
Summary
This chapter will cover the challenges that we have in considering drug resistance in the context of use of antileishmanial drugs. This is not just a problem of lack of definition but also absence of suitable models and assays. We do not have the standardized and validated assay that can define drug “susceptibility”, that is, the in vitro response of a strain/isolate to a standard drug under defined conditions. We do not have the pharmacokinetic and pharmacodynamic data that defines drug “sensitivity” that is the response of a strain/isolate to a standard drug under defined dose and dose schedule with knowledge of pharmacokinetics and the immune status of the host. Without these pieces of information, it is not possible to establish the “breakpoints” for each antileishmanial drug, that is, the susceptibility value that distinguishes wild-type population of parasites from those with acquired or selected resistance mechanisms. The requirements for surveillance and monitoring of drug susceptibility in control/elimination programmes and to guide treatment programmes will also be considered.
The second challenge to be considered will be the nature of the current antileishmanials and knowledge about their mechanisms of action and resistance in relation to the development of molecular markers. We already have resistance to pentavalent antimonials and knowledge of the complexity of the mechanism of action. There are also an increasing number of relapses to Amphotericin-B treatment being reported and markers sought for resistance to this drug. There are also studies on the two new drugs, Miltefosine and paromomycin, which might give an indication of potential markers, as well as sitamaquine which is currently on clinical trial. The third challenge relates to the known variation in the response of different strains and species to standard antileishmanial drugs. There are 17 species of Leishmania that infect humans, and their responses have been documented by different methodologies. The variation in response to drugs shows the possibility of both “intrinsic” and “acquired” resistance. The importance of this resistance, and how it is monitored, also depends upon whether the infection is anthroponotic or zoonotic.
This is a preview of subscription content, log in via an institution.
Buying options
Tax calculation will be finalised at checkout
Purchases are for personal use only
Learn about institutional subscriptionsReferences
Ashutosh, Sundar S, Goyal N (2007) Molecular mechanisms of antimony resistance in Leishmania. J Med Microbiol 56:143–153
Cantón E, Espinel-Ingroff A, Pemán J (2009) Trends in antifungal susceptibility testing using CLSI reference and commercial methods. Expert Rev Anti Infect Ther 7:107–119
Chappuis F et al. (2007) Visceral leishmaniasis: what are the needs for diagnosis, treatment and control? Nat Rev Microbiol 5:873–882
Cos P et al. (2006) Anti-infective potential of natural products: how to develop a stronger in vitro ‘proof-of-concept’. J Ethnopharmacol 106:290–302
Croft SL (2001) Monitoring drug resistance in leishmaniasis. Trop Med Int Health 6:899–905
Croft SL (2004) Drug resistance in leishmaniasis. In: WHO/TDR Scientific Working Group report on Leishmaniasis. World Health Organization, TDR/SWG/04, pp 108–119
Croft SL, Sundar S, Fairlamb AH (2006) Drug resistance in leishmaniasis. Clin Microbiol Rev 19:111–126
Croft SL, Yardley V, Davies C (2005) Drug resistance monitoring in Leishmaniasis. In: Raghunath D, Nayak R (eds) Trends and Research in Leishmaniasis. The 5th Sir Dorabji Tata symposium. Tata-McGraw-Hill Publishing Co. Ltd. New Delhi, pp 167–192
Dorlo TP et al. (2008) Pharmacokinetics of Miltefosine in Old World cutaneous leishmaniasis patients. Antimicrob Agents Chemother 52:2855–2860
Drusano GL (2004) Antimicrobial pharmacodynamics: critical interactions of “bug and drug”. Nat Rev Microbiol 2:289–300
Dutta A et al. (2005) Development of a modified MTT assay for screening antimonial resistant field isolates of Indian visceral leishmaniasis. Parasitol Int 54:119–122
Ephros M, Waldman E, Zilberstein D (1997) Pentostam induces resistance to antimony and the preservative chlorocresol in Leishmania donovani promastigotes and axenically grown amastigotes. Antimicrob Agents Chemother 41:1064–1068
