
Abstract
All of these conditions can be associated with acute pancreatitis, except ?
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others



Keywords
- Acute Pancreatitis
- Systemic Inflammatory Response Syndrome
- Severe Acute Pancreatitis
- Common Bile Duct Stone
- Pancreatic Necrosis
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Self-Assessment Questions
-
1.
All of these conditions can be associated with acute pancreatitis, except ?
-
a.
Smoking
-
b.
Hyperkalemia
-
c.
Genetic mutations
-
d.
Tetracycline
-
e.
Methrotrexate
-
a.
-
2.
Acute pancreatitis could be the first manifestation of a pancreatic adenocarcinoma.
-
a.
True
-
b.
False
-
a.
-
3.
The Cullen’s sign in acute pancreatitis is suggestive of?
-
a.
Necrotizing pancreatitis
-
b.
Retroperitoneal bleeding
-
c.
Central gland necrosis
-
d.
Infected pancreatic necrosis
-
e.
Splenic vein thrombosis
-
a.
-
4.
All of the following statements are related to the systemic inflammatory response syndrome (SIRS), except ?
-
a.
This syndrome usually occurs toward the end of the second week of presentation
-
b.
Cytokine cascades are activated by pancreatic inflammation
-
c.
Pulse >90 beats/min
-
d.
PCO2 <32 mmHg
-
e.
SIRS predisposes to multiple organ dysfunction and/or pancreatic necrosis
-
a.
-
5.
CECT to distinguish interstitial pancreatitis from necrotizing pancreatitis should be performed “at least” 72 hours after admission.
-
a.
True
-
b.
False
-
a.
-
6.
Which statement regarding peripancreatic fluid collections in acute pancreatitis is false?
-
a.
They occur within the first 4 weeks after onset of interstitial edematous pancreatitis.
-
b.
They do not have a definable wall.
-
c.
Most acute fluid collections are sterile.
-
d.
The majority require intervention.
-
e.
They may be found in the small bowel mesentery.
-
a.
-
7.
Total parenteral nutrition (TPN) feeding is preferable to enteral feeding.
-
a.
True
-
b.
False
-
a.
-
8.
The following are accepted treatment options for a patient with organ failure due to infected necrotizing pancreatitis, except ?
-
a.
Necrosectomy with closed irrigation
-
b.
Necrosectomy with open packing
-
c.
Antibiotic therapy alone
-
d.
Retroperitoneal necrosectomy
-
e.
Percutaneous lavage
-
a.
Answers: 1. a, 2. a, 3. b, 4. a, 5. a, 6. d, 7. b, 8. c.
2 Introduction
Acute pancreatitis definition:
-
Acute inflammatory process of the pancreas with a wide range of manifestations and clinical variation, ranging from local inflammation to systemic manifestations such as organ failure.
-
The frequency of acute pancreatitis varies among different countries.
-
In the USA, the frequency of pancreatitis is higher in patients older than 65 years.
-
The rate of pancreatitis in black Americans is 3 times higher than in white Americans.
-
The frequency of pancreatitis is approximately equal in men and women.
Acute pancreatitis is classified into two types.
-
Acute edematous interstitial pancreatitis (AIEP) (85 %) (Figs. 14.1–14.2)
Fig. 14.1 
Interstitial edematous pancreatitis, gross and histologic appearance. In situ photographs (a, b) in a patient with interstitial edematous pancreatitis showing an irregular area of hemorrhage infiltrating the peripancreatic tissues and extending into the mesentery of the small bowel (arrows). Note the tissue retraction due to bands of fibrous tissue. Microphotograph (c) (H&E, 50×) shows acini (arrow) adjacent to an edematous stroma with scattered neutrophils and few plasma cells (left right-up arrow)
-
Acute inflammation of the pancreatic parenchyma and peripancreatic tissues
-
-
Necrotizing pancreatitis (NP), (15 %) (Fig. 14.3)
Fig. 14.3 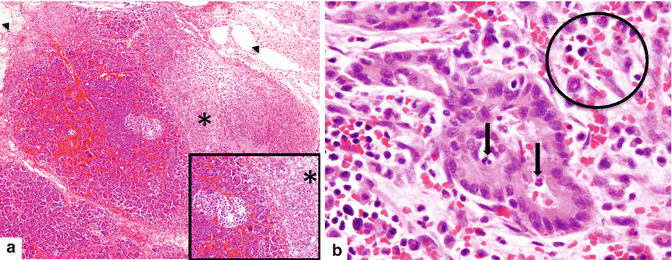
Necrotizing pancreatitis, gross and histologic appearance. In situ photograph (a) and surgical specimen (b) show amorphous necrotic pancreatic and adipose tissue secondary to enzymatic autolysis (a) (arrows). Microphotograph (c) demonstrates necrotizing pancreatitis surrounded by hemorrhage, acute and chronic inflammation, and early fibrosis. Note the complete destruction of a pancreatic lobule (long arrow). The adjacent pancreatic lobule retains normal architecture (short arrow) (H&E, 10×)
-
Inflammation associated with pancreatic parenchymal necrosis and peripancreatic necrosis
-
Sterile or infected
-


3 Pathophysiology
-
First phase: premature activation of trypsin within pancreatic acinar cells
-
Second phase: intrapancreatic inflammation through a variety of mechanisms and pathways
4 Histopathology

