
Abstract
For interpretation of routine posteroanterior (PA) chest radiographs, the anatomy of the trachea, mediastinum, diaphragm, lungs, lung fissures, lung hila, other soft tissue structures and bony structures should be understood (Fig. 19.1). Important anatomic and imaging criteria for each of these structures will be discussed in this chapter.
The normal trachea appears in the PA chest radiograph in the midline. The aortic arch causes slight deviation of the trachea to the right side. This shift is more marked in an expiratory film, due to shortening of the trachea. The transparency of the tracheal lumen normally decreases from cranial to caudal. The maximal width of the trachea is 25 mm (for men) and 21 mm (for women). The right tracheal border, where the trachea is in direct contact with lung tissue, can be traced from the clavicle to the right main bronchus. This border is referred to as the right paratracheal stripe or line and is visible in up to 60% of patients. Its width is normally less than 4 mm. A left paratracheal stripe is generally not visible, because the left tracheal border is in direct contact with the large vessels rather than lung tissue.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others



Keywords
- Lung Parenchyma
- Bronchial Wall
- Bronchogenic Cyst
- Allergic Bronchopulmonary Aspergillosis
- Interlobular Septum
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Normal Anatomy
For interpretation of routine posteroanterior (PA) chest radiographs, the anatomy of the trachea, mediastinum, diaphragm, lungs, lung fissures, lung hila, other soft tissue structures and bony structures should be understood (Fig. 19.1). Important anatomic and imaging criteria for each of these structures will be discussed in this chapter.

Normal anatomy. a Chest X-ray posteroanterior view. 1 Trachea, 2 right main bronchus, 3 left main bronchus, 4 scapula, 5 clavicle, 6 manubrium sterni, 7 azygous vein, 8 aortic arch, 9 left pulmonary artery, 10 left atrium, 11 left ventricle, 12 right atrium, 13 right lower lobe pulmonary artery, 14 lateral costophrenic recess, 15 breast shadow. b Chest X-ray lateral view. 1 Trachea, 2 pretracheal vessels, 3 aortic arch, 4 right upper lobe bronchus, 5 left upper lobe bronchus, 6 left pulmonary artery, 7 right pulmonary artery, 8 scapula, 9 left dorsal costophrenic recess, 10 right dorsal costophrenic recess, 11 stomach, 12 inferior vena cava
1 Trachea and Bronchial Tree
The normal trachea appears in the PA chest radiograph in the midline. The aortic arch causes slight deviation of the trachea to the right side. This shift is more marked in an expiratory film, due to shortening of the trachea. The transparency of the tracheal lumen normally decreases from cranial to caudal. The maximal width of the trachea is 25 mm (for men) and 21 mm (for women). The right tracheal border, where the trachea is in direct contact with lung tissue, can be traced from the clavicle to the right main bronchus. This border is referred to as the right paratracheal stripe or line and is visible in up to 60% of patients. Its width is normally less than 4 mm. A left paratracheal stripe is generally not visible, because the left tracheal border is in direct contact with the large vessels rather than lung tissue.
The trachea is formed of u-shaped cartilaginous rings anteriorly, which are confined posteriorly by an elastic membranous part. The trachea divides at about the level of the 4th thoracic vertebral body (Figs. 19.2 and 19.3). The right main bronchus is steeper than the left. The normal bifurcation angle of the carina is 60–75°. Widening of the bifurcation angle may result from an enlarged left atrium or enlarged carinal lymph nodes.

Normal anatomy of the trachea and bronchial tree (frontal representation of the bronchial tree)

Bronchial divisions. Upper: segmental anatomy of the lungs as viewed from anterior. Lower: segmental anatomy of the lungs as viewed from medial. Lobar boundaries: thick lines; segmental boundaries: thin lines
The right main bronchus divides into three lobar branches for each of the upper, middle, and lower lung lobes. The right upper lobe bronchus gives rise to the (1) apical, (2) posterior, and (3) anterior segments. The bronchus intermedius divides into the middle and lower lobe bronchi. The middle lobe bronchus then bifurcates into (4) lateral and (5) medial segmental bronchi. The lower lobe bronchus divides into (6) apical, (7) paracardiac, (8) anterior basal, (9) lateral basal, and (10) posterior basal segmental bronchi. The left-sided branching is more or less similar. The main bronchus runs about 4 cm from the carina, and then divides into upper and lower lobar bronchi, which in turn divide into segmental branches. The upper lobe gives rise to the (1, 2) apicoposterior and (3) anterior segmental bronchi. The (4) superior and (5) inferior segmental bronchi of the lingula branch off from the upper lobe bronchus. The lower lobe bronchus divides into (6) apical, (8) anterior basal, (9) lateral basal, and (10) posterior basal segmental bronchi.
Bronchial segmentation is of great importance because lung segments are separate functional units. Many diseases are therefore related to individual segments (Table 19.1) (Fig. 19.4).

Schematic representation of cross-sectional segmental lung anatomy
The main imaging findings for the evaluation of the trachea include:
-
Narrowing
-
Tracheal shift (Fig. 19.5)
Fig. 19.5 
Deviation of the trachea to the right side. Chest X-ray posteroanterior view
-
Intraluminal lesions

1 Azygous Vein
The azygous vein is located between the right main bronchus and the trachea. Its normal calibre is ≤ 10 mm, and decreases with Valsalva manoeuvre or during inspiration. Enlargement of the azygous vein is seen with a supine position, or associated with subcarinal lymph node enlargement, pregnancy, portal hypertension, obstruction of the superior or inferior vena cava, right heart failure, and constrictive pericarditis.
1 Mediastinum/Heart
In a normal chest radiograph, the central opacity is formed by the heart, mediastinum, the great vessels, and the sternum. With good centralisation, two-thirds of the cardiac shadow is seen to the left of the midline and one-third to the right, although this is highly variable. The transversal cardiac diameter is < 14.5 cm for females and < 15.5 cm for males.
Enlargement of the cardiac shadow > 1.5 cm in transverse diameter is considered significant.
An apparent enlargement of the cardiac shadow is caused by a short film-focus distance, by a film taken during expiration, as well as by a supine position. The borders of the heart and mediastinum are normally sharply demarcated down to the contact point between the heart and the left diaphragm.
The upper mediastinum begins at the thoracic inlet and ends about the level of the junction of the manubrium–body of the sternum, around the level of the 4th thoracic vertebra. Below this level, the mediastinum is divided into anterior, middle, and posterior divisions.
-
The anterior mediastinum lies between the posterior surface of the sternum and the anterior pericardium. It contains the ascending aorta, superior vena cava, azygous vein, and the thymus gland.
-
The middle mediastinum contains the heart, the great vessels, and the trachea.
-
The posterior mediastinum is bordered by the chest wall and includes the descending aorta, oesophagus, vagus nerve, thoracic duct, and the sympathetic chain.
The mediastinal lymph nodes are divided into visceral and parietal groups. The parietal lymph nodes are the parasternal and diaphragmatic lymph nodes. The rest belong to the visceral group. Lymphatic drainage from the lung, oesophagus, trachea, and thymus is via the paratracheal lymph nodes. The parasternal lymph nodes drain the pleura and chest wall, including the breasts.
Criteria for Delimitation of Cardiac Borders.
The cardiac borders are formed by several structures (Fig. 19.6). The left cardiac border is formed from cranial to caudal by the subclavian artery and vein, aortic arch, descending aorta, pulmonary trunk, left atrial appendage, and left ventricle. In old age, the aorta also contributes to the left border. The right cardiac border is formed by the superior vena cava, azygous vein, the right atrium, and the inferior vena cava. In old age, the aortic arch becomes more elongated and dilated and also contributes to the right border.

Normal anatomy of the mediastinum and heart. a Graphic representation of the mediastinum in sagittal view. b Cardiac borders in the posteroanterior view. c Cardiac borders in the lateral view
1 Mediastinal Lines
Mediastinal lines are areas of contact between the mediastinum and lung (Figs. 19.7–19.13). They are visible on chest radiography when they are tangential to the X-ray beam. A visible shift of these lines may be indicative of a space-occupying lesion of the corresponding mediastinal compartment.

Normal anatomy in the chest X-ray: mediastinal lines

Chest X-ray posteroanterior view. Prominent mediastinal lines (arrows), in a case with provisional diagnosis of lymphoma

Mediastinal lymphoma with right paratracheal lymph nodes. Chest X-ray posteroanterior view (arrows)

Aneurysm of the brachiocephalic trunk. Chest X-ray lateral view shows poor definition of the borders of the proximal aortic arch (arrows)

Enlarged lymph nodes. a Chest X-ray posteroanterior view. b Chest X-ray lateral view shows a widened mediastinum in a patient with sarcoidosis, due to enlarged paratracheal and other mediastinal lymph nodes (arrows)

Chest X-ray posteroanterior view. A known case of central bronchial carcinoma in the left hilum after treatment

Mediastinal lymphoma. Axial CT image in soft tissue window shows lymphoma tissue in the mediastinum causing displacement of anatomic structures
The posterior junction line is formed by the apposition of the visceral and parietal pleura of the posteromedial portion of the upper lobes posterior to the oesophagus and anterior to the third to fifth thoracic vertebrae.
The subclavian-heart line is the counterpart of the posterior junction line, and is also called the anterior junction line (Table 19.2). It is formed by the apposition of anterior visceral and parietal pleura, appearing as a y-shaped line running from the upper sternum down to the heart.
The right paratracheal stripe is up to 4 mm wide (Fig. 19.9). The thin para-aortic line runs longitudinally, lateral to the descending aorta. The azygoesophageal recess extends from the level of the anterior turn of the azygous vein to the level of the aortic hiatus inferiorly, with a mild leftward convexity superiorly and a straight edge inferiorly.
The paraspinal lines are vertical lines extending on both sides of the spine, formed by the layers of the pleura, separating the posterior lung tissue from the paravertebral muscles. The left paraspinal line is < 10 mm wide, and the right < 3 mm. Lateral displacement results from osteophytes, elongated aorta or aneurysm, dilated azygous, and vertebral or paraspinal soft tissue masses (e.g., abscess, lymph nodes, extramedullary haematopoiesis, etc.).
The pleuro-esophageal line is formed by the right wall of the oesophagus, extending from the lung apex to the azygous. It is only visible with an air-filled oesophagus. Normally, the left wall of the oesophagus is not visible.
The retrotracheal line can be visualised in the lateral chest view and is formed by the pleural folds posterior to the trachea. When its width exceeds 4 mm, a mass lesion is suspected.
The retrosternal pleural stripe is also seen in the lateral view; and is formed by the anterior pleural folds and runs downwards, posterior to the manubrium and body of the sternum. The cranial portion is wider, because the brachiocephalic vein lies between the lung and sternum. Caudally it gradually narrows.
In the chest radiograph of children and adolescents, the thymus gland appears as a triangular, sail-shaped structure with sharp borders on both sides of the mediastinum. The right wall is straighter than the left, and is more likely to visualise. The size of the thymus is reduced during inspiration as well as in response to stress disorders. In DiGeorge syndrome, the thymus is not formed. An enlargement of the thymus is often seen in the convalescence phase as well as in adolescent boys.
1 Diaphragm
During inspiration, the dome of the diaphragm is at the level of the 6th rib anteriorly and the 10th rib posteriorly. In the supine position the diaphragm is higher. With expiration, the diaphragm is displaced upwards about 2 intercostal spaces. The upper border of the diaphragm is sharply defined, except for the part of the left diaphragm where the heart is in direct contact with the diaphragm.
Normally, the right diaphragmatic cupola is higher than the left (Fig. 19.14). In about 3% of cases only, the left diaphragmatic cupola is higher than the right one.

Radiographic morphology of the diaphragmatic cupola
A difference between the diaphragmatic cupolas of > 3 cm is considered significant. This may be caused by distension of the stomach or the splenic flexure of the colon.
After exclusion of insufficient inspiratory effort, bilateral elevation of the diaphragm may be caused by the following conditions: bilateral atelectasis, extensive pulmonary fibrosis, subphrenic effusion, or subphrenic causes such as abdominal tumours, pregnancy, massive ascites, hepatosplenomegaly, and obesity.
Causes of focal bulge of the diaphragm are:
-
Subphrenic effusion
-
Liver tumour (abscess, metastasis)
-
Postpneumonic scarring
-
Diaphragmatic hernia
-
Pericardial Fat
1 Lung Fissures
Lung fissures are formed of the adjacent layers of the visceral pleura and they are visible on the chest radiograph only if they are tangential to the X-ray beam. Interlobar fissures separate the lung lobes. The main fissure separates the upper and lower lobes and runs from posterior to anterior starting posteriorly opposite the 5th dorsal vertebral body. Because of its oblique course, it is rarely seen in the PA view.
The right middle lobe is separated from the upper lobe by the horizontal fissure (Fig. 19.19). Accessory fissures can be present such as the superior and inferior accessory fissures. The superior accessory fissure separates the apical lower lobe segment from the remaining lower lobe. The inferior accessory fissure separates the medial basal segment from the remaining lower lobe segments, so it may be called the accessory cardiac lobe. The azygous fissure is an accessory fissure seen in the right upper lung lobe (. Fig. 19.18 ).

Para-aortic lesion. a Chest X-ray posteroanterior view. Opacity projected through the heart shadow. b Lateral view. c Axial CT in lung window showing fat lesion. A: descending aorta; H: posterior mediastinum

Schematic representation of the evolution of the azygous lobe

Schematic representation of major and accessory lung fissures. a Right lung anterior view. b Right lung lateral view. c Left lung lateral view

Azygous lobe fissure. Chest X-ray posteroanterior view shows the azygous lobe fissure as a thin right paramediastinal line (arrows)

Lung fissures. Chest X-ray lateral view shows the major fissure (arrows) and the horizontal fissure (arrowheads)
1 Lung Parenchyma
1 Anatomy of the Lung Parenchyma
Structure of the pulmonary interstitium:
-
Peripheral interstitial compartment:
-
Subpleural connective tissue
-
Peripheral interlobular septa with veins and lymphatics
-
-
Axial interstitial compartment:
-
Surrounding and supporting the bronchovascular bundles
-
-
Parenchymal interstitial compartment:
-
Supporting the inner lumen of the lobules between the acini
-
The basic structure of the lung parenchyma is the broncho-vascular bundle. This refers to the following structures:
-
The pulmonary artery
-
The bronchiole
-
The surrounding connective tissue of the basement membrane of the alveoli
-
The subpleural connective tissue
-
The interlobular and interlobar septa with pulmonary veins and lymphatics
Histologically, the alveoli consist of alveolar epithelium, capillaries, and interstitial connective tissue. The epithelium is in direct contact with the endothelium of the vessels, which permits diffusion of oxygen and carbon dioxide. Pneumocytes in the alveoli are responsible for the secretion of the surfactant, which reduces the surface tension of the alveoli thus preventing their collapse.
The next larger functional unit is the primary lobule. This consists of the lung parts that are supplied by a respiratory bronchiole. These include alveolar ducts, alveolar sacs, and associated alveoli.
The acinus is lung parenchyma distal to a terminal bronchiole.
The secondary lobule is formed of about 4 or more acini. It could be regarded as the smallest unit of lung structure surrounded by connective tissue. It contains, on average, 40 primary lobules. The diameter of the secondary lobule is about 10 mm. The secondary lobule is supplied by a lobular bronchiole that is further divided into the terminal and respiratory bronchioles and the acini.
1 Imaging of Lung Parenchyma
Interpretation of the lung parenchyma on chest radiography is made difficult by the superimposition of vessels, bone, and cartilage on the lung fields. In the apex of the lung, there is even more difficulty due to the superimposition of soft tissues and the clavicles.
Thin-section high-resolution CT enables visualisation of the secondary lobule. It can be thought of as having three primary components: the interlobular septa, the centrilobular region, and the lobular parenchyma.
1 The Lung Hila
Adequate evaluation of the lung hila is crucial on chest radiography. Unfortunately, this is complicated by the superimposition of vessels and bronchi on each other.
In 97% of cases, the left hilum is higher than the right, and in 3% they are almost at the same level. The hila should have the same density and should appear concave laterally.
The structure of the hilum is mainly formed by the pulmonary arteries and superior pulmonary veins. The identification of each vascular structure is important so that any other opacity can be carefully reviewed. Comparison with previous radiographs may be helpful.
Normal, nonenlarged hilar lymph nodes are not visualised. The normal bronchial walls are only visible when they are imaged end on, and appear as a ring-like structure. The anterior segment of the upper lobe bronchus is seen in 45% of cases on the right, and in 50% on the left side. The width of the soft tissue lateral to the bronchus should be < 5 mm, and abnormal thickening may be a sign of underlying malignancy.
1 Pulmonary and Bronchial Vessels
The left pulmonary artery is anatomically located above the left main bronchus (Fig. 19.22). The right pulmonary artery passes anterior to the bronchus.

Schematic representation of two adjacent secondary lobules

Schematic representation of alveolar walls

Schematic representation of the trachea and mediastinal vessels. a Posterior view. b Oblique superior view
The hila are highly variable in size. The maximum diameter of the descending branch of the right pulmonary artery in an adult male is 16 mm, while it is 15 mm in an adult female.
The superior pulmonary vein is lateral to the artery, and is separated from the mediastinum by a 1-cm wide stripe of lung parenchyma. At the level of the first intercostal space, the normal vessel diameter should not exceed 3 mm.
In the upright position, the vessels of the lower lobe are relatively larger compared to those of the upper lobe due to the reduction of perfusion and ventilation. In the supine position, upper and lower lobe vessels are similar in size. The right pericardiac vessels are usually prominent.
Peripheral lung markings are mainly determined by the visibility of vascular structures. Veins and arteries cannot be differentiated reliably from each other because of their similar density and course. However, pulmonary veins typically have fewer branches than arteries, are straighter, bigger and less sharply demarcated. Pulmonary arteries accompany the bronchi, lying posterior and superior. Veins do not follow the bronchi, but run in the interlobular septa. The veins combine to form the superior and inferior pulmonary veins, which empties directly in the left atrium. The site of venous drainage is sometimes seen as a rounded structure to the right of the midline, partly projected on the heart.
The bronchial arteries have variable anatomy; they usually arise from the anterior aspect of the descending aorta opposite the level of the fifth and sixth dorsal vertebrae. In general, there are two branches, one on the left and one on the right, which often share a common origin with an intercostal artery.
When the bronchial arteries enter the hila, they accompany the bronchi. Bronchial veins drain into pulmonary veins, and rarely into the azygous vein.
Normally, bronchial arteries and veins are not visible on a chest radiograph. Enlarged bronchial arteries are seen as multiple small nodules along the hilum and short lines extending into the proximal lung fields. Dilatation of bronchial vessels may be caused by cyanotic heart disease or localised dilatation due to a pulmonary lesion, such as bronchial cancer.
1 The Lymphatic System
The role of the lymphatic system of the lungs is to transport interstitial fluid and foreign material. They run in the interlobular septa, and are connected to the subpleural lymphatic channels and finally drain into the deep lymphatic system in the lung hilum.
Lymphatic channels are normally not visible in conventional radiographs. They can only be seen when the lymphatic vessels are thickened. Thickened lymphatics together with thickened surrounding connective tissue appear on a chest radiograph as what is called Kerley lines. Kerley lines may be transient or persistent.
Intrapulmonary lymphatics drain directly into the broncho-pulmonary lymph nodes (Table 19.3). A small number of intrapulmonary lymph nodes may be visualised on contrast-enhanced CT. The anterior mediastinal nodes at the level of the aortic arch drain the thymus and right heart. The intrapulmonary lymph nodes are located along the main bronchi. The middle mediastinal lymph nodes drain the lungs, bronchi, left heart, trachea, and visceral pleura.
2 Imaging Techniques
Radiologic investigations of the chest represent more than 50% of all radiologic examinations. The chest radiograph is the most widely used imaging modality for routine evaluation of the chest. More advanced modalities such as CT, MRI and echo-cardiography are increasingly being used nowadays for the diagnosis of cardiac, great vessel, mediastinal, and bronchial pathologies.
The previously used imaging technique of bronchography is now rarely used. The use of sonography is essentially limited to evaluating the chest wall, the diaphragm, and pleural fluid collections.
CT is nowadays the standard imaging modality for further evaluation of thoracic diseases, particularly multidetector CT (MDCT). It is commonly used for assessment of lung disorders as well as the mediastinal structures. Improvements in the technique of CT angiography (CTA) have led to replacement of the majority of the indications for conventional angiography (DSA).
The applications of MRI in the chest include the thoracic inlet, the chest wall, and the diaphragm. MR angiography (MRA) may also be used in the chest. Echocardiography plays an important role in the diagnosis of cardiac diseases as well as in acute aortic dissection and some other diseases.
Radioactive isotope techniques such as lung ventilation and perfusion scans are now replaced in most instances by CT. The role of positron emission tomography (PET) is growing for diagnosis and staging of lung cancer and mediastinal tumours.
2 Projection Radiography
The purpose of projection radiography is to assess the thoracic organs. The basic guidelines of chest radiography are presented below, as well as the limitations such as the superimposition of structures and the poor sensitivity to small differences in density between structures. Technical improvements and the use of digital radiography systems are also discussed.
2 Posteroanterior (PA) radiograph
Position of the Patient.
Adequate patient positioning is crucial. The patient should stand facing the cassette holder with the thoracic organs as close as possible to the cassette holder and the shoulders rotated inwards and pressed against the cassette holder so that the patients’ arms and hips are touching the cassette holder (. Fig. 19.23 ).

