
Abstract
Severe tissue trauma leads to an early activation of several danger recognition systems, including the complement and the coagulation system, often resulting in an overwhelming almost synchronic pro- and anti-inflammatory response of the host. Although the immune response is associated with beneficial effects at the site of injury including the elimination of exogenous and endogenous danger molecules as well as the initiation of regenerative processes, an exaggerated systemic inflammatory response significantly contributes to posttraumatic complications such as multiple organ failure (MOF) and early death. Besides pre-existing physical conditions, age, gender, and underlying comorbidities, surgical and anesthesiological management after injury is decisive for outcome. Improvements in surgical intensive care have increased number of patients who survive the initial phase after trauma. However, instead of progressing to normal recovery, patients often pass into persistent inflammation, immunosuppression, and catabolism syndrome (PICS). The characterization and management of PICS will require new strategies for direct monitoring and therapeutic intervention into the patient’s immune function. In this chapter, we describe various factors involved in the inflammatory changes after trauma and aim to understand how these factors interact to progress to systemic inflammation, MOF, and PICS.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- DAMP
- Cytokines
- Serine-Protease System
- Coagulopathy
- Complementopathy
- Neutrophils
- Monocytes/Macrophages
- Organ Dysfunction
4.1 Introduction
Multiple trauma results in a significant blood loss and accumulation of necrotic and/or devitalized tissue in an ischemic-hypoxic environment, both of which will become the origin of coagulatory and inflammatory changes. The inflammatory response after polytrauma is a major part of the host’s molecular danger response. The acute posttraumatic phase of inflammation consists of two rather synchronically mounted columns: the pro-inflammatory response (systemic inflammatory response syndrome, SIRS) and the anti-inflammatory response (compensatory anti-inflammatory response syndrome, CARS) [1]. SIRS includes changes in the heart rate, respiratory rate, temperature regulation, and immune cell activation (Table 4.1) [2]. In the natural course of the inflammatory response after trauma, the balance of the pro- and anti-inflammatory response is in equilibrium, which maintains the biological homeostasis and induces controlled regeneration processes, enabling the patient to recover normally without significant complications. However, the excessive inflammatory response after trauma seems to simultaneously and rapidly involve the induction of innate (both pro- and anti-inflammatory mediators) and suppression of adaptive immunity [1, 3, 4] all of which decisively contribute to the development of the early multi-organ dysfunction syndrome (MODS). Furthermore, a prolonged and dysregulated immune-inflammatory state is associated with delayed recovery and complications, especially the development of late MODS. Based on improved intensive care and organ support, there is often a progress to the clinically evident persistent inflammation, immune suppression, and catabolism syndrome (PICS) which might have replaced the late MODS, but still is associated with a poor outcome, appearing as “silent death” [5].
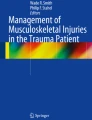
The steps of an inflammatory reaction to trauma involve fluid phase mediators (cytokines, chemokines, coagulation- and complement activation products, oxygen radicals, eicosanoids, and nitric oxide (NO)) and cellular effectors (neutrophils, monocytes/macrophages, and endothelial cells) that translate the trauma-induced signals into cellular responses. These factors are closely interrelated and interconnected by up-regulatory and down-regulatory mechanisms. The combination of these factors may cause severe SIRS, acute respiratory distress syndrome (ARDS) and sepsis, acute kidney injury (AKI), progressing to MODS, depending on the type of injured tissue, the surgical and anesthesiological management after injury, age, gender, genetics, and most importantly, underlying comorbidities and physical conditions (exogenous and endogenous factors) (Fig. 4.1).

Trauma-induced systemic inflammatory response syndrome (SIRS) and complications; NO nitric oxide, ROS reactive oxygen species, NK cells natural killer cells, MOF multiple organ failure
4.2 Damage-Associated Molecular Patterns
Patient survival after severe trauma requires an adequate molecular and cellular danger response. The injured tissues release cytosolic molecules (e.g., ATP), organelles (e.g., mitochondria), histones, nucleosomes, DNA, RNA, matrix, and membrane fragments, all functioning as damage-associated molecular patterns (DAMPs). Furthermore, damage of external and internal barriers (e.g., skin, gut-blood barrier, air-blood barrier, brain-blood barrier) facilitates invasion of microorganisms, resulting in additional exposure to microorganisms-derived pathogen-associated molecular patterns (PAMPs). After multiple injury, the immune system of the injured patient is exposed to both DAMPs (also termed alarmins) and PAMPs, which are summarized as danger-associated molecular patterns [6]. The “3-R-challenge” for the innate and adaptive immune system is to recognize, respond to, and resolve the “molecular danger”. For recognition of the damage, there are effective fluid-phase “master alarm systems”, such as the coagulation and complement cascade, and effective cellular “danger sensors”, such as the pattern recognition receptors (PRR). These systems transfer the damage/danger signals to the cells which in turn mount an acute phase reaction and inflammatory response to resolve the damaged tissue load [7].
4.3 Acute-Phase Reaction
Within an hour after trauma, inflammation resulting from tissue injury induces an increase in plasma concentration of a number of liver-derived proteins (the acute phase proteins, APP). Pro-inflammatory cytokines (IL-1β, TNF, IL-6) released locally by Kupffer cells can systemically influence other cell types such as hepatocytes to synthesize more APPs. Proactive APPs, such as C-reactive protein (CRP), procalcitonin (PCT), serum amyloid A (SAA), complement activation products (C3a, C5a), activated coagulation proteins (FVIIa, FXa, FIIa), proteinase inhibitors, and metal-binding proteins, are increased during this phase [8], whereas the production of inhibitory APPs, such as albumin, high-density lipoprotein (HDL), protein C, protein S, and ATIII are decreased [9, 10].
Plasma concentrations of CRP are normally below 10 mg/l [11]. Hepatic synthesis of CRP is regulated mainly by IL-6. Serum levels of CRP can be detected about 12 h after systemic detection of IL-6. Clinically, the plasma levels of CRP are relatively non-specific and may not correlate with injury severity and are not predictive of posttraumatic complications such as infections [12]. In the context of trauma, it is also still unclear whether the native pentameric or the denatured monomeric form of CRP is responsible for the CRP-induced cellular effects [13].
PCT is physiologically produced in the thyroid gland as the precursor molecule of calcitonin [10]. During sepsis, stimulation by endotoxins or pro-inflammatory cytokines such as IL-1β or TNF dramatically increases the serum levels of PCT up to 1000-fold [14]. In trauma patients, PCT has been proposed as a practical biomarker for predicting posttraumatic complications such as severe SIRS, sepsis, and MODS [14–17].