EUCAST definitive document EDef 7.1 (2008) Method for the determination of broth dilution MICs of antifungal agents for fermentative yeasts. Clin Microbiol Infect 14:398–405
Evans DA (1993) In vitro cultivation and biological cloning of Leishmania. Methods Mol Biol 21:29–41
Fumarola L, Spinelli R, Brandonisio O (2004) In vitro assays for evaluation of drug activity against Leishmania spp. Res Microbiol 155:224–230
Guerin PJ, Bates SJ, Sibley CH (2009) Global resistance surveillance: ensuring antimalarial efficacy in the future. Curr Opin Infect Dis 22:593–600
Hastings IH, Nsanzabana C, Smith TA (2010) A comparison of methods to detect and quantify the markers of antimalarial drug resistance. Am J Trop Med Hyg 83:489–495
Inocêncio da Luz R et al. (2009) In vitro sensitivity testing of Leishmania clinical field isolates: preconditioning of promastigotes enhances infectivity for macrophage host cells. Antimicrob Agents Chemother 53:5197–5203
Jhingran A et al. (2009) Paromomycin: uptake and resistance in Leishmania donovani. Mol Biochem Parasitol 164:111–117
Kumar D et al. (2009) In vitro susceptibility of field isolates of Leishmania donovani to Miltefosine and Amphotericin-B: correlation with sodium antimony gluconate susceptibility and implications for treatment in areas of endemicity. Antimicrob Agents Chemother 53:835–838
Lachaud L et al. (2009) Parasite susceptibility to Amphotericin-B in failures of treatment for visceral leishmaniasis in patients co-infected with HIV type 1 and Leishmania infantum. Clin Infect Dis 48:e16–e22
Laurent T et al. (2007) Epidemiological dynamics of antimonial resistance in Leishmania donovani: genotyping reveals a polyclonal population structure among naturally-resistant clinical isolates from Nepa. Infect Genet Evol 7:206–212
Lourens C et al. (2010) Implementation of a reference standard and proficiency testing programme by the World Wide Antimalarial Resistance Network (WWARN). Malar J 9:375
Mikus J, Steverding D (2000) A simple colorimetric method to screen drug cytotoxicity against Leishmania using the dye Alamar Blue. Parasitol Int 48:265–269
Mondal S, Bhattacharya P, Ali N (2010) Current diagnosis and treatment of visceral leishmaniasis. Expert Rev Anti Infect Ther 8:919–944
Natera S et al. (2007) Leishmania spp.: proficiency of drug-resistant parasites. Int J Antimicrob Agents 29:637–642
Nichols JH (2009) Verification of method performance for clinical laboratories. Adv Clin Chem 47:121–37
Picot S et al. (2009) A systematic review and meta-analysis of evidence for correlation between molecular markers of parasite resistance and treatment outcome in falciparum malaria. Malar J 8:89
Rex JH et al. (1997) Development of interpretative breakpoints for antifungal susceptibility testing. Clin Infect Dis 24:235–247
Rijal S et al. (2007) Antimonial treatment of visceral leishmaniasis: are current in vitro susceptibility assays adequate for prognosis of in vivo therapy outcome? Microbes Infect 9:529–535
Roberts WL, Berman JD, Rainey PM (1995) In vitro antileishmanial properties of tri- and pentavalent antimonial preparations. Antimicrob Agents Chemother 39:1234–1239
Seifert K, Escobar P, Croft SL (2010) In vitro activity of anti-leishmanial drugs against Leishmania donovani is host cell dependent. J Antimicrob Chemother 65:508–511
Sibley CH, Guerin PJ, Ringwald P (2010) Monitoring antimalarial resistance: launching a cooperative effort. Trends Parasitol 26:221–224
Sundar S, Rai M (2002) Laboratory diagnosis of visceral leishmaniasis. Clin Diagn Lab Immunol 9:951–958
Sundar S et al. (2011) Comparison of short-course multidrug treatment with standard therapy for visceral leishmaniasis in India: an open-label, non-inferiority, randomised controlled trial. Lancet 377:477–486
Tripathi P, Singh V, Naik S (2007) Immune response to Leishmania: paradox rather than paradigm. FEMS Immunol Med Microbiol 51:229–242
Turnidge J, Paterson DL (2007) Setting and revising antibacterial susceptibility breakpoints. Clin Microbiol Rev 20:391–408
Vermeersch M et al. (2009) In vitro susceptibility of Leishmania donovani promastigote and amastigote stages to anti-leishmania reference drugs: practical relevance of stage-specific differences. Antimicrob Agents Chemothe 53:3855–3859