Patient positioning for chest X-ray posteroanterior view. Note: The X-ray film should be exposed in such a way that the final acquisition is viewed as a mirror image
Exposure Technique.
For the PA radiograph, the exposure time should be very short < 20 ms and the focus at a distance of typically 180 cm. The tube voltage is usually between 125–150 kV. In general, a moving grid is used to reduce the scattered radiation at a ratio of at least 10:1. Centring is on the 6th thoracic vertebra.
In many instances the PA and lateral chest radiographs are both obtained and interpreted together. In patients under follow-up, only the PA film is obtained.
Indications for PA chest radiograph
-
Diagnosis of pulmonary disease
-
Determination of heart size and/or configuration
-
Follow-up of known inflammatory, neoplastic, or vascular disease
-
Preventive investigation: preoperative, medical staff screening or after T.B. exposure
2 Additional Techniques
In addition to the routine chest PA, the following techniques are used:
-
Expiratory film: a film taken in forced expiration for diagnosis of suspected pneumothorax, as well as for the diagnosis of bronchial obstruction and air trapping
-
Lordotic view: Improves visibility of changes in the lung apices. Nowadays, is largely replaced by CT
-
Bony thorax: fewer hard rays (70 kV) for the best contrast of bony structures, especially of the ribs
2 Lateral Chest Radiograph
Position of the Patient.
The patient stands with his side near the cassette holder with arms raised above the head.
Exposure Technique.
The exposure time should be < 40 ms.
2 Supine Chest Radiograph
Position of the Patient.
The exposure is carried out with the patient in a half-sitting or lying position.
Exposure Technique.
The focal-film distance should be 1 to 1.25 m, or as large as possible. The tube voltage should be between 80–100 kV, and the focal spot size ≤ 1.3 mm.
Indications for supine chest radiograph
-
General: bed-ridden patients who cannot stand up or sit upright away from the bed
-
Intensive medical care control scans for cardiovascular and pulmonary diseases
-
After use of a mechanical ventilation tube or central venous catheter
-
After placement of a chest tube
Special features of supine film are:
-
Diaphragm is higher on both sides than in the upright position
-
Heart: increase in size of the cardiac shadow
-
Restricted assessment of heart size (only possible on follow-up examinations)
-
Widened mediastinum
-
Increased perfusion of the upper lung lobes (baso-apical redistribution of blood)
-
Dilation of upper lobe vessels
-
Pneumothorax is often difficult to diagnose, suggested by a sharp heart border, deep sulcus, or minimal increased transparency
-
Pleural effusions do not form a border, but only a homogeneous opacity declining from basal to cephalic
2 Chest Radiography in Children
Technical factors for chest radiography in children according to age are listed in Table 19.4. As for adult radiography, the following points should be applied:
-
Shortest possible exposure time (in infants the optimal exposure time < 4 ms, closer to 1 ms)
-
Optimisation of focus and total filtration, grid application, and fast-film screen combination
-
Additional filtration of 3.0 mm aluminum equivalent for protection of all organs of the newborn such as thyroid, breast, thymus, and skin glands that lie in the path of the radiation
-
Anti-scatter grid is not used in infants due to the small body volume
-
Grid is used in children from body weight 25 kg depending on body height and anteroposterior chest diameter > 12 cm
2 Screen-Film Radiography
2 Technical Aspects
Conventional radiography is based on the screen-film combination. The X-ray is converted by the intensifying screens into light, which in turn exposes the film. Taking into account the wide contrast range of thoracic structures, screens with a sensitivity class of 200 or better 400 should be used for chest radiography. Currently, the resolution achieved by a screen-film combination of sensitivity class 400 is 2.4 line pairs per millimetre (lp/mm). Radiographic films have characteristic curves that describe the detector. The curves are generally S-shaped.
The dynamic range in chest radiography is high, because the lung absorbs only a small amount of radiation, resulting in a high detector dose. In the mediastinum, the absorption of radiation is high, resulting in a low detector dose. Overall, the ratio between the radiation absorption of the highest density structures of the mediastinum and the lungs is about 1:100, thus exceeding the dynamic range of the system. As a solution, asymmetric screen-film combinations are used.
2 Computed Radiography (CR)
2 Technical Aspects
The basic techniques which can be used for acquisition of digital radiographic images are presented below.
Computed Radiography (CR) is the most common technique for acquisition of digitalised radiographs. A cassette filled with detector material is used instead of the conventional film-screen combination. The detector plates often contain Barium fluoro bromide crystals doped with Europium.
Energy from X-ray photons falling on the detector plate is absorbed and thereby electrons are raised to higher energy levels. Electrons at higher energy levels have the X-ray information stored in the form of a latent image. After exposure, the cassette is read out in a dedicated unit by a scanning laser beam. The laser scanning, in a photo-electronic process, converts the latent image into a digital image. After completion of the read out process, the cassette is exposed to a strong light source so that all data are removed, and the cassette is then ready to be used again. The maximum achievable spatial resolution by CR with a pixel size of 200 n/m is 2 line pairs/mm, for flat-panel detectors it is between 2.5 to 3.5 line pairs/mm.
2 Digital Radiography (DR)
2 Technical Aspects
Digital radiography (DR) could be further divided into direct or indirect digital radiography according to the type of X-ray conversion.
Direct digital radiography needs special X-ray units. The energy of the X-ray photons is directly converted into an electric signal by a detector made of a photoconductive layer, mostly amorphous selenium.
Flat-panel detectors are clinically more useful since the detectors can be mounted in various X-ray stands and tables. In flat-panel detectors, the surface is primarily split into individual active pixels. Each pixel contains its own switching element which is able to convert the incoming X-rays into a proportional electric signal. The most common type of detector is the amorphous silicon detector which consists of a scintillator layer (such as cesium iodide) on top of a photodiode matrix (amorphous silicon). The X-ray energy is converted into visible light by the scintillator layer and the emitted light is then converted into an electric signal by means of the photodiode layer.
2 Fluoroscopy
Conventional X-ray fluoroscopy is rarely used for routine examination of the chest, and only in special situations (Table 19.5.):
-
In a case of unclear findings on the chest X-ray:
-
If CT is not available
-
If oblique or lordotic views do not provide adequate information
-
In follow-up of focal opacities > 5 mm
-
-
In inspiration and expiration using a low-dose technique for diagnosis of phrenic nerve palsy.
Causes of unilateral elevation of the diaphragm
-
Hepatomegaly
-
Meteorism
-
Reflex with subphrenic abscess
-
Phrenic nerve paralysis (e.g., by Pancoast tumour, iatrogenic)
-
Atelectasis
-
Hemiplegia
-
Trauma
-
Pleural disease such as empyema
-
Subpulmonary effusion
Ultrasonography.
Ultrasonography of the chest is limited by the presence of air and bone. According to the indication, ultrasound examination may be performed using ultrasound transducers between 3.5–10 MHz. Different access routes for ultrasound of the chest may be used including abdominal subcostal, intercostal, parasternal, and suprasternal, bypassing the lungs and ribs. For superficial lesions a 10-MHz transducer is commonly used.
Indications.
Ultrasonography of the chest is used to diagnose pleural effusion and may replace conventional radiography. Ultrasonography is also helpful for evaluation of chest wall lesions or localised pleural lesions and enables precise differentiation between solid and fluid lesions. Moreover, tube drain insertion and needle biopsies could be done with sonographic guidance.
2 Bronchography
Bronchography is the radiologic examination of the tracheo-bronchial tree after instillation of a positive contrast agent.
The bronchography procedure consists of:
-
1.
Bronchoscopy
-
2.
Insertion of bronchial catheter
-
3.
Application of iodised oil
-
4.
Chest radiography
Bronchography is no longer used, and is currently replaced by CT. With MDCT, a 3D reconstruction of the tracheo-bronchial system, a virtual bronchogram, could be obtained from axial data.
2 Computed Tomography (CT)
Further radiologic investigation of the chest and thoracic organs is performed by CT, optimally using multidetector computed tomography (MDCT). Techniques such as conventional tomography, angiography, and bronchography are largely replaced by CT. CT enables superimposition-free imaging of the lungs, pleura, hilum, and mediastinum.
Technique.
The patient lies supine and holds his breath during the examination. Normally, acquisition is in inspiration. In special cases, a complementary scan during expiration or in the prone position may be indicated. The arms should be elevated and removed from the scan region in order to avoid increasing the radiation dose and eliminate beam-hardening artifacts. The scan range is from the lowest point of the costophrenic angles up to the thoracic inlet. Intravenous administration of contrast medium enhances the differentiation of mediastinal structures and pulmonary vasculature and gives information about the vascularity of pathologic thoracic lesions. Intravenous contrast administration is also mandatory for CT angiography of coronary or pulmonary arteries. Because of the very wide range of densities of imaged structures (air: −1000 HU, bone +1000 HU), for optimum assessment of the lung and mediastinal structures, different window settings must be used.
2 Magnetic Resonance Imaging (MRI)
MRI has several advantages over other diagnostic imaging modalities including the multiplanar imaging capability in axial, sagittal and coronal orientations, the excellent soft tissue contrast, the noninvasive vascular imaging with the possibility of flow measurement as well as the lack of radiation exposure. Administration of contrast medium further increases the diagnostic performance. Other benefits include additional functional imaging including depiction of metabolites (MR spectroscopy), water molecule motion (MR diffusion), or evaluation of tissue vascularity (MR perfusion studies).
Disadvantages of MRI include the longer acquisition time compared to CT, which results in increased respiratory and motion artifacts such as cardiac activity. However, the duration of acquisition could be significantly shortened with new sequences and software advancement. Motion artifacts can be minimised by ECG or respiratory triggering. For examination of the chest, gradient sequences or new sequences with fast acquisition and the possibility of secondary reconstructions are used.
Several clinical applications of MRI make use of its ability for tissue differentiation including fatty tissue, muscle tissue, and pathologic tissue. MRI is the preferred modality for imaging of lesions of the chest wall, pleura, and the perivertebral space. Furthermore, it is sometimes used for evaluation of the mediastinum, vascular disorders including vascular anomalies, aneurysms, and for inflammatory diseases.
2 Perfusion Scintigraphy
Perfusion scintigraphy is used for the diagnosis or exclusion of pulmonary embolism. It entails the intravenous administration of radiolabelled macroaggregated albumin particles, which disperse as microemboli in the normally perfused lung parenchyma. The radioactivity emitted by the particles is received by a gamma camera in several positions. The distribution of the radioactivity permits qualitative and quantitative assessment of perfusion. Areas with reduced perfusion appear as persistent areas with absent radioactivity. A normal perfusion scan excludes a clinically relevant pulmonary embolism.
However, not every perfusion defect is due to pulmonary embolism, as hypoventilation also leads to reduced perfusion. Therefore, perfusion and ventilation scintigraphy are often combined. The typical pattern of pulmonary embolism on perfusion scintigraphy is a wedge-shaped peripheral perfusion defect.
Improvements in the resolution of multislice CT with faster image acquisition, have led to the increased replacement of perfusion scintigraphy by CT. Advantages of CT include direct imaging of the pulmonary arteries as well as the secondary changes in the lung fields. CT angiography may be used for planning of a possible interventional procedure such as catheter embolectomy.
2 Ventilation Scintigraphy
Ventilation scintigraphy is performed by inhalation of radioactive gases such as Xenon-133 or Technetium-99m aerosols and evaluation of their distribution. Hypoventilated areas show reduced or absent tracer uptake.
For the diagnosis of pulmonary embolism, the findings of the ventilation and the perfusion scintigraphy are evaluated together in addition to the chest radiograph. The diagnosis of pulmonary embolism is based on the finding of the so-called perfusion-ventilation miss-match. Affected areas have normal ventilation and decreased perfusion.
Indications for ventilation scintigraphy include respiratory disorders, whether restrictive or obstructive; bronchial stenosis, as well as the part played by ventilation scintigraphy in the diagnosis of pulmonary embolism as noted above. Acquisition of delayed images (after several hours) is helpful in assessing radioactive material removal, giving information about the activity of the mucociliary transport system.
Restrictive Lung Diseases
Restrictive lung diseases are characterised by reduced lung volume and reduced gas exchange leading to reduced total lung capacity and vital capacity. An increased respiratory activity becomes necessary for inspiration of sufficient amounts of air. At the same time, the cardiac pressure has to be increased, in order to pump the cardiac output through the pulmonary circulation. This leads to an increased right heart strain up to cardiac decompensation. Examples of restrictive lung diseases include lung fibrosis, atelectasis, partial pulmonary resection, pleural thickening, pneumothorax, and chest deformity with limited mobility.
2 Positron Emission Tomography (PET)
Positron-emitting radionuclides are injected into the patient and then integrated into normal metabolism. PET is based on the emission of a positron (β+) from the nucleus of the radionuclide, which then undergoes annihilation with an electron to produce two photons traveling in exactly opposite directions. These can then be detected by coincidence when they strike two detectors at the same time and hence can be localised.
PET is generally limited by poor spatial resolution, so the PET scanner is preferentially combined with a CT scanner housed in the same gantry. The patient is scanned by CT just before PET scanning. The two scans are combined by the software.
In imaging of the chest, diagnostic PET-CT is only indicated in staging of previously diagnosed lung tumours, in investigating an unexplained rise of tumour markers, or in follow-up after treatment. With PET-CT, it is possible to diagnose lymph node infiltration or tumours in atypical sites.
The tracer chosen for PET must not be metabolised in the plasma and should typically have adequate and selective receptor binding. Certain tumour characteristics should be noted to enable choosing the best tracer. Examples are the presence of receptors, whether there are specific antigens (e.g., CEA), the level of metabolic activity of tumour cells, and whether there are specific cell products (e.g., iodine).
F-18-fluorodeoxyglucose (FDG) is used for imaging of tumours with high glucose metabolism, for example; highly differentiated adenocarcinomas and squamous cell carcinomas, sarcomas, and lymphomas. A diagnostic pitfall may be caused by endocrine tumours. FDG is also suitable for detection of florid inflammations.
Advantages of PET include the differentiation between postoperative scarring and tumour recurrence. Tumours in atypical or anatomically complex sites as well as tumours otherwise hidden by postoperative artifact-producing materials can be clearly assessed with PET-CT.
3 Systematic Analysis of the Chest Radiograph
Interpretation of the chest X-ray should follow a systematised scheme:
-
1.
Visual control of image quality:
-
Compliance with European quality guidelines
-
Quality of the exposure with a sharp image of the vessels to the lung periphery, the hilum, heart border, and the diaphragm
-
Full coverage of the thoracic organs in inspiration (diaphragm at the level of at least the 8th rib)
-
Symmetry of the film with projection of the spinous process of the third thoracic vertebra at equal distances from the two sterno-clavicular joints
-
The clavicles should be projected on the 3rd ribs in order to exclude faulty angulation
-
-
2.
Verification of identity:
-
Name of the patient, date of birth, date of examination, and name of institution
-
-
3.
Morphologic analysis:
-
Transparency changes
-
Structural changes
-
Characteristic appearances
-
Systematised image analysis is based on several schemes. It is, however, recommended that every radiologist chooses the scheme that best suits him. The most important point is that the radiologist adheres to the scheme he chooses. Only in this way, mistakes can be avoided and no important findings overlooked.
Examples of schemes from inside outwards: Heart, mediastinum, lungs, ribs, chest wall. From outside inwards: Chest wall, ribs, lungs, mediastinum, heart.
3 Important Radiographic Signs
3 Silhouette Sign
The borders of certain structures on the chest X-ray are visible due to the difference in density between these structures and the adjacent lung tissue. For example, the radio-dense hilum is clearly seen opposed to the adjacent radio-lucent lung tissue. The silhouette sign means absence of the normally present visible borders due to loss of the normal difference in radio-opacity. The cardiac border is usually seen against the adjacent lung, but whenever there is a change of lung tissue density adjacent to the heart, for example by tumour or infiltrate, the cardiac border is no longer visible. The presence of some aerated lung tissue between the tumour or infiltrate and the heart may allow visualisation of the cardiac border.
The silhouette sign enables localisation of lung opacities, for example an opacity that obscures the right cardiac border will be located in the right middle lobe. The left cardiac border is obscured by opacities in the lingula.
The border of the right diaphragm is blurred by right lower lobe pathologies and similarly the left diaphragmatic border by left lower lobe pathologies.
3 Air Bronchogram
The air bronchogram is defined as visualisation of a bronchus against the background of lung parenchyma. The bronchi contain air and are normally seen in the lung hilum only when imaged en-face. Normally, the bronchial walls are too thin to be seen. A bronchus becomes visible when air in the surrounding lung tissue is replaced by denser material that contrasts with the air-containing bronchial lumen.
3 Air Trapping
Inhalation of a foreign body can result in a localised lung hyperinflation. This more commonly occurs in the right side with obstruction of the main bronchus or a segmental bronchus. In general, bronchial obstruction by aspiration may cause either atelectasis due to complete obstruction or hyperinflation due to valve mechanism. In the case of hyperinflation, the affected lung is hypertranslucent and increased in volume. Air-trapping could be shown by fluoroscopy and the mediastinum moves on expiration towards the healthy side.
4 Imaging Criteria
4.1 Imaging Criteria for Assessment of Individual Structures
Systematic analysis of the chest X-ray is summarised in Tables 19.6 and 19.7.
4.1 Trachea
Imaging criteria
-
Normal values: coronal diameter 21–25 mm
-
Stenosis?
-
Course? Displacement?
-
Intraluminal lesions?
-
Rights paratracheal line is widened by:
-
Mediastinal lymphadenopathy
-
Malignant tumours of the trachea
-
Mediastinal tumours
-
Mediastinal fluid
-
4.1 Heart/Mediastinum
The borders of the heart and mediastinal structures are clearly visualised except when it comes into contact with the left diaphragm (see ▶ Sect. 19.1 ).
The right upper mediastinal border is formed by the superior vena cava and the brachiocephalic trunk. With aging, aortic elongation occurs and the aorta contributes to this border. The left upper mediastinal border is less sharply defined. It is formed by the subclavian artery and the aortic knuckle.
Imaging criteria:
-
Widening of the mediastinum
-
The aorto-pulmonary window
-
Air in the mediastinum (pneumo-mediastinum)?
-
Air-fluid levels?
-
Foreign body? (e.g., cardiac valves, stent)
-
Calcifications? (e.g., pericardium, valves, lymph nodes)
-
Size of the heart
-
Contour of the mediastinal borders (e.g., with aneurysms)
4.1 Diaphragm
Normally, the diaphragm has smooth and sharp borders (see Sect. 19.1). The diaphragmatic borders are blurred, according to the silhouette sign, with pathologies affecting the adjacent portions of the lungs. Fibrosis or lung scarring can also lead to blurring of the diaphragmatic borders.
The distance between the left diaphragm and the gastric air bubble should be noted. If it is greater than about 1 cm, a subpulmonary effusion or a tumour may be present.
The costo-phrenic recesses should be comparable on both sides, especially in the lateral radiograph. A blunted recess may be due to pleural effusion or fibrous tissue. For differentiation, comparison with previous films may be helpful or supplementary sonography.
There are many reasons for uni- or bilateral elevation or depression of the diaphragm. Bilateral depression of the diaphragm is due to increased intrathoracic air volume as occurs in emphysema for example. Physiologically, bilateral depression of the diaphragm may be seen in young people and athletes. Bilateral elevated diaphragm may be caused by reduced intrathoracic air volume, reduced mobility of the diaphragm (such as with obesity), or pleura. An expiratory film can differentiate between these causes.
Unilateral elevation of the diaphragm can be caused either by intra- or extrathoracic causes. Extrathoracic causes include abdominal masses such as hepatomegaly or splenomegaly, subdiaphragmatic abscesses. Intrathoracic causes include subpulmonary effusion, atelectasis, phrenic nerve paralysis, pleurisy, or pleural thickening (. Fig. 19.25 ).

Chest X-ray analysis. Depressed flattened diaphragm. Slender elongated heart shadow

Subphrenic abscess. Chest X-ray posteroanterior view shows an air-fluid level over the liver (arrows), elevated right diaphragm due to pain-related limited reparatory effort. Associated basal lung atelectasis
4.1 Cervical Soft Tissues
The sterno-cleidomastoid muscles may appear on the chest radiograph as lateral, vertical, sharply demarcated opacities (Fig. 19.26).

Soft tissue shadows in the chest X-ray
Above the clavicle also in thin individuals, the skin may form a fold that runs parallel to the clavicle as a delicate line that passes medially to the sterno-cleidomastoid. Skin folds may mimic the pleural line of pneumothorax. The continuation of a skin fold line into the surrounding soft tissue enables exclusion of pneumothorax. This is frequently observed in supine radiographs in the intensive care unit. The cause may be that the cassette is placed under the patient without proper lifting of the patient so that the skin is folded.
In the neck soft tissues, particularly in the elderly, calcifications in the thyroid are commonly seen.
4.1 Lungs
Imaging criteria
-
Translucency changes:
-
Increased translucency
-
Reduced translucency
-
-
Parenchymal destruction
-
Opacities:
-
Diffuse (alveolar/interstitial)
-
Circumscribed (nodule)
-
Reticulo-nodular (generalised/focal)
-
4.2 Changes in Lung Translucency
The translucency of the lung is dependent on its density and the degree of X-ray attenuation. The healthy lung has a homogeneous translucency; with a density of 0.3 g/ml. During sleep, there is increased translucency.
The density of lung parenchyma is affected by the following factors:
-
Air
-
Blood
-
Connective tissue fluid
Normal lung density is defined as follows:
-
Air: 4/6th the density
-
Blood in the pulmonary arteries and pulmonary veins: 1/6th the density
-
Connective tissue fluid: 1/8th the density
-
Connective tissue: 1/8th the density
It is essential to note that fluid density is shown regardless whether the fluid is interstitial, alveolar, or intracellularly located. Also note that translucency of the lung has high individual variability and is affected also by extrapulmonary factors, such as obesity and breast shadows.
The diagnosis of parenchymal pathologies of the lung on conventional X-ray is difficult because of the low sensitivity. This means that irreversible pathologic changes such as pulmonary fibrosis may not be diagnosed until an advanced stage. The diagnosis of parenchymal lung diseases is essentially based on the use of CT.
Parenchymal diseases may follow one of the following patterns:
-
Diffuse distribution:
-
Alveolar
-
Interstitial
-
-
Localised distribution:
-
Nodular
-
Reticular
-
-
Combination of nodular and reticular representation:
-
Diffuse
-
Focal
-
4.2 Increased Translucency
Definition.
An increase in translucency is defined as the increase in intrathoracic air content. The increased translucency may be diffuse or localised and vascular markings may be present or absent. It is caused by a reduced absorption of X-rays. The assessment criteria are:
-
Increase in the air distribution:
-
Homogeneous/inhomogeneous increased translucency
-
-
Decreased vascular markings
-
Signs of pulmonary arterial hypertension
-
Displacement of lung fissures:
-
With localised hyperinflation
-
-
Displacement of the diaphragm:
-
Depression inferiorly, below the level of the 6th rib anteriorly
-
Flattening/inversion of the diaphragm
-
-
Increase in the size of the lung:
-
Widening of the intercostal spaces
-
Retrosternal space > 25 mm
-
Increase in the size of the thorax in all directions
-
Causes of Increased Translucency.
-
Intrapulmonary:
-
Increased air content of the lung parenchyma.
-
Dilation of the alveolar spaces.
-
Decreased connective tissue.
-
Loss of the vascular markings due to decreased perfusion.
-
-
Extrapulmonary: Whenever increased translucency is seen on the chest radiograph, all efforts should be made to exclude extrapulmonary causes. A distinction must be made between patient-related etiologies and technical factors. The causes of extrapulmonary increased translucency are:
-
Technical reasons:
-
-
Incorrect positioning of the patient.
-
Mal-position of the X-ray tube.
-
Patient-related causes:
-
-
Thoracic asymmetry (posture, scoliosis).
-
Soft-tissue asymmetry (hemiplegia, absent pectoralis muscle, condition after mastectomy).
4.2 Bilateral Increased Translucency
Bilateral increased translucency with preserved vascular markings is due to increased air content in both lungs. The cause is either an expiratory obstruction as in acute asthma attack, or stenosis of the upper airway (. Table 19.8 ).
Increased translucency with normal intrathoracic air content may be caused by congenital heart disease with decreased pulmonary blood flow (oligemia) or decreased perfusion due to multiple pulmonary emboli.
Obstructive Pulmonary Diseases
Obstructive pulmonary diseases are characterised by an increase in the resistance to airflow in the bronchi. This occurs due to a narrowing of the bronchi either from outside the lumen in the muscular walls, or from inside the lumen by mucus or mucosal thickening. The cause of increased resistance to air inflow may also be extrathoracic, for example compression of the trachea or vocal cord paralysis.
Extrathoracic etiologies result in impairment of inspiration, while intrathoracic obstructive pulmonary diseases usually affect expiration. With impairment of expiration there is prolongation of the expiratory time and increased intra-alveolar pressure. This in turn causes alveolar damage and loss of elasticity so that lung compliance increases. The thorax becomes barrel-shaped. Moreover, the high expiratory pressure necessary to overcome the increased resistance causes compression upon the bronchioles, so that the resistance further increases. The respiratory effort must be markedly increased. The FEV1 (forced expiratory volume in the first second) is significantly limited. A simultaneous disorder in perfusion occurs, with vasoconstriction of hypoventilated alveoli and a consequent increase in resistance in the pulmonary circulation. This leads to the development of pulmonary arterial hypertension, and eventually Cor pulmonale.
Emphysema and bronchial asthma are examples of obstructive lung diseases.
4.2 Emphysema
4.2 Definition
Emphysema is defined as a constant and irreversible enlargement of the alveolar spaces distal to the terminal bronchioles, with destruction of the interstitium of the lobule and the interlobular septa without formation of connective tissue (Fig. 19.28).

Sternocleidomastoid muscles on chest X-ray

Schematic representation of emphysema
4.2 Pathogenesis, Aetiology
Emphysema is often seen with cigarette smoking. Particularly in pan-lobular emphysema in young patients, α1-antitrypsin deficiency should be suspected. Emphysema is thought to result from an imbalance between proteases and protease inhibitors. There may be excess protease, formed in alveolar macrophages and leucocytes; or deficiency in a protease inhibitor such as α1-antitrypsin deficiency. This leads to destruction of the lung parenchyma, and development of emphysema. Smoking plays a significant factor, since it causes a chronic inflammatory response with accumulation of Elastase-producing lymphocytes. Furthermore, Elastase inhibitors are inactivated by direct toxic metabolites of smoking.
The α1-antitrypsin deficiency (also known as: Laurell-Eriksson syndrome; α1-proteinase inhibitor deficiency) is an autosomal recessive inherited disease caused by a mutation in the α1-antitrypsin gene (PI) on the long arm of chromosome 14 (14q32.1). On electrophoresis, different allele variants are detectable, F = fast, S = slow, Z = very slow, M = intermediate. Normal alleles are designated by MM and the most important homozygous defect is ZZ. The α1-antitrypsin is the major plasma proteinase inhibitor, which inhibits the neutrophil Elastase, trypsin, plasmin, and thrombin. The glycoprotein is formed in the liver and transported via the blood. The presence of excess amounts of destructive Elastase leads to the development of pulmonary emphysema. The liver can be also affected by hepatic cirrhosis. Several mutations may occur, the most common two variants include:
-
PiZ: amino acid substitution of glutamine by lysine at codon 342, most commonly seen in northern Europe
-
PiS: substitution of glutamic acid by valine at codon 264, most commonly seen in southern Europe
Plasma concentrations of α1-antitrypsin can be measured. In homozygous α1-antitrypsin deficiency, reduced values are observed up to 15% residual activity. In heterozygous carriers, the level is below the normal range. In heterozygous carriers, genetic typing may be necessary for establishing the diagnosis.
4.2 Clinical Presentation
The condition presents with progressive dyspnea, at first with exercise, later also at rest. This is followed by development of cyanosis and increased serum haemoglobin levels. Chronic lung overinflation leads to the development of the typical barrel chest.
The diffusion capacity is reduced due to reduction of functional parenchyma, meanwhile, the dead space, not participating in gas exchange, is increased.
4.2 Diagnosis
Analysis of blood gases is performed for quantitative determination of gas exchange disorder. Polycythemia is also present. Pulmonary function tests show increased functional residual capacity and residual lung volume with progressive loss of elasticity of the lung. The expiratory phase is prolonged.
Chest X-Ray
-
Low-lying, flat diaphragms (inferior to the 6th rib anteriorly).
-
Inversion of the diaphragm may occur.
-
Widened retrosternal space (> 2.5 cm).
-
Barrel chest with almost horizontal ribs (Fig. 19.29).
Fig. 19.29 
Panlobular emphysema. Chest X-ray posteroanterior view shows confluent emphysematous changes, more marked in the lower zones. The ribs are horizontal
-
Increased translucency (homogeneous/inhomogeneous). The inhomogeneity is caused by the different degrees of involvement of the lung fields, and in part due to the associated linear opacities consistent with compression atelectasis.
-
Vascular markings (Fig. 19.30):
Fig. 19.30 
Emphysema. Chest X-ray lateral view shows an enlarged retrosternal space and depressed flattened diaphragms
-
Decreased peripheral vascular markings are characteristic of emphysematous lung destruction. The distance between radiographically visible vessels becomes larger.
-
Change in calibre of vessels. Vessel calibre decreases and they cannot be traced to the periphery of the lung and show abrupt termination.
-
-
Signs of pulmonary arterial hypertension:
-
Dilatation of the central pulmonary arteries > 19 mm
-
Dilatation of the pulmonary trunk > 46 mm lateral to the carina. Pulmonary trunk dilatation causes secondary narrowing of the retrosternal space.
-


4.2 Centri-Lobular Emphysema
Definition, Aetiology, Clinical Presentation
There is destruction of the dilated proximal respiratory bronchioles by a destructive bronchiolitis with airway obstruction. The upper lobes are most affected. This is also known as smoker’s emphysema. There is often perfusion disorder with subsequent hypoxemia. Clinically, the condition commonly presents with the “blue bloaters” pattern with cyanosis, polycythemia, productive cough, mostly in overweight patients.
CT Imaging (Fig. 19.32):

Panlobular emphysema. Axial CT image in lung window shows thin small vascular markings and confluent areas of low attenuation

Centri-lobular emphysema. Axial CT image in lung window
-
Small areas of homogeneous parenchymal destruction, on background of healthy lung tissue, more in the upper lobes
-
With disease progression, there is often involvement of the entire lobule
-
Reduced vascular markings are first seen in advanced stages
-
In the advanced stage, centri-lobular emphysema becomes indistinguishable from pan-lobular emphysema
4.2 Pan-Lobular Emphysema
Definition, Aetiology, Clinical Presentation
Destruction of the secondary lobule, to a greater extent in the basal lung zones; often associated with α1-antirypsin deficiency. Clinically, the patients usually present with the “pink puffers” pattern with marked dyspnea and only scarce sputum in a rather cachectic patient, because of the increased respiratory activity associated with the increased dead space.
CT Imaging
-
More marked parenchymal damage than with centri-lobular emphysema
-
Destruction of the alveoli
-
Significant decrease in number and calibre of pulmonary vessels
-
Lung density values < −900 to 950
-
Confluence of the emphysematous areas (Fig. 19.31)
-
Lower lobe preference
-
In advanced stages, not easily differentiated from centri-lobular emphysema
-
Typically by deficiency in α1-antitrypsin
4.2 Paraseptal Emphysema
Definition
Paraseptal emphysema represents a special form of emphysema, and is a type of pan-lobular emphysema. The peripheral subpleural lobules and the alveoli near the interlobular septa are affected.
CT Imaging
-
Areas of varying density separated by interlobular septa
-
Typically subpleural
-
More in the dorsal upper lobes
-
Interlobular septa are preserved in early stages
-
In advanced stages, there is destruction of the secondary lobules and subpleural bullae
-
Often occurs in combination with other types of emphysema
Special form: Irregular (or para-cicatricial) emphysema refers to destruction and irregular airspace enlargement with bullous formation, adjacent to localised parenchymal scars, seen with diffuse pulmonary fibrosis and other lung fibrosis.
4.2 Treatment of Emphysema
To prevent disease progression, all pollutants must be avoided such as smoking, dust, etc. Pulmonary infections must be early and aggressively treated. Symptomatic bronchodilator therapy may be given. To prevent bronchiolar collapse, patients with emphysema should learn special breathing techniques, such as “pursed lip” breathing.
Oxygen therapy is indicated for low blood oxygen level, PaO2 < 55 mmHg at rest or during physical activity, and if there is no hypercapnia or PaO2 < 60 mmHg with cor pulmonale. With advanced respiratory failure, administration of oxygen is contraindicated, because hypoxia is the most important respiratory stimulus.
Another treatment option is partial lung resection to reduce hyperinflation and improve cardiac pumping capacity. Another option is lung transplantation.
In α1-antitrypsin deficiency supplementation by human α1-antitrypsin is under trial but the results are still not definitive.
Mismatch: mismatch is due to nonuniform distribution of ventilation in different lung regions or to an altered ratio of ventilation and perfusion. This can occur in the context of obstructive lung diseases. The increased dead space, for example, will contain well-ventilated, but insufficiently perfused alveoli.
4.2 Bronchial Asthma
4.2 Definition, Aetiology, and Pathogenesis
Asthma is a chronic inflammation of the airways, which is associated with obstruction. There are various forms of asthma, often grouped into extrinsic and intrinsic types. Extrinsic asthma is triggered by allergens in the environment. The intrinsic type may be triggered by infections, exercise, or chemical-irritative substances. Mixed forms are also possible. A predisposing factor is a pre-existing atopic condition such as atopic pollinosis or neurodermatitis.
Pathogenesis in a quarter of patients with adult onset asthma is a type I IgE-mediated hypersensitivity reaction. Specific allergens cause degranulation of mast cells and eosinophils that release a large number of mediators. Bronchospasm is caused by smooth muscle contraction and aggravated by glandular hypersecretion and chemotactic stimulation of inflammatory cells. The reaction occurs minutes after allergen exposure and subsides within hours. This is followed by a second phase that is similar to an inflammatory response and has a chronic course.
In some patients, the reaction is IgG-mediated and occurs about 12 hours after exposure. In this pseudoallergic reaction, the same mediator systems are activated. However, prior sensitisation is not necessary and the reaction may occur with first contact.
4.2 Clinical Presentation
Typical symptoms are:
-
Breathlessness episodes with chest tightness
-
Wheezing
-
Breathing becomes possible only with the help of respiratory muscles
-
Prolonged expiration
-
Tachycardia
-
Reduced respiratory movement
-
Glassy sputum
4.2 Diagnosis
Medical history is important, when and how often the episodes occur. Laboratory tests reveal eosinophilia, especially in allergic asthma; associated infections result in increased inflammatory markers. Sputum analysis reveals eosinophils, Curschmann spirals, and Charcot-Leyden crystals. Similar to emphysema, percussion reveals hyper-resonant chest with low-lying diaphragm. Auscultation reveals the typical wheezing and hum. ECG performed during attacks shows sinus tachycardia and possibly signs of right heart strain.
Lung function tests show reduced FEV1 (forced expiratory volume in the first second), increased functional residual capacity, and airway resistance. The peak flow rate is also reduced. The FEV1 increases to normal with inhalation of β2-antagonists. In severe obstruction, there is increased residual volume with decreased vital capacity. Depending on the severity asthma may be classified into intermittent, mild persistent, moderate persistent, and severe persistent grades. This grading is important for stepwise therapy.
In peak flow measurement, similar to FEV1, the maximum airflow rate under forced expiration in L/s is measured. Since this is performed by a simple, inexpensive, small device, this method is suitable for self-monitoring by patients. This enables early recognition of disease progression and helps in optimisation of therapy. The standard values are dependent on age, sex, and size of the patient. The test should be performed every time under similar conditions, preferably in the morning, because circadian variations are possible. Whenever the values drop to less than 80% of the personal best values, revision of therapy is recommended.
Imaging.
Chest X-ray is required mainly for exclusion of other diseases, such as obstructive tumour, pneumonia, or parenchymal lung disease. There are no specific signs for the diagnosis of asthma. During the asthmatic attack, an emphysema-like picture is seen with lowered diaphragms and bilateral increased radiolucency.
4.2 Treatment
Severity of asthma according to the German Airway League:
-
Intermittent asthma: up to 2 day-time attacks per week and 2 night-time attacks per month, FEV1 > 80%.
-
Mild asthma: > 2 day-time attacks per week, but < 1 attack per day and > 2 night-time attacks per month. FEV1 up to 80% reduced.
-
Moderate asthma: day-time daily attacks, > 1 night-time attack per week. FEV1 between 60 and 80%.
-
Severe asthma: permanent clinical symptoms, also common at night. FEV1 < 60%.
The treatment of asthma is based on several pillars, and is particularly important for the radiologist because asthmatic attacks may occur with exposure to radiologic contrast media. The first pillar is avoidance of the triggering allergen. The second pillar is anti-inflammatory and broncho-dilatator medications.
-
For intermittent asthma, an inhaled β2-mimetic is indicated when necessary. In mild persistent asthma this should be supplemented with low-dose inhaled corticosteroid on a regular basis.
-
In the next stage, the basic treatment is corticosteroid inhalation as well as long-acting β2-mimetics. They may be supplemented by oral theophylline or β2-mimetic. During attacks, a rapid-acting β2-mimetic should be used.
-
In severe persistent asthma, therapy is based on high-dose inhaled corticosteroids and long-acting β2-mimetics and possibly systemic corticosteroids and theophylline. During acute asthma attacks, dilatation of the bronchi may be achieved by β2-mimetic inhalation or i.v. theophylline. Patients in a status should also be given a complementary i.v. dose of glucocorticoids and oxygen. A sedative such as Valium may be necessary.
-
In allergic asthma, prophylactic medications to stabilise mast cells like cromolyn and antihistamines are used. In addition, theophylline may be used to stabilise mast cells, as a bronchodilator and for respiratory stimulation.
Status asthmaticus:
-
Patient is managed in a sitting position with monitoring of cardiovascular and pulmonary function
-
Administer oxygen under control of pulse oximeter
-
Sedation is not indicated due to the respiratory depressive effect of benzodiazepines
-
Medications:
-
Up to 250 mg of prednisone i.v.
-
Theophylline 200 mg i.v. (possibly by infusion)
-
With stable circulation Reproterol 90 micrograms i.v. (caution: arrhythmias in previous self-medicated patients)
-
Mucolytics
-
4.2 Unilateral Increased Translucency
The differential diagnosis of unilateral increased translucency may be caused by technical factors, or by changes of the chest wall or pleura. Pulmonary causes include changes of lung parenchyma or pulmonary vasculature.
Causes of unilateral increased t ranslucency
-
Technical reasons:
-
Mal-centred tube, patient rotation
-
-
Soft tissue:
-
Postmastectomy
-
Muscle atrophy such as hemiplegia
-
Congenital muscular asymmetry. E.g., severe scoliosis
-
-
Pleural causes:
-
Pneumothorax
-
-
Disorders of perfusion:
-
Congenital: hypoplastic lung, pulmonary atresia
-
Acquired: pulmonary embolism, tumour-related narrowing of the pulmonary artery
-
-
Disorders of ventilation:
-
Congenital lobar emphysema
-
Bronchial occlusion by mucus
-
Foreign body
-
Central mass
-
Swyer-James syndrome
-
Bronchiolitis obliterans
-
-
Defects of the lung parenchyma:
-
Bullae
-
Compensatory hyperinflation such as after pneumonectomy
-
4.2 Pneumatocele
A pneumatocele is a well-circumscribed increased transparency due to a thin walled cavity in the lung parenchyma (Fig. 19.34). A postinflammatory bronchial stenosis results in a valvular mechanism with overinflation of the lung parenchyma distal to the affected bronchus. The surrounding lung parenchyma is displaced and compressed. Pneumatoceles are frequently seen after Staphylococcal infection or trauma and may be reversible.

