
Abstract
Reconstruction of skull base defects caused by resection of a tumor, osteoradionecrosis, osteomyelitis, or trauma is a challenging undertaking. The reconstructive surgeon’s aim is to correct the defects while minimizing potentially devastating complications such as cerebrospinal fluid (CSF) leak, meningitis, osteomyelitis, extrusion of hardware, and severe facial deformity. Doing so requires the ability to segregate the intracranial compartment from the oronasal cavities. It is also important to obliterate all surgically caused cavities, in order to improve contours and minimize the hollow appearance and seroma formation. Hardware and exposed bone should be covered with well-vascularized flaps to decrease the chances of exposure or osteoradionecrosis following the nearly inevitable radiation treatment. The surgeon should also be able to improve outcomes of facial nerve injury either by performing static facial nerve reconstruction procedures or by interposing a nerve graft between the proximal and distal segments.
Keywords
12.1 Introduction
Reconstruction of skull base defects caused by resection of a tumor, osteoradionecrosis, osteomyelitis, or trauma is a challenging undertaking. The reconstructive surgeon’s aim is to correct the defects while minimizing potentially devastating complications such as cerebrospinal fluid (CSF) leak, meningitis, osteomyelitis, extrusion of hardware, and severe facial deformity. Doing so requires the ability to segregate the intracranial compartment from the oronasal cavities. It is also important to obliterate all surgically caused cavities, in order to improve contours and minimize the hollow appearance and seroma formation. Hardware and exposed bone should be covered with well-vascularized flaps to decrease the chances of exposure or osteoradionecrosis following the nearly inevitable radiation treatment. The surgeon should also be able to improve outcomes of facial nerve injury either by performing static facial nerve reconstruction procedures or by interposing a nerve graft between the proximal and distal segments.
Most smaller defects associated with skull base surgery can be obliterated by the use of local pericranial, temporalis muscle, or nasal septal flaps. Grafts, such as those taken from the fascia lata or fat, may also be utilized in a well-vascularized environment and for very small gaps. These options have been described in previous chapters of this book.
This chapter deals with the general considerations pertaining to skull base reconstruction and the workhorse free flaps most often used. The specifics of each area and techniques for dealing with the special defects that arise in each area are described.
12.2 Anatomical Considerations
We usually refer to the skull base defects according to the 1994 classification of Irish et al. (Fig. 12.1):
-
Region I: tumors arising in the orbits and sinuses, extending into the anterior cranial fossa
-
Region II: tumors originating in the lateral skull base and pterygopalatine fossae
-
Region III: tumors originating in and involving the ear, parotid gland, and temporal bone, frequently involving the facial nerve to a varying extent
Of course, more than one area may be involved in the defect created by the disease.

Schematic description of the skull base regions (From Irish et al.; with permission)
12.3 Reconstruction Method
Most patients who undergo free flap reconstruction have already undergone surgery, radiation, and chemotherapy. Younger patients are better candidates for free flap reconstruction because they can tolerate longer and more radical procedures.
12.3.1 Analysis of the Defect and Considerations
The various tissue components needed for reconstruction and their three-dimensional properties must be taken into account when planning a free flap reconstruction. Table 12.1 describes various solutions that are available for the different elements injured during ablative surgery (Figs. 12.2, 12.3, 12.4, 12.5, and 12.6).

A chimeric flap on two separate perforators: one supplying the muscular component and the other the fasciocutaneous. The muscle component is trimmed to fit and obliterate the sinus cavity

Bony reconstruction using split calvarial bone grafts connected with mini-plates

Titanium mesh can be used for contour, yet following radiation treatment hardware may extrude if not properly covered with well-vascularized tissues

Patient who underwent orbitomaxillectomy, reconstructed with a muscle flap and skin graft over it. Due to radiation, shrinkage of the flap caused distortion of the facial contour and inferior displacement of the lateral eyebrow. These defects should be overcorrected, and the eyebrow should be fixated to the periosteum of the orbital rim

A fascia lata static sling connecting the lateral oral commissure with the zygomatic arch and temporal fascia. The sling overcorrects the position of the commissure, as the fascia relaxes with time and the corner of the mouth will droop
12.3.2 Flap Variations
The optimal choice of flap is decided upon according to the analysis of the defect and its requirements. The following discussion covers the most commonly used flaps.
12.3.2.1 Anterolateral Thigh Flap
The anterolateral thigh (ALT) flap is the most versatile and most frequently used flap in our institution and many others. The ALT flap may be used solely as a fasciocutaneous flap (Fig. 12.7a) if a thin and pliable tissue is required. It may be harvested as a musculocutaneous flap (Fig. 12.7b), with the muscle component tailored to the exact size of the cavity to be obliterated. It can serve as a chimeric flap combined with different tissues (e.g., skin, fascia, and muscle), each on a different vascular branch (Fig. 12.7c). The lateral femoral cutaneous nerve may be harvested for facial nerve cable grafting, or the nerve to the vastus lateralis may be used if that muscle is taken with the flap. Donor-site morbidity is quite minimal, even if the muscle is included in the flap. Patients can be ambulated on day 1 following surgery. If a large skin paddle is taken, the remaining defect can be skin grafted.

(a) A “pure” fasciocutaneous perforator anterolateral thigh flap, based on two muscle perforators. The perforator on the right splits into three smaller skin vessels. (b) A musculocutaneous flap with the skin and muscle component supplied confluently by the same vessels. (c) A chimeric flap. The muscle component is supplied by a separate side branch as the fasciocutaneous component. This allows for more freedom during inset
The harvesting of an ALT flap involves several steps:
-
1.
