay kit.
-
Other mediators: Other markers of oxidative stress, like aldehydes, have been found in EBC, but their instability and lack of specificity limit their use clinically. EBC of COPD patient has a lower pH than normal, and thus, can be used as a marker for airway inflammation [19]. Cytokines are also found in the EBC, but in very low levels (in the range of pg/ml). The level of interleukin 6 (IL-6) was found to be higher in COPD patients.
The range of markers found in the EBC of COPD patients shows the potential of EBC as a tool for diagnosis and/or treatment of COPD.
5.2.6 Use of EBC in Asthma
Several markers have been detected in the EBC of asthma patients, including H2O2, leukotrienes (LTs) and 8-isoprostane. Another factor that is considered as a marker is pH.
-
Hydrogen peroxide (H 2 O 2 ): EBC of heavy smokers and patients with severe asthma has been found to have high levels of H2O2. H2O2 levels in the EBC of patients with severe allergic asthma show an inverse correlation to pulmonary function, as measured by the FEV1/FVC test. Anti-inflammatory therapy of asthma patients has shown an improvement in the FEV1/FVC, along with a decline in the H2O2 levels.
-
Eicosanoids: Eicosanoids are a group of compounds including prostaglandins and related compounds, most of which are formed from arachidonic acid. Leukotrienes (LTs) and 8-isoprostanes, which are eicosanoids, can be measured in the EBC by enzyme immunoassays or by GC/MS (gas chromatography/mass spectrometry). Cysteinyl leukotrienes (Cys-LTs) have been found in the EBC of asthmatic patients, the levels of which seem to be correlated with the severity of the disease, and are found to be reduced by anti-inflammatory drugs. 8-isoprostane is also found in the EBC of asthmatic patients and is correlated with the disease-severity. However, levels of 8-isoprostane do not get completely suppressed by treatment with corticosteroids, and maybe indicative of airway inflammation.
-
pH: Several studies have found that the EBC of asthmatic patients had a pH of 7.5, which is lower than the normal pH of 7.8. Exacerbations of the disease lead to a further decrease in the pH, which was restored with corticosteroid treatment. The advantages of using pH as a marker in EBC includes low costs of collection, good reproducibility and availability of standard references.
-
Exhaled nitric oxide (eNO): Exhaled nitric oxide (eNO) is considered a sensitive marker for airway inflammation, especially in allergic asthma. Higher levels of eNO can indicate exacerbation of the disease. It can also indicate a loss of asthma control. A correlation has been found between the levels of eNO and allergen challenges, especially late asthmatic response (LAR).
5.2.7 Use of EBC in Allergic Rhinitis
Allergic rhinitis, or hay fever, is an inflammation of the nose that occurs when the immune system reacts to allergens in the air. The EBC of people with allergic rhinitis also contains several mediators which can be used as a marker for the disease. Just like EBC of asthmatics have eNO, EBC of people suffering from allergic rhinitis contains nasal nitric oxide (nNO). Standard techniques have been developed for measurement of NO in the airways. Currently, nNO is measured using the portable analyzer, MINO, and the results have been validated against results from standard chemiluminescent assays. Thus, this technique, which is non-invasive, easy and quick, can be used as a tool for diagnosis. Generally, nNO levels range from 400 to 900 parts per billion (ppb). Paranasal sinuses produce high levels of nNO (up to 25 ppm) by the action of inducible nitric oxide synthases (iNOS) of the epithelium. It has been seen that when an inhibitor of NOS is administered to a healthy individual, the nNO levels drop, leading to inflammation of the sinus.
5.2.8 Future Scope of Development
It is evident that EBC contains several molecules that may be considered to be biomarkers, and the marker-profile of EBC varies with the type of disease and its severity. It is now imperative that techniques for collection of EBC and its measurement be standardized. This is a tough ask as each marker differs in stability, solubility, volatility and concentration. As a result, no one technique is enough for the measurement of the different molecules. Presently, one main limitation of EBC measurement is the very low concentration of some biomarkers, thus limiting their measurement due to assays which are not sensitive enough. It is possible that, as potent antibodies are developed, more sensitive assays will also ensue.
