
Abstract
The function of the atrioventricular valve (AVV) complex is one of the most important determinants of prognosis in patients with congenital heart disease. However, the anatomy of the AVV complex is complicated, especially in patients with congenital heart disease, which hampers precise preoperative assessment. Moreover, AVV function is maintained by a very delicate balance of the forces generated by the ventricle, atrium, papillary muscles, and blood flow. The AVV leaflet billows with the increment of the hydrostatic pressure in the ventricle and closes by making coaptation with the adjacent leaflets using this balance of force. The shape and size of the annulus or position and function of the papillary muscles are also very important factors in maintaining the effective coaptation of the leaflets with minimal stress on the leaflet and chordae. If a congenital abnormality of the leaflet or valvular apparatus or an incorrect surgical repair causes an imbalance of the forces at work in this delicate system, the result can be valve failure. Since the advent of real-time three-dimensional echocardiography (3DE), we are able to assess the precise anatomical and functional features of this complicated system.
1 Anatomical Aspects of the Atrioventricular Valve
1.1 Development of the Atrioventricular Valve
During the embryonic development of the heart, the looping of the heart tube is followed by the development of the atrioventricular valve (AVV) in the atrioventricular canal starting with the formation of endocardial cushions by an epithelial to mesenchymal transformation. The proliferation of mesenchymal cells at the base of the embryonic leaflet contributes to its elongation. The patterning of extracellular matrix proteins in the leaflet is accomplished 1 week after birth, with glycosaminoglycan and versican on the atrial side and collagen fibers on the ventricular side. Finally, the nodular thickening of the coaptation zone is formed by the end of the second week after birth [1].
In the mature heart, the mitral valve (MV) leaflet consists of four histological layers, the atrialis, spongiosa, fibrosa, and ventricularis, ordered from the atrial aspect to the ventricular side. The atrialis is the surface layer adjacent to the atrium, which is composed of elastic and collagen fibers covered with overlying endothelium. The spongiosa largely consists of extracellular matrix, proteoglycans and glycosaminoglycans, and elastic fibers. The spongiosa is the major component of the free edge and acts as a cushion to protect the leaflet from the impulse of valve closure. Beneath the spongiosa is the fibrosa, which is comprised of collagen fibers and is located close to the ventricular surface extending to the chordae tendineae. It works as the major load-bearing layer during valve closure. The final layer adjacent to the ventricle is the ventricularis, which is covered by endothelial cells that overlie elastic and collagen fibers [2].
1.2 Normal Anatomy of the Mitral Valve
Figure 2.1 shows a normal MV specimen from a neonate. The MV is comprised of two leaflets (the anterior and posterior leaflets), the annulus, chordae tendineae, and papillary muscles. The anterior leaflet hangs like a curtain, dividing the inlet and outlet portions of the left ventricle (Fig. 2.1). The anterior leaflet (also called the aortic leaflet) occupies a third of the annular circumference and has a fibrous continuity with the aortic valve. The right and left ends of this fibrous continuity are demarcated by the right and left fibrous trigone. The right trigone together with the membranous septum forms the central fibrous body. Although the annulus is recognized as the hinge line of the leaflet on an echocardiogram, from the pathological point of view, the distinctive ringlike fibrous cord that supports the base of the leaflets does not always surround the entire area of the leaflet base. Moreover, a well-formed fibrous cord is frequently absent at the annulus opposite to the fibrous continuity [3, 4]. The posterior leaflet (also called the mural leaflet) occupies two thirds of the annulus and has three or more scallops, which are referred to as the anterolateral (P1), middle (P2), and posteromedial sections (P3). Figure 2.2 shows an en face image of a normal MV constructed by transesophageal 3DE. The three sections of the posterior leaflet and counterparts of the anterior leaflet are well visualized by 3DE. The corresponding sections of the anterior leaflet are labeled A1, A2, and A3, respectively. The area of the anterior leaflet is slightly bigger than that of the posterior leaflet, and the combined surface area of the two leaflets is twice that of the mitral annulus, which provides sufficient area for the creation of a coaptation zone of appositional leaflets.

Normal mitral valve anatomy in a neonate. (a) Mitral valve. The posteromedial papillary muscle usually consists of multiple papillary muscle bundles. On the other hand, the anterolateral papillary muscle usually consists of a single muscle bundle. Note the prominent strut chordae from the top of each papillary muscle inserting on the rough zone of the anterior leaflet. Asterisks indicate the left and right fibrous trigone. (b) Fibrous continuity of the mitral and aortic valve. Arrows indicate fibrous continuity of the anterior mitral leaflet and aortic valve. AL anterior leaflet, ALPM anterolateral papillary muscle, L left coronary cusp, LA left atrium, LT left trigone, LVOT left ventricular outflow tract, N noncoronary cusp, PFO patent foramen ovale, PL posterior leaflet, PMPM posteromedial papillary muscle, R right coronary cusp, S strut chordae

An en face image of a normal mitral valve by three-dimensional echocardiography. The left panel shows a closed mitral valve and the right panel shows an opened valve image. The three scallops of the posterior leaflet are referred to as the anterolateral (P1), middle (P2), and posteromedial (P3) sections. The corresponding sections of the anterior leaflet are labeled A1, A2, and A3, respectively. AO aorta, CFB central fibrous body, MV mitral valve, TV tricuspid valve
The chordae tendineae are classified into three groups: (1) first-order chordae (also called marginal/free-edge chordae), which insert on the free edge of the leaflet, (2) second-order chordae (also called rough zone chordae) that insert on the ventricular surface of the leaflet beyond the free edge, forming the rough zone of the leaflet, and (3) third-order chordae (also called basal chordae), which are unique to the posterior leaflet and arise directly from the ventricular wall or from trabeculations and insert on the basal zone of the posterior leaflet. The two distinctive thick and strong second-order chordae of the anterior leaflet are called strut chordae and arise from the tip of the papillary muscle and insert on the rough zones (Fig. 2.1). Because of their distinctive morphology of chordal branching that resembles the ribs of a fan, the chordae that insert into the commissure are called fan-shaped chordae (also called commissural chordae).