A line is drawn between the anterior superior iliac spine and the lateral border of the patella (the AP line). This line delineates the septum running between the rectus femoris and vastus lateralis muscles. Within this septum lies the major pedicle of the flap, including the descending branch of the lateral circumflex femoral artery and vein (Fig. 12.8a).
-
2.
A skin perforator can be Dopplered halfway down the AP line and about 1.5 cm lateral to it. Additional perforators may be found with less consistency about 5 cm proximally and distally to the previously described point along the leg’s axis. Perforators may be either septocutaneous or musculocutaneous (Fig. 12.8b). Dissection through the muscle should be performed for a true fasciocutaneous flap (Fig. 12.7a). When needed, a muscle is harvested en bloc with the perforators passing through it (Fig. 12.7b).
-
3.
The pedicle is dissected proximally, disconnecting all the side branches until it reaches a length and caliber enabling it to anastomose comfortably to the intended recipient vessels (usually at the site where the pedicle contacts the bifurcation of the profunda femoris vessels).
-
4.
The posterolateral incision of the ALT flap’s skin paddle is incised once the defect can be fully assessed and a template of the skin paddle can be made. (We regularly use a piece of rubber Esmarch bandage to etch the contour of the defect as shown in Fig. 12.7c.)
-
5.
Recipient vessels are established and a good blood flow through them is verified. A wide tunnel connecting the defect to the vessels is dissected, usually in a subcutaneous plane. Only then can the free flap be disconnected from its original site and transferred to the surgical defect.

(a) The septum between the rectus femoris and the vastus lateralis is delineated by the anterior superior iliac spine (ASIS)–patella (AP) line. Perforators (crosses) are around the mid-distance of this line and approximately a centimeter lateral to it. (b) After the skin and fascia are incised, the septum between the rectus femoris and vastus lateralis is entered. The descending branch of the lateral femoral circumflex artery (black arrow) is seen at the base of the cleft. Here an anatomical variant can be seen. The first cutaneous perforator (asterisk) is septal, yet is based on a separate branch, off the lateral femoral circumflex, namely, the “diagonal branch.” The two more distal perforators (white arrows) branch off the main vascular trunk and are muscle perforators
12.3.2.2 Radial Forearm Free Flap
A radial forearm free flap (RFFF) is also reliable and simple to harvest. It is very thin and pliable and is excellent for resurfacing superficial defects or folding over for internal and external lining (Fig. 12.9). The Allen test is performed prior to its harvest to verify that the radial flow is not the dominant blood supply to the palm and fingers. The flap is harvested from the nondominant arm and is centered over the course of the radial artery, distally limited by the wrist crease. The radial artery and venae comitantes are dissected up to the cubital fossa.

A radial forearm free flap is very thin and pliable. Here the flap is harvested both with the radial artery and the venae comitantes and with the cephalic vein as an additional venous drainage. Additionally, the lateral antebrachial cutaneous nerve is also seen in the middle between the vascular pedicle and cephalic vein and, if connected to a stump of a sensory nerve, may render the flap sensate
12.3.2.3 Rectus Abdominis Myocutaneous Free Flap
The rectus abdominis myocutaneous free flap was the flap of choice to reconstruct maxillary defects, but it has fallen out of favor since the ALT became popular. It can be harvested with one or more skin paddles, including a cube of rectus abdominis muscle, to fill cavities. It is based on the inferior epigastric artery, which allows a fairly long pedicle. Donor-site morbidity is more pronounced, however, as bulges and hernias may result even with mesh reinforcement of the rectus sheath. Additionally, the flap may be too bulky in heavier patients, and a simultaneous two-team approach is more difficult because of its location.
12.3.2.4 Additional Flaps
If none of the flaps discussed above are suitable, others are available for reconstruction, including the free gracilis muscle flap and the latissimus dorsi flap.
12.3.3 Recipient Vessels
The minimal requirements for recipient vessels are one artery and one vein. If the flap is large or seems to be inadequately drained by a single vein, an additional vein should be connected, preferably to a different drainage system (such as the external jugular). The superficial temporal vessels (Fig. 12.10a) and the facial vessels (Fig. 12.10b) are the closest ones available for defects in the anterior or middle skull base. They should be dissected from distal to as proximal as possible so that the caliber of the vessels is wide enough to match those of the flap. If a neck dissection is performed, the exposed vessels of the neck can be used as recipients. For region III posterior skull base defects, the required pedicle length is relatively short, and care should be taken that it does not kink during insetting and anastomosis.

(a) Close-up view on the vascular pedicle anastomosed to the superficial temporal vessels. To achieve a larger caliber, the vessels must be dissected caudal to the tragus. An implantable Doppler was used in this case; its wires and cellulose cuff engulf the vein (asterisk). (b) Preoperative marking of the facial artery and vein at the mandibular rim. They are easily palpable or Dopplered at this area
12.4 Postoperative Protocol and Flap Monitoring
The first 5 days after microsurgical reconstruction are considered critical for flap survival and recovery from the skull base surgery itself. Many microsurgical teams have developed a protocol to improve flap survival and increase the chances of early detection of flap failure:
-
1.
Flap monitoring every hour for the first 48 h, every 2 h for the next 48 h, and every 4 h for another 24 h.
-
2.
