
Abstract
Newborns may present with vague signs and symptoms that result from a large variety of aetiologies.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others



Keywords
- Biliary Atresia
- Congenital Adrenal Hyperplasia
- Toxic Megacolon
- Duodenal Atresia
- Meconium Aspiration Syndrome
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
FormalPara Key Points-
Neonatal Resuscitation Program (NRP) guidelines should be employed for management of a newborn in distress [1].
-
Always consider nonaccidental trauma in newborns presenting to the emergency department (ED).
-
Prognosis is often dependent on the underlying aetiology or degree of illness.
-
Overall, early recognition and management will improve long-term outcome.
Section A: Common Assessment and Treatment Elements
Introduction
Newborns presenting with respiratory illness should be evaluated promptly as respiratory failure can precipitate quickly. There are many aetiologies of respiratory illness in the newborn period, of which the most common will be reviewed.
Pathophysiology
-
Respiratory distress syndrome (RDS) is caused by insufficient surfactant production, most commonly in preterm infants.
-
Insufficient surfactant causes inappropriate alveolar expansion.
-
Decreased alveolar expansion leads to respiratory distress.
-
-
Bronchiolitis is the result of a viral infection affecting the lower respiratory tree.
-
Bronchioles become inflamed and increase secretion production.
-
Common viral aetiologies include respiratory syncytial virus, human metapneumovirus, rhinovirus, enterovirus, and coronavirus [2].
-
-
Meconium aspiration syndrome (MAS) results from aspiration of meconium at the time of delivery.
Clinical Features
-
Initial signs of respiratory distress include tachypnoea and increased work of breathing (Table 11.1)
Table 11.1 Signs of respiratory distress versus respiratory failure -
As distress progresses, newborns are at risk of developing respiratory failure and apnoea.
-
RDS presents in the first days of life (Table 11.2)
Table 11.2 Comparison of clinical features and management of RDS and bronchiolitis -
Bronchiolitis is a clinical diagnosis based on physical exam and history [3].
-
Newborns will have increased work of breathing with crepitations and rhonchi on exam.
-
Differential Diagnosis
-
Consider RDS, bronchiolitis, sepsis, bronchopulmonary dysplasia (BPD), pulmonary hypertension, pneumonia, MAS, and pertussis.
-
History of meconium presence in amniotic fluids should raise concern for MAS.
-
When considering pulmonary hypertension, conduct thorough cardiac evaluation.
Investigations
-
Chest radiograph (CXR) should be obtained in patients suspected to have RDS, pneumonia, and foreign body aspiration (Table 11.3).
Table 11.3 Chest x-ray findings in common newborn respiratory diseases -
CXR is not indicated in patients with bronchiolitis [3].
-
Obtain nasal secretions to confirm pertussis infection.
-
If suspected, infectious workup should be completed including blood, urine, and cerebrospinal fluid studies (CSF).
Treatment
-
Intervention can be tailored to a degree of respiratory distress (Table 11.4).
Table 11.4 Recommended interventions based on level of respiratory distress -
Surfactant should be provided to patients with RDS [4].
-
Supportive care, including suctioning and supplemental oxygen, is the treatment of choice for bronchiolitis.
-
Salbutamol, normal saline, and hypertonic saline nebulisers have not been shown to improve outcome in bronchiolitis [3].
-
-
For patients without clear viral aetiology, consider antibiotic coverage.
-
If suspicious for pertussis, start prophylactic antibiotics.
Prognosis
-
Newborns in respiratory distress will require observation and treatment on an inpatient service.
-
Newborns with severe RDS are at risk of requiring long-term supplemental oxygen and developing BPD.
-
Bronchiolitis has an overall good prognosis with resolution of symptoms once the virus infection resolves.
Prevention
-
Prevention of bronchiolitis focuses on reducing virus transmission.
-
Avoidance of preterm delivery unless clinically indicated will decrease the risk of RDS.