4.4 Immune Response After Multiple Injury
The biological immune response after trauma was considered in the past to be divided into an early innate phase and a late adaptive response. However, since multiple intensive interactions between both systems are known (e.g., via the complement cascade), a spatial- or time-dependent discrimination of both systems in regard to pathomechanistic changes after multiple injury is irrational. Both immune mechanisms contribute to effective recognition, activation, discrimination, regulation, and eradication of invading damage- and pathogen-associated signals [18]. Nevertheless, the innate immune response represents the “first line of defense”, consisting of a barrier against exogenous non-self antigens and microorganisms. This includes the integrity of epithelial and mucosal cells: skin, respiratory tract, alimentary tract, urogenital tract, brain, and conjunctiva. Exogenous pathogens that escape the first barrier are rapidly recognized and removed by the multiple components of innate immune cells such as neutrophils, monocytes/macrophages, natural killer cells, and dendritic cells [19]. The innate immune response is closely accompanied by the specifically acquired immune response after the trauma impact. The adaptive immune response is conducted by the interaction of antigen-presenting cells (APCs), dendritic cells, monocytes/macrophages, T-lymphocytes, and B-lymphocytes. The APCs capture invading pathogens and create peptide-MHC (major histocompatibility complex) protein complexes. T-lymphocytes recognize the peptide-MHC protein complex via T-cells expressing antigen-binding receptors (TCRs) and are thereby activated. In turn, activated T-lymphocytes release cytokines to activate and amplify further cells of the immune system. T-helper lymphocytes (CD4+ T cells) differentiate into two phenotypes according to the cytokine release, the Th1 and Th2 lymphocytes. Th1 cells promote the pro-inflammatory response through the release of IL-2, TNF, and interferon-γ (IFN-γ), while Th2 cells produce anti-inflammatory cytokines (IL-4, IL-5, and IL-10), which suppress macrophage activity [10]. Attention has been focused on the Th1/Th2-ratio. IL-12 secreted from monocytes/macrophages promotes the differentiation of Th1 cells by increasing the production of IFN-γ [20, 21]. Several studies have shown that a suppressed IL-12, IL-2, and IFN-γ, and elevated IL-4 are observed after major trauma, which correlated with a shift of the Th1/Th2 ratio towards the Th2-type pattern [22, 23]. This imbalance in Th1/Th2-type cytokine response (from pro- to anti-inflammation) is not only a compensatory response but also increases the risk of infection by immune suppression [20]. However, other reports do not support this view and question the clinical relevance of the Th1/Th2-shift after major tissue injury [24, 25].
4.5 Activation and Dysfunction of the Serine Protease Systems
4.5.1 The Coagulation System: Coagulopathy
Bleeding is a leading cause of death following polytrauma, and acute trauma-induced coagulopathy (ATIC) increases both the risk and severity of bleeding. Clinically, there are several routine laboratory parameters which are indicative of coagulopathy development (Table 4.2). Around one third of severe polytrauma patients are already coagulopathic upon arrival in the emergency room [27] and coagulopathy belongs together with acidosis and hypothermia to the “lethal triad” of polytrauma. Thus, an important diagnostic and therapeutic strategy has been developed proposed as the “STOP bleeding campaign” [29] that addresses three major aspects of coagulopathy: fast detection and stopping of relevant bleeding sources; estimation and resuscitation of the lost blood volume; and rapid monitoring for coagulopathic conditions.
The major mechanism of activation of the coagulation cascade following trauma is via the extrinsic coagulation system [30]. The extrinsic cascade mediates inflammation by tissue factor (TF). Exposure of the FVII to TF (e.g., from injured cells) results in the conversion of FVII to FVIIa. The FVIIa-TF-complexes activate FX to FXa, and FXa converts prothrombin to thrombin (FIIa). Thrombin activates FV, FVIII, and FXI, which results in enhanced thrombin formation. Thrombin also cleaves fibrinogen, and the fibrin clot is formed following polymerization and stabilization. In normal conditions, small amounts of TF are exposed to the circulating blood. However, under pathophysiological conditions, TF is upregulated on the surface of neutrophils, macrophages, and endothelial cells. Endotoxin, activated complement (C5a), and cytokines (IL-1β, TNF) induce TF expression [31]. TF is highly thrombogenic, and its upregulation often results in hypercoagulability, leading to an increased tendency of thrombosis [32, 33]. Another phylogenetically ancient activation pathway is the rather unknown FSAP (FVII activating protease) pathway that is activated by an autocatalytic mechanism promoted by factors released by necrotic or post-apoptotic cells such as nucleic acids, nucleosomes, and polyamines. FSAP can regulate coagulation and fibrinolysis by activating Factor VII and pro-urokinase, respectively. In polytrauma patients, an early and robust activation of FSAP is seen which in turn contributes to the activation of both, the coagulation and complement system [34].
In addition, coagulation mediators (FVIIa, FXa, and FIIa) elicit inflammation with expression of TNF, cytokines, adhesion molecules (MCP-1, ICAM-1, VCAM-1, selectins, etc.), and growth factors (e.g., VEGF) [33]. Inhibitors to prevent a hypercoagulable state include anti-thrombin III (ATIII), protein C, protein S and TF pathway inhibitor (TFPI). ATIII inhibits FIXa, FXa, and thrombin. TFPI suppresses the activity of TF/FVIIa/FXa complexes [35]. Protein C is activated by the thrombin-thrombomodulin complex on endothelial cells, and activated protein C, in combination with free protein S, cleaves and inactivates FV and FVIII [36]. Therapeutically intervening with the production and/or activity of inhibitors could help to improve outcome by mitigating complications such as ARDS.
For example, the CRASH2 trial has recently revealed that early application of tranexamic acid (a synthetic derivative of the amino acid lysine) that inhibits fibrinolysis by blocking the lysine binding sites on plasminogen significantly reduces the risk of death in bleeding trauma patients [37].
4.5.2 The Complement System: Complementopathy
Almost synchronically to the coagulation response, there is an activation of the complement cascade immediately after multiple trauma [38, 39]. The complement system consists of more than 30 proteins. In the resting state, complement proteins circulate as inactive forms in plasma. The activation of the complement system can occur through four pathways (alternative, classical, lectin, and coagulation paths). The classical pathway of complement is activated by antigen-antibody complexes (immune-globulin M or G) or CRP. The alternative pathway is activated by bacterial products such as lipopolysaccharides (LPS). The lectin pathway is initiated by lectin binding to mannose, glucose, or other sugars of microorganisms. Upon activation of the complement system, there is a generation of biologically active peptides. The cleavage of the central complement components C3 and C5 to the anaphylatoxins C3a and C5a, respectively, also induces the formation of opsonins and the membrane attack complexes (MAC, C5b-9) [40, 41]. Early after polytrauma, serum levels of the complement activation products C3a and C5a are significantly elevated and correlate with the severity of the injury (e.g., traumatic brain injury), septic complications, and mortality [27, 38]. The circulating soluble MAC is also enhanced within the first hours after polytrauma but almost not detectable between 4 and 48 h after polytrauma [38, 39]. Regulation of complement activation and protection against complement-mediated tissue destruction is provided by a selection of soluble- and membrane-bound complement regulatory proteins (CRegs). The expression profile of CRegs on leukocytes is specifically altered post polytrauma: CD46 (membrane co-factor protein) is significantly reduced in neutrophils, monocytes, and lymphocytes. In contrast, CD55 (decay accelerating factor) seems to be increased on neutrophils early after trauma. A delayed up-regulation of CD55 has been observed in monocytes from trauma patients. An initial enhancement of CD59 (MAC inhibitor) expression was measured in neutrophils and monocytes at the time of admission. Remarkably, C5a receptor (C5aR), CD59 and CD46 expression on neutrophils reversely correlated with injury severity [42]. The anaphylatoxins C3a and C5a mainly play pro-inflammatory roles, which include the recruitment and activation of phagocytic cells (polymorphonuclear cells, PMNs), monocytes/macrophages, the enhancement of the hepatic acute-phase reaction, stimulation of the release of vasoactive mediators (such as histamine), and promoting the adhesion of leukocytes to endothelial cells and their permeation through injured tissues. C5b forms a complex by the consecutive binding of proteins C6–C9, culminating in the formation of the MAC (C5b-9), which leads to the formation of pores in the cellular membrane causing lysis and death of the target cells [43]. Furthermore, the inflammatory response of complement activation leads to the production of free oxygen radicals and arachidonic acid metabolites and cytokines.