World Health Organisation (2010) Methods for surveillance of antimalarial drug efficacy. WHO, Geneva
WHO Technical Report Series (2010) 949, Control of the leishmaniasis: report of a meeting of the WHO Expert Committee on the Control of Leishmaniases, Geneva, 22–26 March 2010
Williams C et al. (2003) Hydrosoluble formazan XTT: its application to natural products drug discovery for Leishmania. J Microbiol Methods 55:813–816
Wyllie S, Cunningham ML, Fairlamb AH (2004) Dual action of antimonial drugs on thiol redox metabolism in the human pathogen Leishmania donovani. J Biol Chem 279:39925–39932
Yardley V et al. (2006) American tegumentary leishmaniasis: is antimonial treatment outcome related to parasite drug susceptibility? J Infect Dis 194:1168–1175
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Technical Procedures
Technical Procedures
Procedure 1: Biphasic culture media for primary isolation of promastigotes from spleen or bone marrow aspirates
Although several culture media have been described for primary isolation of promastigotes from clinical diagnostic samples, biphasic blood-based media are still considered to be most appropriate and sensitive (Sundar and Rai 2002). The basic composition of promastigote media has been described in practical detail (Evans 1993) with some minor modifications.
A. Biphasic NNN (Novy McNeal Nicolle) medium
– Solid phase (for 100 mL)
Bacto agar (Difco) | 2.0 g |
Sodium chloride (NaCl) | 0.6 g |
Bi-distilled water | 90 mL |
Stir mix and dissolve the ingredients while heating until the agar melts. Autoclave (121°C, 15 min) and allow to cool down to about 45°C before adding 10 mL rabbit blood*. Quickly aliquot into culture tubes in shallow slant position and allow the agar to solidify. Rapidly cool and store in upright position at 4°C. Culture tubes have to be used within 3 weeks of preparation.
– Liquid overlay phase: is not needed since enough condensation water will form during the cooling process. If needed, a small amount of distilled water can be added.
B. Evan’s modified Tobie’s medium
– Solid phase (for 100 mL)
Bacto agar (Difco) | 1.5 g |
Bacto-tryptose (Difco) | 1.5 g |
Sodium chloride (NaCl) | 0.4 g |
Potassium chloride (KCl) | 0.04 g |
Sodium phosphate (Na2HPO4·12H2O) | 0.5 g |
Bi-distilled water | 80 mL |
Stir mix and dissolve the ingredients while heating until the agar melts. Autoclave (121°C, 15 min) and store at 4°C. For use, melt in boiling water or in a microwave and allow to cool down to about 45°C before adding 20 mL rabbit blood*. Quickly aliquot into culture tubes (1 mL/tube) in shallow slant position and allow the agar to solidify. Rapidly cool and store in upright position at 4°C (to be used within 3 w of preparation)
– Liquid overlay phase (Locke solution, for 100 mL)
Sodium chloride (NaCl) | 0.8 g |
Potassium chloride (KCl) | 0.02 g |
Potassium phosphate (KH2PO4) | 0.03 g |
Magnesium sulphate (MgSO4·7H2O) | 0.01 g |
Sodium bicarbonate (NaHCO3) | 0.1 g |
Glucose | 0.25 g |
Bi-distilled water | 100 mL |
Dissolve the ingredients and adjust the pH at 7.4 with HCl or NaOH. Filter sterilize through a 0.22-μ membrane filter and store at 4°C. Depending on the use indication, antibiotics can be added: penicillin 200 I.U/mL + streptomycin 200 or gentamicin at 200 μg/mL. Just prior to use, add 1 mL Locke solution to the Tobie agar slant.
*Blood from rabbits is freshly collected using a syringe prefilled with heparin (25 I.U. heparin/mL blood).
Remark: Always perform a sterility check on each production batch of culture medium. Check for the presence of bacteria after 24-h incubation at 37°C.
Prodecure 2: Monophasic culture media for axenization of promastigotes
Upon successful primary isolation of promastigotes on biphasic blood-based media, it is useful to adapt them to monophasic-defined medium to allow clean large volume cultivation in support of further investigations (susceptibility testing, metacyclogenesis and infection of macrophage cell cultures, e.a.). In literature, various media have been used, but HOMEM and M199 appear to be the standard. Both media can be considered comparable, except that spontaneous metacyclogenesis can be monitored better in HOMEM.