Two groups of papillary muscles are located beneath the commissures, occupying anterolateral and posteromedial positions. The anterolateral papillary muscle is usually a single muscle bundle, while the posteromedial papillary muscle consists of two or three papillary muscle bundles (Fig. 2.1). Both papillary muscles usually have separate heads and the number and shape of the papillary muscle bundles vary among individuals.
1.3 Normal Anatomy of the Tricuspid Valve
Figure 2.3 shows the normal tricuspid valve (TV) of a neonate, the same specimen shown in Fig. 2.1. Although there are many variations to the normal morphology of a TV, the TV is generally accepted to consist of three leaflets: the anterior, septal, and posterior leaflets. Figure 2.4 shows an en face image of a normal TV constructed by transesophageal 3DE. The leaflet and chordae are thinner than those of the MV. The anterior leaflet (also called the superior leaflet) is the largest of the three leaflets, is located in the anterosuperior position, and guards the orifice of the right ventricular outflow tract. The septal leaflet (also called the medial leaflet) is usually larger than the posterior leaflet. Although most of the septal leaflet’s basal attachment is to the interventricular septum, its attachment sometimes extends to the inferior wall. A small fold is frequently observed at the transition between the septal and posterior leaflets. The septal leaflet has a chordal attachment to the ventricular septum, which limits its mobility. These distinctive anatomical features of the sepal leaflet allow the TV to be distinguished from the MV. The posterior leaflet (also called the inferior leaflet) is the smallest leaflet and is located at the inferior position. Compared to the MV, the leaflet morphology of the TV is highly variable, with many indentations of variable depth. The annulus of the TV usually lacks a solid ringlike fibrous cord and is pathologically just a continuation of the fibrous tissue of the leaflet to the subendocardial fiber. The annulus of the septal leaflet is especially indistinct because the anterior part of the leaflet merges with the membranous interventricular septum and is apically displaced from the atrioventricular junction. The commissure between the anterior and septal leaflets (anteroseptal commissure) is located at the most cranial position of the membranous septum and the fan-shaped chordae from the medial papillary muscle attach to the septal and anterior leaflets. The medial papillary muscle is on the bifurcation of the anterior and posterior limbs of the trabecula septomarginalis or is sometimes absent, in which case the chordae arise directly from the trabecula septomarginalis or the crista supraventricularis. The commissure between the anterior and posterior leaflets (anteroposterior commissure) is located roughly at the acute margin of the right ventricle, and beneath it is an anterior papillary muscle, which is the largest papillary muscle, in the right ventricle and has a moderator band attached to its base. The commissure between the posterior and septal leaflets (posteroseptal commissure) is located at the junction of the inferior and septal walls, and beneath it is a posterior papillary muscle. The posterior papillary muscle is on the inferior wall and at the most medial position. Its size varies considerably and is usually small (Fig. 2.3) [5].

Normal tricuspid valve anatomy in a neonate. The tricuspid valve consists of three leaflets. The septal leaflet is tethered by chordae from the ventricular septum and is less mobile compared to the other two leaflets. AL anterior leaflet, APM anterior papillary muscle, CS crista supraventricularis, MPM medial papillary muscle, PAV pulmonary artery valve, PL posterior leaflet, PPM posterior papillary muscle, SL septal leaflet, TSM trabecula septomarginalis

An en face image of a normal tricuspid valve obtained using three-dimensional echocardiography. The left panel shows a closed tricuspid valve and the right panel shows an opened valve image. The tricuspid valve consists of three leaflets. AL anterior leaflet, MV mitral valve, PL posterior leaflet, SL septal leaflet, TV tricuspid valve
2 Anomalies of the Atrioventricular Valve
The etiologies of AVV disease are as follows: congenital, degenerative, inflammatory, endocarditis, rheumatic, ischemic, cardiomyopathies, traumatic, and iatrogenic. These etiologies are associated with the anatomical abnormality or malfunction of one or multiple components constituting the AVV complex, thereby causing regurgitation or stenosis of the AVV. Carpentier et al. classified the mechanisms of mitral regurgitation into three categories [7, 8]. This classification is applicable to the TV or common AVV:
-
Type I: normal leaflet motion (annular enlargement, leaflet perforation, or cleft)
-
Type II: excessive leaflet motion (flail leaflet, ruptured chordae, prolapse, or billowing)
-
Type III: restricted leaflet motion:
-
(a)
Short leaflet or chordae
-
(b)
Leaflet tethering by the papillary muscle
-
(a)
In congenital AVV disease, the multiple pathologies outlined above usually coincide and cause regurgitation and/or stenosis.
2.1 Mitral Valve Disease
The classification of congenital mitral valve anomalies is shown in Table 2.1 [6].
-
1.
Isolated mitral valve cleft (Fig. 2.5): Figure 2.5 shows en face images of an isolated MV cleft by transesophageal 3DE. This case was not associated with an atrioventricular septal defect and the regurgitation was from a cleft. This anomaly was first reported by Petitalot in 1987 [9], and the cleft is often oriented towards the left ventricular outflow tract rather than the ventricular septum, as is usually seen in atrioventricular septal defects. However, in this particular patient, the cleft points towards the ventricular septum.
