General procedure of thoracotomy and laparotomy is described in this chapter. In terms of thoracotomy, three different types of incision such as posterolateral thoracotomy, axillar vertical incision, and axillar skin crease incision were illustrated. Thoracotomy with conservation of the perithoracic muscles by using axillar skin crease incision was described in detail. The position of patient, selection of intercostal space, and postoperative care tips were also discussed. In respect to laparotomy, various types of approaches such as upper abdominal transverse incision, lower abdominal transverse incision, subcostal incision, Mercedes-Benz incision, pararectal incision, and transumbilical approach were illustrated. Transumbilical approaches including upper half-circumumbilical incision, lower half-circumumbilical skin incision, vertical incision in the umbilicus, and umbilical sliding-window technique were described in detail. Abdominal wound closure and postoperative care tips were also discussed.
The figures in this chapter are reprinted with permission from Standard Pediatric Operative Surgery (in Japanese), Medical View Co., Ltd., 2013, with the exception of occasional newly added figures that may appear.
A patient is basically in the lateral position under general anesthesia. Although the pulmonary lobe can be easily excluded in neonates and infants, a better operative field can be obtained by degassing the lungs via differential lung ventilation by using a Fogarty catheter as needed in older children. For patients in whom the intraoperative tip position of the endotracheal tube is problematic (e.g., patients with esophageal atresia), the tip position of the endotracheal tube should be confirmed by using a bronchofiberscope before and after postural change.
1.2 Operations
1.2.1 Position of Patient
After the patient is placed in the lateral position, a pillow of proper height is inserted below the side of the chest to protect the shoulders. Simultaneously, the intercostal space in the affected side should be dilated with slight curvature of the entire chest. The affected arm is elevated by using a handstand or bed cradle to expand to 100–120° (Fig. 2.1). Especially, expanding the arm is necessary for the axillary fold incision. However, caution must be used because an excessively expanded arm may cause brachial plexus palsy. Because infants’ bodies are flexible and tend to assume unstable postures, the anterior and posterior hips should be grasped and fixed thoroughly.
A selection should be made from among the following skin incision approaches: posterolateral thoracotomy, axillar vertical incision, and axillar skin crease incision [1]. Posterolateral thoracotomy (Fig. 2.2a) provides the largest visual field. However, the use of this approach can easily result in subsequent thoracic deformity or elevation of the shoulder because suturing involves a divided part of the muscle, such as the latissimus dorsi muscle, pectoralis major muscle, and sometimes the trapezius muscle (Fig. 2.3). In the axillar vertical incision, a straight skin incision line is made along the middle axillary line (Fig. 2.2b). In the axillar skin crease incision, a loop-shaped skin incision line is made along the skin folds that are located at the most caudal region of the folds existing in the axilla naturally (Fig. 2.2c). After making the skin incision for both the axillar vertical incision and axillar skin crease incision, the dermal flaps should be generated, followed by the performance of thoracotomy by abduction in flexion of the latissimus dorsi muscle and pectoralis major muscle, without dissecting them. The visual field of surgery depends on the size of the window formed by the dermal flaps. However, for the axillar vertical incision, the window can be expanded by extending the skin incision line (Fig. 2.4). Meanwhile, for the axillar skin crease incision, the size of the window is limited. The axillar skin crease incision is the best from a cosmetic viewpoint because the surgical wound will be unified with the folds of the axillary in the long term, with little chance of keloid scar formation (Fig. 2.5). While considering that the visual field is better in the axillar vertical incision, the skin incision approach should be chosen according to the operator’s habituation and skill, the degree of adhesion, etc.
Fig. 2.2
Skin incision line for thoracotomy. (a) Posterolateral thoracotomy. (b) Axillar vertical incision. (c) Axillar skin crease incision
Postoperative wound from the axillar skin crease incision for esophageal atresia (at sixth month after surgery). The skin incised wound (arrow) can barely be distinguished from the folds of the axillary
The intercostal space should be chosen according to the targeted site. The standard selections are as follows: the third or fourth intercostal space for patients with esophageal atresia, the fourth or fifth intercostal space for patients who undergo superior lobe resection, the fifth or sixth intercostal space for patients who undergo inferior lobe resection, and the sixth or seventh intercostal space for patients who undergo surgery for the diaphragm or lower esophagus.
1.2.4 Thoracotomy with Conservation of the Perithoracic Muscles
Regardless of the skin incision approach, it is important to perform thoracotomy while conserving the muscles forming the surroundings of the thorax, such as the latissimus dorsi muscle, pectoralis major muscle, and serratus anterior muscle, as much as possible. This helps to prevent the postoperative limitations of movement and pain and the occurrence of thoracic deformity and elevation of the shoulder during the convalescent phase.