Emphysema. Axial CT image in lung window

Pneumatocele. a Chest X-ray posteroanterior view. b Chest X-ray lateral view. Cystic radiolucent lesion with thin walls in the right lung (arrows)
4.2 Decreased Translucency
Decreased translucency refers to a generalised loss of air-filled spaces. It is caused by an increased density of the tissue in the X-rays path, resulting in increased radiation absorption (Fig. 19.35). Opacities may be acinar, interstitial, or homogeneous. A focal decrease in translucency may be due to nodules (solitary or multiple) or masses.

Calcified right breast implant. Chest X-ray posteroanterior view shows a calcified shadow overlying the right lower lung zone
In the diagnosis of opaque hemithorax, some important observations must be made. Whether the opacity is associated with reduced or increased volume is important. If the diaphragm or the mediastinum move away from the opaque hemithorax, there is increased volume; and the cause is space occupying. This may be caused by marked pleural effusion with no or only small atelectasis. Another cause is an advanced diaphragmatic hernia. This can be diagnosed if intrathoracic herniated intestine is recognised. An inflammatory infiltrate or abscess increases the volume also, but not to the degree that leads to mediastinal shift. With inflammatory infiltrate a positive air bronchogram is common. Pleural mesothelioma may also cause an increase in volume without displacement of the mediastinum.
The mediastinum is shifted to the same side of the opacity, in processes that are nonspace occupying and cause volume decrease. This is seen with atelectasis (. Fig. 19.36 ), after pneumonectomy with compensatory hyperinflation of the remaining lung and fibrous tissue in the affected side. Rarely, a unilateral lymphangitis carcinomatosa is seen with reduced volume.

Atelectasis. Schematic representation of the radiographic appearance of atelectasis
4.2 Atelectasis
4.2 Definition
Atelectasis is a homogeneous opacity due to decreased air in the lung with loss of lung volume. There are four different forms:
-
Obstructive atelectasis: with obstruction of the airway due to various etiologies (e.g., bronchial carcinoma, mucus, foreign bodies), air inside the alveoli is resorbed and not replaced (resorption atelectasis). The air bronchogram sign is not seen.
-
Compression atelectasis: the cause is external pressure, which compresses the affected parts of the lung. The atelectatic segments still theoretically contain air, therefore, in some cases, a positive air bronchogram sign is seen. Causes include pneumothorax, pleural effusion, or elevated diaphragm.
-
Band atelectasis: fine bands of atelectasis appear as narrow, linear shadows in a horizontal orientation within the lung parenchyma (. Fig. 19.37 ). They occur with decreased diaphragmatic mobility. Larger plates of atelectasis are often due to decreased surfactant.
Fig. 19.37 
Linear atelectasis. Chest X-ray posteroanterior view shows band-like linear atelectasis in the right lower lung zone
-
Cicatrisation atelectasis: fibrotic changes of the lung parenchyma in chronic inflammations lead to volume reduction.

Special form: The round atelectasis appears on radiographs as a round, homogeneous opacity in the basal lung segments with contact to focal thickened pleura. A characteristic sign is comet tail-like bronchi, which extend from the round atelectasis towards the lung hilum.
4.2 Imaging
X-ray (Fig. 19.38 ):

Upper lobe atelectasis. a Chest X-ray posteroanterior view shows opacity in the upper zone with upward displacement of the lung fissure. b Axial CT image and c Coronal reformatted CT image show narrowing of the upper lobe bronchi by bronchial carcinoma (arrows)
-
Indirect signs:
-
Signs of loss of volume e.g., elevated diaphragm or hilar displacement
-
Shift of the mediastinum to the affected side due to the volume loss
-
Compensatory hyperinflation of the remaining lung
-
-
Direct signs:
-
Displacement of interlobar fissures as a sign of volume loss
-
Localised decreased translucency due to hypoventilation of the lung parenchyma
CT.
Atelectasis appears dense on CT, sharply demarcated from the surrounding lung parenchyma, with strong contrast enhancement. Additional signs include:
-
Homogeneous compressed lung parenchyma
-
Displacement of vessels as a sign of volume reduction
-
Displacement of interlobar fissures
-
Positive air bronchogram except in complete obstruction atelectasis
Dependent on location there are various signs of Atelectasis (Overview).
Signs of lobar atelectasis according to location
Right upper lobe atelectasis
-
The horizontal fissure is shifted upwards and medially
-
Opacity cranial and medial
-
Right hilum displaced upwards
-
Overinflation of the middle and lower lobes
-
Mediastinum is partially obscured
Middle lobe atelectasis
-
Horizontal fissure moves downwards to the inferior part of the main fissure
-
Partial opacity only due to the limited volume of the lobe
-
The right heart border is obscured
Right lower lobe atelectasis
-
Displacement of the main fissure posteriorly and inferiorly
-
Opacity lies posterior and medial
-
Right hilum shifted inferiorly
-
Obscured right heart border
-
Elevated right diaphragm
-
Hyperinflation of the remaining lung
Left upper lobe atelectasis
-
Displacement of the main fissure anteriorly
-
Opacity left para-mediastinal with central radiolucent line between it and aortic arch
-
Left hilum shifted upward
-
Shift of the mediastinum to the left
-
Overinflation of the right lung
Left lower lobe atelectasis
-
Displacement of the main fissure medially and inferiorly
-
Opacity lies posterior and inferior, behind the heart
-
Shift of the mediastinum to the left
-
Elevated left diaphragm
-
Hyperinflation of the remaining lung
Lingular atelectasis
-
Obscured left heart border
-
Anterior displacement of the main fissure
-
Elevated left diaphragm
4.3 Other Specific Image Findings
4.3 Cavities and Ring Lesions
4.3 Pathogenesis and Diagnosis
A cavity occurs when a rounded lesion undergoes central breakdown and the necrotic material is extruded or coughed away through communication with the bronchial system (Table 19.9). A fluid level may be seen on X-ray if the beam is horizontal. Otherwise they appear as ring shadows (Fig. 19.39). If the beam is tangential, they may appear oval or as parallel lines. CT is more sensitive for the detection of cavities.

Schematic representation of morphology of lung nodules
Bullae, cysts, and cavities can be distinguished, based on the aetiology and appearance. A bulla is thin walled, air filled, occurs with emphysema. Cavities are commonly inflammatory or neoplastic in origin.
4.3 Perivascular Subpleural, Peribronchial Opacities
Inflammatory and other disease processes of the lungs may be associated with thickening of the interlobular septa as well as thickening of the perivascular peribronchial and subpleural spaces:
-
Peribronchial cuffing: thickening of the bronchial wall, clearly visible when the bronchus is seen end on
-
Blurred vascular structures
-
Thickened Interlobular septa
4.3 Nodular Pattern
The nodular pattern is characterised by rounded, sharply defined opacities up to 1 cm in diameter, which are diffusely seen all over the lung fields. The distribution pattern may vary, being symmetrical or asymmetrical, basal or apical distribution. Based on the nodule size, different types are differentiated (Table 19.10)
-
Micronodular (miliary):
-
Tiny nodules, approximately 1–3 mm, sharply defined, not confluent
-
Occurs with opacified alveoli or interstitial changes
-
Example: miliary tuberculosis (Milium = Hirsekorn)
-
-
Macronodular:
-
Discrete nodules with a diameter of 5–10 mm
-
Sharply defined without confluence tendency
-
Examples: sarcoidosis, silicosis, Histiocytosis X, or metastases from thyroid carcinoma
-
-
Reticulo-nodular:
-
Nodular opacities associated with reticular opacities
-
4.3 Reticular Pattern Including Honeycombing
A reticular pattern is defined as a fine irregular network of lines in the lung parenchyma. Different forms can be observed:
-
Fine reticular opacities:
-
More centrally located
-
Formed by the superimposition of thickened septa, also known as Kerley C lines.
-
Normal vascular markings are obscured by the reticular opacities
-
-
Honeycombing:
-
Coarse reticular markings
-
Mostly in basal lung segments in interstitial lung diseases such as end-stage pulmonary fibrosis
-
Caused by extensive fibrosis of the interstitium with distraction of the bronchioles and their irregular dilatation
-
Honey-combing may be complicated by pneumothorax
-
A reticular pattern may be caused by various etiologies including idiopathic interstitial fibrosis, Langhans cell histiocytosis, cystic fibrosis, sarcoidosis type III, pneumoconiosis particularly asbestosis, advanced extrinsic allergic alveolitis, drug toxicity, collagen vascular diseases.
4.3 Pulmonary Nodules
4.3 Definition, Pathogenesis
A nodule is a nearly rounded well-circumscribed opacity with a diameter of about 1–6 cm, larger than those present in the nodular pattern and usually less in number (Fig. 19.39).
Causes of pulmonary nodules
-
Granulomatous diseases:
-
Tuberculosis: usually in the upper lobes, partly calcified, smooth margins, satellite nodules
-
Histoplasmosis: smooth margins, more in lower lobes, satellite nodules, calcifications
-
Silicosis: relatively dense nodules in the middle lung fields, hazy margins
-
Wegener’s granulomatosis: rarely solitary, tends to cavitate
-
-
Neoplasms:
-
Bronchial carcinoma; rapid growth, mostly peripherally located, infiltrative margins
-
Metastases; solitary in a quarter of cases, most common primary tumours include breast cancer, renal cell carcinoma, seminoma, osteosarcoma (calcifications are common)
-
Lymphoma
-
Myeloma
-
Alveolar cell carcinoma; rarely well-circumscribed nodules
-
-
Infections and parasites:
-
Abscess, chickenpox, Aspergillosis, echinococcosis, pneumonia
-
-
Metabolic diseases:
-
Amyloidosis, Gaucher Disease
-
-
Autoimmune diseases:
-
Rheumatoid, hypersensitivity disorders
-
-
Vascular disorders:
-
Arteriovenous malformation; mostly solitary, lobulated, with smooth margins
-
Haematoma: history of trauma, smooth margins, tends to regress
-
-
Others:
-
Sarcoidosis, pneumoconiosis, Histiocytosis X, methotrexate, hamartoma
-
-
Lung sequestration
-
Bronchogenic cyst
4.3 Diagnosis
General criteria include:
-
Sign of benign lesions:
-
Sharp demarcation
-
Solitary lesion
-
Partially calcified
-
-
Signs of malignancy:
-
Rapid increase in size
-
Unsharp borders
-
Spiculations (corona radiata)
-
Pleural finger
-
Umbilication (. Fig. 19.40 and . Table 19.11 )
Fig. 19.40a,b 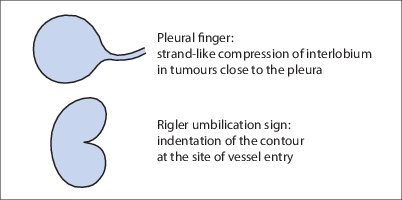
Schematic representation of pleural finger and umbilication signs. a A pleural finger is a fine linear extension from the nodule towards the pleura. b Umbilication sign with indentation of the contour at the site of vessel entry
Table 19.11 Signs of pulmonary nodules
-

4.3 Calcification Pattern as Diagnostic Criteria
Calcifications are common findings on chest radiographs. The aetiology is variable, but in most cases; pulmonary calcifications are caused by old inflammatory processes (Table 19.12). When calcifications are difficult to localise to the lungs, tomography, additional oblique radiography, or CT are recommended.
Calcifications in the thoracic soft tissue have similar causes to soft tissue calcifications elsewhere, including renal failure; dermatologic disorders, post-traumatic myositis ossificans. Calcifications in the breasts may be caused by fibroadenoma, fibrocystic changes, or fat necrosis. Calcifications in the heart often have a characteristic appearance.
Pulmonary calcifications are characterised by:
-
Malignant neoplasms calcify less than benign lesions
-
Fine, laminated calcifications are common with processes that are slowly progressive such as granulomas
-
Chondro-hamartomas display coarse pop-corn calcifications
4.3 High-Resolution CT Patterns
High-resolution CT is a special form of CT, with thin sections (1–2 mm) and large interslice gaps. Alternatively, modern multislice CT (MSCT) allows an adequate thin section collimation. Four different patterns are used for diagnosis and classification of parenchymal changes on high-resolution CT:
-
Increased density:
-
consolidated infiltrates and fibrous changes
-
Ground glass opacity: caused by various processes such as intra-alveolar fluid, thickening of the alveolar wall or alveolar collapse
-
-
Reduced density:
-
In the context of emphysematous changes, decreased perfusion, cavities, cysts, bronchiectasis
-
-
Reticular pattern:
-
Excess fluid or scarring tissue in the interstitium
-
Appears as increased bronchovascular markings, septal or intralobular thickening, or in severe cases as so-called honeycombing
-
Septal or intralobular thickening are typical with lymphangitis carcinomatosis, sarcoidosis, or fibrotic disease
-
-
Nodular pattern:
-
Tiny rounded nodules up to 6 mm in diameter
-
Smooth margins in miliary shadows or alveolar shadowing in alveolitis
-
Nodules are centri-lobular with involvement of the arterioles or alveoli
-
Can be directly adjacent to the pleura, and in some cases show the “tree-in-bud sign”
-
The distribution varies from diffuse with haematogenous seeding throughout the lungs, with lymphatic spread the distribution is along the lymphatic vessels
-
5 Congenital Anomalies
A wide variety of congenital abnormalities affect the region of the thorax and may present difficulties in interpretation of radiologic examinations. A knowledge of such abnormalities is necessary to differentiate variants from pathologic conditions. The most common congenital abnormalities are described in the following section, classified according to the involved structure.
5.1 Bony Skeleton
5.1 Thoracic Deformities
Primary Thoracic Deformities.
This includes:
-
The so-called pigeon chest with convex sternum
-
The funnel chest with concave curvature of the sternum towards the inside
Thoracic deformities lead to a change in the diameters of the thorax, causing a change in position of the thoracic organs. On X-ray, this may be falsely interpreted as cardiac enlargement or simulate pulmonary infiltrate.
Secondary Thoracic Deformities.
A bell-shaped thorax may be seen with osteomalacia or rickets, due to the pseudofractures causing rib deformities, so that the thorax becomes bell shaped with a transverse diameter smaller cranially than caudally. A barrel-shaped chest with an enlarged anteroposterior diameter is usually seen with emphysema due to the increased lung volume with increased kyphosis of the thoracic spine and bulging of the sternum. With scoliosis, the disturbed loading of the skeletal apparatus causes bizarre deformity of the thoracic skeleton with subsequent significant functional limitations (Fig. 19.41).

Chest wall deformity. Chest X-ray posteroanterior view in a patient with advanced dorsal scoliosis with convexity to the right causing a deformed heart shadow and unsharpness of cardiac and mediastinal borders
5.1 Rib Anomalies
In assessing the rib anomalies on X-ray, it is important to be able to identify the anterior and posterior portions of the ribs separately. The posterior part is nearly horizontal and the contours are relatively sharp. Conversely, the anterior part of the rib is oblique with relatively blurred contours.
Calcifications at the costo-chondral junction of the first rib may simulate apical nodules on X-ray.
Common congenital abnormalities of the ribs include bifid or fused ribs. A bifid rib splits anteriorly into two ends. Sometimes the first rib is rudimentary and fuses with the second rib or with the manubrium. Herniation of the lung may be associated. Individual ribs on one or both sides may be absent. Additional cervical or lumbar ribs may be observed (Fig. 19.44). A large cervical rib may cause neural or vascular compression syndrome.

Chest wall deformity. Chest X-ray lateral view. Advanced dorsal scoliosis limits the diagnostic value of the radiograph. The dorsal vertebrae could not be adequately visualised (arrows)

Chest wall deformity. Chest X-ray posteroanterior view. The anterior chest wall deformity is caused by osteolytic lesions of the left fourth and eighth ribs

Cervical rib. Chest X-ray posteroanterior view shows a left cervical rib (arrows)
5.2 Lungs
5.2 Bronchogenic Cyst
5.2 Definition, Epidemiology, and Pathogenesis
Bronchogenic cysts are rare and sporadic. Males and females are equally affected. The onset of symptoms depends on the size and location of the cyst.
Bronchogenic cysts are caused by a congenital defect in the bud formation of the ventral diverticulum of the foregut around the fourth week of gestation. The location of the bronchogenic cyst depends on the timing of the defect. It may be located in the mediastinum or intrapulmonary. Intrapulmonary cysts usually have a connection with the bronchial system, and are lined by ciliated epithelium and filled with either air or mucus. There is no separate blood supply. Mediastinal cysts are more common than intrapulmonary cysts and are usually situated adjacent to the carina. They are also lined with respiratory epithelium, but they usually have no connection to the bronchial system. Accordingly, they are filled with fluid.
5.2 Clinical Presentation
The symptoms are variable, including shortness of breath, recurrent infections, and dysphagia, depending on the location and size of the cyst. Commonly, the cysts are asymptomatic and are discovered as incidental findings during chest radiologic examinations.
5.2 Imaging
Radiography:
-
Rounded opacity with smooth margins
-
Two thirds of intrapulmonary cysts occur in the lower lobes
-
Fluid- or air-filled, depending on the connection to the bronchial system
Additional findings on CT:
-
Density dependent on the protein content of the cyst
-
No contrast enhancement
5.2 Treatment
Surgical excision is indicated in symptomatic cysts with recurrent infections and dyspnea.
5.2 Pulmonary Hypoplasia
5.2 Definition and Aetiology
Pulmonary hypoplasia refers to insufficient formation of the lung that may be unilateral or bilateral. The severity of lung hypoplasia depends on the timing at which the injury occurs. Causes include various forms of intra- or extrathoracic compression of the developing lung, or hypoxia.
5.2 Clinical Presentation
The clinical presentation of pulmonary hypoplasia is variable and depends on the severity. Bilateral pulmonary hypoplasia is not compatible with life. Meanwhile, unilateral pulmonary hypoplasia is associated with high mortality due to infection of the hypoplastic lung.
5.2 Imaging
In unilateral pulmonary hypoplasia, the chest X-ray shows a smaller hemithorax compared to the contralateral side; with decreased vascular markings. The mediastinum is usually shifted towards the affected side.
Special Form: Scimitar Syndrome
In this syndrome there is partial aplasia of the lung associated with anomalous pulmonary vessels. Furthermore, other congenital defects of the ipsilateral diaphragm, such as hernia, as well as scoliosis or spina bifida may be present. The name of the syndrome results from the scimitar-like shape of the anomalous pulmonary vein draining into the inferior vena cava. The condition more commonly affects the right lung; with a higher predilection for women.
On CT there is mediastinal shift towards the affected side due to the induced volume reduction with elevated diaphragm. There is abnormal morphology of the bronchi and the ipsilateral pulmonary artery is small in size.
5.2 Lung Agenesis/Aplasia
5.2 Definition
Lung agenesis refers to the complete absence of one or both lungs.
5.2 Clinical Presentation
The presentation depends on the severity of the malformation, ranging from respiratory failure to completely inconspicuous symptoms when an isolated individual lobule is affected.
5.2 Imaging
Complete lung agenesis or aplasia appears on X-ray as a small totally opaque hemithorax with ipsilateral shift of the mediastinum. There is commonly compensatory hyperinflation of the healthy contralateral side.
5.2 Arterio-Venous Malformations
5.2 Definition, Epidemiology, and Aetiology
Arterio-venous (AV) malformations refer to the connection between a pulmonary vein and artery. They are also known as AV fistula or pulmonary AV aneurysm.
Women are affected about twice as often as men. AV malformations may increase in size with time. The slowly progressive admixture of venous and arterial blood in the shunt is rarely clinically noticed. AV malformations are usually congenital. However, they may be acquired after trauma, iatrogenic following surgical interventions, or postinflammatory. Osler syndrome, a hereditary autosomal dominant disease is usually associated with multiple AV malformations in the lungs and other organs.
5.2 Clinical Presentation
The symptoms depend on the size of the malformation. Most lesions are asymptomatic incidental findings. Common presentations include recurrent epistaxis and haemoptysis. Blood shunting may rarely cause hypoxemia and dyspnea. Cough and chest pain are also rare. Complications such as recurrent cerebral ischemia can be caused by a paradoxical thromboembolism.
5.2 Diagnosis
Hypoxemia can be diagnosed by blood gas analysis. Often, there is consecutive polycythemia.
Imaging.
Radiography shows a sharply demarcated opacity with the following criteria:
-
Often lobulated
-
Sometimes grape-like arrangement
-
Mostly in the lower fields near the diaphragm
Additional findings on CT:
-
The finding of feeding vessels is almost pathognomonic
-
The lesion shows a strong contrast enhancement
5.2 Treatment
Asymptomatic AV malformations require no treatment. Treatment is indicated with increase in size, significant hypoxemia, or embolic complications. In the past, treatment was mainly surgical, either excision of the affected lung portion or ligation of the feeding vessels. Nowadays, the main treatment is with angiographic coil embolisation.
5.2 Pulmonary Sequestration
5.2 Definition, Epidemiology, and Aetiology
Sequestrated lung is defined as functionless, aberrant lung tissue separated from the normal lung, and without connection to the bronchial system. Two types occur, intra- and extralobar sequestration. With extralobar sequestration (one-third of cases), the sequestrated lung lies, in contrast to the intralobar form (two-thirds), outside the normal pleura and is sometimes referred to as an accessory lobe. Extralobar sequestration is most commonly located subdiaphragmatic and on the left side. Intralobar sequestration occurs commonly in the lower lobes. Extralobar sequestration is sometimes associated with diaphragmatic hernia.
Males are affected about four times as often as females. The aetiology is still unclear, it may be due to an inflammatory process. The arterial supply is via central arteries branching from the aorta, and the venous drainage in most cases is into the corresponding pulmonary veins.
5.2 Clinical Presentation
The onset of symptoms is usually in adolescence. Symptoms include chronic cough, sometimes with blood-tinged sputum, chest pain, and recurrent pneumonia. In some cases, the diagnosis of lung sequestration is made in the context of prenatal screening.
5.2 Diagnosis
The diagnosis is also possible by means of ultrasound and color Doppler, depending on the location of the sequestrum.
Radiography:
-
Lobulated, homogeneous opacity
-
Cystic changes are possible; differential diagnosis includes bronchogenic cyst, abscess, tumour, and pneumonia
-
Paravertebral mass; differential diagnosis includes neurogenic tumour
CT (Fig. 19.45):

Intralobar lung sequestration. a Axial MIP reconstruction from CT angiography and b Coronal MIP reconstruction show left basal intralobar lung sequestration with venous drainage to the pulmonary veins (arrows and arrowheads). c Axial CT angiography image in the arterial phase shows direct arterial supply from the aorta (arrows)
-
Homogeneous mass with smooth margins
-
Mass effect
-
Intralobular:
-
Hyperinflation due to aeration through the pores of Kohn
-
Mucus-filled with rudimentary bronchi
-
-
Extralobular:
-
Soft tissue density mass with no connection to the bronchi
-
Strong, homogeneous enhancement
-
5.2 Treatment
Extralobar sequestration can be resected. Intralobar sequestration may be resected as part of segmentectomy or, depending on the size, lobectomy.
5.2 Congenital Emphysema
5.2 Aetiology and Epidemiology
Congenital lobar emphysema is caused by hyperinflation due to ball-valve mechanism obstruction of the afferent lobe bronchus. The obstruction may be due to various causes, such as inflammatory or congenital stenosis or compression by a mediastinal mass. Lobar emphysema is most common in the upper lobes and the middle lobe. Males are affected slightly more often than females. In half the cases, there are other associated anomalies.
5.2 Diagnosis
On chest X-ray as well as CT, there is an over inflated lobe with increased translucency and decreased vessel markings, mediastinal shift and compression atelectasis of the adjacent lobe.
5.2 Treatment
Treatment is by surgical excision of the affected lung lobe (lobectomy), which is also possible by means of bronchoscopy, if bronchial stenosis is not present.
5.2 Congenital Cystic Adenomatoid Malformation (CCAM)
5.2 Definition
This is a congenital malformation of the embryonic subsegmental bronchi with cystic formation, thereby proliferation of the epithelial tissue occurs at the expense of alveolar growth. Males are more commonly affected.
It is classified into three types according to Stroker:
-
Type I: multiple cysts, at least one > 2 cm, lined by columnar epithelium, compression may cause fetal hydrops and pulmonary hypoplasia
-
Type II: multiple cysts, < 1 cm, lined by ciliated epithelium
-
Type III: most rare form, not cystic, causes mass effect with mediastinal shift
5.2 Clinical Presentation
Usually leads to recurrent infections. In rare cases, the malformation is asymptomatic.
5.2 Imaging
Prenatal diagnosis is possible by ultrasonography.
Radiography:
-
Multilocular opacities < 1 cm with mediastinal shift
-
Large solitary cyst > 2 cm
-
Homogeneous opacity of the lung
-
Located in the left lower lobe
-
Associated findings: pneumonia, diaphragmatic hernia, or air-fluid levels.
5.2 Treatment
Although regression is possible, surgical excision should be performed, since there is a risk of malignant transformation.
5.3 Mediastinum
Malformations and variants may also occur in the mediastinum. For example, with situs inversus there is reversal of the positions of mediastinal structures. Other anomalies include pericardial cysts, bronchial cysts, and duplication cysts of the oesophagus.
5.4 Trachea
5.4 Tracheo-Bronchomalacia
5.4 Aetiology and Pathogenesis
Tracheo-bronchomalacia refers to softening of the tracheal cartilage, resulting in a deformity of the trachea. In most cases, the cause is trauma or chronic inflammation. In rare cases, there is a congenital defect in the connective tissue such as Ehler-Danlos syndrome. The most common cause is prolonged intubation, where increased deformability of cartilage is caused by the increased intraluminal pressure.
5.4 Diagnosis
The deformity is most manifest at the main bronchi. CT reconstructed images in a plane perpendicular to the main bronchi show the cross section of the main bronchi not as a rounded structure as expected, but rather as buttonhole shaped. On tangential images there is loss of the bronchial band-like shape, and the lumen of the affected bronchus shows a bulbous deformity. CT may be repeated in inspiration and expiration to compare the findings. Lateral chest radiographs show a decrease in the sagittal diameter of the trachea during expiration. The posteroanterior radiograph shows a saber-like trachea deviated to the right side.
5.4 Other Tracheobronchial Malformations
There are other abnormalities of the tracheobronchial system, all of which occur rarely.
Tracheal agenesis or complete absence of the trachea is in most cases not compatible with life.
Tracheobronchomegaly (Mournier-Kuhn syndrome) refers to abnormal dilatation of the trachea and bronchi during inspiration. The symptoms are variable but usually present with recurrent infections and nonproductive cough. The diagnosis can be made using radiographs during inspiration and expiration as well as complementary CT. A width of more than 3 cm is considered dilatation of the trachea, it is due to defective cartilage; the aetiology is unknown.
Tracheal stenosis is manifested by obstructive symptoms.
Another uncommon anomaly is atresia of a bronchus, which therefore has no or insufficient connection with the distal bronchial system. This leads to mucus retention and compensatory hyperinflation by a ball-valve mechanism or air diffusion through the pores of Kohn. Clinical symptoms occur rarely in childhood. On radiography, localised hyperinflation is typical, however, bronchial atresia may also manifest as localised opacity associated with distal hyperinflation. CT is the modality of choice for diagnosis.
Another anomaly of the tracheobronchial system is an aberrant bronchus, where the right upper lobe bronchus comes off directly from the trachea. Alternatively, an accessory bronchus arises from the trachea, which additionally supplies the right upper lobe bronchus. Mostly this is an asymptomatic incidental finding. With intubation, the lung supplied by this aberrant bronchus is at the risk of under ventilation and hence pneumonia or atelectasis.
A very rare anomaly is a bridging bronchus, referring to a bronchus that originates from the medial aspect of the left main bronchus and then crosses to the right in order to supply the right middle and lower lung lobes. In most cases there is associated bronchial stenosis.
6 Inflammatory Diseases
Inflammatory diseases of the lungs represent the most common indication for chest X-ray. The complexity of diagnosis of inflammatory diseases is due to the variable etiologies and the variable morphologic and radiographic appearances (Tables 19.13, 19.14 and 19.15).
6.1 Pneumonia
Pneumonia is defined as an infection of the lung by a pathogenic organism, resulting in lung consolidation.
Several classification systems for pneumonia may be used. In addition to the classification used below, pneumonias may also be classified; for example, by the site of infection.
CT plays a minor role in the primary diagnosis of pneumonia compared to conventional chest X-ray. Its main use is the diagnosis of complications such as abscess formation, or in the search for a predisposing underlying disease (e.g., tumour).
6.1 Lobar Pneumonia
6.1 Definition
Lobar pneumonia is a localised bacterial infection of the terminal airspaces.
6.1 Clinical Presentation
Acute febrile course with high temperature, cough, blood-tinged sputum, and pain. Lobar pneumonia progresses through stages in which the inflammatory, primarily intra-alveolar oedema spreads through the pores of Kohn, leading to rapid consolidation of the entire lung lobe. In acute illness, X-ray often shows the full extent of opacification.
With development of super-infection by other organisms, there is usually nonuniform consolidation that does not respect segmental boundaries. Multiple ill-defined opacities are seen with development of bronchopneumonia. The transverse Kerley B-lines appear thickened in the affected region due to thickening of the lymphatics and oedema of the interlobular septa. Clinical improvement of pneumonia is usually accompanied by a reduction in the opacity of the affected lobe with re-aeration. Resolution is often complete with return to normal lung architecture.
Factors that carry unfavorable prognosis include involvement of multiple lobes, pathogen detection in blood, and the presence of immune deficiency.
6.1 Imaging
CT of the chest:
-
Homogeneous opacification, strictly limited to lobar boundaries (Fig. 19.46)
Fig. 19.46a,b 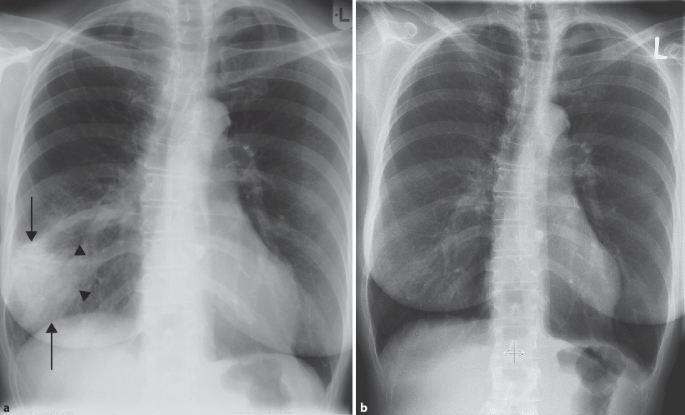
Lobar pneumonia, right middle lobe. a Chest X-ray posteroanterior view shows an opacity that is ill defined medially (arrowheads). b Complete resolution after antibiotic treatment
-
Positive air bronchogram
-
The affected lung lobe has normal volume
-
Complications: pleurisy, abscess, pleural empyema, septicaemia, chronicity (Fig. 19.47)
Fig. 19.47 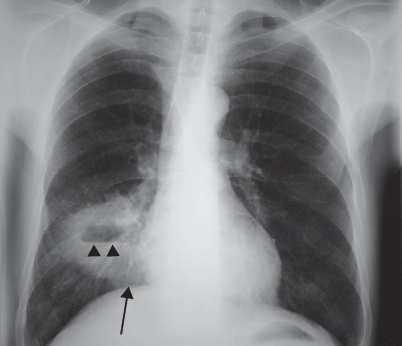
Right middle lobe pneumonia with abscess formation. Chest X-ray posteroanterior view shows an opacity with central radiolucency (cavitation) and a small air-fluid level (arrowheads)
-
DD: Atelectasis