The complement cascade bridges innate and adaptive immunity for defense against microbial pathogens. However, excessive consumption of complement proteins may also cause tissue damage of the host after trauma. Within the first 24 h after multiple injuries, there is a massive reduction in complement hemolytic activity (CH50), which recovers only around 5 days after trauma, and can be used to discriminate between lethal and non-lethal outcome. This trauma-induced reduction of global complement function is referred to as trauma-induced “complementopathy” in analogy with “coagulopathy”, both of which significantly participate to the impairment of the innate immune response after polytrauma (Fig. 4.2).

Posttraumatic activation of the serine protease system; PK prekallikrein, TF tissue factor, FSAP Factor VII activating protease, MBL mannose-binding lectin, MASP-2 mannose-associated serine protease-2, MAC membrane attack complex
4.5.3 The Kallikrein-Kinin System
The kallikrein-kinin system involves a cascade of plasma proteases and is related to the complement and clotting cascade (intrinsic activation) [44]. This contact system consists of plasma proteins factor XII (Hageman factor; FXII), prekallikrein, high molecular weight kininogen (HMWK), and FXI. Contact with negatively charged surfaces such as foreign bodies or the membrane fragments of stimulated platelets activates FXII [44]. The active protein FXIIa converts prekallikrein into the proteolytic enzyme kallikrein, which in turn cleaves the plasma glycoprotein precursor HMWK to form bradykinin [45]. Bradykinin increases vascular permeability and causes dilation of blood vessels by its action on smooth muscle cells. In turn, as a positive feedback loop, kallikrein itself accelerates the conversion of FXII to FXIIa. Kallikrein can also activate fibrinolysis to counterbalance the clotting cascade activated by FXIIa. Furthermore, kallikrein also exhibits chemotactic activity, converting C3 and C5 into the chemoattractant products C3a and C5a, respectively [46].
4.6 Cytokines
4.6.1 Pro-inflammatory Cytokines
Pro-inflammatory cytokines play key local and systemic roles as intercellular messengers to initiate, amplify, and perpetuate the inflammatory response after trauma (Table 4.3). Cytokines are produced by many cell types in all organs. They have multiple targets and act in a pleiotropic manner. Early after trauma, production and release of pro-inflammatory cytokines such as IL-1β, TNF, IL-6, and IL-8 is initiated by monocytes and macrophages. IL-1β and TNF as well as IL-6 and IL-8 are released early after polytrauma [3, 47] and predominantly function as pro-inflammatory mediators to repair damaged tissue. The release of IL-1β and TNF is mainly stimulated by bacterial endotoxins or other microbial products, immune complexes, and a variety of inflammatory stimuli. Upon release, IL-1β and TNF usually return to baseline levels within 4 h. TNF increases the activity of neutrophils and monocytes by activating the underlying endothelium. TNF promotes the expression and release of adhesion molecules such as ICAM1 or E-selectin, and increases the permeability of endothelial cells, which facilitates neutrophil migration into the damaged tissue [48]. Some studies have proposed TNF as a valid serum marker for complications after trauma. However, the results are inconsistent and to date, no data is available indicating whether TNF correlates to the severity of trauma or trauma outcome [49–54]. Many different cell types produce IL-6: In addition to immune cells such as monocytes, macrophages, neutrophils, T cells, and B cells, it is also produced by endothelial cells, smooth muscle cells, and fibroblasts. IL-6 upregulates the hepatic acute-phase response, stimulating generation of C-reactive protein (CRP), procalcitonin, serum amyloid A, fibrinogen, α1-antitrypsin, and complement activation products (e.g., C5a), which then promote neutrophil activation. There is strong evidence that serum IL-6 level correlates with the severity of trauma, trauma pattern (especially in combination with chest trauma), and the risk of subsequent ARDS, MOF, and lethal outcome [47, 55]. Therefore, IL-6 may be considered as a clinically relevant and feasible parameter to estimate the severity of injury and prognosis after trauma [56, 57]. In addition, for patients requiring second or subsequent surgeries following trauma, IL-6 may prove to be an important biological marker in deciding the correct timing of surgery. In trauma patients with high initial levels of IL-6 (>500 pg/dL), it is recommended to delay secondary procedures for more than 4 days [58]. The chemokine IL-8 is secreted by monocytes/macrophages, neutrophils, and endothelial cells. After trauma, serum levels of IL-8 are elevated within 24 h. Its production following trauma stimulates leukocyte recruitment to the injured and inflammation site. Plasma levels of IL-8 correlate with the subsequent development of ARDS and MOF [57, 59–61].
4.6.2 Anti-inflammatory Cytokines
IL-10 is mainly synthesized by T lymphocytes and monocytes/macrophages. It is the pivotal role of IL-10 to inhibit the production of monocyte/macrophage-derived TNF, IL-6, IL-8, and free oxygen radicals [62]. IL-10 plasma levels are proportional to the severity of trauma and to posttraumatic complications [63–67] (Table 4.4). In addition to its pro-inflammatory role, IL-6 also has anti-inflammatory properties. As an immunoregulatory cytokine, IL-6 stimulates macrophages to release anti-inflammatory cytokines such as IL-1 receptor antagonists and soluble TNF receptors [8]. Moreover, IL-6 induces macrophages to release prostaglandin E2 (PGE2), the most powerful endogenous immune suppressant. PGE2 regulates the synthesis of TNF and IL-1β by macrophages and induces the release of IL-10 [68–70].
Overall, it has to be emphasized that almost all cytokines may not act strictly in either a pro- or anti-inflammatory manner, but rather may exhibit a “janus-faced behavior” depending on the underlying tissue, local environment, and trauma conditions. Furthermore, the categorized pro- and anti-inflammatory cytokines follow not a specific temporal pattern but are rather synchronically and rapidly generated and released [1, 3], mounting the overall inflammatory response. When the simultaneous cytokine response is excessive, prolonged, and dysregulated, this may lead to severe complications, such as organ dysfunctions [1] or persistent inflammation, immunosuppression, and catabolism syndrome (PICS) [5] (Fig. 4.3).