Hyperhydration using crystalloids at 100–120 mL per hour. Fluids are calculated at 150 % of maintenance infusion for pediatric patients. Urine output is maintained at about 0.5–1 mL/kg per hour. Diuretics should be used cautiously because they initially deplete fluids from the intravascular space, thus increasing blood viscosity and the tendency to clot.
-
3.
Blood pressure is maintained above 120 mmHg systolic by adding fluids, colloids, dobutamine, and blood transfusions; the use of adrenergic vasoconstrictors is avoided.
-
4.
Hemoglobin and hematocrit are expected to drop, owing to blood loss during surgery and hemodilution. If not contraindicated, the hemoglobin level is best kept at about 10 mg/dL in order to improve the rheologic properties of the blood.
-
5.
Patients are kept on a fasting regimen for the first 24 postoperative hours in case a revision is required.
-
6.
Antibiotic treatment covering the appropriate flora (i.e., cutaneous or oronasopharyngeal) is administered for the first 5 postoperative days.
-
7.
Subcutaneous low-molecular-weight heparin (enoxaparin) is administered at doses appropriate for deep vein thrombosis prophylaxis (40–80 mg once daily) until the patient begins ambulating. The addition of aspirin, full-dose enoxaparin, or polydextran has been shown to increase hemorrhagic and hemodynamic complications, with minimal impact on flap vessel thrombosis. Patients at risk for thrombosis or those who have undergone several revisions of the vascular anastomosis during surgery should receive the full dosage of enoxaparin (1 mg/kg twice daily).
-
8.
The head is kept in a neutral position at 30° elevation. No pressure is applied to the flap itself, the area of anastomosis, or the course of the pedicle.
Flap monitoring includes both clinical evaluation and Doppler reading. Clinically, the flap is checked for color, capillary refill, and temperature. Blood flow is usually assessed with a handheld Doppler device. Superficial nylon 5-0 sutures marking the location of the monitoring perforators or vessels are placed at the end of surgery, as marking pen ink may easily be wiped off. Preferably, both arterial and venous signals should be audible. Alternatively, an implantable Doppler device can be used, especially for muscle flaps (which are clinically more challenging to monitor) or for flaps that are completely buried. The device may be placed on either the artery or the vein. We prefer to monitor the vein because the signal will stop immediately if either an artery or a vein clots, whereas it may take several hours for the flow in an artery to stop in the event of a venous thrombosis. Venous coupling devices are now available with an embedded Doppler probe, and they provide an excellent option.
If intracranial surgery is performed or if the dura is opened, we prefer to admit the patient to the neurosurgical intensive care unit at least overnight.
Unless the patient requires treatment in the neurosurgical ICU, he or she will be transferred to the department that is most familiar with flap monitoring for the following 5 days and is discharged when feeling well and ambulating. Bed restriction or continuous cardiovascular monitoring is usually not required after the first 24 h.
12.5 Complications
Complications can be categorized into surgical site, donor-site, and medical complications.
12.5.1 Surgical Site Complications
Surgical site complications such as CSF leak or meningitis may result from the nature of the intracranial surgery. Measures to minimize the CSF pressure on the surgical site can improve the chances that the flap will achieve a watertight seal, at least in the early recovery period. These measures include head elevation and placement of a continuous CSF drain with removal of 10–20 mL of fluid per day. A fulminating infection may be arrested by perioperative antibiotics and a high level of suspicion of an even minimal sign.
The most dreaded complication of free flap reconstruction is flap failure, due to either arterial or venous thrombosis. Most thrombi will form on the anastomosis suture line and cause ischemia or retrograde stasis. Early recognition and prompt treatment of thrombosis will provide the best chances for flap salvage. Flow must be reinstituted promptly by opening the anastomosis, extracting the thrombus, removing any possible contributing factor (e.g., hematoma, kink, or possible constricting tissues), and reanastomosing the vessel. Additionally, any thrombi inside the flap can be melted by tissue plasminogen activator or streptokinase administered via an intra-arterial injection, leaving the vein open for drainage. Partial flap loss may be encountered in free flaps, usually requiring debridement of the necrotic area after demarcation has been completed. Depending upon the nature of the new defect, the final solutions may include secondary healing, a skin graft, or occasionally an additional flap.
12.5.2 Donor-Site Complications
The most common donor-site complication we encounter is seroma, especially when an ALT flap is used. To minimize this complication, the drain is left inside until the patient begins ambulating and secretions are less than 30 mL per day. An elastic bandage or compression stockings are worn for about 1 month following surgery. Local hematoma should be prevented during surgery by meticulous hemostasis and placement of a large-bore drain in the wound bed.
Sensory loss is often encountered in the area superolateral to the knee when an ALT flap is harvested and in the snuffbox when a radial forearm flap is used. Sparing of the superficial sensory nerve is good policy, unless the nerve is required for reconstruction. The area of numbness often decreases over time, as sensation is regenerated from the surrounding nerve territories.
Wound healing complications are comparatively rare. They can be treated with standard modalities such as dressing changes, antibiotic treatment, and additional surgery, if warranted.
12.5.3 Medical Complications
The medical complications in these patients should not differ from the complications of larger-scale, prolonged surgeries. These patients often suffer from comorbidities such as cardiac, diabetic, and pulmonary conditions. (Several studies put the figure at about 10 % of these patients.) Overhydration should be performed with special care in patients suffering from renal and cardiac conditions.
12.6 Specific Considerations for Microsurgical Reconstruction of Skull Base Defects
12.6.1 Anterior Cranial Fossa Reconstruction
A number of specific problems must be addressed while reconstructing the anterior skull base.