H2O2 can be easily detected in real time using electrodes coated with horseradish peroxidase. Other similar enzyme-based assays may be developed for the lipid mediators, like the 8-isoprostane. Molecular biosensors may be developed which can detect the very low concentrations of certain molecules. Disposable detector sticks may also be developed that can help collect the EBC and monitor its profile.
Clearly, EBC is a novel technique which has great potential in the non-invasive diagnosis and treatment of various lung diseases, especially inflammatory diseases like asthma, COPD and rhinitis.
References
Horváth I, Hunt J, Barnes PJ et al. (2005) Exhaled breath condensate: methodological recommendations and unresolved questions. Eur Respir J 26(3):523–548
Hunt J (2007) Exhaled breath condensate—an overview. Immunol Allergy Clin N Am 27(4):587–596
Montuschi P (2007) Analysis of exhaled breath condensate in respiratory medicine: methodological aspects and potential clinical applications. Ther Adv Respir Dis 1(1):5–23
Davis MD, Montpetit A, Hunt J (2012) Exhaled breath condensate: an overview. Immunol Allergy Clin N Am 32(3):363–375
Sabroe I et al (2007) Targeting the networks that underpin contiguous immunity in asthma and chronic obstructive pulmonary disease. Am J Respir Crit Care Med 175:306–311
Berlyne GS et al (2000) A comparison of exhaled nitric oxide and induced sputum as markers of airway inflammation. J Allergy Clin Immunol 106:638–644
Montuschi P et al (2005) Liquid chromatography/mass spectrometry analysis of exhaled leukotriene B4 in asthmatic children. Respir Res 19(6):119
Kharitonov SA, Barnes PJ (2006) Exhaled biomarkers. Chest 130:1541–1546
Smith AD et al (2005) Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. N Engl J Med 352:2163–2173
Montuschi P et al (2000) Exhaled 8-isoprostane as an in vivo biomarker of oxidative stress in patients with COPD and healthy smokers. Am J Respir Crit Care Med 162:1175–1177
Hunt J (2002) Exhaled breath condensate: an evolving tool for non-invasive evaluation of lung disease. J Allergy Clin Immunol 110:28–34
Gajdocsi R et al (2003) The reproducibility and accuracy of the on-line hydrogen peroxide bioassay and the decreasing effect of storage on H2O2 concentration. Eur Respir J 22(Suppl. 45):279s
Ganas K et al (2001) Total nitrite/nitrate in expired breath condensate of patients with asthma. Respir Med 95:649–654
Ratnawati R et al (2006) Exhaled breath condensate nitrite/nitrate and pH in relation to pediatric asthma control and exhaled nitric oxide. Pediatr Pulmonol 41:929–936
Hunt J et al (1995) Condensed expirate nitrite as a home marker for acute asthma. Lancet 346:1235–1236
Corradi M et al (2001) Increased nitrosothiols in exhaled breath condensate in inflammatory airway diseases. Am J Respir Crit Care Med 163:854–858
Effros RM et al (2003) A simple method for estimating respiratory solute dilution in exhaled breath condensates. Am J Respir Crit Care Med 168:1500–1505
Horvath I et al (2005) Exhaled breath condensate: methodological recommendations and unresolved questions. Eur Respir J 26:523–548
Kostikas K et al (2003) Oxidative stress in expired breath condensate of patients with COPD. Chest 124:1373–1380
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2017 Springer Nature Singapore Pte Ltd.
About this chapter
Cite this chapter
Banerjee, E.R. (2017). Pharmacogenomics and Molecular Diagnostics. In: Perspectives in Translational Research in Life Sciences and Biomedicine. Springer, Singapore. https://doi.org/10.1007/978-981-10-5870-7_5
Download citation
DOI: https://doi.org/10.1007/978-981-10-5870-7_5
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-5869-1
Online ISBN: 978-981-10-5870-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)