
Abstract
Rectal adenocarcinoma accounts for about 30 % of colorectal cancers. The most common type of rectal cancer is adenocarcinoma, which is a cancer arising from the mucosa. Because of its specific anatomical location, this cancer poses two specific problems in terms of treatment that are the sphincter preservation and locoregional recurrences. The latter depends mainly on the depth of involvement of the rectal wall and mesorectum and of the lymph node involvement.
Keywords
- Rectal Prolapse
- Rectal Wall
- Circumferential Resection Margin
- Pelvic Floor Dysfunction
- Sphincter Preservation
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Rectal Carcinoma
Rectal adenocarcinoma accounts for about 30 % of colorectal cancers. The most common type of rectal cancer is adenocarcinoma, which is a cancer arising from the mucosa. Because of its specific anatomical location, this cancer poses two specific problems in terms of treatment that are the sphincter preservation and locoregional recurrences. The latter depends mainly on the depth of involvement of the rectal wall and mesorectum and of the lymph node involvement.
-
Symptoms of rectal carcinoma typically include rectal bleeding and anemia which are sometimes associated with weight loss.
-
The indication for treatment is based on the initial assessment of imaging including endorectal ultrasonography, thoraco-abdominopelvic CT, and rectal MRI. The aim of imaging is to identify groups of patients with different risk of recurrence and to choose the most appropriate treatment. It must respond more specifically to three questions:
-
What is the exact location of the tumor and the distal margin between the lower pole of the tumor and the sphincter? Its importance is crucial in reaching the lower rectal tumors to assess the possibilities of conservative treatment and thus the potential to preserve continence. Sphincter preservation is possible if you have a distal margin of at least 1 cm.
-
What is the stage and the circumferential resection margin? The lateral extension of the tumor is now considered the main risk factor for local recurrence.
-
What are the tumor N (nodal) and M (metastases) staging?
-
-
Rigid sigmoidoscopy, corresponding to the insertion of a rigid optical scope inserted through the anus, is usually performed and allows obtaining biopsy specimen and a more exact measurement of the tumor’s distance from the anus than flexible sigmoidoscopy. Low, middle, and upper rectal tumors are localized between 0 and 5 cm, 5 and 10 cm, and 10 and 15 cm from the anal margin, respectively. The tumor will be also located in relation to the pouch of Douglas. It is also important to specify the location of the tumor in the axial plane and whether the invasion is circumferential or localized.
-
Endorectal ultrasonography is presently the most accurate imaging modality for visualization of the layers of the rectal wall and for the assessment of tumor ingrowth into rectal wall layers with accuracies for T staging varying between 69 and 97 %. However, its sensitivity was shown to be affected by T stage and is higher for staging of superficial rectal tumors (T1 and T2) than for staging of advanced rectal cancer. Moreover, it has a limited value to visualize the mesorectal fascia and to assess the distance from the tumor to this fascia that is, at present, considered to be the most powerful predictor of local recurrence rate.
-
MRI has become a complementary tool for the determination of circumferential resection margin particularly useful in the staging of T3 and T4 and to assess the rectal sphincter in tumor of the low rectal cancer. Technically, rectal MRI is based on T2 sequences in the three spatial planes (sagittal, coronal, and oblique axial perpendicular to the long axis of the tumor) without fat saturation to obtain a good contrast between the tumor and the mesorectal fat. Most staging failures with MR imaging occur in the differentiation of T2-stage and borderline T3-stage lesions. Overstaging is often caused by desmoplastic reactions, and it is difficult to distinguish on MR images between spiculation in the perirectal fat caused by fibrosis alone (stage pT2) and spiculation caused by fibrosis that contains tumor cells (stage pT3). Finally for low rectal tumors, it is necessary to evaluate the sphincter complex composed of the levator ani muscle, with a beam ileococcygeal and beam puborectalis, and external and internal sphincters of the anal canal (Fig. 1). This sphincter complex is well depicted using MRI. The levator ani muscle and the external sphincter consist of striated fibers hypointense on T2 sequence, whereas the internal sphincter is a smooth muscle layer following the internal rectal muscularis that strongly enhanced after injection of contrast material.
Fig. 1 
Rectal adenocarcinoma: Coronal T2-weighted MR image shows a low rectal mass involving the ileococcygeal beam of the levator ani muscle (arrow)
Metastatic lymph nodes must be looked for above the level of the tumor. The evaluation of lymph node by imaging is based on morphologic criteria of size and appearance of the lymph nodes. Currently diameters of 5 mm for the mesorectum location and 7 mm for internal iliac location are retained as threshold values for malignant lymph nodes.