Materials
-
M199 medium, 10× with Hanks’ salts (Sigma M9163)
-
MEM medium (Invitrogen 31095-029)
-
HEPES (Sigma H3375)
-
Adenine (Sigma A2786)
-
Hemin (Sigma H5533)
-
6-biopterin (Schricks Labs 11.203)
-
L-glutamine 200 mM 100× (Invitrogen 25030-024)
-
Sodium bicarbonate 7.5% (Invitrogen 25080-060)
-
Folic acid (Sigma F8758)
-
D-glucose (Invitrogen 49139)
-
D-biotin (Sigma B4639)
-
Fetal calf serum (inactivated) (Invitrogen 10270.106)
-
Triethanolamine (Sigma T1377)
-
HCl 37% (Merck Biochemicals 101834)
-
NaOH (Sigma S8045)
Stock solutions [stored at 4°C unless otherwise mentioned]
-
Hemin stock: 37.5 mg hemin + 15 mL 50% triethanolamine in water (store at −4°C)
-
Biopterin stock: 50 mg 6-biopterin + 1 mL HCl 1 M + 24 mL distilled water (store at −20°C)
-
Adenine stock: 200 mg adenine + 2.5 mL 1 M NaOH + 17.5 mL Milli-Q water
-
Folic acid stock: 15 mg folic acid + 200 μL 1 M NaOH + 18.5 mL Milli-Q water
-
D-biotin stock: 10 mg D-biotin + 500 μL 1 M NaOH + 19.5 mL Milli-Q water
Procedure 3: Cryopreservation of Leishmania promastigotes
Long-term maintenance of Leishmania strains by serial in vitro subculture is contraindicated as the original characteristics may be lost. This is particularly relevant for drug-susceptibility evaluation of clinical isolates. As such, it is important to deposit isolates in a cryobank as soon as possible after primary isolation. The description of the cryopreservation procedure for promastigotes presented below is a practical summary of information available in the public domain (Evans 1993, WHO technical series 2010) and personal experience.
Materials
-
Promastigote culture in logarithmic growth with a cell density of at least 106/mL
-
Cryoprotectant: DMSO (Sigma 41644)
-
Cryoprotectant: glycerol (Sigma G5516)
-
Biofreezer: −70°C
-
1.8-mL cryopreservation tubes (Nalgene Nunc # 377267); internal screw stop
-
Freezing box “Mr. Frosty®” (Nalgene Nunc # 9400945), filled with 250 mL room temperature isopropanol up to the line mark (isopropanol has to be changed every fifth use or at least once per month).
Procedure for freezing
-
Add the cryoprotectant to the promastigote culture under gentle stirring to obtain a final concentration of 5% DMSO or 10% glycerol.
-
Aliquot 1 mL cell suspension to each cryotube, firmly close the lid and put the tubes into the freezing box. Place the box immediately into a −70°C freezer for 24 h, then into the liquid nitrogen tank.
Procedure for thawing
-
Remove the cryotube from the liquid nitrogen and immediately transfer into a 37°C water bath. Hold the tube in the surface of the water bath while very gently and continuously swaying (do not leave the cryotube unattended during the thawing process). With a small bit of ice still remaining in the tube, transfer the tube into the biosafety hood, dry off the outside, and wipe with 70% ethanol before opening to prevent contamination.
-
Transfer the contents of the tube to 5 mL pre-warmed promastigote medium (37°C) in a culture flask or tube.
Remarks
-
For quality control on each freezing batch, one tube should be used to start a standard in vitro culture; good growth should be obtained within 3–4 days.
-
For long-term storage in liquid nitrogen, DMSO is preferred as cryoprotectant. For storage at −70°C, glycerol is preferably used.
-
Using the freezing box “Mr. Frosty®” approximates the programmed freezing scheme of the following: 1°C/min from +18°C to +2°C, then 5°C/min from +2°C to −18°C and finally 10°C/min from −18°C to −70°C (Evans 1993).