Section B : Neonatal Cardiac Emergencies
Introduction
Congenital cardiac deformities may present in the first hours to days to weeks of life. Prompt recognition of a cardiac aetiology is imperative, as management from cardiogenic shock differs from management of other aetiologies of newborn shock.
Pathophysiology
-
Congenital heart defects are a result of abnormal embryogenesis
-
Defects can be classified as cyanotic (Table 11.5) and non-cyanotic (Table 11.6).
Table 11.5 Characteristics of cyanotic heart lesions Table 11.6 Non-cyanotic heart defects -
Cyanosis is a result of right to left shunting of non-oxygenated blood into systemic circulation.
Clinical Features
-
Newborns may present with a variety of findings (Table 11.7).
Table 11.7 Possible clinical features associated with congenital heart disease
Differential Diagnosis
-
Serious bacterial infection (SBI) should be considered in all neonates presenting to the ED.
-
Metabolic abnormalities, respiratory infections, and feeding difficulties can present similarly.
Investigations
-
Assess colour of the newborn and central/peripheral pulses (Fig. 11.1).
Fig. 11.1 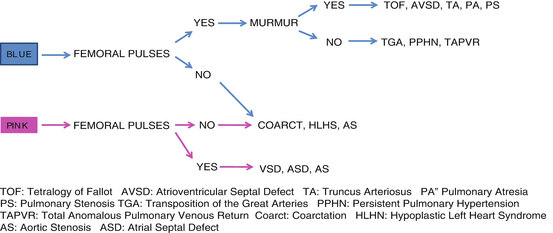
Assessment of infant colour and central pulses
-
Measure four extremity blood pressures and pulse oximetry.
-
In the setting of coarctation, lower extremity blood pressures and pulse oximetry will be decreased compared to right upper extremity.
-
-
CXR should be obtained to assess the cardiac silhouette.
-
Obtain electrocardiogram to assess for rhythm disturbances.
-
Echocardiogram is used to assess cardiac anatomy and function.
-
Consider blood gas to assess pH and arterial oxygenation.
-
Detailed maternal and prenatal history, including ultrasound results, should be gathered.
-
Many maternal conditions and medications can be associated with congenital heart disease [5].
-

Treatment
-
Supplemental oxygen should be provided.
-
Haemodynamic support should be provided with fluids, inotropes, and chronotropes as clinically indicated.
-
The degree of fluid resuscitation is dependent on the underlying cardiac defect.
-
-
Prostaglandins should be initiated to delay closure of the ductus arteriosus in patients suspected of having a shunt-dependent defect.
-
Initial dose – Prostaglandin E1: 0.05 mcg/kg/min
-
-
Initiate inhaled nitric oxide if pulmonary hypertension is suspected.
-
Cardiology consult should be obtained as soon as cardiac defect is suspected.
Prevention
-
Improved management of maternal diabetes and hypertension may decrease congenital heart defects.
Section C: Serious Bacterial Infections (SBI)
Introduction
Any newborn with concern for infectious process should be evaluated and treated immediately. SBIs in neonates include, but not limited to, urinary tract infections (UTIs), bacteraemia, sepsis, meningitis, pneumonia, pyelonephritis, and cellulitis. Neonates with bacterial infection are at high risk for long-term morbidity and mortality [6]. Low threshold for workup of an SBI should be maintained when evaluating children less than 29 days old.
Pathophysiology
-
Newborns have reduced defence against bacterial infections secondary to an immature immune system.
-
The two most common bacteria responsible for infection in newborns are group B streptococcus (GBS) and Escherichia coli (E. coli) [7].
-
UTIs are the most common bacterial infection in this patient group.
-
Necrotising enterocolitis (NEC) is a result of intestinal ischaemia, leading to bacterial overgrowth and gut necrosis [8].
Clinical Features
-
Rectal temperature greater than 38° C is suggestive of infection.