Posttraumatic pro- and anti-inflammatory immune response; PICS persistent inflammation, immune suppression, and catabolism syndrome
4.7 Reactive Oxygen Species (ROS)
Reactive oxygen species are released by leukocytes after exposure to pro- and anti-inflammatory cytokines, chemokines, complement factors, and bacterial products. There are several mechanisms of ROS production: mitochondrial oxidation, metabolism of arachidonic acid, activation of nicotin-adenine-dinucleotide-phosphate (NADPH) oxidase, and activation of xanthine oxidase. With ischemia and subsequent reperfusion, reintroduced molecular oxygen reacts with hypoxanthine and xanthine oxidase generated as the result of ATP consumption during the ischemia phase to generate superoxide anions (•O2 −). Superoxide anions are further reduced to hydrogen peroxide (H2O2) by superoxide dismutase (SOD). The initial ROS (superoxide anion and H2O2) are relatively low-energy oxygen radicals and are not considered to cause high levels of cytotoxicity [71]. The most detrimental agents of the ROS are hydroxyl radicals (•OH) which are generated from superoxide anions and H2O2 by the Haber-Weiss reaction: •O2 − + H2O2 → •OH + OH− + O2 or from H2O2 by the Fenton reaction in the presence of iron (LFeII(H2O2) → LFeIII + OH + OH−) (Fig. 4.4). ROS cause lipid peroxidation, cell membrane disintegration, and DNA damage to endothelial and parenchymal cells [72, 73]. Furthermore, ROS secreted by polymorphonuclear leukocytes (PMN) induce cytokines, chemokines [74], heat shock protein (HSP) [75], and adhesion molecules (p-selectin, ICAM-1) [76] leading to cell and tissue damage.

Production of reactive oxygen species (ROS)
4.8 Cells Implicated in Multiple Trauma
4.8.1 Neutrophils
Early after severe tissue trauma, neutrophils migrate along the chemoattractant gradient of complement activation products, interleukins, and ROS to the site of tissue damage and to remote organ tissue. Neutrophil mobilization is important for wound healing and protection against invading microorganisms, but their immigration to remote organ tissue contributes to SIRS [77]. Neutrophil migration is composed of four steps: The first step, generation of leukocyte selectins (e.g., L-selectins) and E- and P-selectins on the endothelium is induced by anaphylatoxins (e.g., C5a), cytokines (e.g., IL-6), and toxins [78]. These adhesion molecules are responsible for the rolling of neutrophils. The second step involves expression of integrins on neutrophils such as CD11 and CD18, and intercellular adhesion molecules (ICAM-1) and vascular cell adhesion molecules (VCAM-1) on the surface of endothelial cells, all of which are strongly induced by C5a [79–81]. The interaction of these upregulated molecules activate neutrophils to reinforce the contact between neutrophils and endothelial cells (sticking). In the next step, migration and accumulation into tissues occur, mediated by chemokines and complement anaphylatoxins. To migrate through cellular barriers, neutrophils undergo significant deformational changes to permeate through small cellular gaps with the help of locally released matrix metalloproteinases. In the final step, activation of neutrophils occurs to protect against dangerous molecules, microorganisms, and cells. Neutrophils utilize a large arsenal for forming the “first line of defense” after trauma: chemotaxis, phagocytosis, oxidative burst reaction with release of ROS and myeloperoxidase (MPO), generation of NO, leukotriens, platelet-activating factor (PAF), tissue factor (TF), proteases, and multiple pro-inflammatory cytokines. However, the active substances released from neutrophils may not only harm the invading microorganisms or injured cells but also healthy host cells, especially since neutrophils become “long-lived” after trauma by significant inhibition of neutrophil apoptosis. Thus, neutrophils after trauma function as “friend and foe”.
4.8.2 Monocytes/Macrophages
Monocytes/macrophages and neutrophils play a central role for the innate host defense, tissue repair, and remodelling, and for the intermediaries to the antigen-specific adaptive immune response. Monocytes are circulating precursors of macrophages. Monocytes migrate into the different tissues (liver, spleen, lungs, etc.) even in absence of local inflammation and become tissue macrophages. When monocytes/macrophages are activated by various phagocytotic events in response to trauma, they regulate the activation of T and B lymphocytes, which induce antigen presentation by the major histocompatibility complex II (MHC II). Monocytes/macrophages also release chemokines, cytokines (IL-6, TNF, IL-10, IL-12, TGF-β), and various growth factors (fibroblast growth factor [FGF], epidermal growth factor [EGF], and platelet-derived growth factors [PDGF]) that initiate the formation of new extracellular matrix and promote angiogenesis and generation of new tissue at the site of injury. The functional phenotype shifts from a pronounced pro-inflammatory M1 type to a more anti-inflammatory and regenerative M2-type macrophage. The monocyte/macrophage cellular response after minor trauma embodies several beneficial effects for the host. However, major trauma induces massive monocyte/macrophage activation. In this state, the effects of the monocyte/macrophage response become systemic and may also induce detrimental effects. Systemically, the macrophage-modulated immune response influences microcirculation, metabolism, and triggering and progression of remote organ injury. Deactivation of monocytes and decreased expression of MHC II on their surface are observed after major trauma correlating with the severity of injury [82].
4.8.3 Natural Killer Cells
Natural killer (NK) cells are antigen-non-specific lymphocytes that recognize pathogen-associated molecular patterns (PAMPs) of invading microorganisms [83] as well as damaged, transformed, or virus-infected host cells [84]. Since they are not dependent on pre-sensitization [85] to mediate their cytotoxic effects and to release excessive amounts of pro- and anti-inflammatory cytokines within minutes of stimulation, NK cells are regarded as part of the “first line of defense” [86]. Their ability to release immune-modulatory cytokines may provide important regulatory functions during immune response, especially following severe injury. However, studies addressing the role of human NK cells after severe tissue trauma are rare and contradictory. Some studies revealed an increase of NK cells in the early stage after severe trauma [77], whereas NK cell function is greatly depressed by traumatic injury. However, there was no correlation between the NK cell count or activity and injury severity [85, 87]. Concerning the effect of plasma samples from trauma patients on the cytotoxic activity of healthy NK cells in vitro, it has been shown that incubation times of more than 40 h lead to suppressed NK cell function, suggesting that posttraumatic immune suppression is associated with suppression of NK cell activity [85]. Vice versa, murine experiments have collectively shown that NK cells as a key source of interferon γ exert harmful pro-inflammatory effects in the posttraumatic immune response and during the pathogenesis of sepsis [88, 89]. In support, early depletion of NK cells results in reduction of liver IL-6 expression and a 50 % improved survival rate in a murine polytrauma model. Lymphocyte apoptosis in spleen as well as neutrophil infiltration into lungs and liver is also attenuated [88]. Furthermore, in various mouse models of sepsis, depletion of NK cells leads to improved survival [89, 90] suggesting that early posttraumatic activation of NK cells promotes amplification of the inflammatory response, and the subsequent loss of cellular functions might contribute to immune suppression manifested in later stages after trauma [87].
4.9 Mechanisms of the Development of Organ Dysfunction
4.9.1 Severity of Initial Injury (First Hit)
The initial trauma insult activates an inflammatory cascade that stimulates the host immune system. Massive initial trauma impact (first hit) causes severe SIRS. In this situation, the overwhelming production and release of pro- and anti-inflammatory mediators result in rapid MODS and early death.