The following section describes thoracotomy with conservation of the perithoracic muscles by using axillar skin crease incision [1] as an example:
Choose the skin incision line located at the most caudal region of the folds. If it is within the area of folds, it can deviate from the axilla to some extent.
Make an incision in the subcutaneous tissues slightly toward the caudal region, and displace the adipose tissues toward the cephalad portion while being careful not to cut the inside of the adipose tissues of the axilla.
To form the dermal flaps, adequately remove the subcutaneous tissues in the layer of the anterior surface of the fascia. Since the skin of neonates and infants is sufficiently extensible, secure the window of the dermal flaps widely.
In the dorsum, incise the fascia along the anterior border of the latissimus dorsi muscle, which traverses and displaces the latissimus dorsi muscle with the long thoracic nerve posteriorly (Fig. 2.6).
Fig. 2.6
Axillar skin crease incision. Displacement of the latissimus dorsi muscle posteriorly
In the ventral aspect, perform blunt removal of the pectoralis major muscle until clavicle can be palpated by the finger, and displace the pectoralis major muscle anteriorly.
Identify the intercostal space where thoracotomy is planned, and perform abduction in flexion of the serratus anterior muscle so that the chest wall is exposed on the targeted intercostal space. Remove a part of the serratus anterior muscle because it attaches to the ribs in the ventral aspect, and expose the entire intercostal space where thoracotomy is planned (Fig. 2.7).
Fig. 2.7
Axillar skin crease incision. Abduction in flexion of the serratus anterior muscle
Separate the intercostal muscle by using electrocautery while collecting it little by little. In normal thoracotomy, only the pleura are incised. In the extrapleural approach, enter the extrapleural space from outside of the pleura.
1.2.5 Exposure of Operation Field and Protection of Wound Border
A rib retractor should be used in the intercostal space in order to expand the operative field by dilating the intercostal spaces. In axillar vertical incision and axillar skin crease incision, to dilate the window of the dermal flap, a retractor should be used at right angles to the rib retractor. Caution must be used to avoid crushing the border of the wound when it is excessively dilated. A wound protector can be used to protect the wound border.
1.2.6 Wound Closure
For the closure of the chest wound, care must be taken not to close the intercostal space excessively. Regardless of the dissected length of the intercostal space, three to four stitches for the ribs with absorption threads are adequate for closing the space without causing narrowing of the original intercostal space. When the intercostal space is closed excessively, rib fusion may occur, leading to deformation of the thorax. A drain should be inserted into the thoracic cavity as needed. When the subcutaneous tissues are widely removed, a drain can be placed subcutaneously for the short term.
1.3 Postoperative Care Tips
After surgery for treatment of pulmonary hilar lesion and the mediastinum, the postoperative course should be followed by obtaining chest X-rays while carefully monitoring for the onset of chylothorax and complications due to phrenic nerve paralysis.
2 Laparotomy
2.1 Preoperative Management
A patient is basically in the supine position under general anesthesia. For a patient in whom the operative field is located at the retroperitoneum or at a deep site, a pillow of proper height should be inserted below the back, and the abdomen should be elevated with curvature of the vertebral body according to the targeted site.
2.2 Operations
2.2.1 Selection from Among the Laparotomy Approaches
The procedures of laparotomy consist of skin incision, subcutaneous tissue incision, fasciotomy, isolation of the muscle or abduction in flexion, and peritoneum incision. Various approaches can be used, depending on the extent of the surgical field. Generally, in children, a transverse incision made across the cleavage lines is preferable to a vertical incision. Various approaches are described in the following section.
2.2.2 Upper Abdominal Transverse Incision
This incision is a basic approach for abdominal surgery in children (Fig. 2.8a). This approach allows for a large visual field, and the surgical wound is inconspicuous because the incision is made across the cleavage lines. It crosses the rectus abdominis muscle or the round ligament of the liver. In neonates, ensure that ligation of the round ligament of the liver is definitely performed because bleeding may occur. This approach is appropriate for gastrointestinal perforation in which the location of perforation cannot be identified.
Make a skin incision along the horizontal line passing through the midpoint between the xiphoid process and the umbilicus.
The length of the skin incision is based on the circumference of both rectus abdominis muscles, and the left and right lengths are adjusted according to the targeted site (Fig. 2.9).