-
Infants may present with hypothermia, lethargy, increased sleeping, poor feeding, jaundice, vomiting, changes in their respiratory pattern, or abnormal vital signs.
-
Detailed prenatal and antenatal history should be obtained.
-
Risk factors for infection include prolonged rupture of membranes, maternal fever, maternal infection, and lack of appropriate treatment for maternal GBS.
-
-
Abdominal tenderness, distension, vomiting, bloody stool, and lethargy may indicate NEC.
-
Redness, tenderness, or drainage from the umbilicus is concerning for omphalitis.
Differential Diagnosis
-
Consider hypoglycaemia, metabolic dysfunction, hyperbilirubinemia, congenital heart conditions, and neurologic dysfunction when assessing a patient with the above features.
Investigations
-
Workup should include CBC, blood culture, urinalysis, urine culture, and CSF studies including cell count, differential, glucose, protein, and culture.
-
Consider obtaining herpes simplex virus (HSV) tests.
-
In the setting of omphalitis, send culture of umbilical discharge.
-
Obtain cultures prior to antibiotic initiation unless patient is clinically decompensating.
-
For patients with dehydration or concern for metabolic abnormalities, obtain electrolytes and liver function panel.
-
CXR should be considered in newborns with respiratory distress, and hypoxia.
-
NEC diagnosis and management is reviewed in Table 11.11 [9].
Treatment
-
Prompt antibiotic therapy is essential.
-
Initiate broad-spectrum antibiotic coverage with ampicillin and gentamicin and/or cefotaxime.
-
Continue antibiotics until CSF, blood, and urine cultures have resulted.
-
NEC management is reviewed in Table 11.11.
Prevention
-
Appropriate treatment of maternal GBS infections reduces the likelihood of newborn infection [11].
Section D: Newborn Gastrointestinal Emergencies
Introduction
There are a variety of gastrointestinal (GI) emergencies that may present in the newborn period. The majority of diagnoses can be distinguished based on physical exam and radiologic evaluation. Omphalocele and gastroschisis are not discussed in depth, but ED physicians should be aware of these complications.
Hyperbilirubinemia
Pathophysiology
-
Most newborns develop clinical hyperbilirubinemia [12].
-
Most cases of hyperbilirubinemia are physiologic, or secondary to normal delayed conjugation and excretion of bilirubin in the newborn, though pathologic aetiologies must be considered.
-
Factors contributing to higher bilirubin levels are listed in Table 11.8.
Table 11.8 Risk factors for hyperbilirubinemia -
Patients can be classified into low risk, medium risk, or high risk for complications of bilirubin (Table 11.9) [12].
Table 11.9 Classifying newborns into risk category based on age and number of risk factors
Clinical Features
-
Newborns with hyperbilirubinemia will appear jaundiced and may have decreased activity and desire to feed.
-
Jaundice occurs in a cranial to caudal progression and presents within the first week of life, with peak from day 3 to 5.
-
Jaundice presenting within the first 24 h of life is likely pathologic.
Differential Diagnosis
-
Consider underlying genetic abnormalities, including Gilbert, Crigler-Najjar, and Dubin-Johnson, when diagnosing unconjugated hyperbilirubinemia.
-
Also consider causes of elevated direct/conjugated bilirubin, including biliary atresia.
-
Infection and sepsis can lead to increased bilirubin levels.
Investigations
-
Laboratory workup will demonstrate elevated unconjugated bilirubin levels.
-
Consider blood type testing, direct bilirubin level, complete blood count, blood smear, liver function panel, and infectious workup.
Treatment
-
Treatment for hyperbilirubinemia is based on age, risk factors, and level of bilirubin (Table 11.10).
Table 11.10 Trigger levels of total serum bilirubin for phototherapy and exchange transfusion in infants 35 weeks or greater [12] -
The goal of treatment is to prevent encephalopathy secondary to bilirubin deposition in the brain or kernicterus [12].