-
1.
Watertight and complete segregation between the nasal cavity and the intracranial compartment. To achieve a watertight closure, we usually use either de-epithelialized skin or vascularized fascia. A template of the defect is created and cut out of either a rubber Esmarch bandage or foam dressings (Figs. 12.7c and 12.11). It is important to plan the flap so that the vascular pedicle is not facing the intranasal cavity, but rather is directed to the virtual space between the flap and the intracranial compartment. If the flap faces the nasal cavity, the skin can be left intact unless it proves to be too bulky. The muscle can also be used in this setting, but it is more difficult to achieve complete sealing because the muscle may shrivel at its edges.
Fig. 12.11 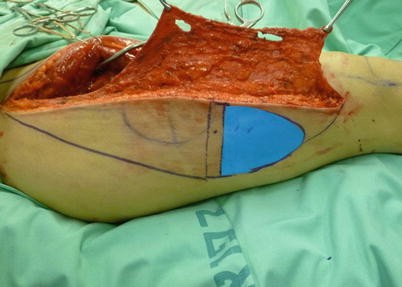
The ALT flap is harvested with an extension of vascularized fascia lata at the anteromedial border of the flap. We use a blue rubber Esmarch to delineate the defect border, which then is transferred to the donor site and facilitates cropping the flap to the exact size needed, even prior to detaching the flap from its blood supply
-
2.
Securing the flap posteriorly in the area of the optic chiasm. It may be difficult to secure the flap posteriorly if there is a bony defect that extends posteriorly to the optic chiasm. It is possible to “stuff” the flap over the remaining bony shelves and reinforce it by intranasal packing, although there may be some shifting of the flap and breach of the nasal–intracranial seal. We usually insert multiple stay sutures, anchoring them onto the dura margins anteriorly when possible. Posteriorly, where the dura is too thin to hold sutures, we drill holes into the skull base (the sphenoid wings) and pass 4-0 resorbable sutures through them in order to secure the flap (Fig. 12.12a). The sutures are then passed through the flap’s edges at the appropriate location, and the surgeon “parachutes” the flap posteriorly into the defect, while the assistant maintains equal tension on all the sutures (Fig. 12.12b).
Fig. 12.12 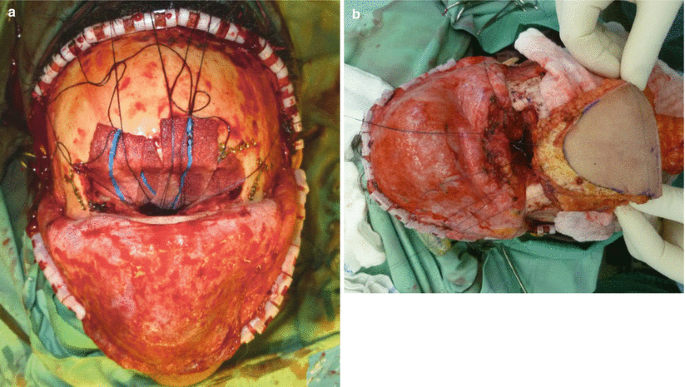
(a) Absorbable 4-0 sutures are passed through holes drilled in the posterior bony rims and are left with the needle as stay sutures until the flap is ready for inset. (b) The flap is “parachuted” into the defect as the stay sutures are held with tension. The skin paddle of the flap is directed inferiorly into the nasal cavity and ethmoidal sinus to the left of the picture, while the vascular pedicle is superior and facing the intracranial compartment
-
3.
Reconstructing a bony contour of the forehead and orbital rims. Contour reconstruction may be achieved by using soft tissue alone. We often find that an excellent contour can be preserved by using de-epithelialized skin under the bicoronal skin flap, especially if there will be no postoperative radiation (Fig. 12.13a–d). A rigid substitution will be needed if the bandeaux or superior orbital rim is removed during surgery. If the bone is not involved in the pathologic process, it may be returned after a window has been created to allow the pedicle to pass through it to the recipient vessels. The orbital rim can be reconstructed using titanium mesh folded into the precise shape. Covering the defect with a flap and forehead skin usually provides an excellent contour and support for the orbits. This procedure is recommended when postoperative radiation will not be required (Fig. 12.14a–e).