6.1 Bronchopneumonia
6.1 Definition, Pathogenesis, and Clinical Presentation
Bronchopneumonia starts with localised infection of the terminal bronchioles by direct pathogen contact. The most common pathogens are Staphylococcus aureus and Gram-negative organisms. In the daily routine the most important classification of pneumonia would be on the basis of the underlying pathogen, which has a significant impact on management and prognosis. The clinical presentation is similar to that of lobar pneumonia.
6.1 Diagnosis
A definitive radiologic diagnosis of the causative pathogen is rarely possible. The primary role of conventional radiography is to verify the localisation of pneumonia, as well as potential complications such as pleural effusion, empyema, pneumothorax, atelectasis, and abscess formation.
CT scan of the chest:
-
Initially, there may be no changes visible
-
Increased bronchial thickening due to mucosal ulceration of the bronchial wall
-
Alveolar shadows, more in lung bases due to alveolar spread
-
No air bronchogram
-
Inhomogeneous contrast enhancement
-
Central break-down with abscess formation possible
Community-Acquired Pneumonia (CAP)
This refers to an acute bacterial infection, acquired in an otherwise healthy, nonhospitalised patient or 4 weeks after past hospitalisation. The pathogen spectrum varies with regional, seasonal, and demographic factors. The most common pathogen is Streptococcus pneumoniae, followed by Mycoplasma pneumoniae, and Haemophilus influenzae.
Antibiotic treatment is normally empirical, i.e., without prior sensitivity testing. In typical bacterial community-acquired pneumonia, penicillin G or macrolide treatment with allergy to penicillin are adequate. Atypical pneumonia as caused by Mycoplasma, Legionella, or Chlamydia requires antibiotic therapy with macrolides such as erythromycin or clarithromycin. Reserve drugs for infections with different pathogens are the quinolones.
Nosocomial Pneumonia
Treatment is started immediately after obtaining samples for antibiotic testing until receipt of the results of sensitivity test. Treatment is with amino-penicillin in combination with a beta-lactamase inhibitor, such as amoxicillin and clavulanic acid, and a third generation cephalosporin. Carbapenems and Teicoplanin are reserve antibiotics.
6.1 Interstitial/Atypical Pneumonia
6.1 Definition
It refers to inflammation of the interstitial lung tissue with virus or mycoplasma. Atypical describes the absence of the normally observed alveolar infiltrates in lobar or bronchopneumonia.
6.1 Clinical Presentation
Impressive is the discrepancy between the relatively mild clinical signs and the pronounced radiographic changes.
Differential Diagnosis
Typical versus atypical pneumonia
-
Typical pneumonia: fever > 38°C without prodromal symptoms, respiratory-related pain, and purulent discharge, laboratory parameters of inflammation with increased leucocytes and elevated ESR.
-
Atypical pneumonia: low-grade fever following previous symptoms such as rhinitis or otitis. Usually very little sputum, not purulent. Non elevated white blood cell count, only mildly elevated ESR.
6.1 Imaging
On chest X-ray there are usually bilateral, centrally located, linear shadows caused by widening of the interstitial septa and peribronchial interstitial thickening.
CT scan of the chest:
-
Diffuse, small nodular opacities, uncommonly coalesce into larger shadows
-
With resorption of infiltrates, thickening of interlobular septa
Virus-induced pneumonia is caused by different pathogens. The changes on conventional chest radiograph as well as CT are all unspecific.
6.1 Treatment
For treatment of a proven mycoplasma infection, macrolides and doxycycline are effective.
In children, pneumonia is commonly caused by respiratory syncytial virus or parainfluenza virus. In adults, the commonest pathogens are Adenovirus and flu viruses. Pneumonic infiltrates caused by cytomegalovirus occur in immune-compromised patients (HIV, leukaemia, immunosuppressive therapy). Radiologic diagnosis is important to follow the course.
Clinical presentation typically includes high fever, cough with or without sputum, as well as a substantial gap between auscultation and radiologic findings.
Chest radiograph:
-
Starting perihilar, reticulo-nodular shadowing, progressing into diffuse infiltrates
-
Diffuse ground-glass-like decrease in translucency can affect entire lobe
-
More basal distribution
-
Often accompanying pleural effusion
There is also a collar or cuffing sign due to the thickened bronchial wall.
6.1 Fungal Pneumonia
Mycotic pneumonia in patients without immune suppression is rare, common pathogens include Aspergillus fumigatus and Candida. There are a number of other fungal pathogens that can infect the lungs. The changes on X-ray or CT are usually nonspecific, so that a diagnosis is possible only by means of direct isolation of pathogens. Risk factors include persistent neutropenia < 500/μl, graft-versus-host disease, long-term corticosteroid therapy, immunosuppressive therapy, or AIDS.
The European Organisation for Research and Treatment of Cancer has revised the definitions of invasive fungal disease. Fungal infection is “proven” when the fungus is directly identified at histopathology or culture. Fungal infection is “probable” when there is combination of one host factor, one clinical criterion, and one mycological criterion. Cases that meet the criteria for a host factor and a clinical criterion but for which mycological criteria are absent are “possible” fungal infections.
6.1 Candidiasis
Candida albicans is a fungus that is found in small numbers in healthy individuals in the stool or oropharynx. In immune-compromised patients, it can lead to exacerbation and invasive infection. Two forms of infection are present: mucocutaneous and systemic forms.
Thrush is the visible oral and esophageal infection with formation of whitish deposits, and is often the first sign of HIV infection. In severe cases, with significant immune suppression, haematogenous spread of candida may occur with generalised involvement of the visceral organs such as the kidneys, liver, or the endocardium. Candida pneumonia occasionally occurs as a complication of Thrush.
6.1 Diagnosis
Candida can be directly identified in bronchial secretions or lung tissue. An indirect evidence of infection is by antibody detection using the Candida haemagglutination test.
X-ray: With haematogenous spread, there are multiple pulmonary lesions without a specific distribution pattern.
CT: a characteristic sign of the fungal lesions is the surrounding ground-glass halo. The bronchogenic manifestation appears as bronchopneumonic infiltrates.
The final diagnosis when candida infection is suspected is made by culturing the pathogen from sputum or transbronchial biopsy.
6.1 Aspergillosis
Aspergillus infection usually occurs through inhalation. The fungus is widespread and can also affect healthy individuals. The manifestations depend on the immune status and may be in the form of allergic bronchopulmonary aspergillosis, aspergilloma localised in a pre-existing cavity, or invasive pulmonary aspergillosis (. Figs. 19.51 and 19.52 ).

Legionella pneumonia in evolution. Chest X-ray posteroanterior view. a Initially there is poorly defined opacity in the middle left lung zone. b Acute clinical phase: nearly homogeneous opacity of the middle and lower zones of the left lung. c Intensive care phase: diffuse confluent infiltration of the left lung, infiltrates start to appear on the right side also

Migratory eosinophilic infiltrates. a Chest X-ray shows right middle zone infiltrates. b Infiltrates appear to “migrate” to the lower zone on follow-up X-ray

Histoplasmosis. Chest X-ray posteroanterior view shows micronodular disseminated calcifications (arrows)

Aspergilloma. a Chest X-ray shows a nodular lesion in the left upper lung zone with a surrounding air halo. b Axial CT image in lung window confirms the radiographic appearance and shows replacement of lung parenchyma by the cavitary lesion with soft tissue density and surrounding air halo

Aspergillosis. a Chest X-ray shows multifocal small rounded nodular lesions mainly in the middle lung zones. b Axial CT image in lung window confirms the radiographic appearance and shows multiple nodules with ill-defined borders
6.1 Invasive Pulmonary Aspergillosis
Invasive pulmonary aspergillosis usually occurs only in immune-compromised individuals, with invasion of small vessels and erosions of large intrapulmonary vessels with associated embolism.
Diagnostic signs are:
Chest X-ray:
-
1–2 cm nodules with haemorrhagic halo (Fig. 19.52a)
-
Accompanying bronchopneumonic opacities
-
With embolic infarcts wedge-shaped areas of translucency
CT (Fig. 19.52b):
-
Small nodules with surrounding ground-glass-like opacity (halo)
-
In advanced stages, the nodules become confluent
-
Central breakdown of the nodules with cavity formation containing an air crescent
-
Rarely enlarged lymph nodes
-
No positive air bronchogram
-
Associated pleural effusion in few cases only
6.1 Aspergilloma (Fig. 19.51)
Aspergilloma is a fungus ball formed of fibrin-glued hyphae that occurs in pre-existing cavities or bronchiectasis. This presents as a homogeneous round opacity with a fine air crescent rim in contrast to the cavity wall. There is surrounding pleural thickening. Clinically, it is often asymptomatic, but may present with haemoptysis.
6.1 Allergic Bronchopulmonary Aspergillosis (ABPA)
Allergic bronchopulmonary aspergillosis is an allergic reaction related to pre-existing asthma. The immune response results in proteolytic destruction of the lung parenchyma with bronchiectatic changes. The morphologic picture is based on alternating infiltrates and lobar consolidations, thickened bronchial walls up to central bronchiectasis, hypoventilation, fibrous changes, and signs of emphysema. The blood picture shows eosinophilia.
6.1 Treatment
The cause should be removed, if known and possible, such as an infected intravenous indwelling catheter. The immune status should be improved. The drug therapy consists of fluconazole or amphotericin B. The treatment should continue for at least 2 weeks beyond eradication.
6.1 Cryptococcosis
6.1 Pathogenesis and Epidemiology
Cryptococcus neoformans is a yeast fungus found in the soil and in bird droppings. Infection is by inhalation and will initially involve the lungs. Haematogenous dissemination can lead to meningoencephalitis, a condition that is fatal without treatment. Cryptococcosis affects about 5% of AIDS patients and is more prevalent in the U.S. than in Europe.
6.1 Clinical Presentation
Lung infection presents with a picture similar to atypical pneumonia with cough, pain with respiration, and scanty expectoration. When cerebral infection occurs, the manifestations include headache, fever, and progressive impaired consciousness associated with cranial nerve palsy.
6.1 Diagnosis
CT: the picture is variable, depending on the immune status of the patient:
-
Small, peripherally located, nodules in the immunosuppressed
-
Confluent infiltrates, usually limited to one lobe, but crossing segmental boundaries
-
Cavitation is rare
-
Identification of the fungus in bronchoalveolar lavage is often necessary for diagnosis.
For diagnosis of cerebral infection, increased intracranial pressure signs should be excluded with MRI and fundoscopy, and then lumbar puncture should be performed. Occasionally the pathogen may be isolated from blood culture.
6.1 Mucormycosis
Mucormycosis, sometimes also called zygomycosis, are fungi that belong to the Mucorales group. The fungi are widespread and are transmitted via air. Infection of the nasal cavity causes a spreading destructive infection of the paranasal sinuses. Furthermore, haematogenous spread and intestinal colonisation are possible. Pulmonary infection is almost always seen in patients with leukaemia or lymphoma. With generalised infection, the prognosis is usually poor, with mortality rates up to 90% according to the literature. The reported mortality rate of pulmonary infection is up to 65%.
6.1 Clinical Presentation
Pulmonary infection manifests with chest pain, fever, and blood tinged sputum. A complication of infection is the invasion of pulmonary vessels which leads to aneurysm formation.
6.1 Imaging
CT:
-
Preference for the upper lobes, with diffuse, rounded lesions with rapid progression in sizes (Fig. 19.53)
Fig. 19.53a,b 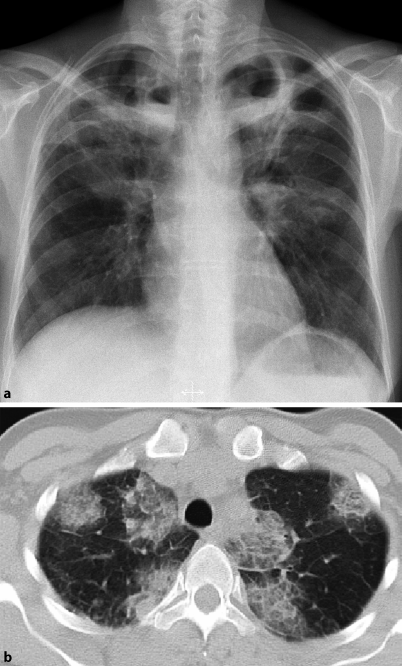
Mucormycosis. a Chest X-ray shows multiple confluent and cloudy opacities, mainly in the upper lung zones, with early central cavitation. b Axial CT image in lung window shows internal structure similar to a bird’s nest
-
Central cavitation with air crescent
-
Internal structure similar to a bird’s nest (Fig. 19.53)
-
Frequently pleural based
-
Surrounding halo
-
Only rarely enlarged lymph nodes

6.1 Pneumocystis carinii (Pneumocystis jirovecii pneumonia)
Pneumocystis carinii is a fungus that was first discovered by Chagas, and belongs to the Ascomycetes. Pneumocystis pneumonia was, until recently, the most common opportunistic infection in HIV patients. It is nowadays only seen in patients with CD4 counts < 400.
Pneumocystis carinii pneumonia (PCP) is commonly the first manifestation of HIV infection.
6.1 Clinical Presentation
Typical manifestations include progressive exertional dyspnea and partial respiratory insufficiency. Elevation of the serum lactate dehydrogenase (LDH) is a sensitive parameter that has a prognostic value as the level of LDH correlates to the severity of disease. In children, the infection often has an acute course. Definitive diagnosis is by identification of the pathogen in bronchoalveolar lavage.
6.1 Imaging
Chest X-ray: At the beginning, the X-ray is often unremarkable. Later on, there is a reticulo-nodular pattern, followed by ground-glass opacities, alveolar infiltrates that spread from the hila to the basal and apical parts of the lungs with sparing of the costophrenic recesses (Fig. 19.54). In advanced stages there are diffuse opacities of the lung fields.

Pneumocystis carinii pneumonia. a Chest X-ray shows interstitial infiltrates with thickened septal lines and relative sparing of the costophrenic recesses. b Coronal CT reconstructed image in lung window shows interstitial ground-glass infiltrate as well as intra-alveolar infiltrate (arrows)
CT: has a higher sensitivity for early detection. Signs include:
-
Ground-glass, perihilar opacities, due to intra-alveolar shadowing
-
Interstitial infiltrates with thickened septa
-
Sparing of the costophrenic recesses
-
With associated immunosuppressive disease, extensive consolidation with positive air bronchogram
-
After treatment, fibrotic; strand-like scarring is possible
-
Occasionally, enlarged lymph nodes, or pleural effusion
6.1 Treatment
The drug therapy of choice for PCP infection is cotrimoxazole. With allergy or resistance to cotrimoxazole therapy, pentamidine may be used.
6.1 Tuberculosis
6.1 Definition and Pathogenesis
Tuberculosis is one of the most common infectious diseases in the world. It is caused by infection with the widespread mycobacteria. The main causative agent is Mycobacterium tuberculosis. The definitive diagnosis can be made by Ziehl-Neelsen staining of patient’s secretions. When grown in culture media, the culture period is about 4 weeks.
It is transmitted as a droplet infection from person to person. People at risk are contacts with reduced, weak immune systems, such as children and the elderly or people with underlying conditions such as HIV or undergoing immunosuppressive therapy. The infection is also largely dependent on social factors; it occurs more frequently in mass shelters such as prisons or camps. Other important factors include drug abuse, alcoholism, and poor nutritional status.
6.1 Clinical Presentation and Diagnosis
The course of tuberculosis is divided into different stages as noted below.
Primary Tuberculosis
Primary tuberculosis refers to the first infection of an individual with the mycobacterium. The inhaled bacteria are phagocytosed by alveolar macrophages. Through an insufficient defense system, intracellular growth of the bacteria occurs with lysis of the macrophages. This leads to an accumulation of intra-alveolar inflammatory cells, known as Ghon’s focus, usually in the right upper lung lobe (see Fig. 19.59). This appears as a small ill-defined infiltrate, associated with hilar lymphadenopathy, as well as central reticular opacities representing lymphangitis. The combination of Ghon’s focus and hilar lymph nodes is also termed Ranke complex.

Schematic representation of primary tuberculosis complex

Tuberculous bronchiolitis. Axial CT image in lung window shows bronchiolitis with associated consolidation (arrows)

Tuberculosis. Axial CT image in lung window shows tuberculous cavity with thick walls (arrows)

Miliary tuberculosis. Axial high-resolution CT image shows ill-defined micronodules (arrowheads)

Ghon’s focus. Chest X-ray shows a small calcified nodular opacity with unsharp borders in the left lung apex (arrows)
With normal immune status, the process eventually starts healing with local scar formation and a granuloma with central necrosis. Radiographically, this appears as rounded calcification (tuberculoma) and enlarged lymph nodes (primary complex) (Fig. 19.55). If such a tuberculoma is present in the apical segment of the upper lobe, it is also called a Simon focus.
A tuberculin test (Mendel Mantoux) is first positive only after about a month. With poor immune status, primary tuberculosis may progress to haematogenous dissemination and manifest as miliary tuberculosis in different organs (Fig. 19.58).
Postprimary Tuberculosis
Postprimary tuberculosis can only occur after an initial infection has taken place. It develops with poor immune status as a reactivation of the primary complex, so that it is more common in the upper lobes. The diagnosis is often an incidental finding, since the symptoms are nonspecific and mild at the beginning. Symptoms include fatigue, persistent cough, and low-grade fever with occasional night sweats. Lymph node enlargement is seen less commonly in immune competent patients, but in > 50% of HIV-positive patients.
The reactivated primary complex can locally progress and spread by continuity into caseating pneumonia. Small, caseating nodular infiltrates are called Assmann infiltrate and represent a form of open tuberculosis. Furthermore, mycobacteria are transported to regional lymph nodes leading to lymphadenitis. Depending on the immune status, this may lead to septicaemia. Other manifestations are bronchial spread, sometimes with cavitation (Fig. 19.57). Bronchial tuberculosis spreads by continuity and affects the bronchial mucosa. This form of tuberculosis is also a form of open tuberculosis. Cavitation occurs with necrosis of the lung parenchyma, and contact with a bronchus. Thick-walled cavities may occasionally contain liquefied tissue material, which can be seen on radiography and CT as air-fluid levels.
A life-threatening complication is infection of the pulmonary arterial wall with pseudoaneurysm formation (Rasmussen aneurysm), which may lead to severe haemoptysis.
Haematogenous spread leads to miliary tuberculosis; multiple small lesions, about 1–2 mm in size, diffusely scattered with decrease in size from lung apex to base. Tuberculous pleurisy is usually large and unilateral, but generally indistinguishable radiologically from other causes of pleural effusion. Landouzy sepsis refers to haematogenous dissemination to other organs, particularly the bone, which usually has a fulminant course.
The lung tissue affected by tuberculosis heals with scarring. On X-ray there are upper lobe linear opacities, radiating from the hilum towards the apex. The hilum is displaced upwards due to fibrosis (rail track sign). Traction bronchiectasis may also be seen, as well as total fibrosis of an entire lobe with compensatory hyperinflation of the remaining lung. In elderly patients with old tuberculosis infection before the era of antibiotic therapy, the post-healing changes are severe on chest X-ray. Surgical manoeuvres were common for treatment of tuberculosis before the antibiotic era, cavities were treated by plombage with oil or thoracoplasty, surgical resection of the affected lung sections with the adjacent structures of the chest wall.
6.1 Treatment
Treatment of tuberculosis consists of a combination of antituberculosis drugs. Treatment is for at least 3 months with isoniazid, ethambutol, and rifampicin. Ethambutol or rifampicin may be replaced by streptomycin. With drug resistance, reserved drugs include prothionamide, ciprofloxacin, capreomycin, and para-aminosalicylic acid. Treatment is afterwards continued with a combination of isoniazid and rifampicin for a further 6–9 months. Miliary tuberculosis or meningitis are treated with a quadruple combination. Treatment is followed by prednisone for 9–12 months. In severe cases with cavity formation, surgical resection may be necessary.
Atypical Mycobacteria
The most common is intracellular mycobacterium avium. The infection is transmitted by inhalation or ingestion from the environment. Atypical mycobacterial infections occur mostly in immune-deficient patients or individuals with compromised lungs. The clinical presentation is usually nonspecific with weight loss, fatigue, and low-grade fever.
Mycobacterial infection in immune-competent individuals appears on X-ray as sharply circumscribed nodules, rarely > 1 cm, scattered throughout the lung, with the so-called “tree in bud” sign. In patients with immune deficiency, there can be rapidly progressive diffuse opacities. In general, the appearance is variable. The differentiation of atypical from typical tuberculosis may not be possible. However, the lack of response to standard therapy may be suggestive.
6.1 Parasites
6.1 Echinococcosis
The commonest infections are with Echinococcus granulosus or cysticus (dog tapeworm) and Echinococcus alveolaris or multilocularis (fox tapeworm). The larvae of E. granulosus settle in the liver in two-thirds of cases and in the lungs in one third. In addition, the CNS, spleen, and kidneys may be affected. The larvae of E. multilocularis settle almost 100% in the liver, although they may grow and spread secondarily to other organs.
6.1 Clinical Presentation
The infection usually remains occult. Only large hydatid cysts can cause compression symptoms or cyst rupture in the lung causing symptoms such as coughing.
6.1 Diagnosis and Imaging
Serology reveals eosinophilia. Furthermore, specific antibodies may be detected by Elisa or indirect haemagglutination test. Cross-reactions between the different types are possible. Because the tests are not positive in all cases, different methods should be combined.
Ultrasound: E. granulosus infestation appears as a smooth-bordered cystic lesion with some calcifications. Incorporated in some cases, the echinococcal membrane is visible together with daughter cysts. The E. multilocularis cyst appears as a cyst with irregular borders and partial calcifications.
Chest X-ray:
-
Solitary, smooth-bordered nodule of variable sizes (Fig. 19.60.)
Fig. 19.60 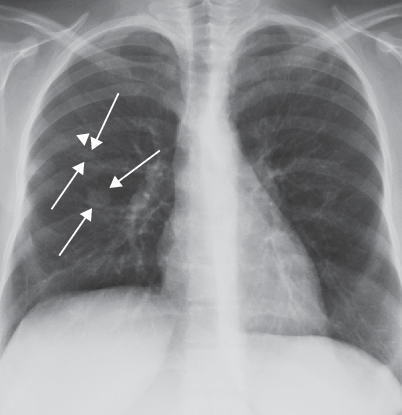
Echinococcosis. Chest X-ray posteroanterior view shows a well-circumscribed, smooth, rounded lesion in the right middle lung zone with central radiolucency (arrows). Another smaller lesion is seen cranially (arrowhead)
-
Rarely, one sees the so-called meniscus sign, in the form of an air crescent between the lung and the hydatid membrane
-
After rupture of the hydatid cyst, the membrane can be seen floating on the air-fluid level

6.1 Treatment
The treatment of E. granulosus is surgically when possible. If surgery is contraindicated or not possible, the instillation of highly concentrated alcohol in combination with albendazole is possible. Infestation with E. multilocularis is treated by a long course of high-dose mebendazole or albendazole.
6.1 Ascariasis
The parasitic roundworm Ascaris lumbricoides has a world-wide distribution. They are transmitted by ingestion of eggs in food contaminated with human feces. The parasites live as larvae in the small intestine, pass through the intestinal walls and the mesenteric veins into the liver, and then spread across the bloodstream into the lungs, where they penetrate the alveolar walls and cause an eosinophilic infiltrate (Loeffler infiltrate). In the alveoli, the ascaris larvae migrate through the lung to the trachea where they are coughed-up and then re-swallowed thus reaching the jejunum. In the jejunum they mature into adult form that produces eggs daily in its reproductive phase.
6.1 Clinical Presentation
A low-grade infestation is often symptomless. Elimination of the worm is then often the first sign of infestation. Heavy infestation causes allergic reactions to the metabolic products of the worms or local symptoms such as vomiting, ileus, or biliary tract obstruction.
6.1 Diagnosis
Serology reveals an intermittent eosinophilia. Chest X-ray reveals multiple recurring or migratory opacities.
6.1 Treatment
Treatment is by administering mebendazole for 3 days or pyrantel in a single dose. Then the dead worms are excreted naturally.
6.1 Mendelson’s Syndrome
6.1 Definition and Pathogenesis
Mendelson’s syndrome is the aspiration of gastric juice. This may be caused or promoted by anesthesia or unconsciousness, elevated diaphragm, swallowing disorders in scleroderma, pregnancy, diverticula, etc. The aspirated acidic gastric juice leads to a chemical irritation of the respiratory epithelium and spasm of the small airways. This leads to pulmonary oedema and secondary infection of the compromised lung tissue. Recurrent aspiration can cause granulomatous and fibrotic changes of the affected lung parenchyma.
6.1 Clinical Presentation
Occasionally the direct aspiration episode is unnoticed. After about 6 hours, bronchospasm becomes evident with hypersecretion, dyspnea, cyanosis, and low-grade fever. Auscultation reveals pronounced coarse bubbly crepitations.
6.1 Diagnosis
At the beginning, the chest X-ray may be unremarkable. Later on, there may be atelectasis and an infiltrate, more in the right lower lung lobe. Blood gas analysis reveals reduced pO2 with elevated pCO2 and acidosis in advanced stages.
6.1 Treatment
If possible, the aspirate should be sucked-out in a head-down position. Drug treatment is with bronchiolytics, glucocorticoids, oxygen, and broad-spectrum antibiotics, which should also cover gram-negative and anaerobic bacteria.
6.1 Pneumonitis
Pneumonitis is an interstitial inflammation of the lung tissue, which is not caused by infectious agents, but rather by chemical or physical irritants, or irradiation.
6.2 Bronchiectasis and Associated Conditions
6.2 Bronchiectasis
6.2 Definition and Pathogenesis
Bronchiectasis is dilatation of medium and small bronchi, usually associated with inflammatory changes in the bronchial wall and surrounding tissue. Bronchiectasis may be localised or diffuse and the changes are irreversible in contrast to the reversible temporary bronchial dilatation that may accompany pulmonary infections.
The pathogenesis of bronchiectasis is complex, and numerous causes are implicated. Pathophysiologically there is weakening of the bronchial walls and an increased intramural pressure. The commonest aetiology is recurrent or chronic inflammatory diseases. Bronchiectasis acquired in early childhood is caused by pulmonary infections, including viral infections, with accompanying bronchiolitis. In adulthood, bronchiectasis may be caused by numerous etiologic bacterial and mycotic (tuberculosis, nontuberculous mycobacteria) infections or due to aspergillosis. Other predisposing factors include cystic fibrosis, the “immotile cilia syndrome,” and severe immune deficiencies. Moreover, other factors include past aspiration of acidic gastric contents, allergic bronchopulmonary aspergillosis, and inhalation of toxic gases. Interstitial pulmonary fibrosis can induce secondary traction bronchiectasis. Obstructive bronchiectasis results from bronchial stenosis due to endobronchial tumours and foreign bodies.
6.2 Morphology
Bronchiectasis can be classified according to morphologic appearance into cylindrical, varicose, and saccular/cystic forms (Fig. 19.61).