Acute hemorrhagic pancreatitis, histology. (a) Acute hemorrhagic pancreatitis with areas of parenchymal (asterisk) and fat necrosis (arrowheads). The inset highlights the red blood cell infiltrate surrounding an islet of Langerhans cells and multiple viable and necrotic acini (H&E, 10×, 20×). (b) The inflammatory infiltrate is composed of neutrophils, lymphocytes, and red blood cells (circle). Neutrophils are also present in the lumen and the epithelium of the ducts (arrows). The stroma surrounding the ducts demonstrates mild edema (H&E, 50×)
-
Necrotizing vasculitis with occlusion and thrombosis of small feeding arteries and draining veins
-
Perilobular and/or panlobular fat necrosis affecting the acinar cells, islet cells, pancreatic ductal system, interstitial fatty tissue, areas of hemorrhage, and devitalized pancreatic parenchyma
5 Etiology of Acute Pancreatitis
-
Most common (80 %)
-
Gallstones
-
Alcohol
-
-
Other causes (20 %)
-
Smoking tabacco
-
Cannabis
-
Hypertriglyceridemia
-
Hypercalcemia
-
Trauma
-
Post ERCP (Post Endoscopic Retrograde Cholangio-pancreatography
-
Genetic mutations (hereditary pancreatitis)
-
Idiopathic
-
Pregnancy
-
Pancreatic divisum
-
Pancreatic neoplasms (adenocarcinoma, IPMN, or neuroendocrine)
-
-
Drugs
-
Immunomodulators
-
6-Mercaptopurine, azathioprine, TNF-α blockers, mycophenolate, tacrolimus, and cyclosporine
-
-
Neurology drugs
-
Valproic acid, carbamazepine, mirtazapine, SSRI, and gabapentin
-
-
Analgesics
-
Sulindac, mesalamine, acetaminophen, opiates, celecoxib, and diclofenac
-
-
Diuretics
-
Furosemide and thiazides
-
-
Antibiotics
-
Trimetropin/sulfamethoxazole, tetracycline, macrolides, rifampin, pentamidine, ceftriaxone, and metronidazole
-
-
Antivirals
-
Didanosine, pegylated interferon-alpha, and lamivudine
-
Hormones
-
Estrogens, steroids, and octreotide
-
-
Chemotherapy
-
Asparaginase, cytarabine, cisplatin, doxorubicin, and vincristine
-
-
Cardiac medications
-
Enalapril, angiotensin receptor blockers, and amiodarone
-
Other common drugs
-
Omeprazole, ranitidine, cimetidine, statins, gliptins, metformin, isotretinoin, and saw palmetto
-
-
-
Infections
-
Viral
-
Mumps, coxsackie, hepatitis B, cytomegalovirus, varicella zoster, herpes simplex, and HIV virus
-
-
Fungal
-
Aspergillus
-
-
Parasitic
-
Toxoplasma, Cryptosporidium, Ascaris, and Clonorchis
-
-
-
Vascular Disease
-
Systemic lupus erythematous
-
Polyarteritis nodosa
-
Atheroembolism
-
Intraoperative hypotension
-
6 Clinical Presentation
-
Acute onset of epigastric and periumbilical pain that may radiate to the back flanks and lower abdomen
-
Nausea and vomiting
-
Severe pancreatitis: fever, hypoxemia, and hypotension
-
Signs of retroperitoneal bleeding:
-
Echymotic discoloration in periumbilical region (Cullen’s sign)
-
Echymotic discoloration along the flank (Grey Turner’s sign)
-
-
Physical examination:
Findings vary depending upon the severity of acute pancreatitis
-
Minimal to severe epigastric tenderness
-
Abdominal distention and hypoactive bowel sounds in case of secondary ileus
-
7 Laboratory Evaluation
-
Serum levels of amylase or lipase ≥3 times the upper limit of normal. (Plasma lipase is more sensitive and specific than plasma amylase.)
-
Leukocytosis
-
Elevated hematocrit from hemoconcentration (extravasation of fluid into third spaces)
Practical Pearls
-
Hyperamylasemia is not specific for acute pancreatitis and may be seen associated with a perforated duodenal ulcer, intestinal obstruction or infarction, cholecystitis, acute peritonitis, and renal insufficiency.
-
The serum amylase may be normal in patients with alcoholic pancreatitis due to the inability of the chronically damaged pancreatic parenchyma to produce amylase.
-
Patients with normal hematocrit and serum level creatine and without rebound or guarding are unlikely to experience complications related to pancreatitis, positive predictive value of 98 %.
-
Diagnosis of acute pancreatitis requires two of the following three features:
-
Characteristic abdominal pain suggestive of acute pancreatitis
-
Serum amylase and/or lipase ≥3 times the upper limit of normal
-
Characteristic findings of acute pancreatitis on CT, MR, or US
-
8 Differential Diagnosis
-
Perforated gastric or duodenal ulcer
-
Mesenteric ischemia or bowel infarction
-
Acute cholecystitis
-
Acute biliary colic
-
Bowel obstruction
-
Inferior wall myocardial infarction
-
Abdominal aortic dissection
9 Phases of Acute Pancreatitis
9.1 Early Phase
-
Systemic disturbances from host response to local pancreatic injury.
-
Usually occurs by the end of the first week but may extend into the second week.
-
Cytokine cascades are activated by pancreatic inflammation which manifest clinically by the systemic inflammatory response syndrome (SIRS).
-
10–20 % of patients develop a systemic inflammatory response syndrome (SIRS).
-
SIRS (defined by two or more of the following criteria):
-
Pulse rate >90 beats/min
-
Respiratory rate of >20 breaths/min or PaCO2 of <32 mmHg
-
Temperature >38.3 C or <36.0 C
-
WBC count of >12,000 cells/ml, <4,000 cells/mm3, or >10 % immature bands (forms)
-
9.2 Late Phase
-
Persistent signs of systemic inflammation or by the presence of local complications
-
Occurs in patients with moderate to severe or severe acute pancreatitis
-
The SIRS in the early phase may be followed by a compensatory anti-inflammatory response syndrome (CARS) that may contribute to an increased risk of infection (translocation of bacteria)
Practical Pearls
-
Local complications evolve during the late phase
-
Radiologic imaging plays a very important role in distinguishing the morphology of local complications for the patient’s management
-
Organ Failure
-
Shock, pulmonary insufficiency, renal failure, or gastrointestinal bleeding
-
10 Definition of Severity of Acute Pancreatitis
10.1 Atlanta Classification
-
Mild acute pancreatitis
-
Absence of organ failure and the absence of local or systemic complications
-
Most patients do not require pancreatic imaging and are usually discharged within 3–5 days of onset of illness
-
-
Moderate to severe acute pancreatitis
-
Presence of transient organ failure or local systemic complications in the absence of persistent organ failure
-
Patients require extended hospitalization but have lower mortality rates than patients with severe acute pancreatitis
-
-
Severe acute pancreatitis
-
Persistent organ failure
-
Single or multiple organ failure
-
Associated with 30–50 % mortality risk
-
Most patients with persistent organ failure have pancreatic necrosis
-
11 Scoring Systems to Determine the Severity of Acute Pancreatitis
-
The initial 12–24 hours of hospitalization is critical during patient management because the highest incidence of organ dysfunction occurs during this period
-
A number of clinical scoring systems have been developed to facilitate risk stratification during this phase
11.1 Bedside Index of Severity of Acute Pancreatitis
Each of these criteria counts as a single point.
-
BUN >25
-
Impaired mental status
-
SIRS
-
Age: 60 years or older
-
Pleural effusion
-
A Bedside Index of severity score >2 points performed during the first 24 hours of hospitalization is associated with a sevenfold risk increase of organ failure and tenfold risk increase of mortality
-
11.2 Harmless Acute Pancreatitis Score
Identify patients at the time of admission who are unlikely to experience complications related to acute pancreatitis.
-
Normal hematocrit and serum level of creatinine without rebound tenderness or guarding
-
Unlikely to develop severe pancreatitis
-
Positive predictive value of 98 %
11.3 Acute Physiologic and Chronic Health Examination (APACHE) II Score
-
Applied within 24 hours of patient admission to an intensive care unit.
-
Score is computed based on several measurements.
-
Higher scores correspond to more severe disease and higher risk of death.
-
Twelve physiologic measurements: age, temperature (rectal), mean arterial pressure, arterial ph, heart rate, respiratory rate, sodium-potassium serum, creatinine, hematocrit, white blood cell count, and Glasgow Coma Scale
11.4 Modified CT Severity Index
Modified CT severity index
Prognostic indicator | Points |
|---|---|
Pancreatic inflammation | |
Normal pancreas | 0 |
Intrinsic pancreatic abnormalities with or without inflammatory changes in peripancreatic fat | 2 |
Pancreatic or peripancreatic fluid collection or peripancreatic fat necrosis | 4 |
Pancreatic necrosis | |
None | 0 |
≤30 % | 2 |
>30% | 4 |
Extrapancreatic complications (one or more of pleural effusion, ascites, vascular complications, parenchymal complications, or gastrointestinal tract involvement) | 2 |
Total score: points are given on a scale from 0 to 10 to determine the grade of pancreatitis and treatment | |
Practical Pearls
-
Many scoring systems have been reported, but none has proven to be perfect.
-
They are superior to clinical judgment for triaging patients to more intensive and aggressive therapy.
12 Imaging
-
Computed tomography (CT) and magnetic resonance imaging (MRI) are the preferred imaging modalities.
-
Contrast-enhanced CT (CECT) is currently the gold standard for evaluating patients with suspected acute pancreatitis.
-
The role of this modality is to confirm or exclude the clinical diagnosis, to establish the cause, to determinate the severity, to detect complications of the acute pancreatitis, and to provide guidance for therapy.
-
Very useful to predict clinical outcome.
-
MR imaging is particularly useful in pregnant patients and in patients who cannot receive iodinated contrast material due to allergic reactions or renal insufficiency.
-
Abdominal ultrasound is an inexpensive, convenient imaging modality helpful to evaluate the presence of gallbladder and/or common duct stones in acute pancreatitis.
Practical Pearls
-
CECT should always be performed 48–72 hours after admission to distinguish interstitial from necrotizing pancreatitis when there is clinical evidence of increased severity.
-
CECT is not recommended earlier because it may provide false information due to pancreatic edema and/or vasoconstriction.
-
The pancreas may appear normal in approximately 25 % of patients with mild pancreatitis.
12.1 Chest Radiographs

Pleural effusion associated with acute pancreatitis. A 43-year-old female with biliary pancreatitis. Portable chest radiograph shows a mild left pleural effusion (arrow)

Pleural effusion associated with acute pancreatitis. A 54-year-old female with interstitial biliary pancreatitis that eventually became necrotic. Portable chest radiograph shows a moderate left pleural effusion (arrow)

Acute respiratory distress syndrome (ARDS) associated with acute pancreatitis. A 75-year-old female patient admitted with acute pancreatitis. Two days after admission, she was hypotensive, oliguric, and hypoxic. Patient was transferred to the intensive care unit. Subsequently, she developed severe hypoxia that required intubation. CECT axial image (a) shows a homogeneous pancreas with mild peripancreatic inflammatory changes (arrows). Sequential portable chest radiographs performed (b) at admission, (c) 1 week following admission, and (d) 2 weeks and (e) 3 weeks after admission demonstrate the progression of bilateral diffuse air space disease in both lungs. Findings suggestive of acute respiratory distress syndrome (ARDS). The patient eventually expired due to multisystemic failure
Findings
-
Pleural effusion (more common on the left side)
-
Basal pulmonary atelectasis
-
Elevation of the hemidiaphragm
-
Progressive diffuse bilateral air space disease (acute respiratory distress syndrome ARDS)
12.2 Abdominal Radiographs (Figs. 14.7–14.10)

Paralytic ileus associated with acute pancreatitis. A 51-year-old female with history of abdominal distention and iatrogenic acute pancreatitis secondary to recent endoscopic retrograde cholangiopancreatography (ERCP). Supine abdominal radiograph reveals distended small bowel loops in the mid abdomen (arrows). Findings suggestive of a localized small bowel ileus

Paralytic ileus associated with acute pancreatitis. A 61-year-old male with a left ventricular assist device (LVAD). Patient developed epigastric pain and abdominal distention. Supine abdominal scanogram (a) reveals the distention of multiple small bowel loops in the mid abdomen (arrows), as well as distention of the transverse colon. Findings suggestive of a paralytic ileus versus bowel obstruction. CECT axial image (b) reveals peripancreatic inflammatory changes (arrowheads) suggestive of acute interstitial pancreatitis. There was no evidence of bowel obstruction

Colon cut-off sign in acute pancreatitis. A 34-year-old male with alcoholic pancreatitis. (a) Supine abdominal radiograph shows distention of the ascending and transverse colon with an abrupt cutoff at level of the splenic flexure (arrow). CECT axial images (b, c) show distention of the transverse colon with an abrupt transition of the diameter at the level of the splenic flexure (b) (arrow) adjacent to the peripancreatic inflammatory changes. Note the spasm and paucity of air in the descending colon (c) (arrowhead)