Fig. 12.13 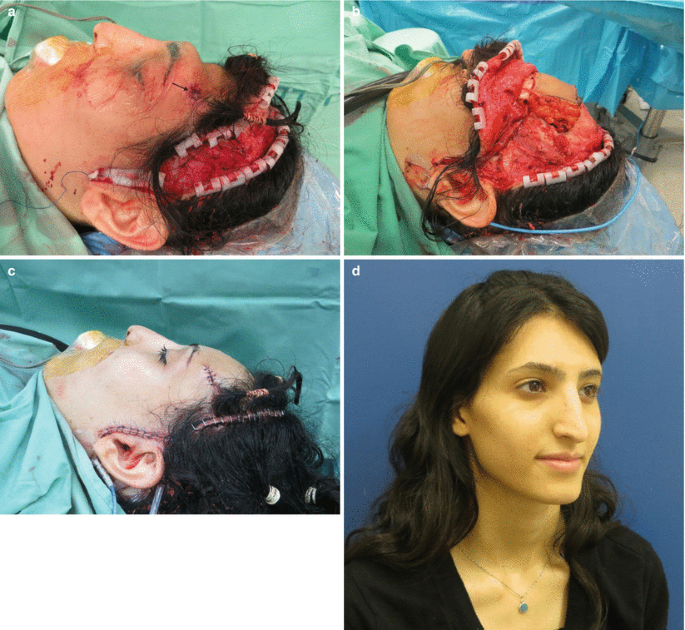
(a) A 24-year-old patient with chronic osteomyelitis of the frontal bone and a fistula to the skin (arrow) underwent removal of the affected bone, leaving significant contour deformity. (b) A de-epithelialized free ALT flap was placed in order to cover the exposed dura and improve the forehead contour. (c) This can be appreciated both at the end of surgery and 1 year postoperatively; no loss of volume is noted (d)
Fig. 12.14 
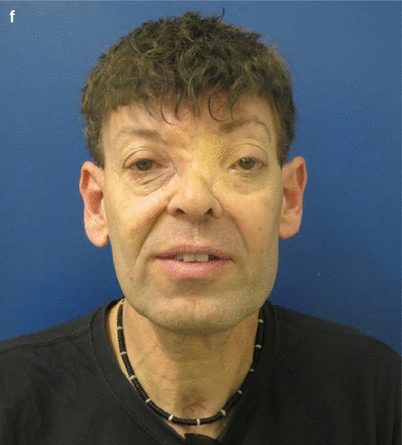
A 48-year-old man with multiple recurrences of a frontoethmoidal meningioma, though benign, destroyed the bony structures and caused exophthalmos and dystopia of the eyes (a, b). The tumor was resected through a combined bicoronal (c) and Weber–Ferguson (d) approach removing the skin of the nasal radix, as the tumor was adherent there. A titanium mesh was used to rebuild the superomedial orbital rims (c), and a large chimeric ALT was used to obliterate both the frontal and the left maxillary cavities (e). (f) The patient underwent several revisions to minimize the size of the skin paddle and decrease its bulk
Another good option is a bone graft. Depending on the required size, the bone may be harvested from a floating rib (either the 10th or 11th). The chest area is marked and the skin is injected with lidocaine and adrenaline. The skin and muscles are elevated off the rib, and the anterior periosteum is incised in an H-shaped incision. The rib is elevated using a periosteal elevator off the posterior periosteum, and an appropriately sized segment is cut off the remaining rib by either a saw or a bone biter. The muscles and skin of the chest are then closed over a thyroid drain, which may be removed in the ensuing days (Fig. 12.15a–d)..
Fig. 12.15 
A 55-year-old man following resection of an adenocarcinoma of the frontoethmoidal sinuses. (a) The bony contour was reconstructed with a “T-bar” created from a split rib graft. (b) The grafts were “sandwiched” in a folded radial forearm free flap and anastomosed to the facial vessels. Final contour can be appreciated both at the end of surgery (c) and in postoperative imaging studies (d)
Other options for bone graft harvesting are a split calvarial bone graft and the internal plate of the iliac crest, although these may be more appropriate for defects of the orbital floor.
-
4.
External skin defect. If external skin is required in addition to a buried component, several options may be considered:
-
The flap may be folded upon itself, with a strip of epithelium removed from the area that is in contact with the subcutaneous tissues. For very thin flaps, it should be taken into account that some of the blood flow to the dermis is via the dermal plexus, and de-epithelialization may damage blood supply to the remaining flap (Fig. 12.16a–d).
-
The flap can be divided into two skin paddles, each based on a separate perforator. This method allows for more versatility in insertion, but there is a danger that one of the flap perforators may thrombose (Fig. 12.17).
-
Skin grafting can be performed over a fascial or muscle portion of the flap lining the skin defect.
Fig. 12.16 
Recurrent adenocarcinoma of the nasal cavity, in a 45-year-old female, presenting as chronic sinus in the right superomedial orbital rim and forehead (a). (b) A free fasciocutaneous ALT flap was harvested according to a template of the skull base defect, and an additional epidermal island was left to close the forehead defect. (c) The flap is parachuted into the defect, with the skin paddle facing the intranasal cavity, and then folded superiorly to cover the frontal region. The postoperative period was not complicated by CSF leakage, as the flap completely obliterated the cavity. (d) Postoperative pictures show closure of the two defects by small skin islands
Fig. 12.17 
Multiple separate skin paddles and muscle components can be taken on different perforators as a chimeric flap and serve for internal and external lining
-
-
5.
Orbital exenteration defect. Defects in region I may involve removal of the contents of the orbital socket. If the medial and inferior walls of the orbit remain intact, the goals of the reconstruction should be limited to lining of the orbit and allowing for a future prosthesis. To achieve a successful prosthetic rehabilitation, the socket area should be left concave in relation to the facial surface. The orbit will granulate and eventually epithelialize if left alone for secondary healing with dressing changes. Most of these patients will require postoperative chemoradiation that cannot always be delayed until the wound heals, however, so we advocate lining the defect with a thin flap, such as a gracilis muscle or a vastus lateralis muscle (Fig. 12.18a–e). The flaps are skin grafted with a split-thickness graft and will rapidly lose their bulk. To prevent a downward pull of the eyebrow, the brow can be sutured to the periosteum of the supraorbital rim. It should be kept in mind that the vascular pedicle of the gracilis muscle free flap is quite short and will probably reach only to the superficial temporal vessels. In contrast, the vastus lateralis has an exceptionally long pedicle, but it may kink or twist and may fare better if anastomosed to the facial or neck vessels.