Schematic representation of the different forms of bronchiectasis
Classification of bronchiectasis
-
Cylindrical bronchiectasis :
-
The commonest acquired form
-
As a rule from the 6th–10th bronchial generations
-
Frequently bilateral basal and dorsal
-
No bronchial tapering towards periphery
-
Bronchi end abruptly
-
-
Varicose bronchiectasis :
-
Beaded form
-
Alternating dilatation and focal scar narrowings
-
More marked ectasia and peribronchial changes than the cylindrical form
-
-
Saccular/cystic bronchiectasis :
-
Advanced form
-
Ballooning dilatation
-
Can involve all lung sections
-
Often associated with bronchial stenosis
-
The number of bronchial bifurcations is significantly reduced
-
Usually limited to the 4th and 5th bronchial generations
-
The differentiation of bronchiectasis into congenital or acquired appears no longer useful because different etiologies cannot be differentiated based on the morphology. Severe forms of bronchiectasis can produce bronchiectatic honeycomb lung. In contrast to the different morphologic forms of bronchiectasis, histopathologically bronchiectasis may be lymphofollicular, hypertrophic, or atrophic.
6.2 Clinical Presentation
The symptoms are nonspecific:
-
In severe bronchiectasis expectoration of large amounts of sputum
-
Commonly recurrent bronchopulmonary infections with or without sputum
-
Recurrent haemoptysis
-
Often mixed infection with Aspergillus
-
Focus for septicaemia and haematogenous abscesses
-
In advanced stages, dyspnea at stress and rest with development of Cor pulmonale
6.2 Diagnosis
Laboratory tests and pulmonary function tests do not provide definitive diagnosis. Imaging plays an important role in the diagnosis and follow-up of the course of the disease.
Imaging.
Chest radiography is still the basic examination for diagnosis and follow-up. Conventional tomography nowadays plays no role, and bronchography, the once gold standard for diagnosis of bronchiectasis, is today rarely used. The invasiveness of the procedure and the need for introducing a bronchial catheter and sedation of patients and the lack of opacification of bronchi distal to obstructive lesions are all limitations of the procedure. The imaging technique of choice today is CT, which has replaced the other methods.
Chest X-Ray.
The sensitivity of the chest radiograph is generally low; however, severe changes induce characteristic findings that allow the diagnosis:
-
Thickened bronchial walls as thin, single or parallel lines; tram-track sign.
-
Ring air-filled shadows with a diameter of 5–20 mm when seen end-on. Mucus-filled bronchi appear as nodules, air-fluid levels appear with incomplete filling.
-
Band-shaped shadows with a width of shading 5–10 mm and several centimetres in length, which are divided at the periphery into a y-shape.
Unspecific associated signs should also be recognised. The pulmonary vessels are increased in size, peribronchial fibrosis often with dystelectasis, which leads to a displacement of fissures. These findings are nonspecific and may be seen with other parenchymal lung diseases. In the generalised forms of bronchiectasis, as with cystic fibrosis or mucociliary dyskinesia, the rest of the lung is hyper inflated.
Criteria of an exacerbation include additional diffuse opacities and patchy consolidations and signs of retention of secretion.
Radiographic criteria of pulmonary hypertension or cor pulmonale may be seen with persistent chronic disease.
Special Type of Bronchiectasis: Mucocele
A mucocele is a mucus-filled dilated bronchus (Fig. 19.62). This appears as a nodule when seen end on, but when the X-ray is tangential it appears as a band arising from the hilum and branching in the periphery. With incomplete mucus filling, an air-fluid level can be visible.

Mucocele. Chest X-ray posteroanterior view shows mucus-filled bronchiectasis in the right and left lower zones (arrows)
CT Diagnosis of Bronchiectasis.
The sensitivity and specificity of CT for diagnosis of bronchiectasis is highly dependent on the selection of the examination protocol. With a thick section scan (8–10 mm), the sensitivity is only 60–80% and the specificity is 90–100%. Therefore, the technique of choice has been the high-resolution HR-CT with 1–2-mm thick layers reconstructed with a high-resolution, edge-sharpening algorithm. With this technique the sensitivity increased to > 95% with a specificity of 93–100%. A suggested protocol for HR-CT is 1.5 -mm thick sections reconstructed with high-resolution algorithms, with a slice gap of 10 mm from the apex to the base, with a matrix of 521 × 512 pixels, and a rotation time of maximum 1 second.
Multislice CT (MSCT) has revolutionised HR-CT imaging of the lungs with thin isotropic sections enabling excellent multiplanar reconstructions. The course and the calibre of the bronchi can be followed, starting from the level of tracheal bifurcation until well into the lung periphery. Because there are no “normal” values for bronchial width, comparison to the contralateral side, as well as to the size of the accompanying pulmonary artery are crucial for the diagnosis of bronchial dilatation. In healthy individuals, it was shown that mild dilatation of the bronchi occurs in up to 26%, with considerable interindividual variability. The diagnosis of bronchial dilatation becomes problematic in patients with enlarged pulmonary arteries, as in pulmonary arterial hypertension or volume load from left to right shunts. Conversely, oligemia is associated with small-sized arteries. It is therefore important to evaluate the second diagnostic criterion, the lack of tapering of the bronchi as well as the third criterion, detection of bronchi in the peripheral third of the lungs.
Diagnostic CT criteria of bronchiectasis are:
-
Dilation of the bronchus in relation to the accompanying pulmonary artery
-
Lack of tapering of the bronchi
-
Detection of bronchi in the peripheral third of the lung
Note: In terms of differential diagnosis, attention should be paid to assessment of the bronchi in the lingual, where the pulsation of the heart and major vessels may result in a double wall appearance simulating bronchiectasis.
On CT, cylindrical bronchiectasis appears as a relatively uniform bronchial dilatation. The most important criterion is the abrupt termination of the bronchiectatic dilatation, as well as the associated changes such as thickened bronchial walls. The latter sign is commonly seen without bronchiectasis in the presence of bronchiolitis. The beaded bronchi of varicose bronchiectasis may be diagnosed by appropriate image reconstructions, especially in the coronal plane. The pronounced changes on CT allow the diagnosis of cystic or saccular bronchiectasis, where individual bronchi appear as cystic masses. Bronchocele or mucocele is dilated bronchus filled with retained secretions.
Besides the detection and morphologic evaluation of bronchiectasis, CT may allow the diagnosis of the cause of secondary bronchiectasis. Active search should be made for endobronchial tumours such as carcinoid tumours, bronchial carcinoma, incarcerated foreign bodies, or fibrotic lung parenchymal changes.
The differential diagnoses of cystic bronchiectasis with air-fluid levels are processes presenting with cavitating nodules. The most important criterion is the thickness of and the smoothness of the bronchial wall.
The radiologic evidence of bronchiectasis may not match the clinical picture of the disease. A conventional chest radiograph can only show advanced disease changes and is suitable for clinical monitoring. CT is the diagnostic method of choice, allowing the differentiation of cylindrical, varicose, and cystic bronchiectasis as well as narrowing of the etiologic differential diagnoses and accurate detection of complications.
6.2 Treatment
Treatment includes the inhalation of mucolytic drugs with bronchial and respiratory exercises. Early antibiotic therapy for respiratory infections is necessary. Haemoptysis may be treated by embolisation. In severe bronchiectasis with strict segmental localisation, surgical resection may be considered.
6.2 Cystic Fibrosis
6.2 Definition and Pathogenesis
Etiologically this is an autosomal recessive disease transmitted on the long arm of chromosome 7 with an incidence of 25:1000 individuals in Germany. It leads to bronchiectatic changes of the whole lungs, progressive loss of lung parenchyma, and eventually respiratory insufficiency.
The cause is a defect in the CFTR gene (cystic fibrosis transmembrane conductance regulator gene), which causes abnormal chloride transport and leads to changes in secretion of various exocrine glands. Normally, sodium is absorbed actively along a gradient through a highly selective ion channel. Intracellular sodium is transported to the extracellular fluid via the Na/K pump. Concomitantly, the transport of chloride ions occurs. Furthermore, chloride may be eliminated via selective channels. Because of the defective CFTR protein, chloride transport is hindered. There is intracellular accumulation of chloride ions. Consecutively, sodium and water are transported into the cell to maintain the electrochemical equilibrium. This results in thickened, highly viscous secretions that block the glands’ ductules with development of cystic degeneration and fibrosis.
In the lungs, the thick viscid airway secretions result in impaired mucociliary clearance, which favors chronic bacterial colonisation and recurrent infections. In most patients suffering from cystic fibrosis, there is also exocrine pancreatic insufficiency.
6.2 Clinical Presentation
The symptoms are characterised by secretion retention in the glandular tissue of various organs or increased sweating. In addition:
-
Recurrent sinusitis and polyps in the paranasal sinuses
-
Purulent sputum due to recurrent bronchitis
-
Colonisation with Pseudomonas results in green-coloured sputum
-
Abnormal small and large intestine secretion with consecutive diarrhoea or constipation
-
In neonates meconium ileus due to thick viscid meconium
Furthermore, cystic fibrosis leads to poor weight gain and growth. In the lungs, usually a rapidly progressive form of bronchiectasis occurs with a barrel chest leading to progressive exertional dyspnea up to orthopnea. In the advanced stage, breathing is almost only possible using the accessory respiratory muscles. In men, infertility is common due to obstruction of the ductus deferens, and in women; reduced fertility due to abnormal cervical secretions.
Diagnosis
Sweat test by the Gibson and Cooke procedure: Stimulation of sweating is performed on the inside of the forearm by applying pads soaked with pilocarpine and with a DC electric current applied to drive the pilocarpine into skin sweat glands increased sweating is induced. The sweat is collected on filter paper and analysed. In cystic fibrosis, there is increased chloride and sodium ion concentration. For verification, a second test is necessary. Additionally, genotyping can be performed.
Pulmonary function tests show an obstructive lung disease with increased airway resistance and reduced FEV1. In the presence of tachypnea, blood gas analysis reveals hypoxemia.
6.2 Imaging
Chest X-ray findings:
-
Interstitial thickening and fibrosis up to a honeycomb pattern obscuring normal vascular and bronchial markings (Fig. 19.63)
Fig. 19.63a–c 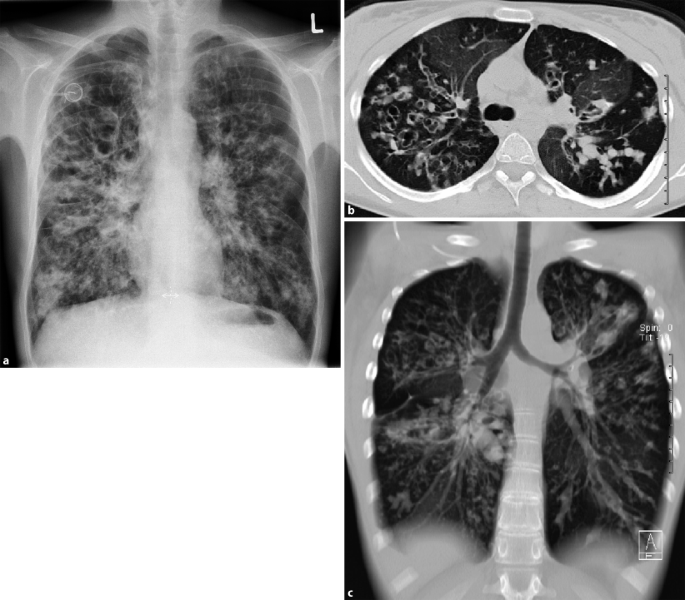
Cystic fibrosis. a Chest X-ray shows interstitial fibrous reticular markings with honeycombing, obscuring the normal vascular/bronchial markings. b Axial CT image and c Coronal reconstructed CT image in lung window confirm the presence of interstitial reticular fibrosis combined with bronchiectatic changes and honeycombing
-
Associated atelectasis
-
Progressive barrel chest

CT findings:
-
Thickened bronchial walls
-
The so-called “tree-in-bud” sign; small centrilobular nodular and branching linear opacities
6.2 Monitoring of Cystic Fibrosis
The Chrispin-Norman radiologic scoring system is widely used to assess respiratory disease progression in cystic fibrosis. The lungs are divided into four quadrants, which are separately assessed for different criteria and given a score (Table 19.16). Subjective score points are added and the total score is calculated.
6.2 Treatment
There is no definitive treatment for cystic fibrosis. The focus is on preservation of organ functions. Adequate energy intake is important to compensate for increased respiratory activity. A special diet must be followed because of malabsorption due to defective pancreatic enzymes. Enzyme replacement and special fat-soluble vitamins may be necessary.
In the treatment of pulmonary involvement, mucus-thinning drugs and bronchodilators are given. Chest exercise and physical therapy are helpful to facilitate expectoration. With infections early high-dose antibiotic therapy is important. In advanced stages, oxygen therapy is indicated to reduce pulmonary hypertension and decrease cardiac stress. The last alternative is lung transplantation and should be considered before more serious damage to the heart occurs.
Chronic Pulmonary Hypertension
This is defined as a persistent increase in the pulmonary artery pressure > 20 mmHg on average, at rest. The pressure is determined by the resistance in the pulmonary blood vessels, the pressure in the left atrium and the cardiac output. The causes of pulmonary hypertension are diverse. It may be idiopathic or primary pulmonary hypertension. Drugs such as amphetamines, as well as collagen diseases, skeletal chest deformity, postpneumonectomy are all causes of pulmonary hypertension. Advanced destruction of the lung parenchyma or recurrent pulmonary embolism leading to hypoxia, in turn cause increased pulmonary arterial pressure via the Euler-Liljestrand reflex.
The clinical presentation is nonspecific at the beginning. There is fatigue, sinus tachycardia, and exertional dyspnea. The advanced stage is characterised by progressive right cardiac decompensation with congested neck veins, oedema, and ascites. Pulmonary pressure measurement can differentiate a latent and manifest form of pulmonary hypertension (Cor pulmonale). Latent pulmonary hypertension is characterised by a mean pulmonary pressure at rest of < 20 mmHg (i.e., no increase), only with exercise does the pressure rise to < 30 mmHg. Manifest pulmonary hypertension is characterised by a pulmonary mean pressure that is increased even at rest to > 20 mmHg. Right heart failure is diagnosed when the mean right atrial pressure is increased at rest to > 9 mmHg.
Treatment approaches include treatment of the cause, for example obstructive lung disease or recurrent pulmonary embolism. Symptomatic oxygen therapy may be indicated for chronic hypoxia to reduce pulmonary arterial pressure. Drug treatment includes the administration of inhaled prostacyclin derivatives for pressure reduction.
6.2 Ciliary Dyskinesia Syndrome
Ciliary dyskinesia syndrome is one of the specific etiologic factors for the development of bronchiectasis. It is an inherited autosomal recessive disease with a defect in chromosome 5p15-p14, which results in impaired mucociliary clearance. This leads to recurrent infections of the upper and lower respiratory tract. The changes are not so marked in comparison to cystic fibrosis.
The so-called Kartagener syndrome is a subtype of ciliary dyskinesia, with situs inversus, sinusitis, and bronchiectasis (Fig. 19.64). The syndrome is inherited as autosomal recessive with an equal sex distribution and prevalence of 1:2000. Bronchiectasis occurs in adolescence and preferentially involves the middle lobe and the lingula.

Ciliary dyskinesia (Kartagener syndrome). Chest X-ray shows situs inversus and paracardiac bronchiectasis (arrows)
6.2 Diagnosis
Definitive diagnosis is made via biopsy of the nasal or bronchial mucosa and demonstration of the motility and structure of the cilia.
6.2 Treatment
Treatment is similar to cystic fibrosis. Mucolytics and bronchodilators can be administered by inhalation. In addition, an early and aggressive antibiotic therapy for infections is important.
6.3 Acute Bronchiolitis
6.3 Definition and Aetiology
Bronchiolitis is a nonspecific disease, accompanied by cough, nasal discharge, and dyspnea, which can lead to respiratory failure. Acute bronchiolitis occurs primarily in children and is caused by viral infections (respiratory syncytial virus (RSV)/para-influenza virus).
6.3 Clinical Presentation
The disease is usually acute with dry cough, wheezes, tachypnea, and difficult feeding in infants. In winter months, acute bronchiolitis is one of the most common reasons for hospitalisation in infants. On chest X-ray there are signs of hyperinflation and a mosaic pattern. The condition may be complicated by pneumonia or bacterial super infection. Auscultation reveals fine vesicular crepitations. There is no obstructive component.
6.3 Diagnosis
RS viruses can be detected by a rapid test in nasal secretions. Serologically there are no clear criteria.
CT/chest X-ray (Fig. 19.65):

Acute bronchiolitis due to heroin inhalation. Axial CT image in lung window shows diffuse, micronodular, confluent infiltrates, with relative subpleural sparing
-
Prominent hilar shadows
-
Increased translucency with reduced vascular markings in the lung periphery
-
Star-like condensations peribronchial
-
“Tree in bud” sign
-
Mosaic perfusion
-
Ground-glass pattern
6.3 Treatment
Treatment depends on the severity of the disease. The presence of respiratory failure, reduced pO2, signs of dehydration, apnea, and comorbidities are indications for hospitalisation. Adequate hydration and oxygen are very important. Pulse oximetry monitoring should be performed. There is no specific medical treatment.
6.4 Chronic Bronchiolitis and Related Diseases
6.4 Chronic Bronchiolitis
6.4 Aetiology, Pathogenesis, and Clinical Presentation
Chronic bronchiolitides have different etiologies and variable symptomatology. They usually occur secondary to other conditions.
The obstructive form is characterised by fibrotic scarring of the bronchioli with progressive dyspnea and dry cough. Sometimes, basal crepitations or crackles are auscultated.
Restrictive forms are characterised by bronchiolar narrowing, so that the alveoli are no longer involved in the gas exchange. This results in atelectasis and interstitial tissue injury. Clinically there is nonproductive cough.
6.4 Imaging
The chest radiograph can only show signs of inflammation of the small airways. With unremarkable signs on radiography and marked clinical signs, further investigation by HR-CT is indicated. The characteristic findings include air trapping due to luminal narrowing of the bronchi, bronchiolar wall thickening, and dystelectasis.
The classification of idiopathic interstitial pneumonias is based on the American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias of 2002.
Diffusion Capacity
Gases in the air reach blood in the lung capillaries by diffusion. According to Fick’s principle, this depends on the gas exchange surface, the wall thickness, and the gradient pressure.
With diffusion impairment there is a decreased diffusion capacity of the lungs and pulmonary circulation. Because of the 20-fold diffusibility of CO2 in the blood compared to oxygen, there will initially be only hypoxemia without increase in PCO2.
Diffusion impairment may have different causes:
-
Increased thickness of diffusion membranes, for example, inflammation, oedema, fibrosis
-
Decreased diffusion surface area, in emphysema, after pneumonectomy, pneumonia, fibrosis, tuberculosis, recurrent pulmonary embolism
Symptoms are caused by increased cardiac output. For example, during exercise when more blood rapidly flows through the lungs and the contact time is not enough for sufficient gas exchange.
6.4 Idiopathic Pulmonary Fibrosis (IPF)/Usual Interstitial Pneumonia (UIP)
6.4 Definition, Epidemiology, Pathogenesis
IPF is sometimes referred to as cryptogenic fibrosing alveolitis. It affects most commonly men in the middle to older age. It is believed that the disease is caused by inhalation of an unknown pollutant. Another theory is a defect in a gene required for surfactant production.
The production of an intra-alveolar exudate is associated with ulceration of the alveoli and damage to pneumocytes. Repair mechanisms lead to fibrogenesis. The prognosis is poor with a median survival time of approximately 5 years.
6.4 Clinical Presentation
Typical symptoms are:
-
Progressive dyspnea with increased diffusion impairment
-
Finger clubbing
-
Basal crackles
-
Cyanosis of the lips and Cor pulmonale in chronic hypoxemia
-
Occasional fever
Diffusion impairment: during gas exchange, oxygen must diffuse from the alveoli to haemoglobin of red blood cells and CO2 diffuses into the alveoli. The amount of gas exchange is dependent on the diffusion surface and the partial pressure.
6.4 Imaging and Diagnosis
On chest X-ray, the early appearance is an increased reticular pattern, more in the lung bases (Table 19.17). On HR-CT, the diagnosis can be made before the changes are visible on radiography. Additional signs include:
-
Symmetric, subpleural, bilateral parenchymal honeycomb pattern, more in the lung bases, which spreads cranially on follow-up
-
There may be associated ground-glass opacities
-
Transition to fibrosis zones possible
-
Traction bronchiectasis due to fibrosis
With extensive ground-glass opacities, other differential diagnoses should also be considered including RB-ILD (respiratory bronchiolitis-associated Interstitial Lung Disease), DIP (desquamative interstitial pneumonia), COP (cryptogenic organising pneumonia), and NSIP (nonspecific interstitial pneumonia).
6.4 Nonspecific Interstitial Pneumonia (NSIP)
6.4 Definition
In the past, all nonclassifiable interstitial pneumonias were grouped under NSIP. NSIP-like conditions are often associated with autoimmune diseases. The patients are usually between the ages of 40 and 50 years. There are no other predisposing factors. Histologically, there is lymphocyte-rich alveolitis. The changes tend to produce peripheral basal fibrosis without a nodular component.
6.4 Clinical Presentation
The disease is slowly progressive; there will be fatigue, weight loss and dyspnea, and rarely fever and finger clubbing.
6.4 Imaging
HR-CT:
-
Predominantly ground-glass opacities; symmetric and subpleural
-
Reticular opacities in approximately 50%; may be associated with traction bronchiectasis
-
“Honeycombing” is infrequent
The radiologic differentiation from UIP is not always possible.
6.4 Desquamative Interstitial Pneumonia (DIP)
6.4 Definition
Desquamative interstitial pneumonia is difficult to distinguish from RB-ILD on CT. Both entities often affect smokers in middle age. In the bronchoalveolar lavage there are increased macrophages, eosinophils, and neutrophils. The prognosis is good on avoiding the inhaled noxious substance and possibly with additional immune modulation therapy.
6.4 Clinical Presentation
Clinically, there is dyspnea, dry cough, and finger clubbing. Auscultation reveals delicate basal crackles.
6.4 Imaging
X-ray/HR-CT:
-
Localised, peripheral, and basal located ground-glass opacities (Fig. 19.66)
Fig. 19.66 
Biopsy-proved desquamative interstitial pneumonia (DIS). Axial CT image in lung window shows diffuse, peripheral, ground-glass pattern, mainly in the lower lobes (L > R)
-
Confluence of infiltrates is possible
-
Fine reticular pattern is common
-
Fibrosis only occurs in late stages

HR-CT can differentiate DIP from UIP by the absence of fibrosis. DIP has, in contrast to RB-ILD, a more homogeneous appearance.
6.4 Respiratory Bronchiolitis Interstitial Lung Disease (RB-ILD)
6.4 Pathogenesis
Respiratory bronchiolitis interstitial lung disease occurs primarily in men between 40 and 50 years with a long history of cigarette smoking. Histologically, broncho-alveolar lavage reveals pigmented alveolar macrophages. Most patients improve with cessation of smoking and possibly corticosteroid therapy.
6.4 Clinical Presentation
The disease manifests itself with increasing dyspnea, hypoxemia, combined obstructive and restrictive functional impairment.
6.4 Imaging
HR-CT:
-
Localised, patchy ground-glass opacities
-
Centrilobular nodules
-
Changes are more peripherally located
-
Mostly upper lobe centrilobular emphysema
-
Air trapping
6.4 Bronchiolitis Obliterans/Cryptogenic Organising Pneumonia
6.4 Aetiology and Pathogenesis
Cryptogenic Organising Pneumonia is idiopathic, i.e., with no identifiable cause. When associated with collagen vascular diseases, inhalation diseases, infections, or drug toxicity, it is called bronchiolitis obliterans. The histopathologic appearance is chronic interstitial inflammation with organising fibrosis in the alveoli and maybe the bronchioles. The diagnosis can only be made after all causes are excluded. The final histopathologic diagnosis may require CT-guided biopsy, as the bronchoalveolar lavage (BAL) is sometimes nonspecific. BAL reveals increased CD8 cells and granulocytes.
Most affected patients are in the 5th decade of life. Males and females are equally affected but the disease affects nonsmokers more than smokers.
6.4 Clinical Presentation
The disease presents with dyspnea, dry cough, sometimes slight fever for about 2 months on average. There is no improvement on antibiotic treatment.
6.4 Imaging
X-ray:
-
Initially patchy ground-glass opacities (Fig. 19.67)
Fig. 19.67 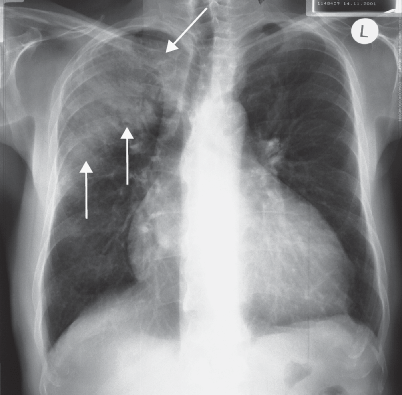
Cryptogenic organising pneumonia (COP). Chest X-ray posteroanterior view shows diffuse consolidation opacity in the right upper lung lobe with air bronchogram (arrows)
-
Usually bilateral lower lobe distribution
-
Commonly positive air bronchogram with thickened bronchial walls
-
Occasionally pleural effusion
-
Enlarged hilar lymph nodes may be present
-
Multifocal, basal consolidations with broad-based contact to the pleura

CT:
-
Large peripheral consolidations in two-thirds of cases
-
Positive air bronchogram
-
The bronchi are sometimes thickened or mildly dilated
-
In about half of cases, peripherally located ground-glass opacities are seen as well as centrilobular nodules due to alveolitis
Special Form: Swyer-James-McLeod syndrome
This syndrome is a disorder that is caused by viral infection before full growth of the lungs. This leads to the development of bronchiolitis obliterans usually limited to one lung. The chronic changes may induce pulmonary artery hypoplasia. The diagnosis is often an incidental finding in adulthood. Pulmonary function tests, however, reveal reduced vital capacity combined with evidence of obstructive disorder. On CT, there is a persistent hyperinflated lung area, near to scarred tissue with bronchiectatic changes.
6.4 Acute Interstitial Pneumonia (AIP)/Hamman-Rich Syndrome
6.4 Definition and Pathogenesis
This is an acute form of interstitial pneumonia. Histopathologically, there is diffuse alveolar damage associated with hyaline membranes, oedema, and a pronounced inflammatory reaction. The lungs are usually diffusely affected. The prognosis is poor, with a fatality rate of approximately two thirds of patients within 3 months, even with modern treatment methods. Spontaneous healing is possible with honeycomb formation. The exact cause of the disease is unknown, but it may be multifactorial due to drugs, or in the context of collagen diseases. Eventually, AIP is diagnosed by exclusion. The final diagnosis can be made by biopsy, which reveals alveolar damage with diffuse fibroblast proliferation.
6.4 Clinical Presentation
The condition presents with flu-like symptoms, as well as rapidly progressive dyspnea, dry cough, as well as diffusion and restrictive impairment in pulmonary function tests.
6.4 Imaging
Chest X-ray/CT:
-
Diffuse alveolar shadowing, more in the lung bases
-
On CT, homogeneous basal ground-glass opacities
-
Diffuse consolidation
-
Discrete fibrotic bands
-
In case of healing “residual honeycombing”
6.4 Lymphoid Interstitial Pneumonia (LIP)
6.4 Definition and Pathogenesis
LIP is a very rare disease, which is found most commonly in the context of autoimmune diseases such as systemic lupus erythematosus, rheumatoid arthritis, and myasthenia gravis. The disease is thus more common in middle or old age women. Histologically, there is an infiltration of the alveolar septa with lymphocytes and histiocytes and enlarged pneumocytes. It may be difficult to be distinguished from pulmonary lymphoma (MALT).
6.4 Clinical Presentation
The disease presents with dry cough and slowly progressive exertional dyspnea.
6.4 Imaging
HR-CT:
-
Ground-glass opacities
-
Reticular pattern
6.4 Treatment
The main therapeutic approach for pulmonary fibrosis is corticosteroids. All forms of idiopathic interstitial pneumonias are largely steroid sensitive. In most cases steroids (prednisolone) are combined with azathioprine or cyclophosphamide. Treatment with interferon is under evaluation.
Spirometry
Spirometry refers to a group of tests that measure various parameters of lung function. There are two methods: closed circuit or open circuit spirometers.
During the examination, the patient inhales through a mouthpiece. The volume and flow of air in and out of the lungs are then measured. The functional parameters of respiration could be either static or dynamic.
Static lung parameters:
-
Forced Vital Capacity (FVC) is the total volume of air that can be exhaled during a maximal forced expiration effort after maximal inspiration. Normal values lie between 4 L for men and 3 L for women. The vital capacity is reduced with restrictive and obstructive disease and severe emphysema.
-
Residual Volume (RV): air remaining after maximal expiration in the lungs. This is normally about 1.5 L. The residual volume is increased in emphysema and decreased in restrictive diseases.
-
Total Lung Capacity (TLC): the entire lung volume consists of the vital capacity and the residual volume.
-
Tidal volume (VT): air volume of about 500 ml, which is inhaled and exhaled with each unforced respiratory cycle.
Dynamic lung parameters:
-
Forced expiratory volume in 1 s (FEV1): the volume that can be exhaled in the first second under force after maximal inspiration. Normally the flow rate is > 2 L/s. FEV1 is significantly reduced in obstructive diseases.
-
Tiffeneau index: the ratio of FEV1/FVC multiplied by 100. The normal value is > 70%. In severe obstruction, it may be reduced to only 40%. In restrictive disease, the Tiffeneau index will increase.
The determination of the measured values in spirometry is extremely dependent on the cooperation of the patient. Furthermore, the values vary as a function of age, sex, and stature of the patient.
Body plethysmography:
In body plethysmography, the patient sits in an airtight chamber and inspires through a mouthpiece into a separate space. Thus, the prevailing pressure in the alveoli (compliance) and airway resistance (resistance) can be determined. The measured values are shown graphically on a pressure-volume diagram, which is characteristic of certain lung diseases. Besides the lung volume and the resistance, the residual volume which remains in the lung after maximal exhalation can be measured. Compliance measurements determine the elasticity of the lungs and thorax as changes in volume of the lungs in correlation to the transpulmonary pressure difference.
6.5 Idiopathic Lung Fibrosis
6.5 Definition and Pathogenesis
Lung fibrosis due to various etiologies causes destruction of lung parenchyma and subsequent functional impairment. Only when all treatable causes are excluded, the diagnosis of idiopathic fibrosis can be made.
General radiologic signs of fibrosis are: (Figs. 19.68 and 19.69)

Idiopathic lung fibrosis. Chest X-ray posteroanterior view shows thickened interstitial lines, diffuse in both lung fields, with elevated left diaphragm

Suspected idiopathic lung fibrosis. a Axial CT image in lung window shows posterior subpleural opacities, fibrosis is possible. b Axial CT image in the prone position, the posterior subpleural changes are no more visible
-
Thickened interstitial structures with cicatricial component
-
Thickened interlobular septa
-
Volume reduction of the affected regions, elevated diaphragm on the affected side
-
Secondary formation of traction bronchiectasis
-
Curvilinear fibrotic bands parallel to the pleura
-
Little ground-glass opacities
-
In late stages signs of pulmonary hypertension with dilatation of the pulmonary arteries
7 Inhalational Lung Diseases and Foreign Body Aspiration
7.1 Pneumoconioses
7.1 Definition, Aetiology, and Pathogenesis
Pneumoconioses are lung diseases caused by inhalation of inorganic dusts which deposit in the lungs inducing tissue reaction. The size of the particles plays a major role in the development of pneumoconiosis. Large particles > 10 microns are filtered out in the nose. Smaller particles with a diameter between 5 and 10 microns can penetrate into the lungs. However, these particles are carried away by the cilia in the bronchial tree and coughed out. Relevant dust particles for the development of pneumoconiosis have a diameter of approximately 1–3 microns which can eventually reach the alveoli passing through other natural filter stations.
Pneumoconiosis occurs most frequently in the context of occupational exposure to dust. The inhaled dust can either be engulfed by macrophages or directly deposited in the lung tissue. For pneumoconiosis to develop, the defense mechanisms of the lungs must be overwhelmed, meaning that the inhaled dust quantity exceeds the mucociliary clearance function of the lung. Therefore, the dust concentration in the air, the daily exposure time, and the duration of exposure are important factors for development of pneumoconiosis.
The primary effect of permanent exposure to dust is irritation of mucous membranes. This results in decreased resistance of the respiratory epithelium, and development of chronic bronchitis. Bronchitis is more common in the dust-exposed population than the normal population. Furthermore, inhaled dust may also have an allergenic effect. This is particularly observed with dusts of plant origin and may eventually cause bronchial asthma. Some particles such as fungal spores or bacteria-contaminated dusts can also cause lung infections.
Histologically, there are two major groups of pneumoconiosis:
-
Fibrogenic
-
Nonfibrogenic
Fibrogenic pneumoconioses are common; inhalation of the dust causes moderate to pronounced fibrous reaction. This results in an irreversible destruction of the alveoli with loss of elasticity of lung tissue. Usually a long exposure time of > 10 years is present. The condition presents initially with fatigue and later with shortness of breath. A causal therapy is not possible and the changes continue to progress even after termination of exposure. Because of restrictive changes and impaired gaseous exchange, the condition may eventually lead to development of Cor pulmonale. The most important causatives are silicosis and asbestosis.
Nonfibrogenic pneumoconioses are characterised by little fibrous reaction so that the alveolar structure is intact. The changes may be reversible after termination of exposure. Impairment of lung function is usually only mild or absent. Nonfibrogenic pneumoconioses include coal workers pneumoconiosis and siderosis.
According to the 10th revision of the WHO’s International Statistical Classification of Diseases and Related Health Problems (ICD-10); there are the following types of pneumoconiosis (Table 19.18).
7.1 Silicosis
7.1 Definition and Pathogenesis
Silicosis means the inhalation and deposition of silica dust in the lungs. This usually occurs as an occupational exposure; especially in miners. The disease has overall decreased in recent years due to a reduced number of miners and improved safety measures. Other at risk occupations include granite, slate and sandstone quarrying, as well as ceramic and pottery production.
The inhaled dust can be directly cytotoxic. In addition, phagocytosis by alveolar macrophages releases cytotoxic byproducts. These macrophages migrate into the lymph spaces towards hilar lymph nodes.
7.1 Clinical Presentation
Clinically, obstruction occurs first, followed by a restriction. This results in pulmonary hypertension, with development of cor pulmonale in the end-stage. Chronic bronchitis is commonly associated. Tuberculosis occurs about 20 times more frequently than in the normal population. Silicosis may have a carcinogenic effect.
There are two different clinical courses:
-
Acute silicosis due to acute pronounced exposure to silica dust over months can cause alveolar filling with proteinaceous material which leads to a progressive loss of lung function and death within years.
-
Chronic silicosis requires a longer exposure time. Progression is slow, but the changes may continue even after termination of exposure. Clinically there is dyspnea at rest and progressive emphysema until development of cor pulmonale. With an early elimination of the pollutant, progression can be stopped.
7.1 Imaging
X-ray: At the beginning there is a fine reticular pattern (Fig. 19.70), and in advanced stages a honeycomb pattern. Well-defined, fine nodules with a maximum diameter of about 1 cm are seen in the upper lobes. With progression, the nodules can become confluent into polygonal opacities with central calcification. Cavity formation in confluent lesions is possible. In the presence of cavitation, the exclusion of reactivated tuberculosis becomes important. Fibrosis leads to formation of cicatricial emphysema. In 5% of cases, silica deposits in the enlarged hilar lymph nodes lead to egg-shell calcifications.