Procedure 4: Cloning of Leishmania promastigotes
In view of the polyclonal nature of Leishmania (Laurent et al. 2007) and dependent on the specific research objectives, it may be indicated to prepare individual clones from the isolate. The only way to ensure that a single promastigote is used as inoculum is by microscopic examination. A particular problem encountered is that single promastigotes mostly fail to grow in culture, the so-called loneliness phenomenon. A practical way to address this problem is the use of spent culture medium and small-volume culture in 96-well microplates.
Materials
-
Flat-bottom 96-well microplates, plastic pipette micro-tips
-
Promastigote culture in logarithmic growth phase
-
Complete M-199 promastigote culture medium
-
“Spent” medium: prepared from a logarithmic growth culture after removal of the promastigotes by centrifugation and filtration (22 μm) of the supernatant. Aliquots are stored at −20°C.
Cloning method
-
Dilute the stock culture 1/100 in complete M199 medium and further prepare a twofold dilution series in a 96-well plate (“donor plate”). Select the well for probing micro-drops that will deliver one organism/drop with a reasonably high probability.
-
The micro-drops are deposited in another 96-well plate (“cloning plate”) (Fig. 2).
Fig. 2 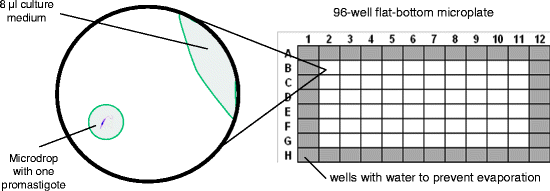
Cloning of promastigotes using the micro-drop method in 96-well plates
-
Place 8 μL complete M199 medium to the side of the wells to minimize evaporation during the manipulations.
-
Insert the micro-tip into the appropriate well in the donor plate and deposit a micro-drop by tip touch in the middle of the “cloning” 96-well plate. Several wells can be done before microscopic verification for the presence of one promastigote (it is advised to have a second person double check).
-
In the wells with one promastigote, 100 μL of “spent” M199 medium is added.
-
Continue the procedure until all the wells of the cloning zone have been processed.
-
Finally, add 100 μL of “complete” M199 medium to the wells with a single promastigote. Fill the remaining wells with 200 μL Milli-Q water.
-
Wrap the “cloning” plate with Parafilm to avoid evaporation and incubate at 25°C.
-
Transfer the grown clones (after ± 1 w) into larger culture tubes with M199 medium.

Procedure 5: Preparation of stock solutions of antileishmanial reference drugs
For in vitro work, it is essential to use pure crystalline substance and avoid commercial drug formulations as vehicle constituents and preservatives may interfere with the outcome of the test. For example, the effects of the preservative chlorocresol in Pentostam® have already been documented (Roberts et al. 1995, Ephros et al. 1997). Furthermore, optimal storage conditions should be adopted to guarantee chemical stability of the compound in hermetically closed bottles in the dark at 4°C. All stock solutions can be made in Milli-Q water.
Reference drugs
Pentavalent antimony (SbV) | Sodium stibogluconate (SSG): Calbiochem 567565 or to be obtained from GSK-UK or Albert David Ltd., India |
Trivalent antimony (SbIII) | Potassium antimonyl tartrate trihydrate (Sigma 383376) |
Amphotericin-B (AmB) | AmB-deoxycholate: Fungizone® (Squibb) |
Miltefosine (MIL) | To be obtained from Zentaris, Frankfurt, Germany |
Paromomycin (PMM) | PMM sulfate (Sigma P9297) |
Preparation of stock solutions
– Sb V (stock solution at 1 mg Sb V eq/mL)
Dissolve 31.9 mg SSG in 10 mL water or PBS while stirring at 37°C for 1 h until a clear solution is obtained. Divide into small aliquots (1 mL) and keep at −20°C. Frozen aliquots may be kept for 3 months. [1 mg SSG contains 0.313 mg SbV eq].
– Sb III (stock solution at 1 mg Sb III eq/mL)
Dissolve 27.7 mg SbIII tartrate in 10 mL water or PBS while stirring until a clear solution is obtained. Divide into small aliquots (1 mL) and keep at −20°C. Frozen aliquots may be kept for 3 months. [1 mg SbIII tartrate contains 0.361 mg SbIII eq].