Fig. 12.18 
A 4-year-old girl with rhabdomyosarcoma of the orbit underwent orbital exenteration (a). A vastus lateralis muscle flap was harvested to fill the whole cavity of the orbit, and anastomosed to the facial vessels, and covered by a thin split-thickness skin graft (b, c). Six months after surgery and radiation treatment (d), she is now referred to fit an ocular prosthesis (e) to match her remaining eye. Note that the muscle flap has contracted and can now suitably fit the volume of such prosthesis
-
6.
Combined defects with maxillary sinuses. These defects involve skull base regions I and II. If the anterior wall of the maxillary sinus is removed, the maxillary sinus needs to be filled, usually by a muscle component of the flap, in order to preserve the cheek contour. If both the anterior and nasal walls are removed, filling is even more important, because air may inflate the cheek flap.
An ALT flap is raised as a chimeric flap, with a muscle cuff included over the terminal vessels of the descending branch of the lateral femoral circumflex artery (Fig. 12.19a–c). It is trimmed to fill the size of the cavity. The muscle component usually does not need to be secured by sutures. If there is a defect of the medial nasal wall, however, we anchor the flap to the rim of the piriform aperture of the soft tissue at the base of the nose. A silicone nasal airway is left in place for at least 1 month, in order to allow the airway to mucosalize without synechiae to the nasal septum (Figs. 12.20 and 12.21).
Fig. 12.19 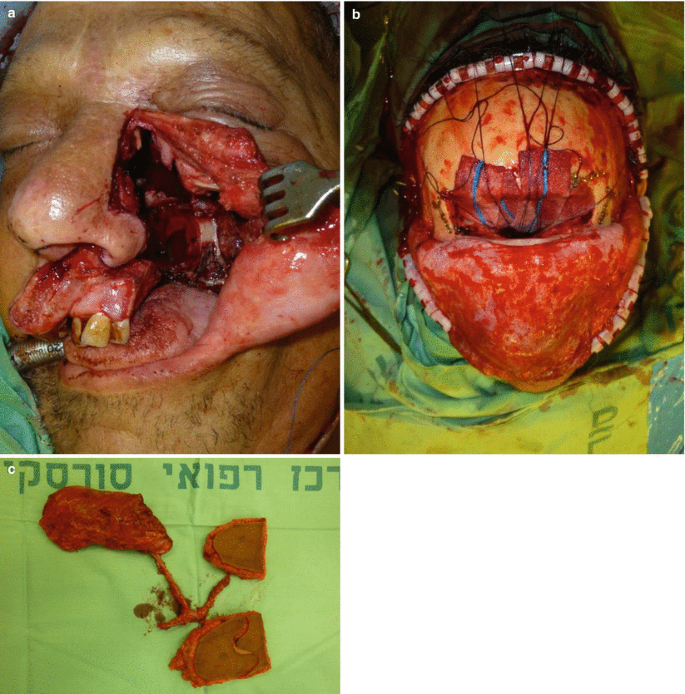
Resection of a recurrent squamous cell carcinoma involving the lateral nasal wall, maxillary and ethmoidal sinuses, and the left hemi-palate in a 67-year-old man (a). (b) A combined approach was used to obliterate all three cavities: skull base, maxillary, and palate. (c) A chimeric three-paddle musculocutaneous ALT flap was harvested
Fig. 12.20 
Anterior maxillectomy involving the lower eyelid, cheek skin, and anterior, superior, and medial maxillary walls (a). The flap harvested with a fascia extension in all dimensions, which served both as lining of the nasal sidewall, and as a sling attached to the medial and lateral canthi for lower eyelid reconstruction alongside a Hughes flap (b). The muscle component is used to obliterate the maxillary sinus and pad the titanium mesh (c)
Fig. 12.21 
A soft nasal airway is used to prevent the flap and nasal walls to form synechiae
-
7.
Blood vessel availability. The superficial temporal vessels are the closest recipient vessels for region I skull base defects. Although these vessels are consistently present, dissection should be performed proximally in order to achieve a larger caliber just before their descent under the parotid gland at the level of the tragus. Care must be taken to examine the patient meticulously for preauricular pulses and to determine whether previous surgery has been performed in this area, because a bicoronal incision may damage these vessels. In addition, the superficial temporal vessels may have been included in a prior radiation field, in which case it may be prudent to choose other available recipient vessels, such as the facial vessels or those further caudal in the neck (e.g., the external carotid and superior thyroid). The facial artery is often transected during level I neck dissection and may have been rendered unsuitable for use. The facial vessels can be palpated or Dopplered; they are dissected out through a 3-cm incision just caudal to the mandibular rim, taking care not to damage any fibers of the marginal mandibular nerve that may cross their path.












12.6.2 Middle Cranial Fossa Defect Reconstruction
The medial cranial fossa is approached medially via a Weber–Ferguson incision or laterally through a transmaxillary or temporal approach. Resection via a medial approach will include some of the walls of the maxillary sinus. Reconstruction of such defects requires restoring the barrier between the intracranial compartment and the oronasal compartment.
-
1.
Suprastructure maxillary defects. These defects include exposure of the dura and possibly also the maxillary vessels, thus requiring hardware reconstruction of the orbital floor. The temporalis muscle is rarely sufficient to reach the cavity medially and entirely obliterate it.