Infected pancreatic necrosis on abdominal radiograph. A 40-year-old male with history of alcoholic pancreatitis, fever, and leukocytosis. Supine abdominal radiograph (a) demonstrates extraluminal pockets of air between the stomach and transverse colon and in the left upper quadrant (arrows). Finding suggestive of extraluminal gas in the upper retroperitoneum. Axial images (b, c) of CECT performed the same day demonstrate inflammatory changes in the pancreas associated with extensive pockets of air in the pancreatic parenchyma, as well as in the peripancreatic tissues (arrows)
Findings
-
Duodenal ileus
-
Localized abdominal ileus (sentinel loop/s)
-
Gasless abdomen
-
Colon cut-off sign (paucity of colonic gas distal to the splenic flexure due to functional spasm of the descending colon secondary to the extrapancreatic inflammation)
-
Abnormal air bubbles in the topography of the pancreas (infected pancreatic necrosis or pancreatic abscess)
-
Mass effect in the gastrointestinal tract (intra or extrapancreatic fluid collections)
12.3 Ultrasound (Figs. 14.11–14.19)

Acute pancreatitis on ultrasound. A 45-year-old female with alcoholic pancreatitis. Transverse scan demonstrates an enlarged pancreas with decreased echogenicity and ill-defined margins (arrows)

Acute pancreatitis on ultrasound. A 48-year-old male with alcoholic pancreatitis. Transverse scan reveals an enlarged pancreas with mild heterogeneous echogenicity (arrows)

Acute pancreatitis on ultrasound. A 29-year-old male with medication-induced acute pancreatitis. Transverse (a) and sagittal (b) scans show diffuse enlargement of the pancreas. Note the mild increased echogenicity of the pancreatic parenchyma (arrows)

Acute pancreatitis on ultrasound. A 54-year-old male with alcoholic pancreatitis. Transverse scan shows diffuse enlargement and decreased echogenicity of the pancreas. Note the ill-defined margins of the pancreas and the presence of a small amount of peripancreatic fluid (arrows)

Acute pancreatitis on ultrasound. A 38-year-old female with biliary pancreatitis. Transverse image reveals a hypoechoic, enlarged pancreas with ill-defined margins (arrows)

Acute pancreatitis on ultrasound. A 41-year-old female with biliary pancreatitis. Transverse image shows an enlarged pancreas with decreased echogenicity and posterior acoustic enhancement (arrows). Findings suggestive of pancreatic necrosis

Acute pancreatitis on ultrasound. A 65-year-old male with alcoholic pancreatitis. Transverse scan shows a hypoechoic pancreas with ill-defined margins and posterior acoustic enhancement (arrows)

Biliary pancreatitis on ultrasound. A 29-year-old female with acute onset of epigastric pain, jaundice, and hyperamylasemia. An abdominal ultrasound was performed to evaluate the pancreas and the biliary system. Transverse scan of the gallbladder (a) reveals multiple gallstones (arrows). Oblique scan of the right upper quadrant (b) reveals a dilated common bile duct with a distally impacted stone (arrowhead). The pancreas was not visualized due to the presence of abundant abdominal gas. Plain CT axial images (c, d) corroborate the presence of multiple gallstones (arrows), the presence of a biliary stone in the distal common bile duct (arrowhead), and peripancreatic inflammatory changes

Indirect signs of acute pancreatitis on ultrasound. A 63-year-old male with epigastric pain and elevated serum lipase. Transverse and sagittal scans (a, b) show a small amount of fluid anterior to the upper pole of the right kidney (arrows). The pancreas could not be demonstrated due to the presence of abundant abdominal gas. Axial (c) and sagittal (d) CECT images performed the same day show mild enlargement of the pancreas, inflammatory changes around the pancreas (arrowheads), and a small amount of fluid anterior to the right kidney (arrows)
Findings
-
Normal size or enlarged pancreas
-
Decrease or increase of the echogenicity of the pancreatic parenchyma
-
Normal or ill-defined pancreatic margins
-
Intra- and/or peripancreatic fluid collections
-
Presence of gallstones and/or choledocolithiasis
Practical Pearls
-
Ultrasonography has severe limitations and the presence of excess abdominal gas (ileus), or patient’s obesity often occlude the visualization of the pancreas.
-
This technique has limited capability in delineating the extent of the extrapancreatic inflammation and/or the detection of pancreatic necrosis.
12.4 Contrast-Enhanced CT (CECT)

Acute interstitial pancreatitis in four different patients on CT. Patient #1: A 30-year-old female with history of diabetes, bipolar disorder, and idiopathic pancreatitis. CECT axial image (a) shows a homogeneous enhancement of the pancreatic gland and mild inflammatory changes around the pancreas (arrows). Patient #2: A 42-year-old male with alcohol-related acute pancreatitis. CECT axial image (b) shows a homogeneous enhancement of the pancreatic gland and mild peripancreatic inflammatory changes (arrows). Patient #3: A 61-year-old male with acute pancreatitis induced by medications. CECT axial image (c) shows a homogeneous enhancement of the pancreas and moderate peripancreatic inflammatory changes (arrows). Patient #4: A 53-year- old male with biliary pancreatitis. CECT axial image (d) shows extensive inflammatory changes in the left and right anterior pararenal spaces as well as in the lesser sac (arrows). Note the heterogeneous enhancement of the pancreas

Acute interstitial pancreatitis in two different patients on CT. Patient #1: A 27-year-old male with biliary pancreatitis. CECT axial image (a) demonstrates heterogeneous enhancement of the pancreatic parenchyma (arrows) and extensive peripancreatic inflammatory changes in the retroperitoneum extending into the mesentery (arrowheads). Patient #2: A 63-year-old male with alcohol-related pancreatitis. CECT axial image (b) demonstrates mild heterogenecity and enlargement of the pancreatic gland with a small amount of fluid in both anterior pararenal spaces, the lesser sac, and subhepatic space (arrows)

Acute interstitial pancreatitis sparing the pancreatic head on CT. A 33-year-old with history of alcohol-related pancreatitis. CECT axial (a–c) and coronal (d) images reveal inflammatory changes around the body and tail of the pancreas (arrows). Note the absence of inflammatory changes around the head of the pancreas (arrowheads)

Acute interstitial pancreatitis associated with extensive perinflammatory changes on CT, clinically mimicking acute appendicitis. A 37-year-old male with diabetic ketoacidosis, dehydration, leukocytosis, and elevated triglyceride levels, complaining of 2 days of periumbilical pain. At admission, the pain was more localized in the right lower quadrant. Findings suggestive of acute appendicitis. CECT coronal (a–c) and sagittal (d) images show poor enhancement of the pancreas and extensive peripancreatic inflammatory changes around the pancreas extending from the root of the mesentery to the right lower quadrant (arrows)


Acute interstitial pancreatitis secondary to hyperparathyroidism on CT. A 41-year-old man with history of intermittent abdominal pain, weakness, bone fractures, joint pain, and episodes of depression. Laboratory: lipase 4,000 units/L, amylase 794 units/L, and serum calcium 14. AP plain film of the skull (a) shows multiple small lytic lesions (arrows). Plain film of the humerus (b) demonstrates an expansile lesion in the proximal shaft (arrows), brown tumor. CECT axial images of the abdomen (c, d) show a heterogeneous, mildly enlarged pancreas and peripancreatic inflammatory changes (arrows). A CT of the chest was performed to evaluate for an ectopic parathyroid adenoma suggested in a Sestamibi study. CECT axial images of the superior chest (e, f) show two a parathyroid adenomas, one posterior to the right lobe of the thyroid (e) (arrow) and the second in the left superior mediastinum (f) (arrow). The patient was taken to the OR with a diagnosis of primary hyperparathyroidism. During surgery, 6 enlarged parathyroid glands were discovered. Photograph (g) shows the enlarged parathyroid glands surgically removed

Focal acute interstitial pancreatitis associated with pancreatic malignancy on CT. A 65-year-old male with acute epigastric pain, hyperamylasemia, and weight loss. CECT arterial phase (a) and portal phase (b) axial images show focal peripancreatic stranding in the distal body and tail of the pancreas (arrows). Note the presence of a low attenuation mass in the same region (arrowheads). Patient underwent a distal pancreatectomy. Final diagnosis: adenocarcinoma of the pancreatic body associated with distal acute pancreatitis

Acute interstitial pancreatitis associated with pancreatic malignancy on CT. A 70-year-old male with history of repetitive attacks of acute pancreatitis, complaining of severe epigastric pain. CECT axial (a) and coronal (b) images show mild peripancreatic inflammatory changes in the body and tail of the pancreas (a) (arrows). Note the presence of an ill-defined cystic mass in the neck of the pancreas (a, b) (arrowheads) associated with mild dilatation of the pancreatic duct. Patient underwent extended pancreaticoduodenectomy. Final pathology: IPMN with small focus of invasive carcinoma

Acute interstitial pancreatitis associated with a benign intraductal papillary mucinous neoplasm (IPMN) on CT. A 72-year-old male with repetitive attacks of acute pancreatitis. CECT axial images (a, b) demonstrate diffuse peripancreatic inflammatory changes (arrows) and an ovoid cystic mass (b) (arrowhead) in the uncinate process. Single-shot fast spin echo T2-weighted coronal image (c) corroborates the presence of a cystic mass in the head of the pancreas (arrowhead) and the peripancreatic inflammatory changes (arrows). Patient underwent a pancreaticoduodenectomy. Final pathology: IPMN with borderline changes

Acute interstitial pancreatitis induced by ERCP and biliary stent placement on CT. A 40-year-old male with cirrhosis secondary to hepatitis C with a prior liver transplant. Patient developed a biliary stricture at the level of the biliary anastomosis. This stricture was treated with a biliary stent placed under endoscopy. One day following this procedure, patient complained of severe epigastric pain. CECT axial images (a, b) reveal marked peripancreatic inflammatory changes around the pancreas extending into the mesentery (arrows). Note the presence of a biliary stent in the common bile duct (arrowheads)