– AmB (20 mM stock solution)
Dissolve 41 mg Fungizone® powder in 1 mL DMSO 100% to prepare the stock solution. Divide into small aliquots (0.2 mL) and keep at −20°C. Frozen aliquots may be kept for 3 months. Further dilutions are made in water but should be used immediately because of limited stability. [MW = 924.08 – 1 g Fungizone® formulation contains 450 mg AmB].
Note: Amphotericin-B from Sigma (A2411) should not be used because of extreme poor solubility.
– MIL (20 mM stock solution)
Dissolve 81.5 mg MIL in 10 mL water or PBS while stirring until a clear solution is obtained. Divide into small aliquots (1 mL) and keep at 4°C. Aliquots may be kept for 3 months (MW = 407.57).
– PMM (20 mM stock solution)
Dissolve 142.74 mg PMM sulfate in 10 mL water or PBS while stirring until a clear solution is obtained. Divide into small aliquots (1 mL) and keep at 4°C. Aliquots may be kept for 3 months. [MW PMM sulfate = 713.71; PMM base = 615.63/salt factor 1.16].
Procedure 6: Drug-susceptibility assay for promastigotes
The promastigote susceptibility assay in principle follows a same format as the micro-dilution protocols that have been established for bacteria and fungi (EUCAST 2008). For quantification of the viable promastigote burden, we propose the use of the dye resazurin, the principle used in the commercial product alamarBlue® (Mikus and Steverding 2000). The resazurin assay is based on the reduction of the blue-colored resazurin by NADH into the pink-colored strongly fluorescent product resorufin. The extent of resorufin formation is linearly related to the number of viable cells. Less attractive alternatives include microscopic counting or the use of MTT (Dutta et al. 2005) or XTT (Williams et al. 2003).
Preparation of resazurin stock solution
-
PPB (potassium phosphate buffer 0.1 M, pH 7.4): dissolve 2.72 g KH2PO4 (Merck 1.04873.1000) and 18.16 g K2HPO4·3H2O (Sigma P5504) in 1 L distilled water; store the buffer solution in aliquots at 4°C.
-
PPB a : Dissolve resazurin sodium salt (Sigma 199303) at 3 mg/mL in PPB (e.g., 300 mg in 100 mL PPB).
-
PPBb a : Prepare a 30 mM stock of potassium ferricyanide (K3Fe(CN)6) (Sigma P8131) in PPB (e.g., 987 mg in 100 mL PPB); it can be stored at 4°C until use.
-
PPB c : Prepare a 30 mM stock of potassium ferrocyanide (K4Fe(CN)6) (Sigma P9387) in PPB (e.g., 1266 mg in 100 mL PPB); it can be stored at 4°C until use.
Mix equal volumes of PPB a , PPB b , and PPB c and dilute the obtained stock solution 1/20 in PPB to obtain the resazurin use solution. Filter sterilize (0.22 μm) and store in the dark at 4°C. It is advised to prepare a new resazurin solution every 2 weeks.
Micro-dilution susceptibility assay for promastigotes
Materials
-
“96-well” plates (flat-bottom)
-
Resazurin “use” solution
-
Spectrophotometer for fluorimetric reading (filter combination 550/590 nm)
-
Promastigote culture in log-phase growth
-
Stock solutions of antileishmanial reference drugs (Procedure 5)
Promastigote susceptibility assay
-
Log-phase promastigotes are harvested and microscopically counted in a counting chamber (=infection inoculum).
-
Promastigotes are seeded into the wells at 105 promastigotes/well and exposed to the serially diluted drugs in a 96-well plate (specific test plate template and dose range to be designed by the investigator – practical example is presented in Fig. 3).
Fig. 3 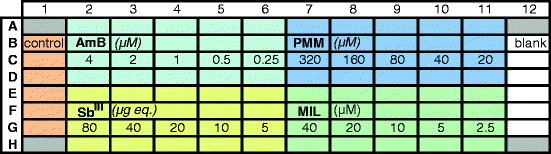
Practical template for susceptibility profiling of promastigotes against current antileishmanial reference drugs (4 replicates/drug). Control: medium inoculated with promastigotes (=100% growth). Blank: medium control without promastigotes (= 0% growth)
-
During incubation for 72 h at 25°C, plates are wrapped in parafilm to avoid evaporation.