Fig. 2.5 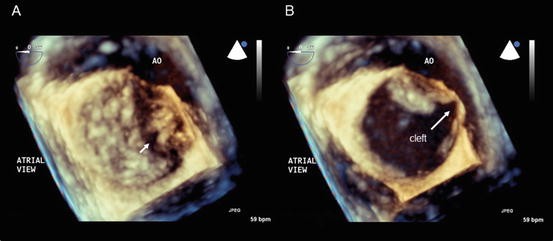
Isolated mitral valve cleft. En face images of a mitral valve at the closed (a) and opened (b) positions obtained using transesophageal three-dimensional echocardiography. The arrow indicates the mitral valve cleft. AO aorta
-
2.
Double orifice mitral valve (Fig. 2.6): A double orifice MV was first described by Greenfield in 1876 and is a rare AVV anomaly characterized by the presence of two or more orifices in the AVV leaflet, each having an independent chordal attachment to the papillary muscles [10]. A double orifice MV rarely occurs as an isolated form and is usually associated with an atrioventricular septal defect, ventricular septal defect, truncus arteriosus, pulmonary stenosis, coarctation or interruption of the aortic arch, a bicuspid aortic valve, tetralogy of Fallot, or Ebstein’s anomaly. A partial atrioventricular septal defect is most commonly seen, accounting for 41 % of associated anomalous lesions. Mitral regurgitation is the most common functional abnormality (43 % of patients), followed by mitral stenosis (13 %) and their combination (7 %). Of note, no functional abnormality of the MV is observed in 37 % of patients [11].
Fig. 2.6 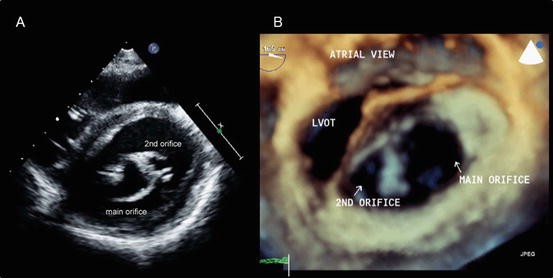
Double orifice mitral valve. (a) A transthoracic two-dimensional echocardiography image. (b) An en face image obtained using transesophageal three-dimensional echocardiography. LVOT left ventricular outflow tract
-
3.
Rheumatic mitral valve disease (Fig. 2.7): Figure 2.7 shows a transthoracic 3DE image of a 12-year-old Afghan boy suffering from rheumatic fever with commissural fusion causing significant MV stenosis. The rheumatic process causes leaflet thickening and fusion of commissures, resulting in limited leaflet movement and a narrowing of the mitral orifice. The chordae tendineae are also involved in fusion, shortening, fibrosis, and calcification, leading to restricted leaflet movement, leaflet malcoaptation, and regurgitation [12].
Fig. 2.7 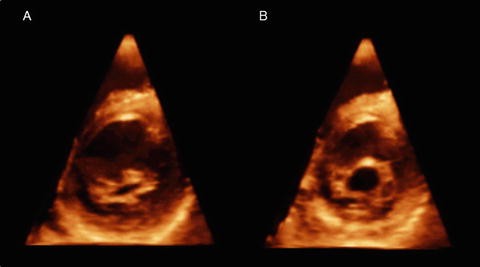
Rheumatic mitral valve disease. Transthoracic three-dimensional images of a mitral valve at the closed (a) and opened (b) positions. Note significant commissural fusion (b)



2.2 Tricuspid Valve Disease
TV anomalies are shown in Table 2.2 [13].
The functional abnormality of TV disease most commonly presents as tricuspid regurgitation. Isolated TV stenosis is very rare and is observed in countries where rheumatic heart disease is prevalent. Rather, TV stenosis commonly presents as combined lesions of stenosis and regurgitation.
The most common causes of congenital tricuspid regurgitation are Ebstein’s anomaly and TV dysplasia. These two entities are clinically similar but anatomically different. Ebstein’s anomaly is characterized by an inferior displacement of the proximal hinge point of the septal and posterior leaflets from the atrioventricular junction and the existence of an atrialized ventricle (Fig. 2.8a,b). On the other hand, the basal attachment of the TV is normal in TV dysplasia. Aaron described the characteristic features of TV dysplasia as follows: [1] focal or diffuse thickening of the leaflets; [2] deficient development of the chordae tendineae and papillary muscles, most often binding down or tethering the valve margin; [3] improper separation of valve components from the ventricular wall; and [4] focal agenesis of valvular tissue [14].

Ebstein’s anomaly. (a) The simultaneous orthogonal 3 planes of a tricuspid valve. Note the significant plastering of the septal and posterior leaflets. Arrows indicate the hyphenated distal attachment of the anterior leaflet to the right ventricular free wall. (b) An en face image of a tricuspid valve in the closed position. (c) An en face image of a tricuspid valve in the opened position. AL anterior leaflet, AO aorta, ARV atrialized right ventricle, LA left atrium, LV left ventricle, LVOT left ventricular outflow tract, PL posterior leaflet, RA right atrium, RV right ventricle, RVOT right ventricular outflow tract, VS ventricular septum
-
1.
Ebstein’s anomaly (Fig. 2.8): The crucial feature of Ebstein’s anomaly is the rotational displacement of the hinge point of the TV leaflet, with maximal apical displacement occurring at the junction of the septal and posterior leaflets and no displacement of the anterior leaflet. This apical displacement creates the atrialized portion of the basal right ventricle. The anterior leaflet is usually large, with normal annular attachments at the atrioventricular junction. However, it is commonly associated with restricted motion. The restriction of the anterior leaflet is caused by short chordae and the expansion of the anterior papillary muscle onto the ventricular surface. In its severe form the chordae tendineae are absent, and linear or hyphenated distal attachment of the leaflet edge to the ventricular wall is observed [15, 16].