Postsurgical acute interstitial pancreatitis on CT. A 57-year-old female who underwent a pancreaticoduodenectomy for an IPMN in the head of the pancreas complaining of epigastric pain 48 hours post surgery. Serum amylase was elevated. CECT axial images (a, b) demonstrate postsurgical absence of the pancreatic head and marked peripancreatic inflammatory changes (arrows) along the body and tail suggestive of acute pancreatitis. Note the presence of a surgical drain in the subhepatic region (arrowhead)

Necrotizing pancreatitis on CT. A 63-year-old female with history of gallstones and epigastric pain, admitted to the hospital with a diagnosis of biliary pancreatitis. Forty-eight hours after admission, patient underwent a cholecystectomy with exploration of the CBD. Seven days following surgery, the patient was hypotensive, diaphoretic, and with severe epigastric pain. CECT axial images (a, b) demonstrate enlargement of the pancreas and lack of enhancement of the parenchyma in the body and tail (arrows) associated with mild peripancreatic inflammatory changes

Necrotizing pancreatitis on CT. A 33-year-old male complaining of 4 days of increased abdominal pain, nausea, vomiting, and fevers. Patient states that he drinks 6–12 beers a day. Labs: serum lipase of 1,400 units/L. Patient was admitted to the SICU for intravenous fluid resuscitation. CECT axial images (a, b) demonstrate lack of contrast enhancement of the pancreatic parenchyma in the body and tail of the pancreas (arrows) and severe peripancreatic inflammatory changes

Necrotizing pancreatitis on CT. A 62-year-old male with history of alcoholic pancreatitis and leukocytosis. CECT axial image reveals mild enlargement of the body and tail of the pancreas with poor enhancement of the pancreatic parenchyma (arrows). Note the presence of a small blood clot in the superior mesenteric vein (arrowhead) and the peripancreatic inflammatory changes

Necrotizing pancreatitis on CT. A 38-year-old male with history of alcohol abuse, complaining of intense abdominal pain. CECT axial image shows enlargement of the head and body of the pancreas with poor enhancement of the pancreatic parenchyma (arrows), peripancreatic inflammatory changes, and a blood clot at the junction of the superior mesenteric vein and splenic vein (arrowhead)

Necrotizing pancreatitis on CT. A 56-year-old female with epigastric pain, with elevated serum amylase and lipase. Patient was transferred to the ICU for supportive care. Initial ultrasound and transverse images (a, b) show gallstones and mild enlargement of the pancreas with a hypoechoic pancreatic parenchyma. CECT axial image (c) shows lack of contrast enhancement of the pancreatic parenchyma (arrows) and mild peripancreatic inflammatory changes

Necrotizing pancreatitis on CT. A 63-year-old female with history of gallstones and epigastric pain was admitted to the hospital with a diagnosis of biliary pancreatitis. Forty-eight hours after admission, patient underwent a cholecystectomy with exploration of the CBD. Seven days post surgery, the patient became hypotensive and diaphoretic and experienced severe epigastric pain. CECT axial (a, b) and coronal (c, d) images demonstrate severe diffuse enlargement of the pancreas with lack of enhancement of the pancreatic parenchyma (a–d) (arrows) and mild peripancreatic inflammatory changes

Necrotizing pancreatitis on CT. A 38-year-old male with history of acute pancreatitis of unknown etiology complaining of persistent abdominal pain. Non-contrast-enhanced CT axial image (a) done at admission reveals prominent peripancreatic inflammatory changes (arrow), diffuse fatty infiltration of the hepatic parenchyma, and gallbladder distention. CECT axial (b) image performed 3 weeks later reveals lack of enhancement of the pancreatic parenchyma in the body and tail of the pancreas (arrow). CECT axial (c) image done 20 weeks after the initial presentation reveals mild atrophy of the body and tail of the pancreas and persistent lack of enhancement in this region (arrow). Due to the persistent symptomatology and unusual radiologic findings, the patient underwent a distal pancreatectomy to rule out a tumor associated with pancreatitis. Final pathology: pancreatic necrosis without evidence of tumor

Necrotizing pancreatitis on CT. A 52-year-old male who presented 6 months earlier with signs of acute pancreatitis, now with persistent left upper quadrant pain. At admission, a plain CT (a) demonstrated peripancreatic inflammatory changes around the body and tail of the pancreas (arrow). At 4 weeks, a CECT (b) shows enlargement of the body and tail of the pancreas and lack of contrast enhancement of the pancreatic parenchyma (arrow). At 6 weeks, CECT (c) shows no significant change (arrow). Due to the persistent pain and CT findings, the possibility of a pancreatic neoplasm associated with focal pancreatitis was considered. Patient underwent a distal pancreatectomy and splenectomy. Photograph of the gross specimen (d) shows necrosis of the body and tail of the pancreas. Final pathology: focal pancreatic necrosis without evidence of pancreatic tumor

Infected pancreatic necrosis on CT. A 25-year-old male with acute alcoholic pancreatitis, fever, and leukocytosis. CECT axial image reveals a large collection of air in the head and proximal body of the pancreas (arrows) associated with lack of enhancement of the pancreatic parenchyma and the presence of peripancreatic inflammatory changes

Infected pancreatic necrosis on CT. A 37-year-old female with biliary pancreatitis and multiorgan failure. CECT coronal image shows diffuse enlargement of the pancreas with lack of pancreatic enhancement and multiple pockets of air (arrows)

Evolution from interstitial acute pancreatitis to noninfected necrotizing pancreatitis to infected pancreatic necrosis on CT. A 55-year-old male admitted with biliary pancreatitis. At 72 following admission, CECT axial image (a) shows mild peripancreatic inflammatory changes. At 3 weeks, CECT axial image (b) shows diffuse enlargement of the pancreas and lack of enhancement of the pancreatic parenchyma (arrows). At 4 weeks, CECT axial image (c) shows persistent necrosis of the pancreas associated with a small amount of air bubbles (arrow). At 6 weeks, CECT axial image (d) shows progression of the air pockets in the necrotic pancreatic parenchyma (arrows)

Perforated duodenal ulcer mimicking infected necrotizing pancreatitis on CT. A 42-year-old male with history of duodenal ulcer complaining of acute onset of epigastric pain and having elevated serum amylase. CECT axial (a–c) and coronal (d) images reveal peripancreatic inflammatory changes associated with air pockets (arrows) surrounding the head and neck of the pancreas. Patient underwent an upper endoscopy that showed an active peptic ulcer. Patient had a good response to proton pump inhibitor treatment and was discharged from the hospital a week later. A control abdominal CT (not shown) demonstrated complete resolution of the peripancreatic inflammatory changes and air pockets

Acute duodenal diverticulitis mimicking infected necrotizing pancreatitis on CT. A 72-year-old male with history of a duodenal diverticulae, complaining of acute epigastric pain and fever. Patient had an elevated white blood cell count, and normal serum, amylase, and lipase. CECT axial (a) and coronal (b) images demonstrate a complex collection of fluid and air in the head of the pancreas (arrows) with mild peripancreatic stranding. Note that the presence of duodenal diverticulum is associated with this collection (arrowhead). Patient was treated with antibiotics. Fluoroscopic image (c) from an UGI study performed a week after following antibiotic therapy demonstrates a large duodenal diverticulum (arrow)

Infected pancreatic necrosis on CT. A 27-year-old male with history of alcoholism developed necrotizing pancreatitis. Patient admitted clinically stable with a sudden deterioration of clinical status, developing a fever and an elevated white count. Previous abdominal CT performed (not shown) demonstrated diffuse necrosis of the pancreas. Possibility of a superinfection of the pancreatic necrosis was considered and therefore aspirated under CT guidance. Material was sent for gram stain and culture/sensitivity. Axial image (a) shows the tip of an 18 gauge sheath needle in the body of the pancreas. Photograph (b) demonstrates the 30 cc of the frank purulent material aspirated. Culture yielded polymicrobial organisms. This infected pancreatic necrosis was managed successfully with percutaneous catheter drainage and antibiotics

Pancreatic and peripancreatic necrosis on CT. A 51-year-old female with biliary pancreatitis and severe respiratory insufficiency. CECT axial (a–d) images show enlargement and necrosis of the body and tail of the pancreas in addition to multiple encapsulated heterogeneous extrapancreatic fluid collections with thick walls in the right inframesocolic region, left anterior pararenal space, and in the right and left extraperitoneal spaces of the pelvis (arrows). Note the areas of high density in the collections located in the right side of the pelvis (arrowheads). Finding suggestive of hemorrhage

Walled off sterile peripancreatic necrosis on CT. A 52-year-old female with acute pancreatitis secondary to a placement of a biliary stent. Follow-up CECT axial (a–d) images, 4 weeks after initial acute attack demonstrate homogeneous, encapsulated peripancreatic collections in the anterior pararenal space and extending into the root of the mesentery (arrows)

Infected walled off collection on CT. A 24-year-old female with documented acute pancreatitis that developed fever and leukocytosis. CECT axial images (a, b) demonstrate well-demarcated, intraperitoneal and inframesocolic, heterogeneous collections with enhancing wall and multiple air pockets. These collections were drained percutaneously with CT guidance. CECT axial image (c) demonstrates a pigtail catheter inside one of the extrapancreatic collections (arrowhead). Photograph (d) shows the aspirated purulent material