-
Initial intervention includes oral hydration, intravenous (IV) hydration, and phototherapy.
-
For high-risk cases or concern for kernicterus, exchange transfusion is employed [12].
Prognosis
-
Overall prognosis of hyperbilirubinemia is very good [12].
-
The incidence of kernicterus is declining with the advent of phototherapy and exchange transfusion, though patients with kernicterus continue to have long-term neurologic morbidities [12, 13].
Prevention
-
Prevention of hyperbilirubinemia focuses on appropriate hydration of the newborn and appropriate treatment of maternal infections at the time of delivery.
-
Awareness of risk factors will assist in early recognition and intervention.
-
Kernicterus is an entirely preventable disease though not reversible [12].
Duodenal Atresia
Pathophysiology
-
Duodenal atresia occurs when there is an occlusion of the duodenum, restricting passage of materials through the small bowel.
-
Overall incidence is reported at 1 in 6,000 births [14]
-
This diagnosis is highly associated with trisomy 21.
Clinical Features
-
Patients will present in the first days of life with bilious vomiting.
-
Physical exam may reveal a scaphoid abdomen.
-
Newborn may pass meconium but is unlikely to have any bowel movements.
-
Prenatal history is often positive for polyhydramnios.
Differential Diagnosis
-
Infection, oesophageal atresia, tracheaoesophageal fistula, pyloric stenosis, and reflux should be considered.
-
Vomiting in the setting of duodenal atresia is bilious in nature, distinguishing this diagnosis from many others.
Investigations
-
Abdominal x-ray will reveal a double bubble sign indicating trapped air in the stomach and proximal duodenum.
-
Electrolytes, including glucose, should be obtained to assess hydration and nutritional status.
Treatment
-
Management of duodenal atresia is reviewed in Table 11.11.
Table 11.11 Characteristics of duodenal atresia, Hirschsprung’s disease, and necrotizing enterocolitis
Prognosis
-
Complications may include dependence of parenteral nutrition, poor growth, perforation of the duodenum, and stricture at the site of anastomosis [15].
Hirschsprung’s Disease
Pathophysiology
-
Hirschsprung’s disease is the result of failed migration of neural crest cells leading to a lack of innervation in a section of the colon.
-
The aganglionic colon is unable to relax, leading to constriction of that segment.
-
Hirschsprung’s disease is more common in males with a 4:1 male to female predominance [16].
Clinical Features
-
Most newborns present with delayed passage of meconium and stool.
-
Ninety-eight percent of normal newborns pass meconium within 48 h.
-
-
Newborns may present with abdominal distension, vomiting, or stringy stools
-
Physical exam reveals a tight anal sphincter and explosive stooling with rectal exam.
-
Patients may present with toxic megacolon – extreme dilation of the colon leading to distension, pain, perforation, and shock.
Differential Diagnosis
-
Consider constipation, meconium ileus, duodenal atresia, or other intestinal obstruction.
Investigations
-
Rectal suction biopsy of the narrowed section of the colon is gold standard for diagnosis [17].
-
Anal manometry and barium enema can assist with diagnosis.
-
If toxic megacolon is suspected, obtain abdominal x-ray, electrolytes, complete blood count, and blood culture.
Treatment
-
Management of Hirschsprung’s Disease is reviewed in Table 11.11
-
In the case of toxic megacolon, provide resuscitation as clinically indicated and IV antibiotics
Prognosis
-
Long-term complications of Hirschsprung’s disease include constipation, bowel dysfunction, and toxic megacolon [17].
Section E: Metabolic Emergencies
Introduction
Metabolic disorders can masquerade as many different diagnoses on initial presentation. In newborns, always consider underlying metabolic disorders such as congenital adrenal hyperplasia (CAH), thyroid dysfunction, fatty acid disorders, amino acid disorders, urea cycle disorders, organic acid disorders, and glycogen storage disease.