Silicosis. Chest X-ray posteroanterior view shows multiple fibrotic changes in the right lung (arrows). There is associated left hilar lymphadenopathy with shell-like calcification (arrowheads)
Silicosis predisposes to the development of tuberculosis. There is a potential carcinogenic effect.
HRCT:
-
Small nodular, fibrotic changes usually centrilobular
-
With increased fibrosis, thickening of the interlobular septa
Large confluent lesions, when asymmetric or unilateral, could be distinguished from bronchial carcinoma by the presence of fibrosis with volume loss and cicatricial emphysema.
7.1 Treatment
There is no definitive therapy for silicosis. Further exposure should be prevented to hinder disease progress. Pulmonary infections must be early treated with antibiotics. Complicated obstructive disorders should be treated similar to the treatment of bronchial asthma.
Caplan Syndrome
This syndrome is silicosis associated with rheumatoid arthritis.
7.1 Asbestosis
7.1 Definition and Pathogenesis
Asbestos is a fire-resistant material which was used in constructions in Germany till the 1990s of the last millennium. Asbestos is the generic form for a heterogeneous group. A particularly aggressive type is amosite asbestos. Other forms are actinolite, anthophyllite, chrysotile, crocidolite, and tremolite asbestos.
The inhalation of asbestos fibers leads to a series of pulmonary and pleural reactions. The inhaled fibers are either taken by the alveolar macrophages or they penetrate the alveolar wall up to the pleura, where they form diffuse pleural thickening or plaques. The needle-like fibres destroy the macrophages inducing cytochemical reactions and formation of fibrosis in the surrounding tissue. Therefore, the asbestos-related changes can be classified into pulmonary and pleural changes.
7.1 Clinical Presentation
The pulmonary form is characterised by interstitial pulmonary fibrosis. This leads to an exertional dyspnea through ventilation impairment and occasional chest pain. There is associated chronic bronchitis.
Asbestos bodies can be identified in the broncho-alveolar lavage, these are asbestos fibres, coated with iron-rich protein sediments at their ends (ferruginous fibres), usually associated with macrophages. Minimal asbestosis refers to the light microscopic detection of asbestos exposure; with fibrosis of a respiratory bronchiole radiating into the adjacent alveolar septa and associated asbestos bodies.
It is generally believed that the carcinogenic effect of asbestos exposure is correlated with the duration of exposure and amount of inhaled fibres. The recognition of an occupational disease is dependent on the history of exposure, lung function tests, and the X-ray.
Complications are bronchial carcinoma and pleural mesothelioma. For bronchial carcinoma to be considered as an occupational disease, the detection of pulmonary fibrosis or histologically proven asbestosis is required.
7.1 Imaging
Chest X-ray:
-
Small, poorly defined focal opacities in the lower lobes
-
Thickened pleura sometimes with thickened lines extending to the parenchyma
-
Small effusions as a sign of asbestos pleuritis
-
Round atelectasis
-
Ill-defined cardiac and diaphragmatic contours
-
Septal thickening
-
Rarely massive fibrosis
CT/HTCT:
-
Basal peripheral micronodules
-
Mostly basal curvilinear opacities
-
Reticular pattern with thickened septa
-
Thickened bronchovascular structures
-
Round atelectasis
-
Cicatricial bands, which converge radially towards the pleura
-
Possibly, honeycomb pattern
-
Pleural plaques
-
Nonspecific pleural thickening, partially stippled or calcified parts
The specific picture of asbestosis on CT and HRCT is thickened interlobar and interlobular septa with a reticular pattern of fibrosis and patchy opacities and round atelectasis. Pleural plaques, sometimes with calcification or pleural thickening are only diagnostic of asbestos exposure, but are not pathognomonic for asbestosis.
7.1 Aluminosis
Aluminosis refers to massive pulmonary fibrosis, which may result from relatively short exposure duration and lead to rather severe respiratory impairment.
7.1 Siderosis
Siderosis is one of the nonfibrogenic pneumoconioses. Siderosis results from inhalation of iron oxide-containing particles, which are phagocytosed by the alveolar macrophages and deposit in the perivascular interstitium. It occurs after long exposure time in distillers and welders.
Imaging.
Chest X-ray/CT:
-
Reticular to reticulo-nodular pattern
-
May regress after cessation of exposure
-
No enlarged lymph nodes
7.1 Anthracosis
Anthracosis is a nonfibrogenic pneumoconiosis. It is caused by inhalation of carbon, which is present in dealing with coal.
7.1 Less-Common Pneumoconioses
An inhalation of a number of other inorganic materials can cause pneumoconiosis, including cerium, tungsten, cobalt, titanium, and beryllium. Radiographic changes are in general nonspecific.
Mixed pneumoconiosis is common with inhalation of multiple materials together or sequentially. A definite diagnosis can be difficult or impossible by X-ray or CT. For recognition as an occupational disease, a lung biopsy may be necessary.
7.1 Extrinsic Allergic Alveolitis
7.1 Definition, Aetiology, and Pathogenesis
Extrinsic allergic alveolitis is caused by inhalation of certain bacterial, animal and plant antigens, fungi, and chemicals. In most cases it is occupational, especially in farmers who have contact with moist hay, with actinomycetes as the causative antigen. Workers who are in contact with malt, garbage, fruit, etc. are exposed to molds. In bird fanciers lung, bird excrement and feathers are the allergens.
Repeated allergen exposure causes chronic granulomatous inflammation caused by type 2 and 3 hypersensitivity reactions. In early stages, these changes are reversible with avoidance of the allergen, in late stages there is often irreversible progress to fibrosis.
7.1 Clinical Presentation
The picture starts to develop acutely after several hours from exposure with flu-like symptoms, exertional dyspnea, and dry cough. After about 2 days, improvement occurs, but renewed allergen exposure causes flare-up. The chronic course leads to progressive exertional dyspnea, fatigue, and weight loss.
7.1 Diagnosis, Imaging
Lung function tests reveal reduced vital capacity with only slightly reduced to normal functional residual capacity; diffusion capacity is also decreased. Laboratory tests reveal elevated erythrocyte sedimentation rate and white blood cell count. Broncho-alveolar lavage shows a CD4/CD8 ratio of < 1, with reduced macrophage and increased neutrophilic granulocytes. Biopsy may be necessary in cases with unclear results.
X-ray:
-
In the early stage, findings are nonspecific (. Fig. 19.71 )
Fig. 19.71a–c 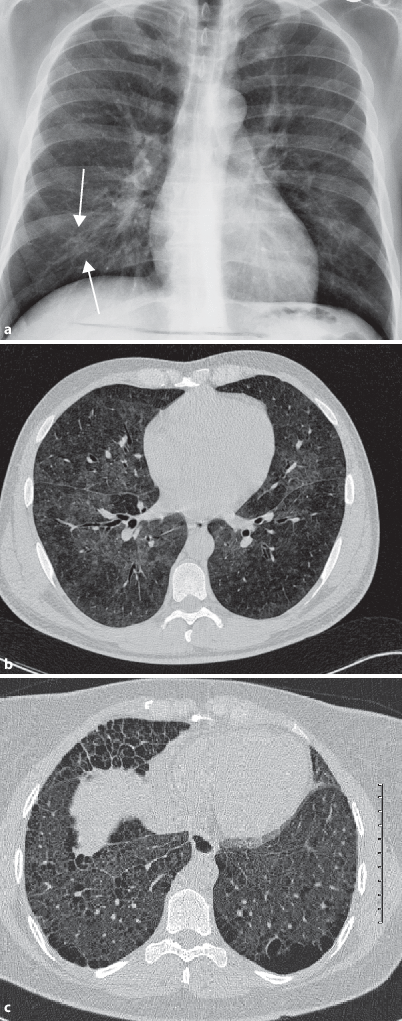
Extrinsic allergic alveolitis. a Chest X-ray posteroanterior view shows a nonspecific image with multiple fine nodular and confluent infiltrates (arrows). b Axial high-resolution CT image shows a ground-glass pattern, with fairly defined borders, air trapping. c Axial high-resolution CT image shows advanced extrinsic allergic alveolitis with fibrous changes and honeycombing
-
Later, fine nodular, sometimes confluent infiltrates in the middle and lower lobes
-
In the chronic stage, fibrotic changes are seen

HRCT allows detection of the disease in its early stages.
HRCT:
-
Differentiation of active inflammation and intraparenchymal scars
-
Small peribronchial inflammatory lesions
-
Ground-glass opacities with small nodular opacities, which may become confluent
-
Sometimes sharply demarcated mosaic pattern
-
Air-trapping
-
Reticular opacities are seen at an advanced stage, with onset of fibrosis
7.1 Treatment
The first step is identification of the causative allergen via a detailed history of the illness. Allergen avoidance is mandatory. In acute cases, oxygen administration is indicated as a symptomatic therapy. Medications are indicated for suppression of the inflammatory response in acute and chronic cases. Corticosteroids are usually the first choice. In acute cases prednisone is administered in a dose of 1–2 mg/kg and then 0.2 mg/kg as a maintenance dose.
7.1 International Labour Organisation (ILO) Classification
The ILO classification is a worldwide classification system for changes in chest radiographs related to dust inhalation. Its primary role is detection of epidemiologic patterns of occupational diseases. For this purpose, a posteroanterior chest radiograph is required in 1:1 format. If this is not possible, the image must not be smaller than two thirds of the original. Different criteria are evaluated, including the image quality, lung lesions, pleural findings, and ancillary findings. The evaluation of image quality is implemented in Germany with +; +/−; +/− − and u.:
-
+ : Good
-
+/−: A technical error is present, which does not impair the diagnosis of pneumoconiosis
-
+/− −: Technical defect limits evaluation, but diagnosis still possible
-
u: Unacceptable
Otherwise, classification is made with letters (p, q, r, etc.) or numbers (1–4). In the pulmonary findings the classification is done according to size, shape, and distribution. Pleural thickening is documented for each side separately with details and localisation. Thickness more than 3 mm and calcifications are also stated. Using symbols, the reader comments on additional findings such as pleural effusion, emphysema, eggshell calcifications, tuberculosis, atherosclerosis etc., with the addition of either “compatible with” or “suspicious of” phrases.
7.2 Noxious Gas Inhalation
Inhalation of toxic gases causes different reactions in the lung parenchyma. Depending on the nature and duration of exposure, either irritation of the bronchi or alveolar damage may develop, which lead to bronchiolitis or pulmonary oedema. Bronchitis cannot be diagnosed on radiographs. Toxic pulmonary oedema, however, is evident on imaging as multiple central, ill-defined opacities that may become confluent in progressive cases.
7.3 Foreign Body Aspiration
Aspiration of foreign bodies is most commonly observed in children. Small objects that may be inhaled include coins, nails, and peanuts. In adults, aspiration of, for example, dental fillings is uncommonly seen. X-ray is usually performed upon suspicion to rule out aspiration and for localisation when possible.
7.3 Clinical Presentation
Upon aspiration, there are usually coughing attacks which can mimic whooping cough in children. Clinical examination reveals weak respiratory sound due to bronchial obstruction with distal hyper-resonance.
7.3 Imaging
As the right main bronchus is more vertically oriented, most inhaled foreign bodies are found there. Depending on the X-ray density, the foreign body can be recognised directly or indirectly. Indirect signs are:
-
Atelectasis due to bronchial obstruction
-
Distal pneumonia
-
Hyperinflation due to ball-valve mechanism obstruction by the foreign body
-
The mediastinum shifts to the healthy side during expiration
Particularly in children with recurrent pneumonia, an unrecognised inhaled foreign should be suspected.
7.3 Treatment
After localisation of the foreign body, extraction should be performed by bronchoscopy. Supplementary antibiotic treatment must be given.
8 Immunological Diseases
8.1 Systemic Vasculitides
Vasculitides are vascular inflammations associated with damage of the involved organs. They can be primary with idiopathic aetiology and may affect the small, medium, or large vessels. Secondary forms are associated with autoimmune diseases such as collagen diseases, rheumatoid diseases, infectious diseases or drug-induced.
8.1 Wegener’s Granulomatosis
8.1 Definition and Pathogenesis
Wegener’s disease is characterised by ulcerative granulomas in the respiratory tract with vasculitis of the small vessels. Renal involvement is common.
8.1 Clinical Picture
Wegener’s granulomatosis runs in stages, the first is localised and is characterised by ulcerations, epistaxis, rhinitis, sinusitis, cough, and microhaematuria. The second stage is characterised by generalisation of organ involvement, with pulmonary granulomas, glomerulonephritis, and systemic symptoms. Radiographically, there are multiple bilateral confluent pulmonary nodules, with cavitations and without characteristic localisation. In two thirds of cases associated pleural effusions occur. Without treatment the prognosis is bad. With aggressive treatment the 5-year survival rate is about two-thirds of affected patients.
8.1 Diagnosis
Specific antibodies can be detected in the blood including C-▶ ANCAs (anti-neutrophil cytoplasmic antibodies). For the final diagnosis, biopsy with histologic evaluation may be necessary.
Chest X-ray/CT:
-
Bilateral, multiple pulmonary nodules with possible diameter of > 5 cm (. Fig. 19.73 )
Fig. 19.72a,b 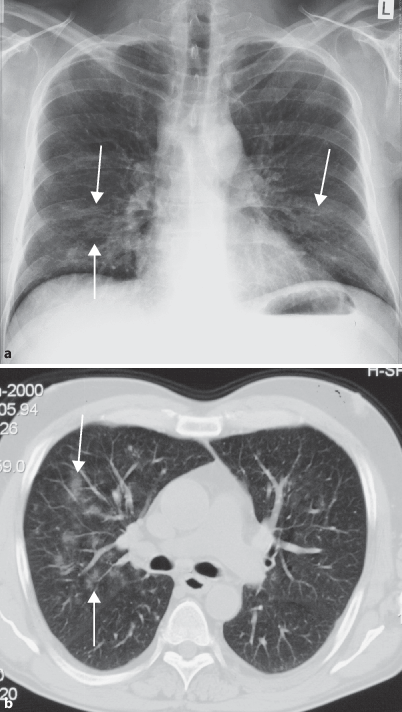
Cocaine inhalation. a Chest X-ray posteroanterior view shows diffuse, bilateral alveolar shadows (arrows). b Axial CT image in lung window shows alveolar infiltrates (arrows) in perihilar distribution in the same patient
Fig. 19.73 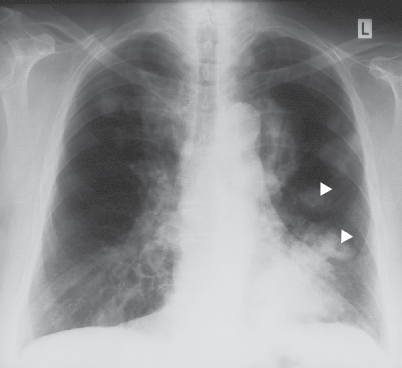
Wegener granulomatosis. Chest X-ray posteroanterior view shows multiple nodular shadows < 5 cm, with cavitation (arrowheads)
-
Central breakdown in about half of all nodules with the formation of cavities with thick irregular inner walls
-
Secondary superinfection possible
-
Rarely enlarged lymph nodes
-
CT may show feeding vessels
-
Ground-glass opacities possible


8.1 Treatment
Treatment of Wegener’s disease runs in three phases. Induction is done first in order to achieve remission. This is started with high doses of corticosteroids and with cyclophosphamide in multiple organ involvement. After remission, a maintenance phase should be started by gradual reduction of medication doses. To prevent recurrence, prophylactic sulfonamide administration should be continued.
8.1 Churg-Strauss Syndrome
8.1 Definition, Pathogenesis, and Epidemiology
Churg-Strauss syndrome is a P-antineutrophil cytoplasmic antibody (P-ANCA)-associated systemic vasculitis affecting small arteries and veins. Often there is associated bronchial asthma. Furthermore, involvement of the vasa nervorum leads to affection of individual nerves. Involvement of the paranasal sinuses is also typical. The causative agent is to date unknown, and idiopathic, multifactorial, and drug-induced etiologies are hypothesised.
There are about 2.5 cases per 100,000 people every year. Women, with an average age of 38 years, are more commonly affected. The survival rate with treatment in the first year after diagnosis is 90%. The 5-year survival rate is 62%. Mortality is caused by the involvement of the myocardium and coronary vessels.
8.1 Clinical Picture
The disease progresses in three phases, with different clinical patterns:
-
Early phase: Allergic symptoms with bronchial asthma and allergic rhinitis
-
Middle phase: Blood eosinophilia and eosinophilic infiltration of tissues, such as the lung and intestine
-
Final stage: Vasculitis of medium and small vessels
Pulmonary involvement leads to dry cough and haemoptysis. Other symptoms vary depending on the affected organ. Common manifestations include mononeuritis multiplex and gastrointestinal tract involvement with bloody diarrhoea.
8.1 Diagnosis
The triad of eosinophilia, asthma, and systemic vasculitis is highly suggestive for the diagnosis. In histologic specimens, an eosinophilic involvement of the perivascular tissue can be seen.
According to the American College of Rheumatology (ACR) the following six criteria distinguish Churg-Strauss syndrome for other diseases. In the presence of four of the criteria a sensitivity of 85% and specificity of 99.7% can be expected:
-
Asthma
-
Blood eosinophilia > 10%
-
Sinusitis
-
Pulmonary infiltrates
-
Histologic evidence of vasculitis with surrounding eosinophilia
-
Mononeuritis multiplex or polyneuropathy
Chest X-ray/CT: eosinophilic infiltrates with transient consolidations occur without typical predilection sites, as well as discrete or confluent nodules, which rarely cavitate. Furthermore, thickened bronchial walls and interlobular septa are common findings.
The CT scan shows subpleural ground-glass opacities and stellate enlarged arterioles.
Differential diagnosis: Wegener’s granulomatosis, Loeffler syndrome, and allergic bronchopulmonary aspergillosis.
8.1 Treatment
The treatment is with high doses of corticosteroids. Additionally, cyclophosphamide is indicated in case of multiple organ involvement or resistance to therapy.
8.1 Behçet’s Disease
8.1 Definition and Pathogenesis
Behçet’s disease is a rare multisystem disorder characterised by small vessel inflammation in young adults around the Mediterranean. Men are affected about twice as often as women. The aetiology is unclear; a genetic predisposition is suspected and HLA B5- and HLA B27-association were found. Furthermore, infectious or autoimmune etiologies are also discussed. The vasculitis is caused by deposition of immune complexes.
8.1 Clinical Picture
The disease is characterised by a clinical triad of genital ulcers, oral ulcers, and uveitis as well as arthralgia and multisystemic vasculitis with involvement of the venous, but also of the arterial vessels with aneurysm and thrombus formation.
The aphthous changes recur 2–3 times a year and heal without scarring. Most patients suffer partial or complete loss of vision due to multiple vascular occlusions in the eye. Small haemorrhages and inflammatory changes are seen in the ophthalmic examination. With involvement of the brain, parenchymal and vascular forms are differentiated. Parenchymal involvement leads to mental disorders, brain stem and motor dysfunction. The course is usually acute and relapsing. Vascular neuro-Behçet is characterised by intracranial hypertension, vascular occlusion, and venous sinus thrombosis. Cerebral infarction or aseptic meningitis are other rare manifestations. Furthermore, as part of multisystem disease, arthritis, mucosal gastrointestinal tract lesions, involvement of peripheral vessels with thrombophlebitis and aneurysm formation may occur. Involvement of the lung may occur with damage of the pulmonary vessels and haemoptysis.
8.1 Diagnosis
The diagnosis is mainly based on the clinical picture. In addition to recurrent oral ulceration, two of the following criteria must be present for diagnosis: skin lesions such as erythema nodosum, genital ulcers, positive pathergy test, or inflammation of the eye such as uveitis or vasculitis of the retina. A positive pathergy test is a local, sterile, pustular reaction 1–2 days after a sting with a sterile needle.
Lumbar puncture reveals increased protein content, leucocystosis, oligoclonal bands, IgG production.
8.1 Imaging
Chest X-ray:
-
Extensive opacities with haemorrhage
-
Subpleural nodules
-
Widened mediastinum by aneurysm
-
Pleural effusion
CT:
-
Pulmonary artery aneurysm
-
pulmonary artery thrombosis
-
Thrombosis of the superior vena cava
8.1 Treatment
There is no definitive therapy. Because of the variability of the clinical manifestation, there are various therapies. Skin and mucosal involvement respond well to high-dose corticosteroids accompanied by immunosuppressants such as azathioprine and cyclophosphamide. Refractory cases often respond to cyclosporin A. Additional therapeutic approaches are based on colchicine or thalidomide or immune modulatory drugs such as interferons.
8.2 Collagen Diseases
Collagen diseases are idiopathic autoimmune diseases that involve the connective tissue. Females are more commonly affected. They include systemic lupus erythematosus, rheumatoid arthritis, systemic sclerosis, polymyositis, Sjogren syndrome, and mixed connective tissue disease. The lung and pleura are commonly involved with pulmonary fibrosis, pleuritis, vasculitis, or other manifestations (Table 19.19).
8.2 Systemic Lupus Erythematosus (SLE)
8.2 Definition, Pathogenesis
Systemic Lupus Erythematosus is an autoimmune disease with unknown cause. Since women of childbearing age are much more commonly affected, a hormonal component in the development of the disease is suggested. Another theory is based on multifactorial exogenous triggers with genetic predisposition.
8.2 Clinical Picture
The commonest symptoms include general fatigue, polyarthritis without erosions, typical skin lesions, such as the butterfly facial erythema, an increased sensitivity to light, and oral ulcers.
The following organs may be involved in SLE:
-
Lungs:
-
Pleuritis, pleural effusion
-
Pulmonary infiltrates
-
Severe attacks of acute pneumonitis with dyspnea, fever, and inspiratory pain
-
-
Kidneys: proteinuria and renal impairment
-
Heart: myocarditis and pericarditis
8.2 Diagnosis
Detection of antinuclear antibodies (ANA) is important in the assessment of the activity. The anti-ds-antibodies and the sm-antigens are more specific, but limited by moderate sensitivity. Sometimes skin biopsy of affected areas is necessary for definitive diagnosis. Laboratory findings show increased erythrocyte sedimentation rate. Sometimes there is pancytopenia.
According to the American College of Rheumatology the presence of four of the following symptoms make SLE probable:
-
Butterfly erythema
-
Discoid skin rash
-
Photosensitivity
-
Mucosal ulcerations
-
Seronegative Arthrititis
-
Pleural effusion, pericardial effusion
-
Proteinuria
-
Neurologic disorder
-
Haemolytic anemia, pancytopenia
-
Antinuclear antibodies
-
Other antibodies (anti-ds, anti-Sm, etc.)
Chest X-ray/CT:
-
Basal, ground-glass opacities either unilateral or bilateral
-
Associated pleural effusion
-
Migrating infiltrates on X-ray
-
Rarely pulmonary fibrosis, with development of ground-glass opacities in the lower lobes, thickening of interlobular septa, reticular opacities, with end-stage honeycombing.
8.2 Treatment
There is no definitive therapy. In the acute phase high doses of corticosteroids are administered. Long-term therapy may be pursued with antimalarial drugs like chloroquine and hydrochloroquin; corticosteroids, azathioprine and cyclophosphamide. Additionally, symptomatic therapy is undertaken for the involved organs.
8.2 Progressive Systemic Sclerosis (PSS)/Scleroderma
8.2 Definition and Pathogenesis
Progressive systemic sclerosis is a multisystem disease involving the skin and internal organs. The cause is unknown, but it occurs more frequently in HLA-DR 5-positive patients. The disease is characterised by an excessive activity of fibroblasts with excessive protein deposition. This is triggered by cytokines such as transforming growth factor B, which is found in much higher concentrations in the blood in patients than in the normal population.
A special form of PSS is the Thibierge-Weissenbach syndrome associated with subcutaneous calcinosis.
8.2 Clinical Picture
At first, the symptoms are nonspecific such as fatigue, arthralgia, and possibly unclear, oedematous swelling of the extremities. This is eventually followed by the typical skin changes, such as hardening and tightening, sclerodactyly, and Raynaud’s phenomenon. Furthermore, there may be multiple organ manifestations such as involvement of the oesophagus with dysphagia and the kidneys with renal insufficiency. In half of cases, nonspecific lung fibrosis occurs, which manifests clinically with dyspnea and dry cough.
8.2 Diagnosis
The diagnosis of scleroderma is usually made clinically. Antinuclear antibodies are detected in > 90% of the patients, such as SLC 70, Anti-centromere antibody and P-CENB.
Chest X-ray:
Findings include basal peripheral reticular or reticulo-nodular infiltrates (. Fig. 19.74 ), which eventually progress to a honeycomb pattern.