Acute pancreatitis associated with pancreatic duct necrosis on CT. A 35-year-old HIV-positive male with acute pancreatitis. CECT axial image (a) and single-shot fast spin echo T2-weighted image (b) show a large intrapancreatic fluid collection in the body of the pancreas with a large exophytic component extending into the peripancreatic tissues. Note the disruption of the pancreatic duct and pancreatic parenchyma at the origin of the collection (arrows)

Acute pancreatitis associated with pancreatic duct necrosis on CT. A 42-year-old male with history of alcoholism, epigastric pain, and elevation of the serum lipase and amylase. CECT axial image displays disruption of the pancreatic parenchyma on the pancreatic body (arrows) associated with a large collection located in the lesser sac. Note the severe peripancreatic inflammatory changes in the left anterior pararenal space

Acute pancreatitis associated with pancreatic duct necrosis on CT. A 65-year-old male with history of alcoholic pancreatitis. CECT axial image shows a fluid collection in the parenchyma of the neck of the pancreas (arrows) and the presence of mild dilatation of the distal main pancreatic duct (arrowheads). Note the inflammatory changes around the pancreas
-
Acute interstitial pancreatitis (AIP) (Figs. 14.20–14.29)
Findings
-
Homogeneous or heterogeneous pancreatic parenchymal enhancement (diffuse or focal due to interstitial parenchymal edema)
-
Normal or mild to severe peripancreatic and retroperitoneal inflammatory changes (fatty stranding) depending on the severity of the acute pancreatitis
-
Varying amounts of peripancreatic fluid
-
Thickening of the retroperitoneal fascia
-
-
Necrotizing pancreatitis (NP) (Figs. 14.30–14.43)
Findings
-
Focal or diffuse lack of pancreatic parenchymal enhancement.
-
The extent of parenchymal necrosis is divided into three categories, depending on the amount of gland involved.
-
<30 % of gland necrosis
-
30–50 % of gland necrosis
-
>50 % of gland necrosis
-
-
The presence of air bubbles in the pancreatic parenchyma suggests an infected necrosis.
-
-
Peripancreatic necrosis alone
Findings
-
Heterogeneous peripancreatic areas of non-enhancement
-
Usually located in the retroperitoneum and lesser sac
-
Contains non-liquefied components
-
-
Pancreatic and peripancreatic necrosis (Figs. 14.44)
Findings
-
Combination of the findings described above
-
-
Walled off necrosis (WON) (Figs. 14.45–14.46)
-
Mature, encapsulated collection of pancreatic and/or peripancreatic necrosis that developed a well-defined inflammatory wall
-
Occurs >4 weeks after onset of necrotizing pancreatitis
-
Findings
-
Heterogeneous intrapancreatic and/or extrapancreatic fluid and non-liquid density with varying degrees of loculations
-
Well-defined, encapsulated wall
-
The presence of air bubbles within these collections suggest the presence of infection
-
Pancreatic duct necrosis (Figs. 14.47–14.49)
-
Necrosis between the pancreatic neck and tail.
-
Associated with disruption of the pancreatic duct.
-
Subtype of necrotizing pancreatitis.
-
Persistent mid-gland collection/s (continuous secretion of pancreatic juice by the pancreatic tail).
-
Poor response to percutaneous or endoscopic drainage.
-
Many cases require distal pancreatectomy as definitive treatment.
-
Findings
-
Pancreatic collection between the head of the pancreas and proximal tail of the pancreas, associated with central interruption of the main pancreatic duct
Practical Pearls
-
Usually, patients with pancreatic duct necrosis respond poorly to percutaneous or endoscopic drainage.
-
Many cases require distal pancreatectomy as definitive treatment.
-
Scarring of the distal pancreatic duct may lead to spontaneous resolution with subsequent chronic pancreatitis of the isolated distal pancreas.
12.5 Magnetic Resonance (MR)

Mild acute interstitial pancreatitis on MR. A 48-year-old male with history of alcohol abuse complaining of epigastric pain, nausea, and vomiting. Laboratory showed an elevated serum lipase. Fat-suppressed gradient echo T1-weighted axial images (a, b) show a normal signal intensity of the pancreatic parenchyma associated with mild perinflammatory changes (arrows). On single-shot fast spin echo T2-weighted axial images (c, d), the inflammatory changes around the pancreas become more evident (arrows). Fat-suppressed contrast-enhanced gradient echo T1-weighted axial (e, f) images show homogeneous enhancement of the pancreas and corroborates the presence of peripancreatic inflammatory changes (arrows)

Acute interstitial pancreatitis on MR. A 47-year-old male with history of gallstones, hypertension, diabetes, and epigastric pain. Single-shot fast spin echo T2-weighted coronal (a–c) and axial (d) images demonstrate mild, diffuse, peripancreatic inflammatory changes (arrows). The signal intensity of the pancreas appears normal. Note the presence of multiple small stones in the gallbladder (d) (arrowheads) and the mild thickening of the gallbladder walls. The biliary system appears normal


Synchronous acute pancreatitis and acute cholecystitis on US, CT, and MR. A 33-year-old female with right upper quadrant pain radiating to the epigastrium reporting episodes of nausea and vomiting. Patient had abnormal liver function tests: lipase of 18,086 units/L and leukocytosis. Patient was initially evaluated with an ultrasound of upper abdomen. Transverse images (a, b) demonstrate multiple stones in the gallbladder associated with pericholecystic fluid (arrows). Oblique scan of the right quadrant (c) shows a dilated common bile duct (diameter of 8 mm); transverse image of the pancreas (d) shows mild enlargement of the pancreas (arrows). CECT axial images (e, f) corroborate the presence of pericholecystic fluid (arrows) and dilatation of the CBD (arrowheads). Additionally, peripancreatic inflammatory changes are noted (arrows). Single-shot fast spin echo T2-weighted image (g) shows small stones in the common bile duct (arrows) and pericholecystic fluid. MRCP thick slab (h) shows diffuse inflammatory changes around the pancreas (arrows). The patient was treated with a laparoscopic cholecystectomy and endoscopic sphincterotomy

Necrotizing pancreatitis on MR. A 58-year-old male admitted with gallstone pancreatitis. Patient was transferred to the ICU for supportive care due to a rapid clinical deterioration. Fat-suppressed gradient echo T1-weighted images (a, b) demonstrate heterogeneous signal intensity of the pancreatic parenchyma (arrows). Single-shot fast spin echo T2-weighted axial images (c, d) demonstrate diffuse enlargement of the pancreas and a high signal intensity mixed with areas of low signal intensity in the body and tail of the pancreas (arrows)

Infected necrotizing pancreatitis on MR. A 72-year-old male with history of alcohol abuse and acute pancreatitis developed multiorgan failure, fever, and abnormal white cell count. Fat-suppressed gradient echo T1-weighted axial (a) and single-shot fast spin echo T2-weighted axial (b) images show enlargement of the pancreas with diffuse low signal intensity throughout the pancreatic parenchyma (arrows). Air in the pancreatic parenchyma was suspected. Immediately following the previous studies, an abdominal CT was performed. CECT axial image (c) corroborated the presence of multiple air pockets throughout the pancreas (arrows)
-
Interstitial pancreatitis (Figs. 14.50–14.52)
Findings
-
Diffuse or focal enlargement of the pancreas.
-
Pancreatic boundaries are blurred.
-
Normal or hypointense signal intensity of the pancreas relative to the liver on T1-weighted images and hyperintense on T2-weighted images.
-
Threadlike, interlobular, hyperintense structures (interlobular septal inflammation).
-
Peripancreatic and/or pancreatic edema or fluid collections.
-
-
Pancreatic necrosis (Figs. 14.53–14.54)
Findings
-
Focal pancreatic necrosis is characterized by spotted, patchy, non-enhancing pancreatic parenchyma on contrast-enhanced MR images.
-
Diffuse pancreatic necrosis is characterized by non-enhancing pancreatic parenchyma on dynamic contrast-enhanced MRI.
-
-
Infected pancreatic necrosis
Findings
-
Focal or diffuse, non-enhancing segments in the pancreatic parenchyma of low signal intensity associated with signal void areas (pockets of air in the pancreatic parenchyma)
-
Practical Pearl
-
The identification of air in the pancreatic parenchyma by magnetic resonance is challenging; however, it is suspected when signal void areas are identified. Corroboration by abdominal radiographs or CT is necessary.
13 Treatment
-
Patients with organ failure at admission have a higher mortality.
-
The highest mortality is among those patients with multisystem organ failure and sustained organ failure for >48 hours.
-
Patients with signs of organ failure require admission in an intensive care unit or step-down unit.
-
Organ failure (acute pancreatitis)
-
Approximately 10 % of patients. Mostly transient with very low mortality.
-
Median prevalence of organ failure in necrotizing pancreatitis is 54 % (more common in infected necrosis).
-
Practical Pearl
-
Respiratory failure is the most common form of organ dysfunction.
13.1 Treatment Guidelines
-
Vital signs, oxygen saturation, and fluid balance should be carefully monitored.
-
Aggressive IV fluid replacement is the cornerstone of therapy.
-
250–500 ml/h × 24–48 hours, with frequent reevaluations during that time.
-
Recommendations
-
Patients should have the head of the bed elevated.
-
Lactate Ringer’s solution reduces the incidence of SIRS compared to saline solution.
Practical Pearls
-
There is evidence that early aggressive fluid resuscitation prevents or minimizes pancreatic necrosis and improves survival.
-
Lactate Ringer’s solution is associated with positive effects on acid-base homeostasis.
-
Nutritional support
-
In mild pancreatitis, oral intake is restored within 3–7 days, when patient is hungry and does not have nausea or vomiting and pain is controlled without medications
-
Low-fat diet is recommended to start.
-
In severe pancreatitis, nutritional support should be initiated when it becomes clear that the patient will not be able to consume nourishment by mouth for several weeks.
-
Enteral feeding is preferable to total parenteral nutrition (stabilizes gut barrier function, is safer and less expensive than TPN).
-
Nasogastric (NG), nasoduodenal (ND), or nasojejunal (NJ) tube feedings are equivalent.
-
Unless patient is retching and vomiting in which case NJ is more reasonable.
-
-
Practical Pearl
-
Enteral feeding is associated with a reduction in mortality, systemic infection, and multiorgan dysfunction.
-
Organ dysfunction (management)
-
Pressor agents for sustained hypotension
-
Intubation and assisted ventilation for respiratory failure
-
Renal dialysis for intractable renal failure
-
13.2 Treatment of Infected Necrosis