A muscle-only flap, however, can fill this cavity and provide additional vascularized padding to any hardware that may be inserted. The gracilis muscle is one good option, although anastomosis should be to the superficial temporal vessels because the vascular pedicle length is relatively short. The vastus lateralis muscle is an even a better option. It can be tailored to the exact size required (see Fig. 12.20a–c), and the pedicle is long enough to reach the facial vessels or the neck vessels if needed, and a fascial extension can be taken with the muscle to cover any hardware placed.
The rectus abdominis is also an excellent donor site for a muscle-only flap or a musculocutaneous flap. Again, a muscle tailored to the exact size required can be harvested, and the inferior epigastric pedicle length is quite long, to reach the recipient vessels. Donor-site morbidity may be more significant than with other flaps, however. Fascia closure should be reinforced with an inlaid taut Prolene mesh that is secured with nonabsorbable sutures through the rim of the anterior rectus sheath to avoid future bulging. An abdominal binder should be worn for 4–6 weeks postoperatively.
-
2.
Lateral approach defects. These may be combined region II and III defects, which may require a transmaxillary approach and the removal of the mandibular ramus and the posterolateral maxilla. The defect may include both internal oral lining and external skin. Bony reconstruction of the posterolateral mandible is usually not required, and soft tissue alone is sufficient to replace its bulk. An excellent option for this reconstruction is a rectus abdominis flap and an ALT flap, with two skin paddles on separate perforators. Alternatively, if the intraoral defect is minimal, a muscle-only flap sutured to the defect’s edges will effectively mucosalize within about 2 weeks and will adequately seal the intraoral contents.
12.6.3 Posterior Cranial Fossa Defects
These defects usually involve the auricular, mastoid, and temporal bone region, often involving some or all of the facial nerve branches.
-
1.
Total or partial auriculectomy defects. The repair of total auriculectomy defects is usually straightforward (Fig. 12.22a–f). A large fasciocutaneous, ALT, or rectus abdominis flap can cover the entire area as a patch. If the defect is deeper because of bony resection, a muscle component can be included and fitted into the deeper areas so that the external surface will be level due to the stacking of the two components.
If the auditory canal is preserved, the flap is designed in a kidney shape that surrounds the canal, and the thinned skin edges or fasciae are thinned and funneled into the canal (Fig. 12.23a–c). It is our experience, however, that even the thinnest flaps are not thin enough and that the canal narrows with time, so that efforts to preserve it ultimately yield marginal benefit. At least the superior third of the auricle should be preserved if possible, so that eyeglasses can be supported (Fig. 12.24a–c).
Fig. 12.22 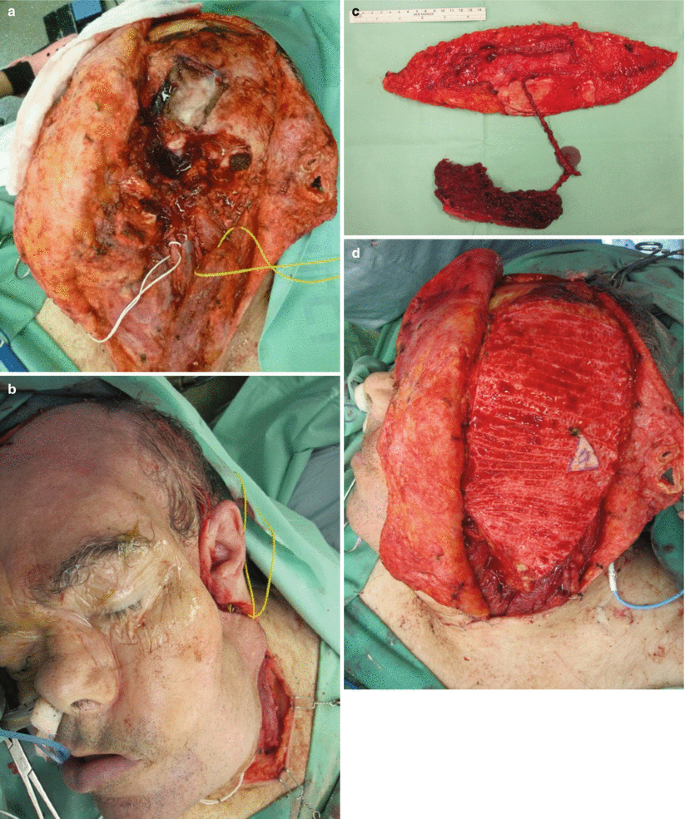

A large parotidectomy, lateral skull base resection, and external auditory canal and middle ear resection, with preservation of the external ear structures (a). A significant deformity is created if left in reconstructed, as well as high probability of surgical site complications such as seroma, infection, and CSF leak (b). A large chimeric ALT flap is harvested (c), and totally de-epithelialized, apart from a tiny skin paddle left to obliterate the auditory meatus (d, e). The contour improvement can be viewed at the end of surgery (f)
Fig. 12.23 
A total parotidectomy, mandibular ramus resection, and anterior auditory canal resection, following a large parotid SCC metastasis in a 62-year-old man (a). The defect was reconstructed with a fasciocutaneous ALT flap. The fascia lata served also as a static sling and it was funneled into the auditory canal and sutured to the skin there. It was stented primarily with a Merocel (Medtronic; Minneapolis, MN, USA) foam stent (b), and later the patient returned to wearing a fitted hearing aid (c)
Fig. 12.24 
Long-standing osteoradionecrosis of the temporal bone, 15 years following parotidectomy and radiation treatment (a). The affected bone has been thoroughly removed, yet the superior third of the auricle was left intact (b, c) as to support eyeglasses
-
2.