Pathophysiology
-
Metabolic emergencies in a newborn result from a range of disorders and deficiencies.
-
Pathophysiology is entirely dependent on the underlying disorder.
Clinical Features
-
Newborns may present with poor weight gain, feeding difficulties, lethargy, emesis, diarrhoea, and decreased movement.
-
Female and male infants with CAH present with slight variation [18].
-
Females will likely have ambiguous genitalia with enlarged clitoris.
-
Males tend to present with salt wasting and electrolyte abnormalities including hyponatremia and hypokalaemia.
-
Differential Diagnosis
-
Consider sepsis, genetic disorders, and cardiac abnormalities in these patients.
Investigations
-
Newborn screening results should be reviewed.
-
Glucose levels should be obtained immediately.
-
Blood gas should be obtained to assess for signs of metabolic acidosis or alkalosis.
-
Multiple metabolic disorders can present with electrolyte derangement.
-
Obtain ACTH, cortisol, and 17-hydroxyprogesterone levels if concerned for CAH [18].
-
Consider urine organic acids, serum amino acids, acylcarnitine profile, lactate, and pyruvate in non-emergent phase.
-
Consider thyroid studies in patients with clinical signs or maternal history of antithyroid antibodies.
Treatment
-
Provide dextrose for patients with hypoglycaemia defined as less than 2.6 mmol/L or symptomatic.
-
Oral feeds with dextrose (milk, formula) if patient tolerates.
-
IV dextrose 10 % bolus of 2 ml/kg.
-
If blood sugar remains low, consider an IV infusion of 10 % dextrose.
-
-
Consider stress-dose steroids if CAH and adrenal crisis are suspected [10].
-
Hydrocortisone IV: 50–100 mg/m2
-
-
Correct electrolyte abnormalities as indicated.
-
CAH patients may require sodium chloride supplementation [18].
-
Consider sodium benzoate for sodium replacement after discussion with an endocrinologist.
-
Prognosis
-
Many metabolic disorders require long-term dietary supplementation or restriction.
Prevention
-
Newborn screening should be administered on all newborns in the first 3 days of life.
Section F: Haematologic Emergencies
Introduction
Bruising, bleeding, and petechiae are not common presenting issues in newborns, though when present, should raise concern. Broad differentials should be maintained for these clinical features.
Pathophysiology
-
In neonatal alloimmune thrombocytopenia, maternal antibodies cross the placenta and target paternally derived antigens, causing destruction of the platelet.
-
Autoimmune thrombocytopenia occurs when maternal antibodies target maternal and neonatal platelets.
Clinical Features
-
Patients may present with easy bleeding, petechiae, and purpura.
-
Assess if males experienced prolonged bleeding with circumcision.
-
-
Mental status changes could be indicative of intracranial haemorrhage.
Differential Diagnosis
-
Consider vitamin K deficiency, neonatal alloimmune thrombocytopenia, and autoimmune thrombocytopenia.
-
Also consider nonaccidental trauma, infection, underlying coagulopathy, necrotizing enterocolitis, haemophagocytic lymphohistiocytosis, and leukaemia.
Investigations
-
Gather thorough history including maternal medications, illnesses, birth history, and vitamin K administration.
-
Obtain complete blood count, coagulation panel.
-
Maintain a low threshold for infectious workup
-
Cranial computerised tomography (CT) scan or ultrasound should be completed if concerned for intracranial bleed.
-
Consider haematology/oncology consult.
Treatment
-
Immediately administer vitamin K if not previously given or coagulopathy is suspected.
-
Vitamin K: 0.5–1 mg intramuscularly, subcutaneously, or intravenously [10]
-
-
Provide platelet transfusion if patient is thrombocytopenic and actively bleeding (Table 11.12).
Table 11.12 Potential triggers for platelet transfusion -
Consider fresh frozen plasma in setting of moderate to severe bleeding.