-
2.
The TV of a patient with hypoplastic left heart syndrome (Fig. 2.9): In patients with hypoplastic left heart syndrome, tricuspid regurgitation is one of the most important risk factors for mortality and/or ventricular dysfunction [17]. Figure 2.9 shows severe tricuspid regurgitation in a patient with hypoplastic left heart syndrome after a Norwood operation. This patient had mild regurgitation before the Norwood operation. However, as the dysfunction and dilation of the right ventricle progressed, tethering of the septal leaflet by the chordae from the septum became prominent, and regurgitation deteriorated.
Fig. 2.9 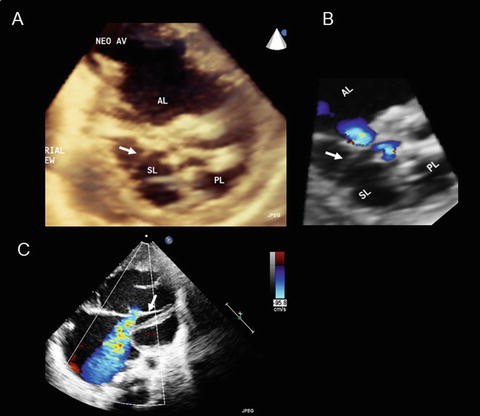
Tricuspid valve in hypoplastic left heart syndrome. (a) An en face image of a tricuspid valve in the closed position obtained using transthoracic three-dimensional echocardiography. (b) A corresponding image to that in panel A obtained using color Doppler three-dimensional echocardiography. (c) A four-chambered view showing tethering of the septal leaflet and severe tricuspid valve regurgitation. The arrow indicates the tethering chordae from the ventricular septum to the margin of the septal leaflet. AL anterior leaflet, AV aortic valve, PL posterior leaflet, SL septal leaflet

2.3 Common Atrioventricular Valve
-
1.
Common AVV
The essential features of an atrioventricular septal defect (AVSD) are the defect of the atrioventricular septum and the abnormalities of the AVV. There are four subtypes of AVSD: complete, intermediate, transitional, and partial AVSD [18]. In complete and intermediate AVSD, there is a single annulus, although in intermediate AVSD there are two separate right and left orifices divided by a tongue of tissue that connects the superior and inferior bridging leaflets (Fig. 2.10). Complete AVSD is subdivided into three types according to the anatomy of the superior bridging leaflet (Rastelli classification). Figure 2.11 shows representative 3DE images of Rastelli type A and C defects. Rastelli A accounts for 60 % of all complete AVSDs, Rastelli C accounts for 35 %, and Rastelli B is rare and accounts for less than 5 % of cases. Partial and transitional AVSDs have distinct right and left AVV annuli, and the left AVV invariably has a cleft (Fig. 2.12). Transitional AVSD is a subtype of partial AVSD and is associated with a small or restrictive inlet VSD.
Fig. 2.10 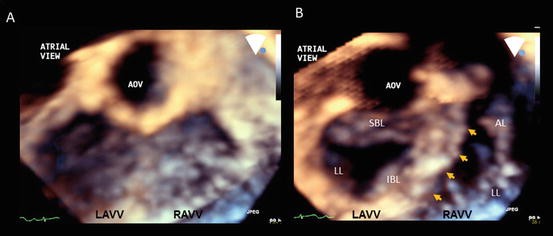
Intermediate atrioventricular septal defect. (a) An en face image of an atrioventricular valve in the closed position. (b) An en face image of an atrioventricular valve in the opened position. Arrows indicate tongue tissue connecting the superior and inferior bridging leaflet and dividing the orifice into two. AL anterior leaflet, AOV aortic valve, IBL inferior bridging leaflet, LAVV left atrioventricular valve, LL lateral leaflet, RAVV right atrioventricular valve
Fig. 2.11 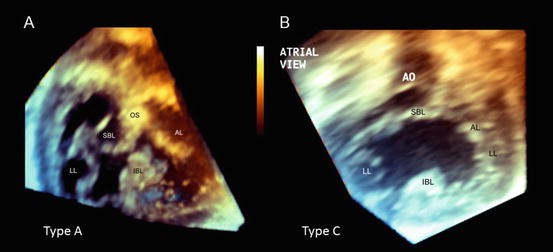
Complete atrioventricular septal defect. (a) An en face image of Rastelli type A. (b) An en face image of Rastelli type C. AL anterior leaflet, AO aorta, IBL inferior bridging leaflet, LL lateral leaflet, OS outlet septum, SBL superior bridging leaflet
Fig. 2.12 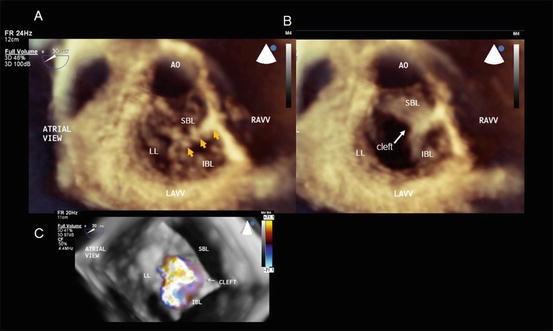
Partial atrioventricular septal defect after repair. (a) An en face image in the closed position. Arrows indicate the sutured cleft and the cleft is oriented towards the middle of the ventricular septum. (b) An en face image in the opened position. (c) A corresponding image to that in panel A by color Doppler three-dimensional echocardiography. Significant regurgitation is seen from the residual cleft and the commissure between the inferior and lateral leaflets. AO aorta, IBL inferior bridging leaflet, LAVV left atrioventricular valve, LL lateral leaflet, RAVV right atrioventricular valve, SBL superior bridging leaflet
-
2.