Pancreatic necrosis treated with surgical marsupialization. A 45-year-old male with history of hepatitis C, acute pancreatitis, and respiratory and renal failure. Patient developed infected pancreatic necrosis and underwent open surgical debridement, with marsupialization of the lesser sac. Plain CT axial images (a, b) reveal diffuse enlargement of the pancreas with a heterogeneous pancreatic parenchyma and the presence of small air bubbles (arrowheads). Photograph (c) reveals the cast of necrotic tissue removed from the pancreatic bed. Photograph of the patient’s postsurgical abdomen (d) reveals a large surgical defect in the anterior abdominal wall from the previous marsupialization. Note the presence of a large surgical drain


Pancreatic necrosis treated with percutaneous external lavage. A 38-year-old male with infected pancreatic necrosis. Patient was treated by the interventional radiology service with multiple percutaneous lavages under fluoroscopy. Pre-procedure CECT axial image (a) shows diffuse necrosis and air pockets in the pancreatic parenchyma. Photograph (b–d) shows the catheters and cannulas used to perform the percutaneous lavages. CECT axial image (e) shows two drainage catheters (arrows) placed under CT guidance within the pancreatic bed (arrows). Fluoroscopic image (f) after catheter injection of diluted contrast shows the presence of an amorphous cavity in the pancreatic bed. Photograph (g) shows the material aspirated from the necrotic cavity after several lavages with saline solution through the catheters under fluoroscopic guidance (h). Sequential CECTs show the response of the pancreatic necrosis after several external lavages. CECT (i, j) done before the external lavages; CECT (k, l) performed 6 weeks later shows a decrease in size of the necrotic pancreatic parenchyma; CECT (m) performed 11 weeks later shows almost complete disappearance of the pancreatic necrosis. Note the atrophy of the pancreatic gland
-
Most patients with infected necrosis have systemic toxicity, fever, and leukocytosis.
-
CT-guided percutaneous aspiration with gram stain and culture is indicated when infected necrosis is suspected.
-
If gram-negative organisms are isolated, the antibiotics recommended are:
-
Carbapenem, a fluoroquinolone plus metronidazole, or a third-generation cephalosporin plus metronidazole pending results of culture sensitivity.
-
If gram stain reveals the presence of gram-positive bacteria, the antibiotic recommended is vancomycin until results of culture and sensitivity are determined.
-
-
Surgical debridement (Figs. 14.55)
-
Standard care for infected pancreatic necrosis
-
-
Types of surgery
-
Necrosectomy with close continuous irrigation via indwelling catheters
-
Necrosectomy with open packing
-
Necrosectomy with closed drainage without irrigation
-
-
Complications
-
Fascial dehiscence
-
Wound problems
-
Hemorrhage
-
Gastrointestinal fistulas
-
Incisional hernia
-
-
Current alternative procedures
-
Minimally invasive retroperitoneal necrosectomy
-
Laparoscopic necrosectomy with placement of large caliber drains under direct surgical inspection
-
Percutaneous external lavage of infected necrosis (Figs. 14.56)
-
Endoscopic drainage and lavage
-
Practical Pearls
-
Percutaneous external lavage of infected necrosis has significantly lower morbidity and mortality than surgical necrosectomy.
-
Best suited for the stable patient.
-
Its success depends on the close interdisciplinary approach between the surgeon and the interventional radiologist.
-
Requires multiple sessions, initially 3 times a week of aggressive lavage and suction debridement of necrotic material.
13.3 Gallstone Pancreatitis Management
-
Retained common bile duct stone could lead to organ failure.
-
By causing ascending cholangitis or intensification of the pancreatitis.
-
-
Urgent ERCP and biliary sphincterotomy (preferably within 48 hours of admission).
-
Indications
-
Severe biliary pancreatitis with retained bile duct stones
-
Acute cholangitis
-
-
-
Elective ERCP with biliary sphincterotomy
-
Indications
-
Imaging study demonstrating persistent common bile duct stone
-
Elevation of LFTs
-
Poor surgical candidate for laparoscopic cholecystectomy
-
Strong suspicion of bile duct stones postcholecystectomy
-
-
-
Indications for MRCP or endoscopic ultrasound to determine need for ERCP
-
Clinical course not improving sufficiently to allow timely laparoscopic cholecystectomy and intraoperative cholangiogram
-
Pregnant patient
-
High-risk difficult ERCP
-
-
Cholecystectomy
-
Laparoscopic cholecystectomy is the treatment of choice in biliary pancreatitis (BP) to prevent further attacks.
-
Surgery should be done when all symptoms have disappeared and laboratory values have returned to normal.
-
Surgery is recommended during admission or within 6 weeks.
-
Practical Pearl
-
The indication for early cholecystectomy is to prevent recurrent attacks of biliary pancreatitis, as recurrence rate is as high 30 % without removal of the gallbladder
14 Acute Pancreatitis: Complications
-
Peripancreatic fluid collections
-
Pseudocysts
-
Abscess
-
Hemorrhage
-
Pancreatic fistulas
-
Venous thrombosis
-
Gastric or bowel obstruction
14.1 Acute Peripancreatic Collection (Figs. 14.57–14.59)

Acute peripancreatic fluid collections on CT. A 35-year-old female with a history of biliary pancreatitis diagnosed 3 weeks prior to complaint of abdominal distention. CECT axial images (a, b) demonstrate multiple peripancreatic thin walled fluid collections in the lesser sac, root of the mesentery, and left anterior pararenal space (arrows)

Evolution of acute peripancreatic fluid collections on CT. A 30-year-old female with history of biliary pancreatitis and acute peripancreatic fluid collections. Axial images (a, b) from CECT performed at admission show an enlarged pancreas with heterogeneous density associated with mild peripancreatic inflammatory changes (arrowheads) and multiple fluid collections in the lesser sac and right anterior and right posterior pararenal spaces (arrows). Follow-up CECT axial images (c, d) performed 7 weeks after previous admission show a spontaneous dramatic decrease in size and number of the peripancreatic collections. Two residual collections are noted: smaller in size, one in the root the of mesentery (c) (arrows), and the other (d ) in the lesser sac (arrow)

Symptomatic acute peripancreatic collection on CT. A 27-year-old female with history of biliary pancreatitis, abdominal pain, shortness of breath, borderline renal function, and marked abdominal distention. CECT axial images (a, b) demonstrate multiple peripancreatic fluid collections with a thin wall, located in the lesser sac, left and right anterior pararenal spaces, root of the mesentery, and mesentery of the small bowel (arrows). Due to the patient’s progressive respiratory deterioration, it was decided to percutaneously drain these collections under CT guidance. Axial images (c, d) from CECT done after the percutaneous drainage demonstrate a significant decrease in size of the fluid collections. Patient’s clinical status improved dramatically after this procedure
-
Peripancreatic fluid collections associated with interstitial edematous pancreatitis with no associated pancreatic necrosis.
-
Occur within the first 4 weeks after onset of interstitial edematous pancreatitis.
-
Most are sterile and usually resolve spontaneously without intervention.
CECT Criteria
-
Homogeneous collection with fluid density
-
Confined by normal peripancreatic fat planes or small bowel mesentery
-
No definable wall
-
Adjacent to the pancreas
Treatment
-
Conservative
-
Percutaneous drainage in symptomatic patient
Practical Pearl
-
Significant clinical improvement has been noted after percutaneous drainage of large or multiple acute peripancreatic collections in patients with abdominal pain, vomiting, nausea, shortness of breath, or organ/multiorgan failure.
14.2 Pancreatic Pseudocyst
(For figures please refer to Chap. 18 )
-
Collection of pancreatic juice enclosed by a non-epithelialized wall that occurs as a result of acute pancreatitis.
-
A period of at least 4 weeks is required from the onset of acute pancreatitis to form a well-defined wall composed of granulation and fibrous tissue.
CECT Criteria
-
Well-encapsulated intra- or peripancreatic cystic mass
Treatment
-
Observation if patient is asymptomatic
-
Percutaneous or endoscopic catheter drainage
-
Surgical decompression by cyst-gastrostomy or cyst-jejunostomy
14.3 Pancreatic Abscess (Figs. 14.60–14.61)