-
If concerned for an antibody-mediated process, consider intravenous immunoglobulin (IVIg) and/or platelet transfusion [19, 20].
-
Antibiotic therapy for infants with suspected bacterial infection
Prognosis
-
Intracranial haemorrhage and lower platelet levels are associated with increased risk of morbidity and mortality [21].
-
Majority of newborns with thrombocytopenia have good outcomes [21].
Prevention
-
Administration of vitamin K immediately following birth
-
Close monitoring of infants born to moms with idiopathic thrombocytopenia
Section G: Neurologic Emergencies
Introduction
Seizures may present in the neonatal period as a secondary process or as a primary seizure disorder. The primary goal after stabilisation of the patient should be to uncover and manage the underlying aetiology of the seizure.
Pathophysiology
-
Seizures are more frequent in preterm infants and infants with hypoxic ischemic encephalopathy (HIE) [22].
-
Abnormal movements occur secondary to withdrawal from maternal drug exposure, commonly opioids.
Clinical Features
-
Seizures may manifest with abnormal extremity or eye movements.
-
Withdrawal symptoms are listed in Table 11.13 [23].
Table 11.13 Comparison of neonatal seizures and withdrawal syndrome -
Neonatal abstinence scoring may be utilised to assess for risk of neonatal withdrawal.
-
Differential Diagnosis
-
Aetiologies of seizure range from encephalopathy, stroke, HIE, metabolic disorders, infection, to genetic disorders [24].
-
Electrolyte abnormality can present abnormal movements or behaviour.
-
Nonaccidental trauma should always be considered.
Investigations
-
Obtain glucose and electrolytes in infants with abnormal movements.
-
Gather thorough history, including maternal history, maternal medications, maternal infections, and birth history [24].
-
Obtain head imaging
-
Complete infectious workup, including CSF studies, should be performed.
-
Send urine and meconium toxicology screens to assess for withdrawal syndrome.
Treatment
-
If hypoglycaemia is present, correct with IV dextrose.
-
Consider treating a seizing neonate with phenobarbital or phenytoin [24].
-
If seizures are nonresponsive to the above medications, please consider lorazepam or levetiracetam.
-
In cases of neonatal withdrawal, provide supportive care and tailor medical management based on maternally abused drug (Table 11.13).
Prognosis
Prevention
-
Maternal education on the harms of drug use
References
Kattwinkel J, Perlman J, Aziz K, Colby C, Fairchild K, Gallagher J, et al. Neonatal resuscitation: 2010 American heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Pediatrics. 2010;126(5):1400–13.
Mansbach JM, Piedra PA, Teach SJ, Sullivan AF, Forgey T, Clark S, et al. Prospective multicenter study of viral etiology and hospital length of stay in children with severe bronchiolitis. Arch Pediatr Adolesc Med. 2012;166(8):700–6.
Ralston SL, Lieberthal AS, Meissner HC, Alverson BK, Baley JE, Gadomski AM, et al. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134(5):e1474–502.
Kendig JW, Notter RH, Cox C, Aschner JL, Benn S, Bernstein RM, et al. Surfactant replacement therapy at birth: final analysis of a clinical trial and comparisons with similar trials. Pediatrics. 1988;82(5):756–62.
Liu S, Joseph KS, Lisonkova S, Rouleau J, Van den Hof M, Sauve R, et al. Association between maternal chronic conditions and congenital heart defects: a population-based cohort study. Canadian Perinatal Surveillance System (Public Health Agency of Canada). Circulation. 2013;128(6):583–9.
de Louvois J, Halket S, Harvey D. Neonatal meningitis in England and Wales: sequelae at 5 years of age. Eur J Pediatr. 2005;164(12):730–4.
Holt DE, Halket S, de Louvois J, Harvey D. Neonatal meningitis in England and Wales: 10 years on. Arch Dis Child Fetal Neonatal Ed. 2001;84(2):F85–9.