An initial trauma insult of lower severity induces a moderate state of SIRS/CARS. In this instance, inflammatory and immune cells undergo some “priming”. However, some patients develop posttraumatic complications, such as sepsis, AKI, ARDS, and MODS. The development of these complications is regulated by various exogenous and endogenous factors. Among these factors, it is important to understand the relationship between the biological changes and the anatomical region of initial injury. The central nervous system is a rich source of inflammatory mediators. Traumatic brain injuries (TBI) with the disruption of the blood-brain barrier (BBB) allow immune cells to migrate into the subarachnoid space, leading to an accumulation of leukocytes from the periphery [10, 91–93]. Trauma to the chest area, particularly lung contusions, leads to an early increase in plasma mediators, which is associated with systemic inflammatory and anti-inflammatory reactions, such as pneumonia, ARDS, and MODS [94–96]. Patients with severe soft tissue injuries to the extremities with resulting hemorrhagic shock or severe muscle crush syndrome are at risk of developing more serious remote organ injury (e.g., AKI). Ischemia/reperfusion injury (I/R) leads to the production of large quantities of ROS. Femoral fractures with soft tissue injuries usually result in alteration of hemodynamic parameters such as increased cardiac output, tachycardia, decreased systemic vascular resistance, and decreased hepatic blood flow [97]. Long bone fractures and unstable pelvic fractures are characterized by high blood loss and are associated with severe soft tissue injury, which initiate both a local and systemic inflammatory response [65, 98–102]. These bodies of evidence suggest that the initial trauma itself predisposes trauma patients to posttraumatic complications.
4.9.2 Two-Hit Theory
Traumatized patients who survive the initial injury (“first hit”) may still be at risk of death from sepsis and multiple organ failure. Secondary insults following the initial injury amplify the systemic inflammatory response and upset the balance of pro- and anti-inflammatory mediators, pro- and anti-coagulatory factors, pro- and anti-apoptotic events, and pro- and anti-regenerative processes. Secondary insults (“second hits”) are compounded by endogenous and exogenous factors. Endogenous secondary insults include respiratory distress, cardiovascular instability, ischemia and reperfusion injury, and infection. Exogenous secondary insults include surgical and anesthesiological interventions [103–105], blood transfusions, and – not to forget – missed injuries.
Clinical studies have revealed that orthopedic surgical intervention can also cause major changes in the inflammatory response, and these changes are in proportion to the magnitude of surgery. For instance, femoral nailing induces an increase in systemic plasma levels of IL-6 and IL-10. In these patients, human leukocyte antigen-DR expression on monocytes is reduced as well [106, 107]. Furthermore, reamed femoral nailing appears to be associated with greater impairment of immune reactivity than un-reamed nailing [107].
Blood transfusions are a paramount therapy in the management of trauma/hemorrhagic shock patients. However, various studies have demonstrated that blood transfusions are associated with infection, SIRS, ARDS, and MODS after trauma [108–113], also representing a “second hit” for the multiply injured patient.
4.9.3 Ischemia/Reperfusion Injury
Ischemia/reperfusion (I/R) injury is a common and important event in clinical situations such as trauma, hemorrhagic shock, cardiac arrest (hypoxemia, hypotension of systemic tissue), contusions, lacerations, vascular injuries, and compartment syndrome (increased pressure in a preformed anatomical compartment with resulting hypoperfusion and hypoxemia of local tissue). Inadequate microvascular flow results in the activation of leukocytes and converts local endothelial cells into a pro-inflammatory and pro-thrombotic phenotype. I/R injury consists of two specific stages. During the first stage of ischemia and hypoxemia, oxygen and nutrients are deprived from tissues temporarily by the disruption of blood supply. During the ischemic phase, the lack of oxygen leads to decreased production as well as consumption of adenosine triphosphate (ATP). As consumption of ATP continues, it is degraded into adenosine diphosphate (ADP) and adenosine monophosphate (AMP), which is further degraded to inosine and hypoxanthine [114]. ATP depletion leads to an alteration in intercellular calcium and sodium concentration. It also results in the activation of cytotoxic enzymes such as proteases or phospholipases, all cumulating to reversible or irreversible cellular damage. The second stage of reperfusion is the revascularization or reestablished supply of oxygen to the ischemic tissue. The hallmark of the reperfusion phase is the generation of by-products of neutrophil activation, which induces secondary tissue damage and organ dysfunction. On reperfusion with the reintroduction of molecular oxygen into the ischemic tissue, oxygen reacts with leukocytes and endothelial cells promoting the generation of reactive oxygen species and platelet-activation factor. The interactions of neutrophils and endothelial cells have been shown to contribute to massive interstitial edema caused by microvascular capillary leakage after reperfusion injury.
4.9.4 Barrier Breakdown
The ischemia and reperfusion injury with ATP depletion is a major cause for breakdown of physiological organ-blood barriers, such as blood-brain, blood-gut, and blood-alveolus barrier. Broken barriers characterized by diffuse microvascular leakage and tissue edema are thought to be main drivers of bacterial translocation (BT) and sepsis [115]. Bacterial translocation is defined as the phenomenon of both viable and nonviable bacteria as well as their products (bacterial cell wall components, LPS, and peptidoglycan) crossing the intestinal barrier to external sites such as the mesenteric lymph nodes, liver, and spleen. BT occurs as a result of a loss of integrity of the gut barrier function after trauma, hemorrhagic shock, and burns [116], and may be associated with posttraumatic complications [117, 118]. Although most data on BT and its complications have shown consistent results in animal models of hemorrhagic shock, trauma, and severe burns, its importance in humans is questionable, with variable results in clinical studies. In addition, it is still debatable whether BT is an important pathophysiologic event or simply an epiphenomenon of severe disease [119].
4. Conclusion
Following trauma, acute inflammatory reactions may be triggered by infections (bacterial, viral, fungal, parasitic) and microbial toxins, or by any of several molecules released from necrotic tissue (HMGB1, hyaluronic acid, etc.). Pattern recognition receptors (PRRs), including toll-like receptors, can detect these stimuli and trigger a signaling pathway that leads to the production of various mediators. In the acute phase of trauma, vasodilatation is induced by vasodilatatory mediators (NO, prostaglandins), quickly followed by increased permeability of the microvasculature. Vasodilatation and extravasation of plasma result in hemoconcentration, facilitating the peripheral migration of neutrophils. Neutrophil migration from the blood stream into interstitial tissue is divided into several steps, which are mediated by endothelial cell adhesion molecules, cytokines produced by monocytes/macrophages and various other cells, chemokines, the complement system, and arachidonic acid. Migrated neutrophils produce several mediators such as neutral protease, reactive oxygen species (ROS), lipids (leukotriene, PAF), and tissue factor (TF). These mediators act as secondary tissue damage mediators and pro-coagulatory factors depending on the degree of initial injury as well as additional insults. During inflammation, the plasmaic cascade, consisting of the complement cascade, the kallikrein-kinin system, and the coagulation cascade, is activated by toxins and inflammatory mediators. Activation of the complement system induces generation and depletion of complement activation products, causing an increase in vascular permeability, chemotaxis, opsonization, activation of the coagulation cascade, and trauma-induced complementopathy. Excessive activation of the coagulation system results in a hypercoagulable state, leading to an acute trauma-induced coagulopathy (ATIC). Activation of the kallikrein-kinin system results in kinins with vasoactive properties. In addition to its role in stimulating inflammation, the immune system (innate and adaptive) is a main driver for the barrier breakdown, clinically evident as diffuse microvascular leakage syndrome and organ failure. The exact knowledge of the pathophysiological changes after polytrauma is a prerequisite for effective, targeted, and patient-tailored future therapies to support the immune and organ functions after severe tissue trauma.