-
After the stated incubation period, 50 μL of resazurin use solution is added to each well, and the plates are further incubated for 24 h in the dark.
-
Fluorescence reading using the filter combination 550–590 nm and calculation of the ED50 using appropriate software.

Remark: Pentavalent antimony (SbV) has been shown to be inactive against promastigotes and is not included. Although the exact mechanism of action of antimonials is not yet known, it is generally accepted that SbV is in fact a pro-drug that requires biological reduction to the trivalent form (SbIII) (Wyllie et al. 2004). There are indications that SbIII has some activity against the promastigote stage and has for this reason been included in the panel of drugs.
Procedure 7: Drug-susceptibility assay for intracellular amastigotes
The intracellular amastigote assay is currently considered as the gold standard in drug discovery research and for evaluation of drug resistance in field strains, despite the more complex and labor-intensive protocol (Vermeersch et al. 2009). In this procedure, primary peritoneal mouse macrophages are proposed as host cell, although host cell-dependent variations have been indicated (Seifert et al. 2010). A problem specifically encountered with field strain promastigotes is their variable degree of in vitro growth and metacyclogenesis, influencing the level of cellular infection and hence the outcome of the sensitivity testing. Depending on their growth characteristics, either spontaneous or artificially induced metacyclogenesis can be used (Inocêncio da Luz et al. 2009). A general flowchart of the whole assay is presented in Fig. 4.

Time flow chart of the intracellular amastigote susceptibility test with indication of the option for preconditioning of promastigotes
Isolation and culture of primary peritoneal mouse macrophages (MΦ)
-
Complete culture medium: 500 mL RPMI-1640 (Invitrogen 21875-034) supplemented with 10 mL penicillin-streptomycin (Invitrogen 15140-122), 5 mL L-glutamine (Invitrogen 25030-025) and 25 mL heat-inactivated fetal bovine serum (FCSi)
-
2% starch suspension: weigh 0.2 g potato starch into a test tube and semi-sterilize by incubating at 80°C for at least 2 h. Add 10 mL sterile PBS just before use and stir until all the starch is homogeneously suspended (warm up, if necessary).
-
Stimulation and harvesting of macrophages (MΦ): disinfect the abdomen of Swiss mice (± 25 g, male or female) with 70% ethanol and inject 1 mL of the starch suspension intraperitoneally. Macrophages are collected 2 days later after killing the mice with a CO2 overdose or cervical dislocation. All next steps are executed in a LAF to maintain sterility. After disinfection of the abdomen with 70% ethanol, 10 mL pre-warmed (37°C) complete RPMI-1640 is injected intraperitoneally, after which the abdomen is gently massaged to distribute the fluid and suspend the cells. After removal of the abdominal skin, the exposed peritoneum is disinfected with 70% ethanol, and the abdominal fluid with cells is aspirated. The number of macrophages is determined in a counting chamber, and the cell suspension is appropriately diluted with complete RPMI-1640 (37°C) to obtain a cell suspension of about 300,000 macrophages/mL.
-
Seeding of macrophages: dispense 100 μL macrophage suspension (30,000 macrophages per well) in each well of a 96-multiwell tissue culture plate and incubate at 37°C and 5% CO2 to be used 24 h later.
Metacyclogenesis of promastigotes
Promastigotes in stationary phase are generally used to infect macrophages. However, spontaneous metacyclogenesis of some field isolates is sometimes problematic because of very slow growth. In these cases, preconditioning of promastigotes may be useful to enhance cell infectivity and obtain more stable infections (Inocêncio da Luz et al. 2009).
-
Preconditioning of promastigotes: promastigotes are cultured in M199 medium until day 5 (early stationary phase). The promastigotes are separated by centrifugation, and the culture medium is replaced by Schneider’s medium at pH 5.4, supplemented with 20% FCSi. The promastigotes are incubated for another 24 h at 25°C before being used for infection of macrophages.
In vitro susceptibility test in primary mouse macrophages
-
Prepare a suspension of (preconditioned) metacyclic promastigotes at 3 × 106/mL in RPMI-1640.
-
Add 100 μL promastigote suspension into each well already containing 100 μL macrophage culture (→ infection rate = 10 promastigotes/macrophage) and incubate at 37°C and 5% CO2 for 24 h.