After dilating the subcutaneous tissues, incise the anterior sheath of the rectus abdominis muscle by using electrocautery.
Hold and incise the peritoneum in order to avoid causing damage to the abdominal organs, and subsequently perform the operation.
2.2.3 Subcostal Incision
This approach is used for surgery in the hepatobiliary system and the right diaphragm on the right side and for the left diaphragm and the gastric cardia on the left side (Fig. 2.8b). In small infants whose costal arch is almost horizontal and whose skin is sufficiently extensible, the transverse incision along the cleavage is made only on the skin, and the subcutaneous tissues can be removed at the anterior surface of the fascia to incise the fascia and muscle under the costal arch.
2.2.4 Mercedes-Benz Incision
This is a laparotomy approach in which the bilateral subcostal incisions are connected at the center, and a median incision is made in the cephalad portion. It is used for liver transplantation in older children (Fig. 2.8c).
2.2.5 Lower Abdominal Transverse Incision
This approach is used for surgery of the ileocecum, the colon and rectum extending from the sigmoid colon, the genitourinary system, and the pelvic structures (Fig. 2.8d). In a type of surgical incision known as the Pfannenstiel incision, only the line of the skin incision is made caudally, and a loop-shaped incision is made on the folds so that the scar will be hidden by the pubic hair; for the fasciae and muscle, a transverse incision is made on the center of the lower abdominal region.
2.2.6 Pararectal Incision
This approach is used for cholecystectomy and appendectomy, although it is currently not used frequently because laparoscopic surgery has been developed (Fig. 2.8e).
2.2.7 Transumbilical Approach
Since the umbilicus has been defined as an insertion site for a laparoscopic port, abdominal surgery that utilizes the umbilical region is performed with the purpose of making a surgical wound smaller and less noticeable from a cosmetic viewpoint.
Upper half-circumumbilical incision: a skin incision is made on the cranial semicircle of the folds at, or slightly inside of, the umbilical ring, and the subcutaneous tissues are removed to expose the white line and anterior sheath of the rectus abdominis muscle; subsequently, laparotomy is performed with a median incision (Fig. 2.10a). A transverse incision is also made on the rectus abdominis muscle, if necessary. This approach is used for hypertrophic pyloric stenosis, duodenal atresia, and intestinal atresia. When the window of the skin secured with a wound retractor is too small, dilate it by adding a horizontal supportive incision to the skin (omega-shaped [Ω] incision).
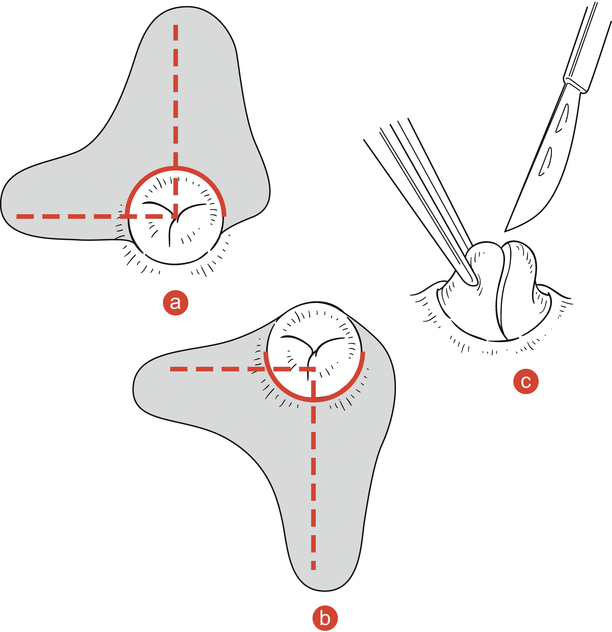
Fig. 2.10
Skin incision for the transumbilical approach. The oblique line indicates the range of removal of the subcutaneous tissues. The dotted line indicates the incision line of the fascia. (a) Upper half-circumumbilical incision. (b) Lower half-circumumbilical skin incision. (c) Vertical incision in the umbilicus
Lower half-circumumbilical skin incision: incise the caudad semicircle of the folds of the umbilical ring, and similarly perform an operation at the lower abdomen (Fig. 2.10b). This approach is used for ovarian cyst and Meckel’s diverticulum.
Vertical incision in the umbilicus: since surplus skin is folded in the camerostome of the center of the umbilical region, when retracting and exposing the bottom of the umbilicus to make an incision, a long incision line can be secured sufficiently only in the umbilical ring (Fig. 2.10c). This approach can be applied when performing surgeries for appendicitis, Meckel’s diverticulum, ovarian cyst, etc., by displacing the targeted organ outside the wound from the window by using a scope with forceps.