References
Xiao W, Mindrinos MN, Seok J, et al. A genomic storm in critically injured humans. J Exp Med. 2011;208:2581–90.
Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101:1644–55.
Gebhard F, Bruckner UB, Strecker W, et al. Untersuchungen zur systemischen posttraumatischen Inflammation in der Frühphase nach Trauma, Hefte zu der Unfallchirurg, vol. 276. Berlin/Heidelberg/New York: Springer; 2000. p. 276.
Adib-Conquy M, Cavaillon JM. Compensatory anti-inflammatory response syndrome. Thromb Haemost. 2009;101:36–47.
Gentile LF, Cuenca AG, Efron PA, et al. Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care. J Trauma Acute Care Surg. 2012;72:1491–501.
Matzinger P. The danger model: a renewed sense of self. Science. 2002;296:301–5.
Gebhard F, Huber-Lang M. Polytrauma–pathophysiology and management principles. Langenbecks Arch Surg. 2008;393:825–31.
Lin E, Calvano SE, Lowry SF. Inflammatory cytokines and cell response in surgery. Surgery. 2000;127:117–26.
Gruys E, Toussaint MJ, Niewold TA, et al. Acute phase reaction and acute phase proteins. J Zhejiang Univ Sci B. 2005;6:1045–56.
Keel M, Trentz O. Pathophysiology of polytrauma. Injury. 2005;36:691–709.
el Hassan BS, Peak JD, Whicher JT, et al. Acute phase protein levels as an index of severity of physical injury. Int J Oral Maxillofac Surg. 1990;19:346–9.
Gosling P, Dickson GR. Serum c-reactive protein in patients with serious trauma. Injury. 1992;23:483–6.
Taylor KE, van den Berg CW. Structural and functional comparison of native pentameric, denatured monomeric and biotinylated C-reactive protein. Immunology. 2007;120:404–11.
Castelli GP, Pognani C, Cita M, et al. Procalcitonin as a prognostic and diagnostic tool for septic complications after major trauma. Crit Care Med. 2009;37:1845–9.
Mimoz O, Benoist JF, Edouard AR, et al. Procalcitonin and C-reactive protein during the early posttraumatic systemic inflammatory response syndrome. Intensive Care Med. 1998;24:185–8.
Uzzan B, Cohen R, Nicolas P, et al. Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: a systematic review and meta-analysis. Crit Care Med. 2006;34:1996–2003.
Wanner GA, Keel M, Steckholzer U, et al. Relationship between procalcitonin plasma levels and severity of injury, sepsis, organ failure, and mortality in injured patients. Crit Care Med. 2000;28:950–7.
Lenz A, Franklin GA, Cheadle WG. Systemic inflammation after trauma. Injury. 2007;38:1336–45.
Pillay J, Hietbrink F, Koenderman L, et al. The systemic inflammatory response induced by trauma is reflected by multiple phenotypes of blood neutrophils. Injury. 2007;38:1365–72.
Trinchieri G. Interleukin-12 and the regulation of innate resistance and adaptive immunity. Nat Rev Immunol. 2003;3:133–46.
Watford WT, Moriguchi M, Morinobu A, et al. The biology of IL-12: coordinating innate and adaptive immune responses. Cytokine Growth Factor Rev. 2003;14:361–8.
Decker D, Schondorf M, Bidlingmaier F, et al. Surgical stress induces a shift in the type-1/type-2 T-helper cell balance, suggesting down-regulation of cell-mediated and up-regulation of antibody-mediated immunity commensurate to the trauma. Surgery. 1996;119:316–25.
Spolarics Z, Siddiqi M, Siegel JH, et al. Depressed interleukin-12-producing activity by monocytes correlates with adverse clinical course and a shift toward Th2-type lymphocyte pattern in severely injured male trauma patients. Crit Care Med. 2003;31:1722–9.
Heizmann O, Koeller M, Muhr G, et al. Th1- and Th2-type cytokines in plasma after major trauma. J Trauma. 2008;65:1374–8.
Wick M, Kollig E, Muhr G, et al. The potential pattern of circulating lymphocytes TH1/TH2 is not altered after multiple injuries. Arch Surg. 2000;135:1309–14.
Brohi K, Singh J, Heron M, et al. Acute traumatic coagulopathy. J Trauma. 2003;54:1127–30.
Maegele M, Lefering R, Yucel N, et al. Early coagulopathy in multiple injury: an analysis from the German Trauma Registry on 8724 patients. Injury. 2007;38:298–304.
Greuters S, van den Berg A, Franschman G, et al. Acute and delayed mild coagulopathy are related to outcome in patients with isolated traumatic brain injury. Crit Care. 2011;15:R2.
Rossaint R, Bouillon B, Cerny V, et al. The STOP the bleeding campaign. Crit Care. 2013;17:136.
Chu AJ. Blood coagulation as an intrinsic pathway for proinflammation: a mini review. Inflamm Allergy Drug Targets. 2010;9:32–44.
Ritis K, Doumas M, Mastellos D, et al. A novel C5a receptor-tissue factor cross-talk in neutrophils links innate immunity to coagulation pathways. J Immunol. 2006;177:4794–802.
Abraham E. Coagulation abnormalities in acute lung injury and sepsis. Am J Respir Cell Mol Biol. 2000;22:401–4.
Chu AJ. Tissue factor mediates inflammation. Arch Biochem Biophys. 2005;440:123–32.
Kanse SM, Gallenmueller A, Zeerleder S, et al. Factor VII-activating protease is activated in multiple trauma patients and generates anaphylatoxin C5a. J Immunol. 2012;188:2858–65.
Riddel Jr JP, Aouizerat BE, Miaskowski C, et al. Theories of blood coagulation. J Pediatr Oncol Nurs. 2007;24:123–31.
Rigby AC, Grant MA. Protein S: a conduit between anticoagulation and inflammation. Crit Care Med. 2004;32:S336–41.
Shakur H, Roberts I, Bautista R, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376:23–32.
Burk AM, Martin M, Flierl MA, et al. Early complementopathy after multiple injuries in humans. Shock. 2012;37:348–54.
Hecke F, Schmidt U, Kola A, et al. Circulating complement proteins in multiple trauma patients–correlation with injury severity, development of sepsis, and outcome. Crit Care Med. 1997;25:2015–24.
Fosse E, Pillgram-Larsen J, Svennevig JL, et al. Complement activation in injured patients occurs immediately and is dependent on the severity of the trauma. Injury. 1998;29:509–14.
Mollnes TE, Fosse E. The complement system in trauma-related and ischemic tissue damage: a brief review. Shock. 1994;2:301–10.
Amara U, Kalbitz M, Perl M, et al. Early expression changes of complement regulatory proteins and C5A receptor (CD88) on leukocytes after multiple injury in humans. Shock. 2010;33:568–75.