Pancreatic abscess on CT. A 30-year-old male with history of diabetes experienced an attack of acute pancreatitis 4 weeks prior to admission and was discharged 1 week later. Patient returned to the emergency room complaining of chills and fever. Laboratory showed marked leukocytosis. Plain CT axial image reveals a large fluid collection with multiple gas bubbles involving the entire pancreas (arrows). This pancreatic abscess was drained successfully with a percutaneous catheter

Pancreatic abscess on CT. A 45-year-old female transferred from an outside institution with a diagnosis of complicated acute pancreatitis. At admission, patient presented with fever, abdominal pain, and leukocytosis. Plain CT axial image (a) reveals a large fluid collection involving the entire pancreas (arrows). The correlation of clinical and radiological findings was suggestive of a pancreatic abscess. Under ultrasound guidance, the pancreatic collection was aspirated. Fetid, frank purulent material was obtained (Photograph b)
-
Pancreatic or peripancreatic collection containing pus.
-
It is a life-threatening complication.
-
It may be secondary to an infected pseudocyst or intra- or peripancreatic collection.
-
-
Pancreatic abscess should be considered in any patient who is still febrile or becomes febrile 2 or more weeks after an attack of acute pancreatitis.
-
Other symptoms
-
Abdominal pain, nausea and vomiting, tenderness, palpable mass, leukocytosis, and occasional hyperamylasemia.
-
Infected collections usually contain one or more enteric organism or Candida if prior antibiotic has been instituted.
-
CT represents the most useful technique for diagnosing pancreatic abscess.
-
-
-
CECT criteria
-
Pancreatic or peripancreatic collection with intraluminal gas
-
Pancreatic or peripancreatic collection with peripheral wall enhancement
-
-
Differential diagnosis if intraluminal gas present
-
Fistulous connection with a hollow viscera
-
-
Treatment
-
Percutaneous or endoscopic catheter drainage
-
Surgical drainage recommended in unsuccessful percutaneous or endoscopic drainage, in complex multiloculated collections, or for collections difficult to access percutaneously
-
Practical Pearl
-
The absence of air pockets within a pancreatic collection or the lack of peripheral wall enhancement does not exclude the diagnosis of a pancreatic abscess. In questionable cases, fine-needle aspiration (FNA) of the collection with US or CT guidance is recommended for further evaluation.
14.4 Hemorrhagic Pancreatitis (Figs. 14.62–14.63)

Hemorrhagic pancreatitis on CT. A 78-year-old male transferred from an outside institution for complicated acute pancreatitis. Shortly after arriving, patient developed acute severe epigastric pain, altered mental status, shortness of breath, and signs of acute peritonitis. Plain CT axial (a–c) and coronal (d) images show diffuse enlargement of the pancreas. Note the diffuse amorphous high-density areas within the pancreas (arrows). Finding suggests the presence of acute hemorrhage. Patient underwent an exploratory laparotomy, during which multiple blood clots were found in the lesser sac as well as in the pancreatic bed. These blood clots were removed along with a large necrotic pancreatic cast. Patient had a complicated postoperative medical course with acute and chronic respiratory failure and eventually expired

Hemorrhagic pancreatitis on CT. A 58-year-old female with biliary pancreatitis who suddenly became tachycardic and hypotensive. Patient developed an ecchymotic area in the left flank (Grey Turner’s sign) (Photograph a) (arrows). Plain CT axial (b–d) images demonstrate extensive peripancreatic inflammatory changes associated with areas of high density (arrows). Finding suggestive of acute hemorrhage
-
Acute bleeding may occur in severe pancreatitis.
-
It is an unusual complication of acute pancreatitis.
-
Intraparenchymal and peripancreatic extravasations of activated enzymes are responsible for damage to the pancreatic vascular network including feeding capillaries, arteries, and/or draining veins.
-
Clinical Presentation
-
Change in the character of the abdominal pain, tachycardia, hypotension, and diaphoresis
Laboratory
-
Sudden decrease of the hematocrit
Imaging
-
Magnetic resonance imaging (MRI) is better than CT for detecting hemorrhagic pancreatitis because the signal intensity changes of hemorrhage on MRI can be sustained for an extended time and have different MR features of hemorrhage at various times.
-
CT findings
-
Intraparenchymal and/or peripancreatic collections with areas of high density on plain CT images
-
-
MRI findings
-
Intraparenchymal and/or peripancreatic spotted patchy threadlike or girdle-shaped hyperintensity on T1-weighted images with fat suppression
-
Treatment
-
Fluid resuscitation and blood transfusions
-
Arterial embolization (bleeding pseudoaneu-rysm)
14.5 Pancreatic Fistula (Figs. 14.64)


Pancreatic fistula associated with acute pancreatitis, diagnosis, and treatment. A 29-year-old male with history of alcoholic pancreatitis who developed ascites refractory to treatment. Analysis of the aspirated ascitic fluid showed an elevated amylase. CECT axial images (a, b) demonstrate the presence of massive ascites and a small fluid collection adjacent to the proximal body of the pancreas (arrow). This finding, along with the clinical and laboratory findings, suggests the possibility of a pancreatic fistula. An endoscopic retrograde cholangiopancreatogram (ERCP, c) demonstrates extravasation of the contrast media from the pancreatic duct in the proximal body of the pancreas (arrows) confirming the presence of a pancreatic fistula. A stent (d) was placed successfully under endoscopy guidance to bypass the disrupted pancreatic duct (arrow). Axial (e, f) images of a CECT performed 1 week later demonstrate a decrease in the amount of intraperitoneal fluid and a pancreatic stent in the main duct (arrows). Note the interval increase in size of the peripancreatic fluid collection (f) (arrowheads).Axial (g) and coronal (h) images from a follow-up CECT performed 4 months later demonstrate resolution of the intraperitoneal fluid as well the peripancreatic fluid collection. Note the pancreatic stent in place (arrows). The pancreatic stent was successfully removed 2 months later
-
Unusual complication of acute pancreatitis
-
Pancreatic fistulas develop secondary to a disruption of the main pancreatic duct, smaller ducts, pancreatic parenchyma, or rupture of a pancreatic pseudocyst.
Classification
-
Internal fistulas: peritoneal cavity, retroperitoneum, and pleural space
-
External fistulas: pancreaticocutaneous
Symptoms/Signs
-
Asymptomatic
-
Shortness of breath
-
Ascites
-
Early satiety and vomiting (collection compressing the stomach)
-
Abdominal or back pain
Clinical Suspicion
-
Ascites or pleural effusion refractory to treatment, enlarging fluid collection
Definitive Diagnosis
-
Detection of high levels of amylase in aspirated abdominal or pleural fluid
Best Imaging Modalities
-
ERCP/MRCP
ERCP findings
-
Extravasation of contrast from pancreatic duct
MRCP findings
-
Disruption of the pancreatic duct associated with intra- or peripancreatic fluid collections
Treatment
-
Somatostatin analogs (decrease the volume of fistula output and seem to aid fistula healing)
-
Endoscopic placement of pancreatic stent to bypass duct disruption
-
Total parenteral nutrition
-
Cystogastrostomy and cystenterostomy (surgical anastomosis to control the pancreatic leak)
-
Surgical resection
14.6 Venous Thrombosis/Occlusion (Figs. 14.32–14.34, 14.65–14.69)

Splenic and superior mesenteric thrombosis associated with acute pancreatitis on CT. A 49-year-old male with alcoholic pancreatitis. Incidental finding on imaging. CECT axial images (a, b) show mild inflammatory changes, fluid around the pancreas, and the presence of extensive low attenuation material in the splenic and superior mesenteric veins (arrows)

Portal vein thrombosis associated with acute pancreatitis on CT. A 55-year-old male with gallstone pancreatitis. Incidental finding on CT. CECT axial images (a, b) demonstrate a large thrombus in the main portal vein extending into the right portal vein (arrows)

Portal vein thrombosis associated with acute pancreatitis on CT. A 77-year-old female with idiopathic pancreatitis. Incidental finding on CT. CECT axial (a) and coronal (b) images reveal a large nonocclusive thrombus in the main portal vein (arrows)

Splenic vein occlusion associated with acute pancreatitis on CT. A 67-year-old male who presented with an episode of acute pancreatitis. CECT axial images (a–c) reveal a large complex collection involving the tail of the pancreas extending into the spleen (arrows) and mild peripancreatic inflammatory changes in the rest of the pancreas. Note the prominence of the short gastric veins, multiple venous collateral in the territory of the left gastric vein (arrowheads), and the lack of identification of the splenic vein

Splenic vein occlusion associated with necrotizing pancreatitis on CT. A 37-year-old male with history of alcoholic pancreatitis complaining of intense abdominal pain. CECT axial (a, b) and coronal (c) images show lack of contrast enhancement in the body and tail of the pancreas associated with peripancreatic inflammatory changes. Note the absence of the splenic vein (arrows) and the presence of prominent short gastric veins (arrowhead)
-
Venous thrombosis or occlusion is not a rare condition in acute pancreatitis.
These complications are more common in:
-
Alcohol induced, necrotizing, and chronic pancreatitis
Venous structures most commonly involved (in order of frequency: separately or in combination):
-
Splenic vein
-
Portal vein
-
Superior mesenteric vein
Pathogenesis
-
Stasis, spasm, mass effect from surrounding pancreatic inflammation, and direct damage of the venous wall by liberated enzymes
Clinical Manifestations
-
Often an incidental finding on imaging
-
Upper GI bleeding
-
Liver failure
-
Hypersplenism
-
Small bowel ischemia
-
Ascites
Best Imaging Modality
-
Doppler US and CECT
Findings
-
Absence of flow in the vein(s) involved
-
Partial or complete venous intraluminal filling defect in vein(s) involved (partial thrombosis)
-
Lack of identification of the splenic vein associated with multiple local venous collaterals is diagnostic of splenic vein thrombosis.
Treatment
-
Conservative
-
The use of anticoagulants is controversial.
Practical Pearls
-
Splenic vein thrombosis can lead to gastric varices that can bleed.
-
If the patient is very ill, treatment is usually a splenectomy or embolization of the splenic artery.
14.7 Pseudoaneurysms (Figs. 14.70–14.71)