Ballance WA, Dahms BB, Shenker N, Kliegman RM. Pathology of neonatal necrotizing enterocolitis: a ten-year experience. J Pediatr. 1990;117(1 Pt 2):6–13.
Brook I. Microbiology and management of neonatal necrotizing enterocolitis. Am J Perinatol. 2008;25(2):111–8.
Verani JR, McGee L, Schrag SJ. Division of bacterial diseases, national center for immunization and respiratory diseases. Prevention of perinatal group B streptococcal disease – revised guidelines from CDC. MMWR Recomm Rep. 2010;59(RR10):1–32.
American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004;114(1):297–316.
Rasul CH, Hasan A, Yasmin F. Outcome of neonatal hyperbilirubinemia in a tertiary care hospital in Bangladesh. Malays J Med Sci. 2010;17(2):40–4.
Kuenzler KA, Rothenberg SA. Duodenal atresia. Fundamentals of pediatric surgery. New York: Springer; 2011.
Bishay M1, Lakshminarayanan B, Arnaud A, Garriboli M, Cross KM, Curry JI, et al. The role of parenteral nutrition following surgery for duodenal atresia or stenosis. Pediatr Surg Int. 2013;29(2):191–5.
Suita S, Taguchi T, Ieiri S, Nakatsuji T. Hirschsprung’s disease in Japan: analysis of 3852 patients based on a nationwide survey in 30 years. J Pediatr Surg. 2005;40(1):197–201.
DeLorijn F, Kremer LCM, Reitsma JB, Benninga MA. Diagnostic tests in Hirschsprung disease: a systematic review. J Pediatr Gastroenterol Nutr. 2006;42:496–505.
Speiser PW, Azziz R, Baskin LS, Ghizzoni L, Hensle TW, Merke DP, et al. Congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(9):4133–60.
Ouwehand WH, Smith G, Ranasinghe E. Management of severe alloimmune thrombocytopenia in the newborn. Arch Dis Child Fetal Neonatal Ed. 2000;82(3):F173–5.
Ovali F, Samanci N, Ermis B, Akdogan Z, Dagoglu T. Alternative therapies for neonatal autoimmune thrombocytopenia. Vox Sang. 1998;74(3):198–200.
Stanworth SJ, Clarke P, Watts T, Ballard S, Choo L, Morris T, et al. Platelets and Neonatal Transfusion Study Group. Prospective, observational study of outcomes in neonates with severe thrombocytopenia. Pediatrics. 2009;124(5):e826–34.
Ronen GM, Penney S, Andrews W. The epidemiology of clinical neonatal seizures in Newfoundland: a population-based study. J Pediatr. 1999;134(1):71–5.
Hudak ML, Tan RC. Committee on drugs, committee on fetus and newborn, American Academy of Pediatrics. Neonatal drug withdrawal. Pediatrics. 2012;129(2):e540–60.
Co JP, Elia M, Engel Jr J, Guerrini R, Mizrahi EM, Moshé SL, et al. Proposal of an algorithm for diagnosis and treatment of neonatal seizures in developing countries. Epilepsia. 2007;48(6):1158–64.
Ronen GM, Buckley D, Penney S, Streiner DL. Long-term prognosis in children with neonatal seizures: a population-based study. Neurology. 2007;69(19):1816–22.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer India
About this chapter
Cite this chapter
Cochran, C.L., Soni, P.P. (2016). Neonatal Emergencies. In: David, S. (eds) Clinical Pathways in Emergency Medicine. Springer, New Delhi. https://doi.org/10.1007/978-81-322-2713-7_11
Download citation
DOI: https://doi.org/10.1007/978-81-322-2713-7_11
Published:
Publisher Name: Springer, New Delhi
Print ISBN: 978-81-322-2711-3
Online ISBN: 978-81-322-2713-7
eBook Packages: MedicineMedicine (R0)