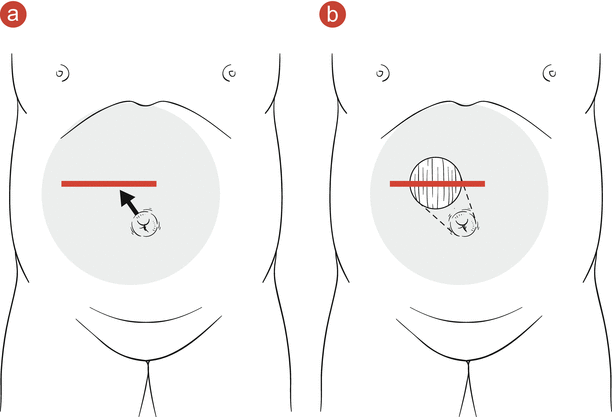
Umbilical sliding-window technique [2]: make a circumferential skin incision along (or slightly inside) the umbilical ring, and widely remove the subcutaneous tissues in the anterior surface of the fasciae while leaving the skin of the umbilical region on the abdominal wall (Fig. 2.11a). Then, move the window formed by the dermal flap horizontally to the incised part of the muscle (Fig. 2.11b: sliding). For hypodermatomy of the umbilical region, leave the subcutaneous fat around the skin in the umbilical region and maintain blood flow of the skin. In addition, the skin window can easily be moved horizontally by removing the subcutaneous tissues thoroughly from the incised fascia as well as the contralateral navel. This technique can be applied at various sites, including the upper and lower abdomen, because the operation is performed right over the targeted organ. By expanding the range of removal of the subcutaneous tissues, laparotomy can be performed in the region away from the navel. By expanding the window with supportive incision of the skin, this technique can be applied to surgery for the biliary system and diaphragm.
Fig. 2.11
Umbilical sliding-window technique. (a) Widely remove the subcutaneous tissues from the region around the incised muscle to the contralateral navel (shadow area). (b) Move the skin window horizontally to the incised part of the fascia
2.2.8 Exposure of Operation Field and Protection of Wound Border
Operations, including the transumbilical approach, have recently tended to be performed with smaller skin incision wounds. A wound protector helps to secure the visual field of the surgery and to protect the wound border (Fig. 2.12).
Fig. 2.12
Exposure of operation field and protection of wound border by a wound protector. Duodenoduodenostomy by using umbilical sliding-window technique with a wound protector
The closed abdomen procedures include suturation of the peritoneum and the transversalis fascia, suturation of the anterior layer of rectus sheath, and suturation of the subcutaneous tissues and the skin. Dehiscence of the fascia may cause abdominal incisional hernia and scarring in the wounded area. Therefore, double-layer suture is desirable for the peritoneum, muscular layer, and subcutaneous tissues to layers (Fig. 2.13). For patients in whom re-laparotomy is expected at a higher rate (e.g., patients with biliary atresia), absorbable adhesion barrier materials for preventing adhesion should be used before closing the abdomen.
Fig. 2.13
Layer-to-layer suture for abdominal wound closure. Using absorption threads, suture the peritoneum, transversalis fascia, anterior layer of rectus sheath, subcutaneous tissues, and skin by each layer
Currently, with the exception of peritonitis associated with intestinal perforation, the abdominal cavity drain is rarely used. When the subcutaneous tissues are widely removed by using the umbilical sliding-window technique, subcutaneous emphysema or redness may occur postoperatively. If this is troublesome for the patient, a thin subcutaneous drain should be placed with slight compression of the skin.
References
Taguchi T, Nagata K, Kinoshita Y, Ieiri S, Tajiri T, Teshiba R, Esumi G, Karashima Y, Hoka S, Masumoto K. The utility of muscle sparing axillar skin crease incision for pediatric thoracic surgery. Pediatr Surg Int. 2012;28:239–44.
Odaka A, Hashimoto D. Umbilical approach using the sliding-window method to avoid a large abdominal incision: report of two pediatric cases. Pediatr Surg Int. 2005;21:928–3.
Department of Pediatric Surgery, Osaka Medical Center and Research Institute for Maternal and Child Health, 840 Murodo-cho, Izumi, Osaka, 594-1101, Japan
Usui, N. (2016). Thoracotomy and Laparotomy.
In: Taguchi, T., Iwanaka, T., Okamatsu, T. (eds) Operative General Surgery in Neonates and Infants. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55876-7_2