Common-Inlet Atrioventricular Connection
The common-inlet atrioventricular connection is characterized by the connection of both atria to a single ventricular chamber by a common AVV. This type of atrioventricular connection is usually associated with a common atrium and is predominantly observed in patients with heterotaxy syndrome, especially in those with right atrial isomerism (RAI). The connection of the common AVV and the underlying ventricle is classified into three types, and this classification is used in Shizuoka Children’s Hospital (Shizuoka, Japan) (Fig. 2.13). Type A refers to a balanced connection, with the common AVV communicating equally with both underlying ventricles, and accounts for 46 % of patients with RAI. Type B is an unbalanced connection, with the common AVV communicating predominantly with the unilateral ventricular chamber, and accounts for 19 % of RAI patients. Type C is the univentricular connection, with the common AVV communicating solely with the unilateral chamber, and accounts for 35 % of RAI patients. Figure 2.14 shows 3DE and 2DE images of type B with severe AVV regurgitation. In patients with RAI, the grade of AVV regurgitation is closely related to prognosis [19].
Fig. 2.13 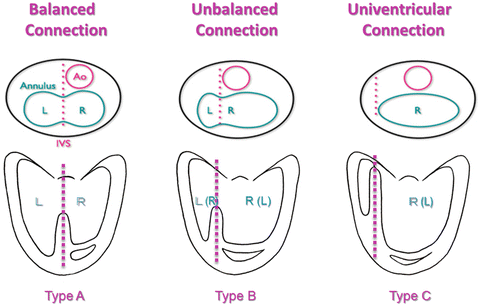
Classification of atrioventricular connections in heterotaxy syndrome (Shizuoka Children’s Hospital Classification). AO aorta, L left ventricle, R right ventricle
Fig. 2.14 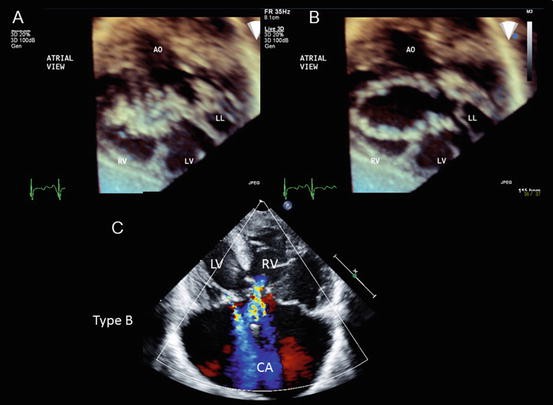
Common-inlet atrioventricular connection in right atrial isomerism (type B). (a) An en face image in the closed position. (b) An en face image in the opened position. (c) Severe atrioventricular valve regurgitation. AO aorta, CA common atrium, LL lateral leaflet, LV left ventricle, RV right ventricle





3 Functional Assessment of the Atrioventricular Valve by Three-Dimensional Echo
3.1 Assessment of the Shape and Area of the Annulus in the AVV
The AVV leaflet is exposed to large fluid shear stresses, hydrostatic pressure, and large in-plane tensions during the systolic phase. Under these stresses, the AVV leaflet expands its area by as much as about 50 % by stretching its undulated collagen fibers [20, 21]. The leaflet expands to its limit very quickly at the beginning of valve closure. This expansion is followed by a plateau phase and a dramatic increase of leaflet stiffness to prevent further leaflet deformation. To cope with leaflet stress, the leaflet is configured into a curved surface during the systolic phase, which is called billowing. The annulus is known to form a saddle shape during systole. The saddle shape of the annulus and the billowing of the leaflet are the main components for the leaflet curvature formation that contributes to the reduction of leaflet stress (Fig. 2.15) [22]. Like the MV annulus, the TV annulus also forms a saddle shape (Fig. 2.16) [23]. Salgo et al. showed that leaflet stress is minimized when the ratio of saddle height to commissural width, which is a surrogate of annular saddle-shaped nonplanarity, is over 20 % [22]. A 3DE study found that in normal human adults this ratio is 24 ± 5 % [24]. Furthermore, the saddle shape of the annulus optimizes force distribution on the chordal system as the load is divided more evenly among the chordae with a saddle-shaped annulus than with a flat annulus [25]. The close relationship between the flattening of the annulus and the worsening of MV prolapse due to the elongation or rupture of the chordae has been reported [24]. On the other hand, leaflet stress also works as a leaflet coaptation force for the prevention of regurgitation. For example, the anterior leaflet of the MV is positioned parallel to systolic flow in the LV outflow tract, and the force exerted by the blood stream on the anterior leaflet works as a coaptation force, and also it expands the aortic valve annulus and enhances the saddle shape of the MV annulus during systole. Therefore, stress on the leaflet works both ways, and as long as the stress on the leaflet and the tension on the chordae are balanced, the leaflet functions normally. However, if a congenital abnormality of the valve or valvular apparatus or an incorrect surgical repair causes abnormally increased leaflet stress, it leads to valve failure.