Imaging is also useful to assess response to chemoradiation assessment treatment. MRI is considered as the imaging modality of choice and should be performed 6–8 weeks after the end of treatment. A decrease in T2 signal and volume reduction ≥70 % are the signs that are better correlated with histological response and progression-free survival. MR diffusion-weighted sequences improve the performance of MRI to identify tumor remnants and to select the complete response (Fig. 2).
Fig. 2 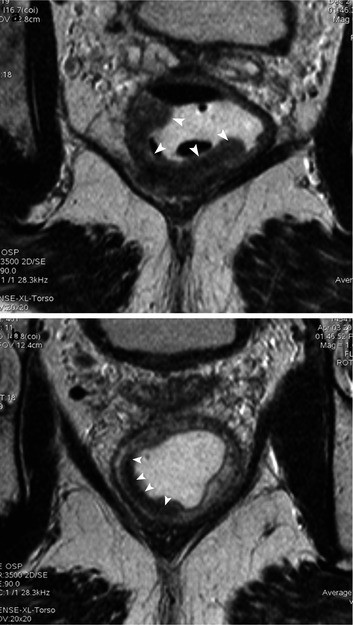
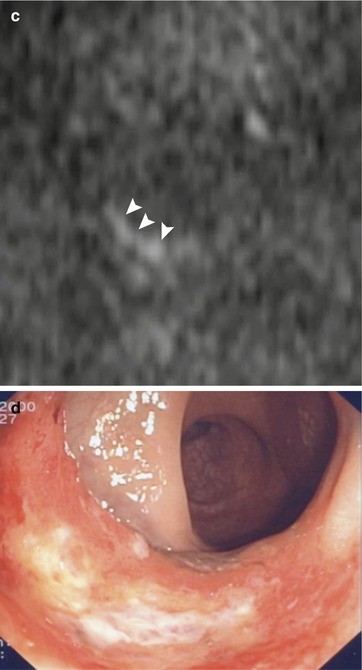
Rectal adenocarcinoma (arrowheads) prior (a) and after neoadjuvant chemoradiation (b). T2-weighted images depict tumor shrinkage in a patient with complete clinical response. After neoadjuvant chemoradiation, scarring tissue is visible in the tumoral bed (low signal intensity on T2-weighted image and poor signal on heavily diffusion-weighted image) (c). (d) shows the endoscopic features of mucosal scarring tissue after neoadjuvant therapy
-
Neoadjuvant chemoradiotherapy is currently used prior to surgery in rectal carcinoma with mesorectal fascia involvement or with tumor margin close to the mesorectal fascia and mesorectal suspected lymph nodes. Neoadjuvant cht-RTX leads to a complete clinical response in about 30 % of patients.
-
The assessment of complete clinical response requires combination of endoscopy and imaging. DW MR imaging in combination with conventional T2-weighted sequence seems to be a promising tool in differentiating between partial response and complete clinical response. In patients with complete clinical response to neoadjuvant therapy, minimal invasive treatment as TEM or wait-and-watch policy have been recently proposed instead of conventional TME; however, these alternative approaches do not reach a complete consensus among the surgical community and are still under clinical investigation.
The postoperative assessment is based on CT as well as MRI and 18F-FDG PET in cases of difficulties due to fibrotic radiation therapy changes.



Rectal Prolapse
-
Rectal prolapse refers to a wide spectrum of conditions characterized by the prolapse of the rectum with respect to its anatomical position associated often with pelvic floor dysfunction. Different types of rectal prolapse can be categorized:
-
Full-thickness rectal prolapse
-
Mucosal rectal prolapse
depending on the rectal wall layers involved in the prolapse.
Moreover other subclassification is possible considering the degree of prolapse:
-
External prolapse
-
Internal prolapse
depending in the rectal wall or the prolapsing mucosa is pulled out of the anus or not during evacuation and straining or at rest.
Moreover a variant of rectal prolapse is represented by rectal intussusception (either external or internal–occult intussusception). In case of intussusception a proximal prolapsing rectal segment telescopes into a distal rectal segment leading to severe obstruction during defecation. The intussusception can be devised in rectorectal or rectoanal intussusception depending on the segment that hosts the intussuscipiens, the prolapsing rectal segment.
Rectal prolapse is often associated with rectocele formation and other pelvic organ prolapse (cystocele, colpocele, enterocele) depending on the overall pelvic floor dysfunction.
-
-
Symptoms are represented by various combinations of obstructed defecation, fecal incontinence, hemorrhoids, and rectal ulceration associated sometimes with urinary incontinence.