Splenic artery pseudoaneurysm associated with acute interstitial pancreatitis on CT. A 71-year-old male with history of alcoholic pancreatitis and respiratory failure. CECT axial images (a, b) demonstrate diffuse enlargement of the pancreas and a small pseudoaneurysm in the tail of the pancreas (arrows)

Splenic artery pseudoaneurysm associated with acute pancreatitis on CT. A 55-year-old male with history of multiple attacks of pancreatitis. CECT axial images (a, b) display a round focal area of contrast enhancement similar to the abdominal aorta (arrowhead) within a large collection in the tail of the pancreas (arrows). Finding consistent with a pseudoaneurysm of the splenic artery

Splenic artery pseudoaneurysm associated with acute pancreatitis. A 50-year-old male with history of alcoholic pancreatitis, complicated by a pseudocyst. Patient went to an outside facility with increased abdominal pain and was found to have evidence of hemorrhage into the pseudocyst. Patient was referred to the interventional radiology service for diagnostic visceral angiogram and possible embolization of splenic artery. Axial image (a) from CECT initially done at outside institution reveals a small area of low attenuation in the tail of the pancreas (arrow) associated with mild peripancreatic inflammatory changes. In the follow-up CECT (b–c) performed 4 weeks later, axial images reveal a large collection with high density in the tail of the pancreas extending into the lesser sac (arrows). Finding suggestive of acute hemorrhage into the known pancreatic pseudocyst. A selective angiogram of the splenic artery performed the same day (d) shows a small pseudoaneurysm of the splenic artery in the body of the pancreas (arrow). This pseudoaneurysm was successfully treated with multiple endovascular coils (e) (arrow)
-
Rare complication of acute pancreatitis
-
More common in chronic pancreatitis.
-
Most frequently associated with pseudocysts.
-
Rupture of pseudoaneurysm is rare; however, the mortality rate is high when it occurs.
Pathogenesis
-
Autodigestion of the arterial walls by the pancreatic enzymes
-
Direct damage from severe inflammation
-
Vascular wall erosion from pancreatic enzymes within the pseudocyst or direct vascular compression or ischemia
Most common arteries involved in order of frequency:
-
Splenic
-
Gastroduodenal
-
Pancreaticoduodenal
-
Gastric
-
Hepatic
Clinical Features
-
Unexplained gastrointestinal bleeding
-
Sudden expansion of a pseudocyst
-
Unexplained drop in hematocrit
-
Incidental finding on imaging
Best Imaging Modality
-
Direct catheter angiography (allows imaging of small vessels and concomitant treatment)
Angiography and CECT Criteria
-
Round or ovoid structure with contrast enhancement pattern (similar to the aorta) within a pancreatic pseudocyst or adjacent to a pancreatic or peripancreatic artery
Treatment of Choice
-
Selective coil embolization under angiographic guidance
Options
-
Thrombin embolization
-
Endovascular grafts
-
Simple ligation
Practical Pearl
-
In those rare patients where it is difficult to catheterize the artery involved, the alternative is to access the artery percutaneously for treatment with vascular coils or direct thrombin injection.
14.8 Gastric or Bowel Obstruction
(Refer to: Chapter 16 , Fig . 16.46)
-
Rare complication of acute pancreatitis
-
Secondary to the compression of the stomach, small bowel, or colon by a pancreatic fluid collection, pseudocyst, or by the peripancreatic inflammatory process
Clinical Manifestations
-
Nausea
-
Vomiting
-
Early satiety
-
Abdominal distention
Best Imaging Modality
-
CECT
CECT Criteria
-
Obstruction of the stomach, small bowel, or colon by a pancreatic/peripancreatic collection or by an inflammatory process
Treatment
-
Percutaneous or endoscopic decompression of fluid collection/s, nasogastric tube
14.9 Biliary Tract Obstruction
-
Rare complication of acute pancreatitis
-
Secondary to the compression of the common bile duct by acute pancreatic fluid collection or pseudocyst
-
More commonly associated with chronic pancreatitis
Clinical Manifestations
-
Jaundice
-
Vomiting
-
Fever, chills, and leukocytosis (acute cholangitis)
Best Imaging Modality
-
CECT/MRCP
CECT Criteria
-
Dilatation of the biliary system secondary to a compression of the common bile duct by pancreatic collection or by a pseudocyst
Treatment
-
Percutaneous or endoscopic decompression of the pancreatic fluid collection or pseudocyst.
15 Teaching Points
ACUTE pancreatitis | |
|---|---|
Classification | Acute interstitial edematous pancreatitis (AIEP) 85 % Necrotizing pancreatitis (NP), (15 %) |
Etiology | Gallstones, alcohol 80 % Others 20 % |
Clinical presentation | Acute onset of abdominal pain Nausea and vomiting Severe: fever, hypoxemia, hypotension |
Laboratory evaluation | Elevation of the serum amylase and lipase Leukocytosis, elevated hematocrit (hemoconcentration) |
Phases of acute pancreatitis | Early: SIRS 10–20 % Late: CARS (bacterial translocation) |
Severity of acute pancreatitis Atlanta classification | Mild Moderate to severe Severe |
Scoring systems | Bedside index (first 24 h) Harmless Acute Pancreatitis Score APACHE II Modified CT Severity Index |
Imaging | Preferred imaging modality: CECT AIP: homogeneous or heterogeneous enhancement of pancreatic parenchyma associated with peripancreatic inflammation NP: lack of enhancement of the pancreatic parenchyma Infected: gas bubbles in pancreatic or peripancreatic tissue |
Treatment | Aggressive IV fluid replacement Nutritional support (enteral feeding) Management of the complications Organ dysfunction: pressor agents, assisted ventilation, renal dialysis Infected necrosis: surgical debridement or percutaneous external lavage |
Complications of acute pancreatitis | Peripancreatic fluid collections Pancreatic pseudocyst Pancreatic abscess Hemorrhagic pancreatitis Pancreatic fistulas Venous thrombosis/occlusion Pseudoaneurysms Gastric or bowel obstruction Biliary tract obstruction |
Treatment of complications of acute pancreatitis | Peripancreatic fluid collections: observation or drainage (symptomatic) Pancreatic pseudocyst: observation or drainage (symptomatic) Pancreatic abscess: percutaneous or endoscopic drainage and antibiotics Hemorrhagic pancreatitis: fluid resuscitation, blood transfusion, arterial embolization (acute arterial bleeding) Venous thrombosis/occlusion: controversial, anticoagulants Pseudoaneurysm: coil embolization Gastric or bowel obstruction: percutaneous or endoscopic drainage of fluid collection/s, nasogastric tube Biliary tract obstruction: percutaneous or endoscopic drainage of the pancreatic fluid collection or pseudocyst |
Recommended References
Balthazar EJ. Acute pancreatitis: assessment of severity with clinical and CT evaluation. Radiology. 2002;223(3):603–13.
Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–11.
Matos C, Cappeliez O, Winant C, Coppens E, Deviere J, Metens T. MR imaging of the pancreas: a pictorial tour. Radiographics. 2002;22(1):e2.
Morgan DE. Imaging of acute pancreatitis and its complications. Clin Gastroenterol Hepatol. 2008;6(10):1077–85.
Mortele KJ, Wiesner W, Intriere L, et al. A modified CT severity index for evaluating acute pancreatitis: Improved correlation with patient outcome. AJR Am J Roentgenol. 2004;183(5):1261–5.
Predicting the severity of acute pancreatitis. 2014. http://www.uptodate.com/contents/predicting-the-severity-of-acute-pancreatitis. Accessed 8 July 2014.
Sandrasegaran K, Tann M, Jennings SG, et al. Disconnection of the pancreatic duct: An important but overlooked complication of severe acute pancreatitis. Radiographics. 2007;27(5):1389–400.
Sleeman D, Levi DM, Cheung MC, et al. Percutaneous lavage as primary treatment for infected pancreatic necrosis. J Am Coll Surg. 2011;212(4):748–52; discussion 752–4.
Thoeni RF. The revised atlanta classification of acute pancreatitis: its importance for the radiologist and its effect on treatment. Radiology. 2012;262(3):751–64.
Urban BA, Fishman EK. Tailored helical CT evaluation of acute abdomen. Radiographics. 2000;20(3):725–49.
Wu BU, Banks PA. Clinical management of patients with acute pancreatitis. Gastroenterology. 2013;144(6):1272–81.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2016 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Casillas, J., Sleeman, D., Ahualli, J., Ruiz-Cordero, R., Echenique, A. (2016). Acute Pancreatitis (AP). In: Multidisciplinary Teaching Atlas of the Pancreas. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-46745-9_14
Download citation
DOI: https://doi.org/10.1007/978-3-662-46745-9_14
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-46744-2
Online ISBN: 978-3-662-46745-9
eBook Packages: MedicineMedicine (R0)