The effect of stress reduction by leaflet billowing in a computer model. (a) Stress on leaflet without billowing of leaflet. (b) Stress on leaflet with billowing of leaflet. Note the significant stress reduction (blue color) resulting from the billowing curvature of the leaflet under the same saddle shape conditions. Leaflet stress is calculated based on the von Mises distortion energy theory. A warm color is associated with higher stress (Salgo et al. [22]; with permission)

Saddle shape of the mitral and tricuspid valves. The bending angle becomes most acute in early diastole in the mitral and tricuspid valves. AO aorta, IC isovolumic contraction, IR isovolumic relaxation, MV mitral valve, RVOT right ventricular outflow tract, SEM standard error of the mean, TV tricuspid valve
In normal children, the saddle shape becomes the most prominent at early diastole in both the MV and TV (Fig. 2.16) [23], and the grade of the saddle shape is closely related to ventricular function and the grade of regurgitation (Fig. 2.17) [26]. The annulus becomes flat when there is significant AVV regurgitation or reduced ventricular function, placing more stress on the leaflets and leading to further worsening of regurgitation [24, 26]. The area of the annulus also has an important role in maintaining normal AVV function. It has been known that, in adults, the annular area of the MV becomes small during systole to support good leaflet coaptation and reduce leaflet stress and that during diastole it expands to reduce resistance of the annulus to blood inflow [27, 28]. However, this pattern of annular area change during the cardiac cycle is not always the case in children. In the majority of children, the annular area of the MV expands during systole and reaches maximum before the opening of the MV. This pattern is similar to the change of left atrial volume during the cardiac cycle, suggesting the influence of left atrial volume on the annular area [23]. In the TV, the annular area becomes small during systole and expands during diastole in children, which is the same pattern as that observed in adults [29]. The reduction of annular area by ventricular septal bowing towards the right ventricle during systole is especially important for retaining good leaflet coaptation, as the mobility of the septal leaflet of the TV is limited compared to that of the other two leaflets. Atrial contraction is also an important factor in the reduction of the annular area in advance of the beginning of systole; the MV reduces its area by about 10 % during atrial contraction, and the TV reduces its area by about 16 %, suggesting a greater dependence of areal reduction on atrial contraction in the TV [23].

Saddle shape and grade of tricuspid valve regurgitation in hypoplastic left heart syndrome. The saddle shape of the tricuspid valve becomes flat with the progression of regurgitation. IC isovolumic contraction, IR isovolumic relaxation, TR tricuspid valve regurgitation, TV tricuspid valve
3.2 Papillary Muscle and Chordal Position in 3DE
The position and function of the papillary muscles are also very important factors for maintaining normal AVV function. To cope with the force on the leaflets, the papillary muscles generate tension and shorten during systole so as not to cause prolapse of the leaflets. The contraction and shortening of papillary muscle occurs as follows: isometric contraction of the papillary muscle coincides with isovolumic contraction of the ventricle, and the shortening of the papillary muscle begins at the early ejection phase and continues throughout the ejection phase and also during the isovolumic relaxation phase [30]. Although the contraction of the papillary muscle is important for normal AVV function, the position of the papillary muscles has been elucidated as an even more crucial factor for AVV function through enthusiastic investigations of functional mitral regurgitation in adults after myocardial infarction. Three-dimensional echocardiography (3DE) enabled us to assess the spatial relationship among the papillary muscles, annulus, and leaflets [24, 31]. The lateral displacement of the papillary muscle from the annulus due to LV enlargement or myocardial infarction causes the abnormal tethering of leaflets and an imbalance of the force distribution on the chordae, leading to regurgitation [31, 32]. The lateral displacement of the papillary muscle is also a cause of TR in patients with HLHS or left AVV regurgitation in AVSD after repair [26, 33].
3.3 Prolapse and Tethering Analysis in 3DE
The commercially available software MVQ (QLAB Cardiac 3DQ; Philips Medical Systems, Andover, MA) allows for quantitative geometrical measurement of AVV based on acquired transesophageal 3DE data [34]. This software assists in the step-by-step creation of a three-dimensional AVV model, proceeding through the annulus, coaptation line, leaflets, and tips of the papillary muscles, and the created AVV model can be manipulated in a three-dimensional space and overlaid on three simultaneous orthogonal planes (Fig. 2.18). Based on the created three-dimensional AVV model, MVQ is able to measure the following parameters: the intercommissural and anteroposterior annular diameters, the annular area, the area, length, and angle of each leaflet, the tethering height, the coaptation leaflet angle, and the angle between the aortic valve annulus and AVV annulus. The 3DE data also provide quantitative information on tethering, prolapse, and billowing of the leaflet. Takahashi and Smallhorn analyzed tethering and prolapse volume of leaflets and showed a close relationship between tethering or prolapse volume and grade of TR in patients with HLHS [35]. They also showed that prolapse is closely related to annular dilation and age, suggesting that prolapse is mostly a secondary change due to increased stress on the chordae and leaflet over the years. On the other hand, tethering is more frequently seen in younger patients, suggesting an intrinsic abnormality of the chordae and/or papillary muscles. It may also be related to the hemodynamic condition of the palliative stage. The volume overload and coronary insufficiency caused by systemic to pulmonary artery shunting sometimes lead to ventricular dilation and/or dysfunction [17]. The ventricular dilation leads to the enlargement of the annulus, ventricular dysfunction leads to a flat annular shape, and both ventricular dilation and dysfunction lead to a lateral displacement of the papillary muscles and leaflet tethering, which are all causative of increased leaflet stress and maldistribution of force on the chordae and, hence, of chordal elongation or rupture and prolapse of the leaflet. These factors are all interrelated and form feedback loops, sometimes causing a vicious cycle (Fig. 2.19).