Facial nerve repair. Resection of some or all of the branches of the facial nerve is fairly common when surgery involves the posterior cranial fossa. Once a nerve is severed, the fascicles distal to the cut will undergo Wallerian degeneration. Following primary repair or nerve graft interposition between the two cut edges, however (Fig. 12.25a), function will reportedly return regardless of the patient’s age, comorbidities, or postoperative radiation treatment. Therefore, we attempt these repairs whenever possible, even if only to maintain some static tone. Some function can return within 6 months, and recovery may continue up to 2 years following surgery. These repairs should be done under the microscope, with the native nerves and grafts at no tension whatsoever. The nerves are sutured with 10-0 or 11-0 nylon sutures connecting the perineurium on both sides. We try to coapt the edges so that no fascicles are seen to protrude from the suture line, with the aim of ensuring the growth of more nerve fibers along the entire conduit to the target organ (Fig. 12.25b). A nerve graft is usually reversed, anastomosing the distal nerve graft to the proximal nerve stump and vice versa, again in order to minimize the loss of nerve fascicles through the side branches.
There are multiple donor sites for nerve grafts. The greater auricular nerve is the most readily available, but it is short and usually quite wide, making it more suitable as a single graft. Alternatively, the fascicles of the greater auricular may be divided to form two branches. Another classic donor site is the sural nerve. It can be harvested either proximal to distal (starting between the two heads of the gastrocnemius muscle, dissecting the nerve and following it more distally) or distal to proximal (starting posterior to the lateral malleolus and following it more proximally). The former method seems to result in a smaller area of loss of sensation at the lateral foot.
Nerve grafts can also be taken while harvesting the flap. For example, the lateral femoral cutaneous nerve can be dissected with an ALT. Alternatively, the nerve to the vastus lateralis of the muscle can be included in the flap, whereupon the vastus lateralis is taken and is no longer the nerve’s target organ. In a radial forearm flap, the lateral antebrachial cutaneous nerve is found in the subcutaneous fat of the forearm and can easily be taken as a nerve graft along with the flap (Fig. 12.9).





(a) A cable graft taken from the lateral femoral cutaneous nerve. The proximal end is marked. This graft can be used to interpose between a main stump and two nerve endings, or its fascicles can be divided and used as two separate nerve grafts. (b) Intraoperative view of three cable grafts of the facial nerve to the frontal, zygomatic, and buccal branches (clockwise, respectively)
12. Conclusions
Microsurgical skull base reconstruction is a valuable tool in the practitioner’s armamentarium. It supplies solutions to the larger and more complicated cases of defects that follow previous surgery and chemoradiation, with better preservation of function, aesthetics, and quality of life.
Suggested Reading
Chang DW, Robb GL. Microvascular reconstruction of the skull base. Semin Surg Oncol. 2000;19:211–7.
Dean NR, White HN, Carter DS, Desmond RA, Carroll WR, McGrew BM, Rosenthal EL. Outcomes following temporal bone resection. Laryngoscope. 2010;120:1516–22.
Fliss DM, Gil Z, Spektor S, Leider-Trejo L, Abergel A, Khafif A, Amir A, et al. Skull base reconstruction after anterior subcranial tumor resection. Neurosurg Focus. 2002;12:e10. 15.
Gil Z, Fliss D. Pericranial wrapping of the frontal bone after skull base tumor resection. Plast Reconstr Surg. 2005;116:395–8.
Hanasono MM, Silva A, Skoracki RJ, Gidley PW, DeMonte F, Hanna EY, et al. Skull base reconstruction: an updated approach. Plast Reconstr Surg. 2011;128:675–86.
Heffelfinger R, Murchison AP, Parkes W, Krein H, Curry J, Evans JJ, Bilyk JR. Microvascular free flap reconstruction of orbitocraniofacial defects. Orbit. 2013;32:95–101.
Iida T, Mihara M, Yoshimatsu H, Hara H, Koshima I, Kawai K, et al. Reconstruction of an extensive anterior skull base defect using a muscle-sparing rectus abdominis myocutaneous flap in a 1-year old infant. Microsurgery. 2012;32:622–6.
Irish JC, Gullane PJ, Gentili F, Freeman J, Boyd JB, Brown D, Rutka J. Tumors of the skull base: outcome and survival analysis of 77 cases. Head Neck. 1994;16:3–10.
Marzi SJ, Benscoter B, Leonetti JP. Contemporary options for lateral skull base reconstruction following tumor extirpation. Curr Opin Otolaryngol Head Neck Surg. 2011;19:330–4.
Mohammed-Ali RI, Robbins AE, Hussain O, Fitzgerald A, Carroll T, Smith AT, Yousefpour A. Six-year retrospective study of reconstructive options for defects of the skull base after resection of tumour. Br J Oral Maxillofac Surg. 2013;51:719–24.
Richmon JD, Yarlagadda BB, Wax MK, Patel U, Diaz J, Lin DT. Locoregional and free flap reconstruction of the lateral skull base. Head Neck. 2014. doi:10.1002/hed.23725.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Berlin Heidelberg
About this chapter
Cite this chapter
Fliss, D.M., Gil, Z. (2016). Microsurgical Reconstruction of Skull Base Defects. In: Atlas of Surgical Approaches to Paranasal Sinuses and the Skull Base. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-48632-0_12
Download citation
DOI: https://doi.org/10.1007/978-3-662-48632-0_12
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-48630-6
Online ISBN: 978-3-662-48632-0
eBook Packages: MedicineMedicine (R0)