Hemorrhoids are quite common in case of rectal prolapse. Recent theory on hemorrhoid pathogenesis postulates that the primum movens of hemorrhoid formation is represented by the presence of redundant and prolapsing rectal mucosa; therefore, one of the modern treatments proposed to care for hemorrhoids as well as rectal prolapse is represented by STARR (stapled transanal rectal resection).
-
Imaging plays a role in defining the type and degree of rectal prolapse and the overall pelvic floor dysfunction with relevant impact on patient management considering the different surgical options (STARR, laparoscopic ventral rectopexy, levatorplasty, perineal rectosigmoidectomy with Delmore repair) or possible conservative treatment (dietary prescription and biofeedback training).
-
MR defecography represents modern imaging; however, the conventional X-ray defecography still has a role in the accurate assessment of mucosal prolapse.
Rectocele
-
Rectocele is defined as bulging or outpouching of the rectal wall during defecation. Usually rectocele involves the anterior rectal wall, and it is common in women (especially after hysterectomy). In anterior rectocele the anterior rectal wall bulges through the rectovaginal septum into the posterior vaginal wall, and it is visible at physical examination. Rectocele is often associated with pelvic floor dysfunction, rectal prolapse, and obstructed defecation syndrome. Rectocele size consists in the measurement of anteroposterior depth of convex wall protrusion extending beyond the expected margin of normal rectal wall: small rectocele (<2 cm), moderate rectocele (2–4 cm), and large rectocele (>4 cm).
-
MR defecography represents an accurate radiation-free imaging modality for pelvic floor dysfunction and rectocele measurements (Fig. 3).
Fig. 3 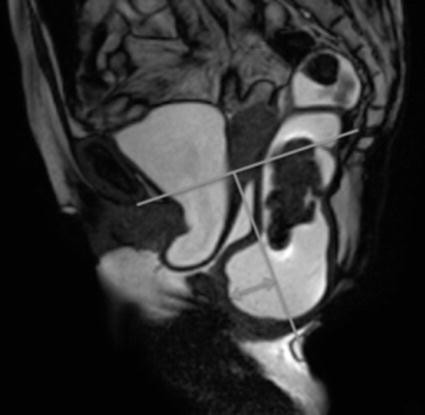
MR defecography image acquired during defecation phase showing descending perineum with respect to the pubococcygeal line. Anterior rectocele is clearly visible as an anterior bulging of the rectal wall. Double-arrow line indicates how to measure rectocele width

Suggested Reading
Beets-Tan RG, Beets GL, Vliegen RF, Kessels AG, Van Boven H, De Bruine A, von Meyenfeldt MF, Baeten CG, van Engelshoven JM (2001) Accuracy of magnetic resonance imaging in prediction of tumour-free resection margin in rectal cancer surgery. Lancet 357(9255):497–504
Brown G, Richards CJ, Bourne MW, Newcombe RG, Radcliffe AG, Dallimore NS, Williams GT (2003) Morphologic predictors of lymph node statue in rectal cancer with use of High-spatial-resolution MR Imaging with histopathologic comparison. Radiology 227(2):371–377
Iafrate F, Laghi A, Paolantonio P, Rengo M, Mercantini P, Ferri M, Ziparo V, Passariello R (2006) Preoperative staging of rectal cancer with MR Imaging: correlation with surgical and histopathologic findings. Radiographics 26(3):701–714
MERCURY Study Group (2007) Extramural depth of tumor invasion at thin-section MR in patients with rectal cancer: results of the MERCURY study. Radiology 243(1):132–139
Ptok H, Ruppert R, Stassburg J, Maurer CA, Oberholzer K, Junginger T, Merkel S, Hermanek P (2013) Pretherapeutic MRI for decision-making regarding selective neoadjuvant radiochemotherapy for rectal carcinoma: interim analysis of a multicentric prospective observational study. J Magn Reson Imaging 37(5):1122–1128
Seynaeve P, Billiet I, Vossaert P, Verleyen P, Steegmans A (2006) MR imaging of the pelvic floor. JBR 89:182–189
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Italia
About this chapter
Cite this chapter
Paolantonio, P., Dromain, C. (2014). R. In: Imaging of Small Bowel, Colon and Rectum. A-Z Notes in Radiological Practice and Reporting. Springer, Milano. https://doi.org/10.1007/978-88-470-5489-9_18
Download citation
DOI: https://doi.org/10.1007/978-88-470-5489-9_18
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-5488-2
Online ISBN: 978-88-470-5489-9
eBook Packages: MedicineMedicine (R0)