Three-dimensional mitral valve model created by MVQ. (a) The simultaneous orthogonal planes of the mitral valve based on transesophageal three-dimensional echocardiography volume data. (b) A three-dimensional mitral valve model. The leaflet area colored in red signifies prolapse, and the area colored in blue signifies tethering. A anterior, AL anterolateral, P posterior, PM posteromedial

Interrelation of atrioventricular valve regurgitation and ventricular dilation and/or dysfunction. EDP end-diastolic pressure, PM papillary muscle
3.4 Quantitative Assessment of Regurgitation
The quantitative assessment of AVV regurgitation by echocardiography remains challenging. Although several echocardiographic methods have been proposed, a true gold standard evaluation is still lacking. Measurement of the effective regurgitant orifice area (EROA) and regurgitant volume is currently recommended as a quantitative assessment. The proximal isovelocity surface area method or the pulsed Doppler-derived flow volume method is used to estimate EROA or regurgitant volume. However, both methods are indirect measurements based on several imprecise assumptions. The well-accepted surrogate to the direct measurement of EROA is the vena contracta width, which is the narrowest cross section of the regurgitant jet. However, as the EROA is not always circular, it cannot be assessed by a vena contracta width in a single dimension by 2DE. 3DE enables the direct measurement of EROA by placing the cropping plane perpendicular to the jet direction at the narrowest area of the jet stream. The EROA is then measured by manual planimetry of the color Doppler jet signal. This method is reportedly accurate and the regurgitant volume can be estimated as the vena contracta area multiplied by the velocity time integral of the regurgitant jet on the continuous-wave Doppler [36]. However, the low temporal resolution of color Doppler 3DE due to the slow volume rate is a limitation of current 3DE systems.
Conclusion
3DE offers new insights into AVV anatomy and function. An en face view of the AVV from the atrial side created by 3DE approximates the surgeon’s view, making it easier for echocardiologists to communicate the anatomy and pathology of the AVV to surgeons prior to the operation. Moreover, 3DE ushered in a new era of functional assessment of the AVV by enabling the creation of a three-dimensional computer model. This modality has an enormous potential to deepen our knowledge and may ultimately lead to virtual AVV repair if three-dimensional anatomical information is combined with pulsed Doppler-derived 3D flow dynamics information.
References
Kruithof BPT, Krawitz SA, Gaussin V (2007) Atrioventricular valve development during late embryonic and postnatal stages involves condensation and extracellular matrix remodeling. Dev Biol 302:208–217
McCarthy KP, Ring L, Rana BS (2010) Anatomy of the mitral valve: understanding the mitral valve complex in mitral regurgitation. Eur J Echocardiogr 11:i3–i19
Ho SY (2002) Anatomy of the mitral valve. Heart 88:iv5–iv10
Angelini A, Ho SY, Anderson RH, Davies MJ, Becker AE (1988) A histological study of the atrioventricular junction in hearts with normal and prolapsed leaflet of the mitral valve. Br Heart J 59:712–716
Silver MD, Lam JHC, Ranganathan N, Wigle ED (1971) Morphology of the human tricuspid valve. Circulation 43:333–348
Davachi F, Moller JH, Edwards JE (1971) Disease of the mitral valve in infancy: an anatomic analysis of 55 cases. Circulation 43:565–579
Carpentier A, Chauvaud S, Mihaileanus S (1990) Classification of congenital malformations of the mitral valve and their surgical management. In: Crupi G, Parenzan L, Anderson RG (eds) Perspectives in pediatric cardiology, vol 2. Part 3, Pediatric cardiac surgery. Future Publishing, Mt Kisco
Zias EA, Mavroudis C, Backer CL, Kohr LM, Gotteiner NL, Rocchini AP (1998) Surgical repair of the congenitally malformed mitral valve in infants and children. Ann Thorac Surg 66:1551–1559
Petitalot JP, Chaix AF, Bonneau G, Rousseau G, Barraine R (1987) Latent congenital mitral insufficiency caused by an isolated mitral cleft. Diagnosis by two-dimensional echocardiography and pulsed Doppler. Ann Cardiol Angeiol (Paris) 36(7):347–350
Greenfield W (1876) Double mitral valve. Trans Pathol Soc (London) 27:128–129
Zalzstein E, Hamilton R, Zucker N, Levitas A, Gross GJ (2004) Presentation, natural history, and outcome in children and adolescents with double orifice mitral valve. Am J Cardiol 93:1067–1069
Rusted IE, Scheifley CH, Edwards JE (1956) Studies of the mitral valve. II: certain anatomic features of the mitral valve and associated structures in mitral stenosis. Circulation 14:398–406
Bruce CJ, Pellikka PA, Connolly HM (2009) Tricuspid stenosis and regurgitation. In: Wang A, Baashore TM (eds) Valvular heart disease. Humana, New York
Aaron BL, Mills M, Lower RR (1976) Congenital tricuspid insufficiency: definition and review. Chest 69:637–641
Carpentier A, Chauvaud S, Mace L, Relland J, Mihaileanu S, Marino JP, Abry B, Guibourt P (1988) A new reconstructive operation for Ebstein’s anomaly of the tricuspid valve. J Thorac Cardiovasc Surg 96:92–101
Chauvaud S, Mihaileanu S, Gaer J, Carpentier A (1996) Surgical treatment of Ebstein’s malformation—the ‘Hôpital Broussais’ experience. Cardiol Young 6:4–11