Mastellos D, Lambris JD. Complement: more than a ‘guard’ against invading pathogens? Trends Immunol. 2002;23:485–91.
Sugimoto K, Hirata M, Majima M, et al. Evidence for a role of kallikrein-P6nin system in patients with shock after blunt trauma. Am J Physiol. 1998;274:R1556–60.
Joseph K, Kaplan AP. Formation of bradykinin: a major contributor to the innate inflammatory response. Adv Immunol. 2005;86:159–208.
Amara U, Flierl MA, Rittirsch D, et al. Molecular intercommunication between the complement and coagulation systems. J Immunol. 2010;185:5628–36.
Gebhard F, Pfetsch H, Steinbach G, et al. Is interleukin 6 an early marker of injury severity following major trauma in humans? Arch Surg. 2000;135:291–5.
Dinarello CA. Proinflammatory cytokines. Chest. 2000;118:503–8.
Ayala A, Perrin MM, Meldrum DR, et al. Hemorrhage induces an increase in serum TNF which is not associated with elevated levels of endotoxin. Cytokine. 1990;2:170–4.
Rabinovici R, John R, Esser KM, et al. Serum tumor necrosis factor-alpha profile in trauma patients. J Trauma. 1993;35:698–702.
Rhee P, Waxman K, Clark L, et al. Tumor necrosis factor and monocytes are released during hemorrhagic shock. Resuscitation. 1993;25:249–55.
Roumen RM, Hendriks T, van der Ven-Jongekrijg J, et al. Cytokine patterns in patients after major vascular surgery, hemorrhagic shock, and severe blunt trauma. Relation with subsequent adult respiratory distress syndrome and multiple organ failure. Ann Surg. 1993;218:769–76.
Stylianos S, Wakabayashi G, Gelfand JA, et al. Experimental hemorrhage and blunt trauma do not increase circulating tumor necrosis factor. J Trauma. 1991;31:1063–7.
Zingarelli B, Squadrito F, Altavilla D, et al. Role of tumor necrosis factor-alpha in acute hypovolemic hemorrhagic shock in rats. Am J Physiol. 1994;266:H1512–5.
Biffl WL, Moore EE, Moore FA, et al. Interleukin-6 in the injured patient. Marker of injury or mediator of inflammation? Ann Surg. 1996;224:647–64.
Pape HC, Tsukamoto T, Kobbe P, et al. Assessment of the clinical course with inflammatory parameters. Injury. 2007;38:1358–64.
Partrick DA, Moore FA, Moore EE, et al. Jack A. Barney Resident Research Award winner. The inflammatory profile of interleukin-6, interleukin-8, and soluble intercellular adhesion molecule-1 in postinjury multiple organ failure. Am J Surg. 1996;172:425–9.
Pape HC, van Griensven M, Rice J, et al. Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: determination of the clinical relevance of biochemical markers. J Trauma. 2001;50:989–1000.
DeLong Jr WG, Born CT. Cytokines in patients with polytrauma. Clin Orthop Relat Res. 2004;(422):57–65.
Donnelly SC, Strieter RM, Kunkel SL, et al. Interleukin-8 and development of adult respiratory distress syndrome in at-risk patient groups. Lancet. 1993;341:643–7.
Pallister I, Dent C, Topley N. Increased neutrophil migratory activity after major trauma: a factor in the etiology of acute respiratory distress syndrome? Crit Care Med. 2002;30:1717–21.
Oswald IP, Wynn TA, Sher A, et al. Interleukin 10 inhibits macrophage microbicidal activity by blocking the endogenous production of tumor necrosis factor alpha required as a costimulatory factor for interferon gamma-induced activation. Proc Natl Acad Sci U S A. 1992;89:8676–80.
Armstrong L, Millar AB. Relative production of tumour necrosis factor alpha and interleukin 10 in adult respiratory distress syndrome. Thorax. 1997;52:442–6.
Donnelly SC, Strieter RM, Reid PT, et al. The association between mortality rates and decreased concentrations of interleukin-10 and interleukin-1 receptor antagonist in the lung fluids of patients with the adult respiratory distress syndrome. Ann Intern Med. 1996;125:191–6.
Giannoudis PV, Smith RM, Perry SL, et al. Immediate IL-10 expression following major orthopaedic trauma: relationship to anti-inflammatory response and subsequent development of sepsis. Intensive Care Med. 2000;26:1076–81.
Neidhardt R, Keel M, Steckholzer U, et al. Relationship of interleukin-10 plasma levels to severity of injury and clinical outcome in injured patients. J Trauma. 1997;42:863–70.
Pajkrt D, Camoglio L, Tiel-van Buul MC, et al. Attenuation of proinflammatory response by recombinant human IL-10 in human endotoxemia: effect of timing of recombinant human IL-10 administration. J Immunol. 1997;158:3971–7.
Opal SM, DePalo VA. Anti-inflammatory cytokines. Chest. 2000;117:1162–72.
Phipps RP, Stein SH, Roper RL. A new view of prostaglandin E regulation of the immune response. Immunol Today. 1991;12:349–52.
Tilg H, Trehu E, Atkins MB, et al. Interleukin-6 (IL-6) as an anti-inflammatory cytokine: induction of circulating IL-1 receptor antagonist and soluble tumor necrosis factor receptor p55. Blood. 1994;83:113–8.
Sasaki M, Joh T. Oxidative stress and ischemia-reperfusion injury in gastrointestinal tract and antioxidant, protective agents. J Clin Biochem Nutr. 2007;40:1–12.
Cristofori L, Tavazzi B, Gambin R, et al. Early onset of lipid peroxidation after human traumatic brain injury: a fatal limitation for the free radical scavenger pharmacological therapy? J Investig Med. 2001;49:450–8.
Kong SE, Blennerhassett LR, Heel KA, et al. Ischaemia-reperfusion injury to the intestine. Aust N Z J Surg. 1998;68:554–61.
Remick DG, Villarete L. Regulation of cytokine gene expression by reactive oxygen and reactive nitrogen intermediates. J Leukoc Biol. 1996;59:471–5.
Schreck R, Rieber P, Baeuerle PA. Reactive oxygen intermediates as apparently widely used messengers in the activation of the NF-kappa B transcription factor and HIV-1. EMBO J. 1991;10:2247–58.
Gasic AC, McGuire G, Krater S, et al. Hydrogen peroxide pretreatment of perfused canine vessels induces ICAM-1 and CD18-dependent neutrophil adherence. Circulation. 1991;84:2154–66.
Hua R, Chen FX, Zhang YM, et al. Association of traumatic severity with change in lymphocyte subsets in the early stage after trauma. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2013;25:489–92.
Zallen G, Moore EE, Johnson JL, et al. Circulating postinjury neutrophils are primed for the release of proinflammatory cytokines. J Trauma. 1999;46:42–8.
Law MM, Cryer HG, Abraham E. Elevated levels of soluble ICAM-1 correlate with the development of multiple organ failure in severely injured trauma patients. J Trauma. 1994;37:100–9.
Seekamp A, Jochum M, Ziegler M, et al. Cytokines and adhesion molecules in elective and accidental trauma-related ischemia/reperfusion. J Trauma. 1998;44:874–82.