Basal lung fibrosis in scleroderma. Chest X-ray posteroanterior view shows bilateral basal diffuse interstitial opacities (arrows)
HR-CT:
-
Thickened interlobular septa
-
Micro nodules, ground-glass opacities, thickened pleura
-
Central parts of the lung are involved only in advanced stages
Complications include aspiration pneumonia and pulmonary hypertension.
8.2 Treatment
There is no definitive therapy. The disease progress may be controlled by immunosuppressive drugs such as methotrexate or cyclophosphamide. Organ complications should be treated symptomatically. Physiotherapy is often necessary to maintain the ability to move.
8.2 Rheumatoid Arthritis
8.2 Definition and Pathogenesis
Rheumatoid arthritis is the most common form of connective tissue diseases. It leads to an inflammatory joint destruction with preference for the peripheral joints. Like many other autoimmune diseases, women are more frequently affected. The exact aetiology of the disease is unknown, but it is assumed to have multifactorial aetiology and 75% of the affected patients are HLA-DR4 positive. Because of interacting lymphocytes and monocytes there is an increased production of cytokines and auto-antibodies against the Fc fragment of IgG, the so-called rheumatoid factors. The synovium is involved with hyperplasia and infiltrated by inflammatory cells, with excessive pannus formation. This leads to increasing destruction of the joints with stiffness and deformity.
8.2 Clinical Picture
Patients complain of nonspecific general symptoms such as fatigue, low-grade fever, and muscle pain. Usually the small joints of the hands and feet are affected first. Metacarpo-phalangeal and proximal interphalangeal joints are preferably involved, with positive Gaenslen’s sign, or painful handshake. There is associated morning stiffness. Other manifestations such as Baker’s cysts or carpal tunnel syndrome may also be found. Subcutaneous swellings caused by rheumatoid nodules may be present on the extensor surfaces of joints. Progressive destruction leads to deformity and loss of function of the affected joints. Extra-articular manifestations of rheumatoid disease include pericarditis, pulmonary involvement, polyneuropathy, and conjunctivitis.
8.2 Diagnosis
For diagnosis of rheumatoid disease according to the American College of Rheumatology, four of the following criteria must be present:
-
Morning joints stiffness (lasting at least 1 hour)
-
Palpable swelling of three or more joints
-
Arthritis of hand or finger joints
-
Symmetric arthritis (simultaneous, bilateral, same joint regions)
-
Rheumatoid nodules
-
Rheumatoid factor detection in blood
-
Typical X-ray changes (juxta-articular osteoporosis and/or erosions)
Chest X-ray:
-
Pleuritis with pleural effusion
-
Pleural thickening
-
Reticulo-nodular fibrosis pattern that merges into the honeycomb lung pattern
-
Traction bronchiectasis caused by fibrosis
-
Intrapulmonary rheumatoid nodules are smooth to lobulated nodules, usually subpleural. Calcifications or cavitation are possible, and cavitating nodules appear as ring shadows.
HR-CT or MSCT: CT allows detection of pulmonary changes before the onset of symptoms. The changes are similar to pulmonary fibrosis, ground-glass opacities and traction bronchiectasis.
8.2 Treatment
Treatment of rheumatoid arthritis has several goals: first, to slow the progression of the disease, to keep the ability to move and to decrease patient’s complaints. Immunosuppressive agents such as methotrexate, sulfasalazine, hydroxychloroquine, chloroquine, aurothioglucose, and azathioprine are used. In addition, pain and inflammation can be reduced with nonsteroidal anti-inflammatory drugs. Immune modulatory therapies such as TNF-α and interleukins can be tried. Additionally, physiotherapy treatment should be done. If necessary, affected joints can be surgically replaced with prostheses.
8.2 Polymyositis and Dermatomyositis
8.2 Definition and Pathogenesis
Polymyositis and dermatomyositis are generalised chronic autoimmune inflammatory processes of the muscles and skin. Other connective tissues may also be affected. Women are affected twice as often as men. The age of onset is between 30 and 60 years. In about half of the cases, there is a pulmonary involvement. The exact aetiology is unknown. Pathophysiologically, a cytotoxic process directed against muscle antigens is the most accepted theory, as evidenced by the finding of CD8 cells that penetrate into the muscle fibres and lead to their destruction.
Dermatomyositis may occur also as part of paraneoplastic syndrome with lung and breast tumours, or be associated with other connective tissue diseases.
8.2 Clinical Picture
Clinically, there is painless muscle weakness. Dermatomyositis leads to red rash, diffusely distributed in the face and upper extremities. Whitish atrophy of the skin can be seen over the joints. In addition, subcutaneous calcifications and yellowish keratinisation of the nail occur. Associated general symptoms are common such as fatigue, weakness, and depression. Complications include myocarditis, alopecia, and gastrointestinal complaints such as dysphagia and diarrhoea. The course of the disease can range from rapid-progressive to mild-progressive over years.
8.2 Diagnosis
Laboratory tests show elevated C-reactive protein level, lactate dehydrogenase and aspartate aminotransferase as well as autoantibodies. The damage to the muscles leads to abnormal findings on electromyography; with fibrillations at rest and low amplitude polyphasic potentials with stimulation. Muscle biopsy is often necessary for definitive diagnosis. It shows perivascular infiltration with CD4 cells and intramuscular CD8 cells with muscle necrosis.
Chest X-ray and CT features include aspiration pneumonia due to dysphagia, and pulmonary fibrosis with basal ground-glass opacities and peribronchial thickening with transition into a honeycomb pattern. There is often associated COPD.
8.2 Treatment
Definitive therapy is only possible in tumour-associated forms. Therefore, the presence of tumours must be excluded. Medical therapy is based on immune suppression with corticosteroids, azathioprine, and methotrexate. In about half the cases, complete remission can be present after 5 years.
8.2 Sjögren’s Syndrome
8.2 Definition and Pathogenesis
Sjögren syndrome is a slowly progressive autoimmune disease with lymphocytic infiltration of the salivary and lacrimal glands with CD4 cells. It can occur primarily as an independent disease or associated with other autoimmune diseases or secondary to rheumatoid arthritis. Women are affected more frequently than men, with an age of onset of about 50 years. Frequently, HLA B8 and DR 3 are present. The exact aetiology is unknown.
8.2 Clinical Picture
The clinical picture is dominated by the sicca symptoms of xerophthalmia and xerostomia. There may be associated Raynaud’s syndrome, severe fatigue, arthralgia, renal involvement with nephritis and primary biliary cirrhosis. Involvement of the lungs manifests through persistent cough, dyspnea, and frequent infections due to thickened trachea-bronchial secretions. As a complication, enlarged lymph nodes may be seen, which can in turn transform into Hodgkin’s disease.
8.2 Diagnosis
The diagnosis is usually clinical. Associated malignancy should be ruled out. Xerophthalmia can be quantified with Schirmer’s test. Laboratory tests reveal biochemical evidence of Ro (SSA) and La (SSB) antibodies. The ESR is almost always increased. Salivary gland biopsy shows focal lymphocytic infiltrations.
Chest X-ray/CT:
-
Bronchial wall thickening
-
“Tree in bud” sign
-
Air-trapping
-
Bronchiectasis
-
Basal reticulo-nodular pattern
8.2 Treatment
There is no definitive therapy. The symptoms may be alleviated with artificial saliva or tears. Salivation can be stimulated by, for example, gum chewing. In case of high inflammatory parameters, immune-suppressive or immune-modulatory therapy with corticosteroids or cyclosporine are indicated.
8.3 Amyloidosis
8.3 Definition and Pathogenesis
Amyloidosis is extracellular protein deposition in the interstitium of various organs. There are different forms such as AA, AL, and hereditary amyloidosis, classified according to their biochemical structure.
The most common is AA amyloidosis, which is an acute-phase reactant produced mainly in the liver in response to multiple cytokines in various chronic rheumatic and autoimmune diseases. The kidney, liver, spleen, and gastrointestinal tract are predominantly affected. This leads to proteinuria up to renal failure, hepatosplenomegaly, constipation, and ulcers.
In AL amyloidosis, or light chain amyloidosis, the AL-proteins are formed by plasma cells. The symptoms vary depending on the affected organ.
8.3 Clinical Presentation
Defective proteins, in the form of amyloid, deposit in various organs. Accordingly, symptoms can range from heart failure due to involvement of the myocardium to liver cirrhosis due to amyloid deposition in the liver. The clinical picture is determined by the infected and damaged organ.
Deposition in the lungs can be either tracheobronchial, or parenchyma whether nodular or diffuse. Involvement of the lungs, together with heart and kidneys, carry poor prognosis.
8.3 Imaging
Definitive diagnosis of amyloidosis in suspected cases could be reached by biopsy of the affected organ. Biopsy of the lung for diagnosis of amyloidosis may be either transcutaneous or open. By staining with Congo-red, amyloid produces green light in the polarising microscope. In addition immunohistochemistry is performed for diagnosis of the amyloid type.
Tracheobronchial deposition of amyloidosis is usually not recognisable on chest X-ray. In generalised amyloidosis, the chest radiograph often reveals changes only at an advanced stage; with thickened septa or central peribronchovascular thickening by amyloid deposits, and less commonly with miliary shadows.
CT shows endobronchial plaques (difficult to differentiate from malignant lesions). The parenchymal form is characterised by solitary or less commonly multiple nodules, which can reach a diameter of up to 5 cm and is/are located in the basal lung sections. The borders are variable from round and smooth to oval and lobulated. In addition, coarse calcifications can be found in the nodules.
8.3 Treatment
The target of treatment of AA amyloidosis is to prevent severe organ damage with anti-inflammatory therapy. In addition, treatment of the causative condition should be tried. The treatment of AL-amyloidosis is difficult because there is no causal therapy and consists of systemic chemotherapy in addition to corticosteroids. There is also no curative treatment for hereditary amyloidoses. The last line of treatment is transplantation of the affected organ.
8.4 Diffuse Pulmonary Haemorrhage
There are various causes for diffuse bleeding into the lung parenchyma:
-
Idiopathic pulmonary haemosiderosis
-
Cardiovascular abnormalities
-
Goodpasture’s syndrome
-
Systemic vasculitides/collagen diseases: SLE, Wegener’s granulomatosis, ITP
-
Coagulation disorders
-
Cancers: leukaemia, Kaposi’s
-
Exogenous: toxic, traumatic
8.4 Goodpasture’s Syndrome
8.4 Definition and Pathogenesis
Goodpasture’s syndrome consists of pulmonary haemorrhages and rapidly progressive glomerulonephritis, triggered by antibasement membrane antibodies. The exact aetiology is unknown, but an association with infection is assumed. The disease is commonly associated with HLA DR2. Men are affected more frequently and mortality is high if untreated.
Immunohistochemistry can demonstrate IgG deposits along the tubular basement membrane. Also in the lungs, it results in IgG deposition at the basement membrane of the alveoli.
8.4 Clinical Picture
In most patients, there is a combination of pulmonary and renal symptoms, anemia as a result of chronic blood loss, and cough with haemoptysis. In a small percentage of patients, there is isolated lung involvement. The presentation is similar with anemia and cough with haemoptysis. Renal involvement with rapidly progressive renal impairment leads to uremia with anuria. Accompanying nonspecific symptoms such as fever and muscle aches can occur.
8.4 Imaging
Chest X-ray shows ill-defined, patchy shadows of different density, either confluent or nodular. Regression of haemorrhage is possible within days. Follow-up may show the development of progressive irreversible fibrosis.
8.4 Treatment
There is no definitive therapy. At the onset of the disease, daily plasmaphoresis may slow the progression. An additional immune-suppressive therapy with glucocorticoids and cyclophosphamide improves the prognosis. Furthermore, the progressive kidney damage resulting in anemia and hypertension must be treated. As a last resort, kidney transplantation may be done.
8.4 Idiopathic Pulmonary Haemosiderosis (IPH)
8.4 Definition and Pathogenesis
Idiopathic pulmonary haemosiderosis is a rare disease of unknown aetiology, first described by Virchow. The disease is characterised by episodes of pulmonary haemorrhage. The disease is proposed to be triggered by exogenous factors in the presence of genetic predisposition. The majority of patients are children and young adults.
8.4 Clinical Picture and Diagnosis
Patients complain of haemoptysis, cough, dyspnea, and restrictive ventilation disorder. Laboratory tests show microcytic anemia. Broncho-alveolar lavage shows increased siderophages. Biopsy may be necessary for definitive diagnosis.
8.4 Imaging
Chest X-ray/CT show a picture similar to pneumonia; with diffuse opacities and symmetric perihilar, fine nodular pattern.
8.4 Treatment
Treatment includes steroids, blood transfusion for severe anemia, prophylactic antibiotics, and oxygen.
8.5 Langerhans Cell Histiocytosis
8.5 Definition and Pathogenesis
Other synonyms for this disease are histiocytosis X and eosinophilic granuloma of the lung. Histiocytosis is a granulomatous disease of unknown aetiology characterised by the presence of large histiocytes containing rod- or racket-shaped organelles (Langerhans cells). The proposed pathogenesis is a defect in cellular interaction between T-cells and Langerhans cells, based on cytokine imbalance. The disease is often generalised, but can also be limited to the lung. The peak incidence is in young adults, and smokers are affected more.
Histologically, the disease can be classified into three stages; a cell-rich early-stage, a fibroblast proliferative stage, and a fibrocyte stage. Generalised forms can occur with involvement of lymph nodes, skin, brain, liver, intestines, etc.
The course is variable ranging from spontaneous remission to death because of respiratory failure.
8.5 Clinical Presentation
The clinical presentation is variable. Some patients are totally asymptomatic, other patients present with generalised complaints. The most common affected organs are bone followed by skin. With involvement of the lung, patients complain of nonspecific symptoms such as cough, pain, weight loss, haemoptysis, and dyspnea.
8.5 Diagnosis and Imaging
Pulmonary function tests reveal limited diffusion capacity and obstructive ventilation disorder. The diagnosis can be reached by detection of > 5% Langerhans cells in the bronchoalveolar lavage. Immunologically, there is a reaction with CD68 antibodies.
X-ray/CT of the chest show a reticulo-nodular pattern (. Fig. 19.75 ). Later, peribronchial nodules develop with a maximal diameter of 5 mm (differential diagnosis: sarcoidosis with sparing of the costophrenic angles). During the course, fibrotic changes occur on a background of a reticulo-nodular pattern. Small cysts with thick walls are seen diffusely in the lung fields (differential diagnosis: cystic metastases). The cysts tend to be confluent. In the end-stage, pulmonary fibrosis with a honeycomb pattern and without lung volume reduction is seen (differential diagnosis: cystic fibrosis). Enlarged lymph nodes are rare. Silicosis can be ruled out by history of occupational exposure.

Langerhans cell histiocytosis. a Chest X-ray posteroanterior view shows reticulo-nodular opacities with peribronchial nodules. b Axial CT image in lung window shows some solid nodules (arrows); other nodules with cavitation (arrowhead)
8.5 Treatment
There is no definitive therapy. Spontaneous remission is possible. In case of respiratory restriction, immune-suppressive therapy is indicated.
8.6 Sarcoidosis
8.6 Definition, Epidemiology, and Pathogenesis
Sarcoidosis is a multisystem granulomatous disease. Histologically, the granulomas are characterised by increased CD8 cells in the periphery and CD4 cells in the centre.
Sarcoidosis is a disease of young people with peak incidence between 20 and 40 years. Women are slightly more affected than men. Black people are affected more than Caucasians; in addition blacks are more prone to fibrosis.
The aetiology of sarcoidosis is unknown. A genetic predisposition, viral infection, or infection with mycobacteria are proposed. Activated macrophages, monocytes, and lymphocytes accumulate in the interstitium, alveoli, and vessels. Noncaseating granulomas form and are characterised by monocytic giant cells of Langerhans. The lung is the most affected organ. In stage I, two thirds of patients show spontaneous remission within a few months (. Fig. 19.76 ). In advanced stages, remission is seen in only about half of the patients. Residual reduction of lung function can be seen.

Schematic representation of sarcoidosis type I–III
8.6 Clinical Presentation
The symptoms are nonspecific in the early stages. Later, symptoms depend on the affected organ. There are two forms, acute and chronic. In acute sarcoidosis, also known as Löfgren’s syndrome, there is erythema nodosum, monoarthritis, and enlarged hilar lymph nodes, most commonly in young women. It is usually associated with flu-like symptoms. The chronic form is usually characterised by nonspecific symptoms such as fatigue, cough, low-grade fever, etc. The diagnosis is often incidental on chest radiography.
In addition, there may be peripheral lymph node enlargement, involvement of the eyes with iridocyclitis and uveitis, the nervous system, renal and myocardial granuloma formation.
8.6 Imaging
The most common finding is intrathoracic lymph node enlargement. This appears on chest X-ray as hilar enlargement (Fig. 19.77) with lobulation, or obliteration of the aorto-pulmonary window. The lymph nodes may also calcify during the course of the disease. Sarcoidosis can cause a variety of parenchymal pulmonary changes. The following findings may be detected on CT:

Sarcoidosis. a Type I sarcoidosis. Chest X-ray posteroanterior view shows bilateral well-circumscribed, smoothly enlarged hilar shadows due to bihilar lymphadenopathy (arrows). b Type III sarcoidosis. Chest X-ray posteroanterior view shows bilateral hilar enlargement and interstitial fibrosis with honeycombing. c Type III sarcoidosis. Axial CT image in lung window shows diffuse bilateral centrally located infiltrates with interstitial thickening
-
Bilateral, diffuse, ground-glass opacities with irregular contour and without characteristic distribution pattern
-
Associated fine nodular interstitial pattern along the bronchi
-
Apical involvement similar to tuberculosis is possible
-
Reticulo-nodular pattern, usually bilateral and symmetric
-
Nodule-like opacities with a tendency to cavitate may be seen
-
Irreversible fibrotic bands, directed from the hila towards the apices, with formation of traction bronchiectasis and/or bullae
-
Transition to a honeycomb lung
-
In rare cases, pleural involvement with pleural effusion
Compression of vessels or bronchial structures is possible as a complication.
Radiologic stages of sarcoidosis
Stage I:
-
Bilateral hilar lymphadenopathy with enlarged, well-demarcated hila (Fig. 19.77).
-
Widened mediastinal shadow by mediastinal lymphadenopathy
-
Partially calcified lymph nodes
-
Rarely associated alveolitis with ground-glass pattern
-
Spontaneously reversible
Stage II:
-
Perihilar small granulomas
-
Increased interstitial reticular shadows
-
Associated small nodules
-
In rare cases, large nodules that may resemble bronchial carcinoma
-
In the mean time, regressive course of the hilar lymphadenopathy
-
Steady decrease in hilar lymphoma
-
On CT, up to 2 mm, perivascular and peribronchial nodules, which can simulate lymphangitis carcinomatosis
Stage III:
-
Transition to irreversible, predominantly central lung fibrosis
-
Striated bands stretching from the hila
-
Honeycomb pattern
8.6 Further Diagnostic Measures
After a positive X-ray finding, bronchoalveolar lavage may be performed and shows a macroscopic cobblestone-like pattern of the bronchial mucosa. Lymphocytes are increased to more than 50% of the cells, with T-lymphocytes more than two-thirds. The higher the CD4/CD8 ratio is, the more likely is sarcoidosis. Conversely, the CD4/CD8 ratio is decreased in silicosis. Laboratory tests show an elevated ESR, IgG, and angiotensin-converting enzyme (ACE). For evaluation of activity, Gallium scintigraphy may be used. In cases associated with ACE elevation, it may be used for monitoring activity.
In addition, other organs should be screened for the disease and tuberculosis should be excluded. In some cases, definitive diagnosis is only possible by the histologic proof of noncaseating granulomas through tissue biopsy.
The Kveim test, named after the Norwegian Morten Kveim, was used in the past for diagnosis of sarcoidosis, where pasteurised sarcoid tissue was injected subcutaneously. With active sarcoidosis, red induration appears after few weeks in about two-thirds of patients, histologically identified as granuloma. Because other lymphadenopathies such as tuberculosis or leukaemia show positive results, this test is no more reliable.
8.6 Treatment
Corticosteroids are used for symptomatic cases. After response to treatment, follow-up is indicated every 6 months.
8.7 Lymphangioleiomyomatosis
8.7 Definition and Pathogenesis
Lymphangioleiomyomatosis (LAM) is a disease that affects almost exclusively women between 30 and 40 years. It is characterised by uncontrolled proliferation of atypical smooth muscle fibers in the lungs, the bronchi, and the lymphatic/vascular systems. LAM was first described in 1937. It leads to bronchiolar narrowing due to peribronchial smooth muscle proliferation leading to the formation of emphysematous cysts. Intrapulmonary vessels are also affected, leading to development of pulmonary hypertension. Occasionally the thoracic duct is dilated. LAM can also affect extrapulmonary organs such as the uterus, kidneys, and pancreas. Associated angiomyolipomas of the kidneys are common. There are two different types of LAM, a rare sporadic variant, and another form in tuberous sclerosis patients. In the sporadic variant, atypical oestrogen receptors can be detected in the lung tissue or in the affected extrapulmonary organs. The mean survival time is about 10 years after the first diagnosis.
8.7 Clinical Presentation
Clinical symptoms may precede the radiographic findings by a long time; patients may complain of progressive dyspnea, spontaneous pneumothorax or chylothorax.
8.7 Diagnosis and Imaging
There are neither specific laboratory tests nor characteristic pulmonary function tests. The differential diagnosis of CT-detected pulmonary cyst formation is histiocytosis-X (Fig. 19.78). Cystic changes of LAM have, however, no apical predilection as with histiocytosis. Emphysematous changes must be recognised, which is difficult in early stages of the disease.

Lymphangioleiomyomatosis. Axial CT image in lung window shows fine reticulo-nodular pattern of the lungs, with transition to a honeycomb pattern
The final diagnosis depends on lung biopsy.
Chest X-ray:
-
Reticulo-nodular pattern
-
Associated pleural effusion or pneumothorax
-
Transition into honeycomb pattern
-
Increased lung volume
HR-CT:
HRCT may also show characteristic changes that are unrecognised on chest X-ray. In the early stage the picture is similar to that of emphysema with small, thin-walled, polygonal cysts; evenly distributed over the entire lungs, with a wall thickness of up to 2 mm and a size rarely larger than 5 cm in diameter. The remaining parenchyma is normal. Occasionally, involvement of the lymphatic structures leads to interstitial thickening, Kerley lines, and pleural effusion.
8.7 Treatment
There is no definitive treatment. So far, patients were treated with medroxyprogesterone with moderate success. Another experimental drug is Rapamycin. The only treatment for end-stage disease is organ transplantation.
9 Neurocutaneous Syndromes (Neurofibromatosis, tuberous sclerosis)
Neurocutaneous syndromes are a group of hereditary disorders characterised by involvement of the neuroectodermal organs. These include phacomatosis syndromes such as neurofibromatosis, Sturge-Weber-Krabbe syndrome, tuberous sclerosis syndrome, and von Hippel-Lindau syndrome. Other neurocutaneous syndromes include Leschke syndrome, Maffucci syndrome, Klippel-Trenaunay syndrome, Osler-Weber-Rendu and Peutz-Jeghers syndrome.
Lung involvement may be seen especially with neurofibromatosis, tuberous sclerosis, and Bourneville-Pringle’s disease.
Neurofibromatosis is an autosomal dominant inherited disease. The disease is characterised by development of fibromas along the peripheral nerves, cutaneous fibromas, and the characteristic “Cafe au lait” patches. The lung is affected in approximately 20% of patients with pulmonary fibrosis. In a few cases the changes progress centrally with associated bullous changes. The mediastinum and the chest wall may also be affected. Neurofibromas may form in the middle and posterior mediastinum, as well as along the chest wall.
Tuberous sclerosis is a rare, autosomal dominant inherited disorder that in most cases results in death before the age of 20. The disease is characterised by adenoma sebaceum, epilepsy, and mental retardation. In rare cases, it leads to involvement of the lung parenchyma with a lymphangioleiomyomatosis-like picture.
10 Alveolar Microlithiasis
10 Definition and Pathogenesis
Alveolar microlithiasis is a rare disease; in about half the cases hereditary. It is characterised by intra-alveolar accumulation of calcium phosphate microliths, with reactive fibrosis of the surrounding interstitial tissue. There is usually a discrepancy between the severe radiologic changes and the milder clinical picture.
10 Imaging
The chest X-ray shows the “sandstorm-like” picture; with micronodular, calcified densities; typically blurring the mediastinal contours.
CT reveals centri-acinar microliths with interstitial fibrosis and ground-glass opacities.
11 Alveolar Proteinosis
11 Definition and Pathogenesis
Alveolar proteinosis is a rare disease characterised by intra-alveolar accumulation of protein and phospholipid-rich material. It may be related to increased production by the alveolar macrophages or decreased absorption. Men between 20–50 years are more commonly affected. However, the disease was also described in children.
11 Clinical Presentation
The symptoms are nonspecific with progressive dyspnea, fatigue, weight loss, and hypoxia. Restrictive changes are seen in pulmonary function tests. Secondary infections are common.
11 Imaging
Chest X-ray: this shows perihilar opacities, more pronounced centrally, with a reticular component. Infiltrates may change in their location with time.
CT: this shows ground-glass opacities, associated with a reticular pattern due to interlobular septal thickening. Reticulations superimposed on ground-glass opacities are called a “crazy paving” pattern with a geographic distribution. Pathologic areas alternate with completely inconspicuous lung parenchyma.
11 Treatment
There is no definitive therapy. The method of choice is therapeutic bronchoalveolar lavage, which must be carried out several times.
12 Pulmonary Neoplasms
12.1 Imaging Findings
12.1 Pulmonary Nodules (see also Sect. 19.4.3)
The sensitivity of lung nodule detection by conventional radiography for nodules < 6 mm is extremely low, but the sensitivity increases when the nodule is calcified. With a diameter of 6–10 mm, about 50% are detected by conventional radiography. For nodules > 10 mm, the sensitivity is almost 100% (. Table 19.20 ).
CT offers the best accuracy for detection of nodules. The sensitivity of CT for detection of nodules < 6 mm is about 70%, and increases to 95–100% for nodules > 6 mm nodules. The most problematic nodules are solitary, centrally located, perivascular nodules. The sensitivity of MRI is lower for nodules < 6 mm, it increases up to 85–100% for lesions with a diameter > 6 mm (. Fig. 19.79 ).

MRI of a pleural-based nodule. Axial T2-weighted MRI image shows homogeneous high-signal pleural-based nodule
Modern cross-sectional imaging is based on multislice CT with its high resolution. CT may be used for screening for pulmonary nodules in people at risk.
In addition to the detection of pulmonary nodules, diagnostic imaging should also aim at identification of the imaging criteria of other nodules in order to achieve an exact differential diagnosis or aetiology (. Tables 19.21–19.26 ). For example, the diagnosis of pulmonary metastases in CT may be based on morphologic criteria (Fig. 19.80), as well as analysis of i.v. contrast enhancement and tumour volumetry on follow-up (Table 19.25). The differential diagnoses must include the most common benign nodules such as intrapulmonary lymph nodes, focal infections, and the various forms of granulomas and benign tumours, such as hamartomas (Table 19.21). Intrapulmonary lymph nodes are characterised by their shape, basal distribution, and the size maximum of up to 12 mm. The most common primary malignant processes in the lung are bronchial carcinoma, carcinoid tumour, and malignant lymphoma. Important characters for the differential diagnosis include the distribution pattern, localisation, and morphology.

Pulmonary metastases from renal cell carcinoma. Axial CT image in lung window shows multiple, rounded, smoothly bordered, well-circumscribed nodules, most are peripheral (subpleural) in location. A known case of intrapulmonary metastasis of renal cell carcinoma
An important criterion in the differential diagnosis of pulmonary nodules is tumour volumetry on follow-up. It is suggested that the tumour doubling time for malignant neoplasms is between 20–400 days, the standard deviation is 7–2800 days. Conversely, benign nodules lack the increase in volume with time, especially granulomas. Rapid increase in volume is seen with inflammatory processes (Table 19.22). Hamartomas and intrapulmonary lymph nodes are characterised very slow increase in size.
12.1 Solitary Pulmonary Nodule Diagnosis
The characterisation of pulmonary nodules is currently based on multislice CT, although the specificity continues to be limited. The information retrieved by CT on pulmonary nodules is curtailed by the limits of spatial resolution.
Nodules containing fat can be diagnosed as hamartoma or lipoid pneumonia with high diagnostic accuracy (Fig. 19.81). Nodules with large coarse calcifications can be diagnosed as calcified granulomas, especially if there is no significant contrast enhancement (< 15 H.U.). Conversely, coarse calcifications and endobronchial location with considerable enhancement is characteristic of carcinoid tumour. With atypical calcification pattern and no soft tissue component, osteosarcoma metastases must be considered.

Lipoid pneumonia. Axial CT image in lung window shows a large mass with predominantly low density and small central calcium density (arrows)
Size and Growth of the Nodule.
One of the diagnostic criteria for classification of a pulmonary nodule is the size of the nodule. As a rule, an incidentally discovered solitary nodule with a size < 10 mm should be considered benign. A solitary nodule with a diameter < 30 mm is suspicious for malignancy. The growth rate of a nodule is also important for the differentiation of benign and malignant nodules. The volume doubling time for benign lesions is about 300–700 days, while that for malignant lesions is between 20–400 days.
As a general rule, volume doubling in less than 20 days or more than 500 days is a sign of benignity with high reliability.
Outer Contour of the Nodule.
Another important criterion for differentiation of benign from malignant nodules is the outer contour of the nodule. Nodules associated with fibrotic changes have predominantly concave outline. Neoplastic lesions, on the other hand, have a predominantly convex outline.
Other Imaging Criteria.
Other additional criteria may help in the differential diagnosis of pulmonary nodules, for example, a “feeding vessel” sign is highly suggestive of arteriovenous malformation.
Analysis of contrast enhancement in CT is performed using soft tissue window images. The attenuation of nodules is measured by the so-called “regions of interest” (ROI), before and after administration of contrast medium. The attenuation difference is calculated and analysed. According to the literature, contrast-enhancement of > 15 H.U. is in favor of malignancy, with 98% sensitivity and a specificity of 58% (Table 19.22).
-
Benign lesion: < 15 H.U. enhancement
-
Grey zone: 16–25 H.U. enhancement
-
Malignant lesion: > 25 H.U. enhancement
The use of MRI for characterisation of pulmonary nodules has not been evaluated extensively and is currently under investigation. The use of positron emission tomography (PET) enables the acquisition of further additional information about the metabolic activity of a lesion. However, some benign lesions with high metabolism can be PET positive.
Another criterion for the evaluation of pulmonary nodules is the frequency: solitary pulmonary nodules are, in most cases, granulomas, followed by, in descending order of frequency, bronchial cancer, hamartoma, and metastasis.
12.1 Interventional Radiology of Pulmonary Nodules
The work-up for evaluation of suspicious pulmonary nodules include diagnostic and interventional imaging. Percutaneous biopsy guided by CT proved to be very effective (Figs. 19.82 and 19.83). Both fine needle aspiration or core biopsy are possible. It is important during planning the procedure to choose the shortest possible puncture path through the lung parenchyma, preferably at right angle to the pleura, and the passage through inflammatory processes should be avoided.