Ohye RG, Gomez CA, Goldberg CS, Graves HL, Devaney EJ, Bove EL (2004) Tricuspid valve repair in hypoplastic left heart syndrome. J Thorac Cardiovasc Surg 127:465–472
Cetta F, Minich L, Edwards W, Dearani JA, Puga FJ (2008) Atrioventricular septal defects. In: Allen HD, Driscoll DJ, Shaddy RE, Feltes TF (eds) Moss and Adam’s Heart disease in infants, children, and adolescents, 7th edn. Lippincott Williams & Wilkins, Philadelphia
Ota N, Fujimoto Y, Hirose K, Tosaka Y, Nakata T, Ide Y, Sakamoto K (2010) Improving results of atrioventricular valve repair in challenging patients with heterotaxy syndrome. Cardiol Young 20:60–65
Sacks MS, He Z, Baijens S, Wanant S, Shah P, Sugimoto H, Yoganathan AP (2002) Surface strain in the anterior leaflet of the functional mitral valve. Ann Biomed Eng 30:1281–1290
He Z, Sacks MS, Baijens L, Wanant S, Shah P, Yoganathan AP (2003) Effects of papillary muscle position on in-vitro dynamic strain on the porcine mitral valve. J Heart Valve Dis 12:488–494
Salgo IS, Gorman JH, Gorman RC, Jackson BM, Bowen FW, Plappert T, Sutton MG, Edmunds LH (2002) Effect of annular shape on leaflet curvature in reducing mitral leaflet stress. Circulation 106:711–717
Nii M, Roman KS, Mcowan CK, Samllhorn JF (2005) Insight into normal mitral and tricuspid annular dynamics in pediatrics: a real-time three-dimensional echocardiographic study. J Am Soc Echocardiogr 18:805–814
Lee AP, Hsiung MC, Salgo IS, Fang F, Xie JM, Zhang YC, Lin QS, Looi JL, Wan S, Wong RHL, Underwood MJ, Sun JP, Yin WH, Wei J, Tsai SK, Yu CM (2013) Quantitative analysis of mitral valve morphology in mitral valve prolapse with real-time 3-dimensional echocardiography: importance of annular saddle shape in the pathogenesis of mitral regurgitation. Circulation 127:832–841
Jimenez JH, Soerensen DD, He Z, He S, Yoganathan AP (2009) Effects of a saddle shaped annulus on mitral valve function and chordal force distribution: an in vitro study. Ann Biomed Eng 31:1171–1181
Nii M, Guella V, Roman KS, Mcowan CK, Samllhorn JF (2006) Three-dimensional tricuspid annular function provides insight into the mechanisms of tricuspid valve regurgitation in classic hypoplastic left heart syndrome. J Am Soc Echocardiogr 19:391–402
Ormiston JA, Shah PM, Tei C, Wong M (1982) Size and motion of the mitral valve annulus in man, II: abnormalities in mitral valve prolapse. Circulation 65:713–719
Kaplan SR, Basheim G, Sheehan FH, Legget ME, Munt B, Li XN, Silvarajan M, Bolson EL, Zeppa M, Arch M, Martin RW (2000) Three-dimensional echocardiographic assessment of annular shape changes in the normal and regurgitant mitral valve. Am Heart J 139:378–387
Tei C, Pilgrim JP, Shah PM, Ormiston JA, Wong M (1982) The tricuspid valve annulus: study of size and motion in normal subjects and in patients with tricuspid regurgitation. Circulation 66:665–671
Marzilli M, Sabbah HN, Goldstein S, Stein PD (1985) Assessment of papillary muscle function in the intact heart. Circulation 71:1017–1022
Otsuji Y, Handschumacher MD, Liel-Cohen N, Tanabe H, Jiang L, Schwammenthal E, Guerrero JL, Nicholls LA, Vlahakes GJ, Levine RA (2001) Mechanism of ischemic mitral regurgitation with segmental left ventricular dysfunction: three-dimensional echocardiographic studies in models acute and chronic progressive regurgitation. JACC 37:641–648
Nielsen SL, Nygaard H, Fontaine AA, Hasenkam JM, He S, Anderson NT, Yoganathan AP (1999) Chordal force distribution determines systolic mitral leaflet configuration and severity of functional mitral regurgitation. JACC 33:843–853
Takahashi K, Mackie AS, Thompson R, Al-Naami G, Inage A, Rebeyka IM, Ross DB, Khoo NS, Colen T, Smallhorn JF (2012) Quantitative real-time three-dimensional echocardiography provides new insight into the mechanisms of mitral valve regurgitation post-repair of atrioventricular septal defect. J Am Soc Echocardiogr 25:1231–1244
Shanks M, Delagado V, Ng ACT, van der Kley F, Schuijf JD, Boersma E, van de Veire NRL, Nucifora G, Bertini M, de Roos A, Kroft L, Schalij MJ, Bax JJ (2010) Mitral valve morphology assessment: three-dimensional transesophageal echocardiography versus computed tomography. Ann Thorac Surg 90:1922–1929
Takahashi K, Inage A, Rebeyka M, Ross DB, Thompson RB, Mackie AS, Smallhorn JF (2009) Real-time 3-dimensional echocardiography provides new insight into mechanisms of tricuspid valve regurgitation in patients with hypoplastic left heart syndrome. Circulation 120:1091–1098
Marsan NA, Westenberg JJM, Ypenburg C, Delgado V, van Bommel RJ, Roes SD, Nucifora G, van der Geest RJ, de Roos A, Riber JC, Schalij MJ, Bax JJ (2009) Quantification of functional mitral regurgitation by real-time 3D echocardiography. J Am Coll Cardiol Img 2:1245–1252
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Japan
About this chapter
Cite this chapter
Nii, M. (2015). Assessment of Atrioventricular Valve Anatomy and Function in Congenital Heart Diseases Using Three-Dimensional Echocardiography. In: Senzaki, H., Yasukochi, S. (eds) Congenital Heart Disease. Springer, Tokyo. https://doi.org/10.1007/978-4-431-54355-8_2
Download citation
DOI: https://doi.org/10.1007/978-4-431-54355-8_2
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-54354-1
Online ISBN: 978-4-431-54355-8
eBook Packages: MedicineMedicine (R0)