-
Remove the non-internalized promastigotes by discarding the culture medium (200 μL) and replenish by adding 190 μL RPMI-1640 medium to all the wells, making sure not to touch the monolayer and avoid cross-contamination.
-
Finally, transfer with a multichannel pipette 10 μL of the reference drug dilutions 20× onto the infected macrophages (avoid touching the monolayer) and incubate in a CO2 incubator for 4 days at 37°C.
Determination of intracellular amastigote burdens
Giemsa staining procedure
-
20% Giemsa solution: prepare a work solution by diluting Giemsa (Accustain®, Sigma) 1/5 in demineralized water and filter (0.22-μm membrane filter) to remove particulate matter. Always use freshly prepared staining solution (10 mL work solution is needed per 96-well plate).
-
Staining of microtiter plates: discard the medium from each well of the test plates, allow the plates to dry to the air and dispense 150 μL absolute methanol to each well for 10 min (fixation). Next, discard the methanol, allow the plates to dry to the air, dispense 100 μL Giemsa work solution in each well and stain for about 15 min. Discard the Giemsa solution and collect in chemical waste container, rinse the stained plates with tap water and allow drying to the air. The plates are now ready for microscopic reading.
Determination in intracellular amastigote burdens
-
Up till now, microscopic counting is the only option to determine of the total parasite burden, which is calculated as the percentage of infected macrophages X the mean number of amastigotes per macrophage. At least 100 macrophages need to be counted, and the infection is judged adequate if at least 70–80% of the macrophages are infected.
-
The results are expressed as the percent reduction of the total parasite burden compared to the non-treated infected control and the 50% inhibitory concentration (IC50) is calculated using appropriate software (e.g., Statview®).
Remarks
-
An almost identical assay template as proposed in Procedure 5 can be used, except that pentavalent antimony (SbV) should now be included (e.g., by replacing AmB) (Fig. 5).
-
For standard drug-susceptibility assays, polystyrene microtiter plates have sufficient optical qualities for microscopic evaluation of intracellular amastigote burdens (using an invert microscope with long-focus objectives). For more accurate evaluations, LabTek™ culture chambers (Nunc 177445 or 178599) can be used, allowing 500× magnification under oil immersion.
-
In order to more easily compare the results in different experimental series, it is important to include a drug-sensitive reference strain in each test and calculate an activity index (AI), as had been proposed for antimonials (Yardley et al. 2006).
-
In the case that mice are not available for collection of primary macrophages, other macrophage-like cell types can be used (Seifert et al. 2010). Among the different options, J774A.1 and THP-1 cells are most widely used.
-
J774 cells are seeded at 105 cells/well in a 96-well microplate and infected at a multiplicity of infection of 10:1. Plates are microscopically read after Giemsa staining for 10 min.
-
THP-1 cells need to be stimulated with phorbol 12-myristate 13-acetate (PMA, Sigma P8139) before becoming adherent. Variable levels of stimulation may influence the test outcome (levels of adherence and infection).
Fig. 5 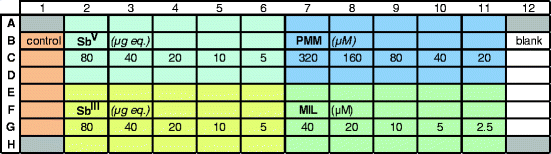
Practical template for susceptibility profiling of intracellular amastigotes in MΦ against current antileishmanial reference drugs (four replicates/drug)
-

Rights and permissions
Copyright information
© 2013 Springer-Verlag Wien
About this chapter
Cite this chapter
Maes, L., Cos, P., Croft, S.L. (2013). The Relevance of Susceptibility Tests, Breakpoints, and Markers. In: Ponte-Sucre, A., Diaz, E., Padrón-Nieves, M. (eds) Drug Resistance in Leishmania Parasites. Springer, Vienna. https://doi.org/10.1007/978-3-7091-1125-3_19
Download citation
DOI: https://doi.org/10.1007/978-3-7091-1125-3_19
Published:
Publisher Name: Springer, Vienna
Print ISBN: 978-3-7091-0238-1
Online ISBN: 978-3-7091-1125-3
eBook Packages: MedicineMedicine (R0)