Simon SI, Green CE. Molecular mechanics and dynamics of leukocyte recruitment during inflammation. Annu Rev Biomed Eng. 2005;7:151–85.
Ayala A, Ertel W, Chaudry IH. Trauma-induced suppression of antigen presentation and expression of major histocompatibility class II antigen complex in leukocytes. Shock. 1996;5:79–90.
Chalifour A, Jeannin P, Gauchat JF, et al. Direct bacterial protein PAMP recognition by human NK cells involves TLRs and triggers alpha-defensin production. Blood. 2004;104:1778–83.
Lanier LL. NK cell recognition. Annu Rev Immunol. 2005;23:225–74.
Morrison G, Cunningham-Rundles S, Clowes Jr GH, et al. Augmentation of NK cell activity by a circulating peptide isolated from the plasma of trauma patients. Ann Surg. 1986;203:21–4.
Lodoen MB, Lanier LL. Natural killer cells as an initial defense against pathogens. Curr Opin Immunol. 2006;18:391–8.
Joshi P, Hauser CJ, Jones Q, et al. Mechanism of suppression of natural killer cell activity in trauma patients. Res Commun Mol Pathol Pharmacol. 1998;101:241–8.
Barkhausen T, Frerker C, Putz C, et al. Depletion of NK cells in a murine polytrauma model is associated with improved outcome and a modulation of the inflammatory response. Shock. 2008;30:401–10.
Chiche L, Forel JM, Thomas G, et al. The role of natural killer cells in sepsis. J Biomed Biotechnol. 2011;2011:986491.
Badgwell B, Parihar R, Magro C, et al. Natural killer cells contribute to the lethality of a murine model of Escherichia coli infection. Surgery. 2002;132:205–12.
Ghirnikar RS, Lee YL, Eng LF. Inflammation in traumatic brain injury: role of cytokines and chemokines. Neurochem Res. 1998;23:329–40.
Morganti-Kossmann MC, Satgunaseelan L, Bye N, et al. Modulation of immune response by head injury. Injury. 2007;38:1392–400.
Schmidt OI, Heyde CE, Ertel W, et al. Closed head injury–an inflammatory disease? Brain Res Brain Res Rev. 2005;48:388–99.
Knoferl MW, Liener UC, Perl M, et al. Blunt chest trauma induces delayed splenic immunosuppression. Shock. 2004;22:51–6.
Perl M, Gebhard F, Bruckner UB, et al. Pulmonary contusion causes impairment of macrophage and lymphocyte immune functions and increases mortality associated with a subsequent septic challenge. Crit Care Med. 2005;33:1351–8.
Strecker W, Gebhard F, Perl M, et al. Biochemical characterization of individual injury pattern and injury severity. Injury. 2003;34:879–87.
Schirmer WJ, Schirmer JM, Townsend MC, et al. Femur fracture with associated soft-tissue injury produces hepatic ischemia. Possible cause of hepatic dysfunction. Arch Surg. 1988;123:412–5.
Giannoudis PV, Pape HC, Cohen AP, et al. Review: systemic effects of femoral nailing: from Kuntscher to the immune reactivity era. Clin Orthop Relat Res. 2002;(404):378–86.
Hauser CJ, Joshi P, Zhou X, et al. Production of interleukin-10 in human fracture soft-tissue hematomas. Shock. 1996;6:3–6.
Hauser CJ, Zhou X, Joshi P, et al. The immune microenvironment of human fracture/soft-tissue hematomas and its relationship to systemic immunity. J Trauma. 1997;42:895–903.
Pape HC, Schmidt RE, Rice J, et al. Biochemical changes after trauma and skeletal surgery of the lower extremity: quantification of the operative burden. Crit Care Med. 2000;28:3441–8.
Perl M, Gebhard F, Knoferl MW, et al. The pattern of preformed cytokines in tissues frequently affected by blunt trauma. Shock. 2003;19:299–304.
Angele MK, Chaudry IH. Surgical trauma and immunosuppression: pathophysiology and potential immunomodulatory approaches. Langenbecks Arch Surg. 2005;390:333–41.
Flohe S, Flohe SB, Schade FU, et al. Immune response of severely injured patients–influence of surgical intervention and therapeutic impact. Langenbecks Arch Surg. 2007;392:639–48.
Ni CN, Redmond HP. Cell response to surgery. Arch Surg. 2006;141:1132–40.
Giannoudis PV, Smith RM, Bellamy MC, et al. Stimulation of the inflammatory system by reamed and unreamed nailing of femoral fractures. An analysis of the second hit. J Bone Joint Surg Br. 1999;81:356–61.
Smith RM, Giannoudis PV, Bellamy MC, et al. Interleukin-10 release and monocyte human leukocyte antigen-DR expression during femoral nailing. Clin Orthop Relat Res. 2000;(373):233–40.
Malone DL, Dunne J, Tracy JK, et al. Blood transfusion, independent of shock severity, is associated with worse outcome in trauma. J Trauma. 2003;54:898–905.
Moore EE, Johnson JL, Cheng AM, et al. Insights from studies of blood substitutes in trauma. Shock. 2005;24:197–205.
Moore FA, Moore EE, Sauaia A. Blood transfusion. An independent risk factor for postinjury multiple organ failure. Arch Surg. 1997;132:620–4.
Sauaia A, Moore FA, Moore EE, et al. Early predictors of postinjury multiple organ failure. Arch Surg. 1994;129:39–45.
Shander A. Emerging risks and outcomes of blood transfusion in surgery. Semin Hematol. 2004;41:117–24.
Silliman CC, Moore EE, Johnson JL, et al. Transfusion of the injured patient: proceed with caution. Shock. 2004;21:291–9.
Nakao A, Kaczorowski DJ, Sugimoto R, et al. Application of heme oxygenase-1, carbon monoxide and biliverdin for the prevention of intestinal ischemia/reperfusion injury. J Clin Biochem Nutr. 2008;42:78–88.
Goldenberg NM, Steinberg BE, Slutsky AS, et al. Broken barriers: a new take on sepsis pathogenesis. Sci Transl Med. 2011;3:88ps25.
Macintire DK, Bellhorn TL. Bacterial translocation: clinical implications and prevention. Vet Clin North Am Small Anim Pract. 2002;32:1165–78.
Fukushima R, Alexander JW, Gianotti L, et al. Bacterial translocation-related mortality may be associated with neutrophil-mediated organ damage. Shock. 1995;3:323–8.
Nieuwenhuijzen GA, Goris RJ. The gut: the ‘motor’ of multiple organ dysfunction syndrome? Curr Opin Clin Nutr Metab Care. 1999;2:399–404.
Lichtman SM. Bacterial [correction of baterial] translocation in humans. J Pediatr Gastroenterol Nutr. 2001;33:1–10.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Huber-Lang, M., Gebhard, F. (2016). Inflammatory Changes and Coagulopathy in Multiply Injured Patients. In: Pape, HC., Sanders, R., Borrelli, Jr., J. (eds) The Poly-Traumatized Patient with Fractures. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-47212-5_4
Download citation
DOI: https://doi.org/10.1007/978-3-662-47212-5_4
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-47211-8
Online ISBN: 978-3-662-47212-5
eBook Packages: MedicineMedicine (R0)