Anterior mediastinal mass. Clinical history of gastric pull-up after surgical excision of carcinoma of the gastric cardia. Now suspected recurrence. a Chest X-ray posteroanterior view shows air-fluid level on the right side due to gastric pull-up. Additionally, there is suspected pulmonary metastasis in the right lung base (nodule R). On the left there is opacity cranial to the aortic arch (arrowheads). b Chest X-ray lateral view confirms the gastric shadow as an anterior radiolucent zone (arrows). c Coronal MR image shows the aerated right mediastinal gastric interposition (arrows), and additional marginally enhancing anterior mediastinal mass lesion. d CT-guided biopsy of the left anterior mediastinal mass proved its neoplastic nature. Note the right metastatic lung nodule (R)

Pleural-based nodule. a Axial CT image shows a right pleural-based nodule with smooth margins and homogeneous structure. b CT-guided needle biopsy: the needle position inside the tumour is verified. Histology: pleural fibroma
Relative contraindications for performing biopsy include the puncture path traversing the interlobar septum, gross reduction in lung function, single functioning lung, and; in particular, signs of pulmonary hypertension. The risks from lung biopsy procedure include the development of radiologically evident pneumothorax in about 30–50%. However, those requiring therapy are only 3–4%. Minimal bleeding into the lung parenchyma is observed in up to 70%, but haemoptysis in only 2–4%. The risk of air embolism is less than 1%.
12.2 Benign Pulmonary Tumours
Benign lung tumours are uncommon. The diagnosis can often be made only histologically. They include hamartomas, papillomas, lipomas, neurofibromas, haemangiomas, and endometriosis.
12.2 Hamartomas
12.2 Definition
Hamartomas are relatively common benign mixed tumours without infiltrative growth. Pulmonary hamartomas consist of fibrocyte cells from the bronchial walls, chondrocytes, smooth muscle, and fat.
12.2 Imaging
On imaging, hamartomas are lobulated nodules < 4 cm, which are usually unilateral and occur in the lung periphery (Fig. 19.84). Coarse lumpy popcorn calcifications are associated with the cartilaginous component. Depending on the composition of the tumour, contrast enhancement on CT is possible.

Hamartoma. Chest X-ray posteroanterior view shows a well circumscribed left para-hilar nodule with smooth outlines
It is important to detect the presence of fat content within the lesion on CT so as to exclude malignancy.
12.2 Haemangiomas
Haemangiomas usually appear as peripheral nodules, and often are misdiagnosed as metastases. The evidence of connection to a major vessel is rarely present.
12.3 Malignant Diseases of the Lungs
12.3 Lymphangitis Carcinomatosis
12.3 Definition and Pathogenesis
Lymphangitis carcinomatosis refers to the infiltration of lymphatic vessels by malignant cells. This may be seen in carcinomas of the bronchi, breast, stomach, and prostate, due to haematogenous spread. The prognosis is poor without or with treatment.
12.3 Clinical Presentation
The clinical picture is usually nonspecific, with dry cough and fatigue. Not infrequently, lymphangitis is completely symptomless.
12.3 Imaging
Chest X-Ray:
-
Interstitial up to reticular pattern
-
Kerley’s B lines
-
Associated pleural effusion on the affected side
-
Mostly unilaterally
CT:
-
Relatively homogeneous thickened broncho-vascular perihilar structures
-
Thickened fissures and interlobar septa
-
Scattered nodules
Tumour infiltration of mediastinal lymph nodes causes their enlargement. The differential diagnoses include other pulmonary interstitial diseases such as pulmonary oedema and sarcoidosis.
12.3 Bronchial Carcinoma
Imaging is a corner-stone in the diagnosis, differential diagnosis, and follow-up of thoracic malignancies, in addition to procedures such as bronchoscopy or mediastinoscopy (Figs. 19.86 and 19.87).

Lymphangitis carcinomatosa. a Chest X-ray posteroanterior view shows diffuse infiltrates of both lung fields (L > R). b Axial CT image in lung window shows diffuse interstitial thickening on both sides

Bronchial carcinoma. Axial CT image in lung window shows a large mass in the right upper lobe with speculated margins or corona radiata

Bronchial carcinoma with stenosis of the pulmonary artery. a Axial CT image in soft tissue window shows advanced central bronchial carcinoma with mediastinal infiltration and stenosis of the left pulmonary artery (arrows). b Axial T2-weighted MR image shows solid hypointense lesion (arrow) with associated pleural effusion (arrowheads). c MR angiography (CE-MRA): verification of stenosis of the pulmonary artery (arrows)
Conventional radiography gives limited information. CT and, in some cases, MRI are the primary imaging modalities.
Bronchial carcinoma is the most common cancer in males. In addition to early detection, imaging should be targeted at the therapy-relevant criteria. These include surgical resectability, response to chemo- and radio-therapy, and early detection of recurrence.
12.3 Staging
12.3 Imaging Staging
Knowledge of the current TNM staging of bronchial carcinoma is one of the requirements for interpretation.
The staging applies only to bronchial carcinomas; prior histopathologic diagnosis and typing is required.
Methods for assessing the T, N, and M categories (Tables 19.27 and 19.28) are:
Clinical examination, imaging techniques, endoscopy and/or surgical exploration
12.3 Clinical Classification
For staging of the primary tumour (T) refer to Table 19.27, for nodal and metastatic spread Table 19.28.
12.3 Pathological Classification
The pathologic staging corresponds to the same TNM stages. pN0: Regional dissection and negative histologic examination of six or more lymph nodes.
12.3 Histopathologic Grading
Grading is defined as follows:
-
GX: degree of differentiation cannot be evaluated
-
G1: Well differentiated
-
G2: Moderately differentiated
-
G3: Poorly differentiated
-
G4: Undifferentiated
12.3 Staging Grouping
The tumour stages are derived from the TNM classification of bronchial carcinomas (Table 19.29).
Evaluation of the lymph node status is essential for staging. It is important to differentiate N0 from N1, N2, and N3. It is worth noting that normal hilar or mediastinal lymph nodes are usually hardly visualised by CT. The morphology and size of the lymph nodes are still currently used as criteria for infiltration. Central necrosis is rare and nonspecific. False-positives results occur with hyperplastic lymph nodes, while false-negative results occur with micrometastases.
The use of CT as a rule allowed accurate detection of the TNM and end stage only in 50–60%.
Earlier classification
Until recently, classification by the Veterans Administration Lung Cancer Study Group was used for the classification of small cell bronchial carcinomas. This has now been abandoned in favor of the TNM classification.
“Limited disease”
-
Primary tumour confined to one hemithorax
-
Ipsilateral hilar lymph nodes
-
Ipsilateral supraclavicular lymph nodes
-
Ipsilateral and contralateral mediastinal lymph nodes
-
Existing atelectasis
-
Nerve injury such as recurrent laryngeal and/or phrenic nerve palsy
-
Small effusion without malignant cells
“Extensive disease”
-
Contralateral hilar lymph nodes
-
Contralateral supraclavicular lymph nodes
-
Chest wall invasion (also ipsilateral)
-
Pleural metastases
-
Lymphangitis carcinomatosis
-
Superior vena cava syndrome
-
Contralateral metastases
-
Distant metastases (liver, brain, bones, other lymph nodes, etc.)
12.3 Importance of Imaging for the Diagnosis and Treatment Planning
The use of multislice CT with secondary reconstruction, and in addition, the possibility of virtual bronchoscopy, has led to significant improvement in results of diagnostic imaging. In particular, imaging data should be used to allow distinction between candidates for lobectomy and those for pneumonectomy, and to evaluate the exact criteria of resectability. Factors that mandate pneumonectomy include invasion of the pulmonary vessels, involvement of the upper and lower lobe bronchi, or involvement of the main bronchus with a distance < 2 cm from the carina.
The CT scan technique for assessment or detection of primary bronchial neoplasms should be performed with intravenous contrast administration (60–100 ml of contrast medium at a flow rate 2 mm/s, with delay 30–50 s). Techniques for data reconstruction include multiplanar reconstruction (MPR) and maximum intensity projection (MIP). CT angiography (CTA) may also be performed when indicated.
12.3 Adenocarcinoma
12.3 Definition and Epidemiology
Adenocarcinoma is the most frequent lung cancer in nonsmokers. Often middle-aged women are affected. The tumours are usually located peripherally. The origin is unclear. Adenocarcinomas are relatively common in pulmonary parenchymal scar.
12.3 Imaging
Chest X-ray:
-
Peripheral mass
-
Slow growth, but early metastasis
-
Radiating strands in terms of spicules or corona radiata
-
Displaced lung fissures
Alveolar cell/bronchoalveolar carcinomas are uncommon tumours that originate from alveolar epithelium and adjacent bronchioles (Fig. 19.88). Patients present with cough, sometimes with expectoration of copious thin mucus, chest pain, and haemoptysis. The chest radiograph may show a solitary nodule or multiple small nodules up to diffuse areas of consolidation. The nodules increase in number in the lung bases. Another picture is pneumonia-like spread with patchy opacities. Large nodules are ill defined, have bubble-like lucencies or air bronchograms; they are partly confluent, bilateral but more prominent on the right side. On CT, it may appear as a solitary nodule with positive air bronchogram, with radiating strands and retraction of the pleura. Alternatively, a “crazy paving” pattern is seen, caused by mixed alveolar and interstitial opacities or a pneumonia-like spread.

Alveolar carcinoma. a Chest X-ray posteroanterior view shows an area of ill-defined opacity in the left lung. b Axial CT in lung window shows diffuse alveolar and interstitial infiltrates
12.3 Secondary Neoplasms (Metastases)
12.3 Lung Metastases
The diagnosis of lung metastases represents one of the most important tasks of diagnostic radiology.
For the diagnosis of pulmonary metastases, the chest radiography and CT are most commonly used (Figs. 19.80, 19.89, and 19.90). In individual cases, MRI may be used as a complementary method. Positron emission tomography (PET) or PET-CT is increasingly used for metastatic work-up and is especially beneficial for detection of mediastinal and hilar lymph node metastases.

Calcified pulmonary metastasis. Axial CT in lung window shows partially calcified, left perihilar metastatic nodule (arrows), in a patient with vaginal cancer
The detection of a lung nodule is a particular challenge to the knowledge of the radiologist. Inflammatory and other benign causes as well as vascular structures should be differentiated from primary and secondary malignant tumours. The radiographic finding of single or multiple pulmonary nodules during initial diagnosis or follow-up of cancer patients’ diagnosis has a significant impact on the oncology treatment decision. Further evaluation is then usually performed by CT for accurate diagnosis. CT examination is optimised by the intravenous administration of contrast medium, secondary multiplanar reconstructions, and volumetric studies.
Typical criteria of lung metastases include the rounded configuration, the sharp boundaries, and the absence of cavitation, as well as the multiplicity. Another important criterion is the location. Metastases are most commonly peripherally located, perivascular, perilymphatic, and typically basal.
Atypical findings with lung metastases include cavitation, either spontaneous or after treatment. In rare cases, spontaneous pneumothorax occurs that gives the indication of the presence of metastatic sarcoma. Another atypical finding includes the occurrence of endobronchial metastases. These may be seen with malignant melanoma, renal cell carcinoma, and breast cancer. They may cause bronchial obstruction with distal segmental or subsegmental atelectasis. Calcifications within metastases are common with osteosarcoma, ovarian cancer or treated metastases with secondary calcification. Cavitation may be seen in metastases from several primary tumours, such as colorectal cancer as well as endobronchial metastases. Haemorrhagic metastases have ill-defined, blurred borders on CT, so the appearance is atypical. Pleural metastases occur with different frequencies in different tumours.
Primary Tumours.
The finding of peripheral lung nodules/metastases, without known primary tumour, is due to breast cancer in about 20% of patients. The radiologic literature points to the role of experienced radiologists in characterisation of lung nodules. In a few cases, however, histologic confirmation is needed.
Data on primary tumours and probability of pulmonary metastases are shown in Tables 19.30, 19.31 and 19.32.
Follow-Up.
The following points are important to consider when evaluating follow-up examinations of lung metastases:
-
The location and size of lung metastases (CT is the procedure of choice)
-
Metastases of highly vascularised tumours, such as thyroid carcinoma tend to present with multiple small lung metastases
-
The patient’s age and prognosis
12.3 Kaposi’s Sarcoma
12.3 Definition and Pathogenesis
Kaposi’s sarcoma is a disease often associated with HIV infection. The incidence has significantly decreased with improved antiretroviral therapies. The incidence is still high, however, with low CD4 counts (< 200). Men are more commonly affected than women. The pathogenesis is still not clear; the current theories suggest the origin to be from herpes (HHV-8)-infected monocytes, or endothelial cells or smooth muscle cells.
The disease presents with cutaneous reddish macules or plaque-like lesions which may later ulcerate. Visceral involvement may occur especially of the gastrointestinal tract, lungs, and lymph nodes. Involvement of the lungs results in centrally located hypervascular nodules along the bronchovascular structures.
Stages of HIV infection
-
1.
Asymptomatic HIV disease without clinical symptoms and with > 500 CD4 cells/μl
-
2.
HIV infection with diseases and symptoms not specific to AIDS, but related to weak cellular immunity, such as herpes zoster or idiopathic thrombocytopenic purpura, symptoms such as fever and diarrhoea lasting more than a month
-
3.
AIDS disease in severe immune deficiency
The number of CD4 cells is less than 200 cells/μl. The AIDS-defining diseases include opportunistic infections, such as CMV infection, Candida infection of the oesophagus and tracheobronchial system, histoplasmosis, atypical mycobacteria, Pneumocystis carinii and cryptococcal lung infections, and cerebral manifestation of toxoplasmosis. Tumourous AIDS-defining diseases include lymphomas, particularly Burkitt’s lymphoma, cerebral lymphoma, and immunoblastic lymphoma. Another disease that affects the central and peripheral nervous system is progressive multifocal leucoencephalopathy.
12.3 Clinical Presentation
Kaposi’s sarcoma involving the lung will present with nonspecific symptoms such as cough, haemoptysis, and sometimes fever.
12.3 Imaging
Kaposi’s sarcoma appears on the chest radiograph as poorly demarcated, basal distributed, nodules with a size of approximately 1 cm. In approximately 50% of patients, there is associated small pleural effusion (. Fig. 19.91 ) and mediastinal lymph nodes.

Calcified pulmonary metastasis. Axial CT in soft tissue window shows heavily calcified left basal metastasis (arrows) in a patient with colorectal carcinoma

Kaposi’s sarcoma. a Chest X-ray posteroanterior view shows diffuse opacities in the right lung base with right-sided pleural effusion. b Axial CT in lung window shows a right basal nodular lesion with unsharp borders (arrows)
HRCT shows ill-defined flame-shaped nodules along the bronchovascular bundle, with infiltrative characters as well as interstitial parenchymal changes.
12.3 Lymphoma
12.3 Definition and Pathogenesis
Lymphomas are multisystem diseases, which often involve the intrathoracic lymph nodes in the mediastinum and hilum. In younger patients, in the 2nd or 3 decades of life, Hodgkin’s lymphoma is more common (. Table 19.33 ), while in patients older than 60 years, non-Hodgkin lymphoma is more common.
In addition, supplementary features are denoted:
A: Without accompanying symptoms
B: General symptoms such as fever, night sweats, weight loss
Non-Hodgkin lymphoma is currently evaluated according to the criteria established by WHO classification into low risk, intermediate risk, and high risk lymphoma, depending on the dominant cell type (Table 19.34).
12.3 Imaging
Typically there is widening of the mediastinum due to involvement of the mediastinal lymph nodes with lymphoma. There may also be convex opacity in the aorto-pulmonary window, opacity in the retrosternal space, and hilar enlargement. Occasionally, there is extension into the surrounding lung tissue, which results in thick linear pulmonary opacities.
CT enables earlier diagnosis of pulmonary infiltration (. Figs. 19.92 and 19.93 ). It reveals intrapulmonary nodules that vary in number, size, and shape, from a single nodule to multiple military-sized nodules and up to large masses. Bronchi are characteristically not obstructed.

Pulmonary lymphoma nodule. Axial CT in lung window shows right intrapulmonary nodule, with unsharp borders due to its infiltrative character and bronchiectatic changes (arrows)

Malignant lymphoma infiltration. a Chest X-ray anteroposterior view shows pulmonary infiltrates on both sides, bilateral, ill-defined, diffuse, confluent pulmonary infiltrates. b Axial CT in lung window shows patchy infiltrates in the right lung, confluent on the left side
13 Circulation Disorders
13 Pulmonary Hypertension
13 Definition and Pathogenesis
Pulmonary hypertension is defined as elevation of the mean pulmonary artery pressure above 25 mmHg at rest. It can be either primary, without identifiable cause or secondary to obstruction of the pulmonary vessels due to pulmonary embolism or destruction of the lung parenchyma by emphysema or fibrosis. An increased blood flow due to left-right shunt also leads to pulmonary hypertension. Chronic hypoventilation can induce reflex constriction of the pulmonary vessels and cause pulmonary hypertension. This may occur in uncommon conditions such as Pickwickian syndrome, chronic hypercapnia, or living in high altitudes.
13 Clinical Presentation
Patients complain of significant exertional dyspnea, with increase in right heart strain up to failure. This leads to ascites, leg oedema, and haemoptysis.
13 Imaging
Signs of pulmonary hypertension in chest X-ray include:
-
Dilatation of the right descending pulmonary artery > 15 mm
-
Narrowing of the retrosternal lucent area in the lateral view
-
Enlargement of the cardiac shadow (right atrium and right ventricle)
-
Dilatation of the azygous vein > 7 mm
-
Change in calibre of the vessels, vessels are significantly larger centrally and smaller in calibre peripherally
13 Pulmonary Oedema
13 Definition and Pathogenesis
Pulmonary oedema is defined as abnormal interstitial and alveolar accumulation of fluid. Causes of pulmonary oedema include:
-
Pressure increase in the capillaries from pressure rise in the left atrium due to reduced output through the left heart:
-
Left ventricular failure
-
Mitral stenosis
-
-
Increased capillary membrane permeability, with increased filtration pressure. Possible causes are:
-
Toxic gases inhalation (e.g., phosgene, chlorine gas, nitrogen dioxide)
-
Aspiration (e.g., gastric juice)
-
Drugs
-
Hypoxia
-
-
Reduced oncotic pressure, for example in:
-
Renal insufficiency
-
Iatrogenic overhydration
-
Impaired lymphatic flow
-
13 Clinical Presentation
The patients present with progressive dyspnea, tachycardia, frothy sputum, and cyanosis. Coarse bubbly crackles are auscultated.
13 Diagnosis
Pulmonary Congestion
With cardiac decompensation, pulmonary oedema develops slowly starting in the stage of cardiac pulmonary congestion with pulmonary venous redistribution, then proceeding to the stage of interstitial oedema then intra-alveolar oedema.
The diagnosis of developing pulmonary congestion is difficult. In such cases, the combination of several radiographic findings is significant for diagnosis, while each finding alone is not. Enlargement of pulmonary vessels may be seen, which may be more conspicuous if previous radiographs are available for comparison. In general, more vessels become visible in pulmonary venous hypertension. The vessels in the upper lung zones are normally smaller than lower zones due to the higher hydrostatic pressure in the lower zones. With pulmonary congestion, redistribution of flow occurs and the upper zone vessels become enlarged (Fig. 19.94).

Blood flow redistribution. Chest X-ray posteroanterior view shows also an enlarged heart
Interstitial Oedema
Increased interstitial fluid is visible radiographically in the form of the so-called Kerley lines. Three types of Kerley lines could be differentiated (Fig. 19.95):

Schematic representation of Kerley’s lines of interstitial oedema
-
Kerley A: fine lines in the middle fields pointing towards the hilum
-
Kerley B: delicate horizontal lines, subpleural above the diaphragm in the lower lung fields
-
Kerley C: perihilar interstitial increased lung markings
In frontal radiographs, end-on imaged bronchi appear as indistinct ring shadows with thick walls due to mucosal oedema. The central vessels’ walls appear inconspicuous.
Alveolar Oedema
When fluid accumulates in the alveoli, the chest X-ray shows central opacities producing a characteristic butterfly distribution pattern (Fig. 19.96). Alveolar fluid appears as focal opacities, which can be differentiated from nonaffected areas. The opacities usually do not reach the lung periphery. In addition, basal lung segments are more affected due to the higher hydrostatic pressure.

Pulmonary oedema. a Chest X-ray posteroanterior view shows patchy alveolar shadowing, on both sides. b Chest X-ray supine view 6 hours later shows alveolar pulmonary oedema with diffuse bilateral oedema in a butterfly-like distribution
Chronic Pulmonary Oedema
Chronic pulmonary congestion and oedema may lead to irreversible fibrosis of the lung parenchyma.
Heart Failure
Acute heart failure results in the rapid development of interstitial and alveolar oedema. Interlobular septa are thickened and Kerley B lines are seen (Table 19.35). Furthermore, thickening of the peribronchial interstitium and thickening of the lung fissures are present. Associated pleural effusion is possible.
13 Pulmonary Embolism
13 Definition and Pathogenesis
Pulmonary embolism is defined as the occlusion or narrowing of the lumen of one of the pulmonary arteries by circulating embolic material. The commonest origin of emboli is pelvic or lower limb deep venous thrombosis. Apart from thromboembolism, septic emboli, fat, air, and amniotic fluid emboli are possible causes.
Pulmonary embolism leads to pressure overload on the right ventricle, which can lead to cardiogenic shock. Blood gas analysis shows hypoxemia and hypercapnia.
Mortality, often within the first few hours, depends on the extent of embolism and the presence of associated disorders and can reach up to 90%. Without treatment, pulmonary embolism can lead to irreversible damage to the right heart and recurrent embolism may occur. Therapeutic anticoagulation significantly reduces mortality.
13 Clinical Presentation
The presentation varies depending on the extent. Severe pulmonary embolism results in sudden onset of shortness of breath, chest pain, syncope, tachycardia, and haemoptysis.
13 Diagnosis
At diagnosis, various clinical parameters such as the vital signs, chest X-ray, ECG, and blood gas analysis must be evaluated. It is important to obtain full clinical history, searching for risk factors of thrombosis such as tumours, immobilisation, pregnancy, smoking, oral contraceptives. Venous thrombosis should be ruled out using duplex ultrasound of the leg veins. In up to half of the patients, ECG will reveal right heart strain (S1Q3T3 pattern), right bundle branch block, and sinus tachycardia.
Clinical examination may show clinical signs of deep venous thrombosis such as redness and tenderness of the legs as well as signs of right heart failure with congested neck veins.
Ventilation/perfusion scintigraphy can detect or rule out pulmonary embolism. However, unreliable results are common.
Laboratory investigations include D-dimer. A negative D-dimer can rule out pulmonary embolism. However, some case reports were published reporting the presence of pulmonary embolism with negative D-dimer.
According to the current guidelines for management of suspected pulmonary embolism, the first step for haemodynamically stable patients is correlation between D-dimer and clinical probability. Negative D-dimer in a patient with low clinical probability requires no further assessment. With high clinical probability, regardless of the outcome of D-dimer testing, further investigations are required, including Duplex ultrasound of the legs, CT angiography, or scintigraphy.
D-dimer is a product that results from the proteolysis of fibrin. The sensitivity of D-dimer testing is very high up to 95%. A positive test is of low specificity, but a negative test has high predictive value to exclude pulmonary embolism. It is important to remember that in pregnant women, the D-dimer test is positive physiologically.
Haemodynamically unstable patients require monitoring in an intensive care unit. The first modality for diagnosis is echocardiography to assess right ventricular dysfunction as evidence for diagnosis, and then immediate therapy could be initiated.
13 Imaging
The chest X-Ray image is largely nonspecific, and an unremarkable chest radiograph does not exclude the presence of pulmonary embolism. Signs described in the literature include the Westermark sign, defined as localised decreased vascular markings in the lung parenchyma distal to an occluded artery. The affected artery may be dilated and narrows accordingly. Focal haemorrhage or infiltrate in the affected lung may appear as segmental, wedge-shaped opacity in the lung parenchyma, which is called Hampton’s hump. This pleural-based opacity forms over about one week. There may be associated pleural effusion and/or elevated diaphragm, and in severe cases, dilatation of the azygous vein.
Definitive diagnosis requires pulmonary angiography, which has now been replaced by CT angiography as the gold standard for diagnosis (. Figs. 19.97 and 19.98 ). Pulmonary embolism could be directly diagnosed in contrast-enhanced CT angiography, in the arterial phase, as filling defects in the pulmonary arteries up to the subsegment level. Emboli may also cause complete occlusion with abrupt vessel termination. Indirect signs include enlarged central pulmonary artery, dilated right ventricle, and enlarged superior and inferior vena cava. Associated pleural-based infiltrates or wedge-shaped consolidations may be seen.

Pulmonary embolism. Digital subtraction angiography shows an embolus in the right lower lobar pulmonary artery as a filling defect (arrows)

Large embolus in the left main pulmonary trunk. a Axial CT image in soft tissue window shows a filling defect in the left main pulmonary trunk. b Coronal reconstructed CT image in soft tissue window demonstrates the full extent of the embolus in the left main pulmonary trunk (arrows)
13 Treatment
Urgent anticoagulation therapy with heparin reduces mortality. Extensive embolism may be treated with systemic thrombolytic therapy with streptokinase, rtPA, urokinase, or mechanical thromboembolectomy. Another approach is catheter embolectomy and fragmentation. After therapy, prophylaxis with vitamin K antagonists is indicated.
In emergency, the administration of nitroglycerin spray, pain relief with morphine 2 mg i.v. and sedation may be performed.
No intramuscular injection if thrombolysis therapy is planned.
The treatment planning is based on the haemodynamic function, which is classified as follows:
-
I:
haemodynamically stable without right ventricular dysfunction → anticoagulation with heparin
-
II:
haemodynamically stable with right ventricular dysfunction → consider systemic thrombolysis
-
III:
shock (systolic BP < 100 mm Hg, heart rate > 100 bpm) → systemic thrombolysis
-
IV:
Resuscitation required → systemic thrombolysis therapy even in the presence of contraindications
13 Hepatopulmonary Syndrome
13 Definition and Pathogenesis
Hepatopulmonary syndrome is a disorder of the pulmonary circulation in chronic liver disease. It is characterised by disturbance of gas exchange, intrapulmonary vascular dilatation with resulting arterial hypoxemia. The exact pathogenesis is to date unknown. The syndrome may develop independent of the severity of liver disease; pulmonary involvement is often the limiting factor for patients’ survival time. It is assumed that arterial hypoxemia is caused by intrapulmonary shunting, limited diffusion capacity, and unbalanced perfusion. Intrapulmonary vasodilatation is triggered by complex mechanism of action.
13 Clinical Presentation
Most show nonspecific, mild pulmonary symptoms. Severe cases of arterial hypoxia result in dyspnea with cyanosis and finger clubbing and chest pain on breathing. Cutaneous spider nevi may be seen. The cardiac output is usually increased.
13 Diagnosis and Imaging
Hypoxemia with pO2 < 80 mmHg without causative pulmonary or cardiac dysfunction and with known liver disease raises the suspicion of hepatopulmonary syndrome. Pulmonary function tests reveal normal lung volume and no obstructive changes, but the diffusion capacity is reduced. Blood gas analysis can show a difference between the standing and supine positions, a difference of 5 mmHg is considered significant.
Chest X-ray shows a bilateral interstitial pattern. On CT, there is also an interstitial pattern as well as peripheral dilatation of the pulmonary vessels. The shunting and the intrapulmonary vasodilation could be diagnosed by contrast-enhanced echocardiography. Alternatively, pulmonary perfusion scintigraphy may be performed for diagnosis.
Contrast-enhanced echocardiography is performed after intravenous injection of contrast material. Under normal conditions, contrast appears in the right ventricle only, and due to its large size, the contrast molecules do not pass the pulmonary capillaries. In the presence of right-left shunt, the contrast agent will be detected in the left ventricle. Depending on the time lag for contrast appearance in the left ventricle, the location of the shunt could be inferred. In an intracardiac shunt, contrast arrival in the left ventricle is rapid, while in intrapulmonary shunt, the contrast arrives slowly after a time delay of about 5 cardiac cycles.
13 Treatment
Recovery of the lung may occur after improvement of liver function. In severe hypoxia, oxygen supply is necessary. There is no definitive or specific drug therapy. Experimentally, reduction of the number of bacteria in the intestine by antibiotic treatment was attempted, in order to reduce the production of endotoxins. Moreover, portal hypertension may be lowered by transjugular intrahepatic portosystemic shunt insertion, whereby improvement of oxygenation can be achieved.
13 Adult Respiratory Distress Syndrome (ARDS)
13 Pathogenesis
Adult respiratory distress syndrome or ARDS is an acute respiratory failure in adult patients without previous lung disease. The condition may be due to a variety of causes leading to direct injury such as pulmonary contusion, near-drowning, aspiration, intoxication, or indirect injury such as polytrauma, sepsis, blood transfusions, etc. The result is activation of various processes that lead to abnormal permeability of the pulmonary capillaries and impaired surfactant production, leading to intra-alveolar haemorrhage and parenchymal oedematous exudates.
The development of ARDS proceeds in three stages: in the first stage, increased capillary permeability causes interstitial oedema. Later on, there is reduction in surfactant-producing pneumocytes, which leads to accumulation of fluid in the alveoli. The lack of surfactant leads to formation of microatelectasis and hyaline membranes. In the final stage, there is proliferation of the endothelium and transition into an irreversible process of fibrosis.
13 Clinical Presentation
The condition presents with rapidly progressive severe dyspnea, hypoxemia, cough, and respiratory failure up to intubation necessity due to hypoxemia, hypercapnia, and respiratory acidosis.
13 Diagnosis and Imaging
In the early stages, blood gas analysis plays the most important role in diagnosis. Changes in chest X-ray often appear after a certain time delay (6–12 hours), and are important for monitoring the course of the disease (. Table 19.36).
-
Stage I:
-
After 24 h: progressive dyspnea, tachypnea with moderate hypoxia and respiratory alkalosis
-
Chest X-ray: incipient oedema usually limited to thickened bronchial walls (peribronchial cuffing), with blurred margins of the hila and vessels, heart size normal
-
-
Stage II:
-
After 48 hours: severe dyspnea, orthopnea, and cyanosis
-
Progressive congestion, formation of hyaline membranes
-
Chest X-ray: interstitial oedema with homogeneous opacities and positive air bronchograms
-
-
Stage III:
-
After 36 hours: severe hypoxia and hypercapnia also under oxygen ventilation
-
Chest X-ray: confluent infiltrates, white lungs
-
After about one week, irreversible fibrosis develops with increased reticular shadows. Opacities start to fade out.
13 Treatment
If possible, the underlying cause should be treated. ARDS itself must be treated symptomatically. Particularly important is adequate ventilation of the entire lungs, which may be achieved by having the patients lie on the so-called RotoRest bed for ventilation of the posterior portions of the lungs. Another therapeutic manoeuvre is mechanical ventilation with positive end-expiratory pressure.
14 Iatrogenic Complications
14 Lung Transplantation
Complications after lung transplantation may be divided into acute and chronic. Imaging plays an important role in diagnosis of rejection and other complications, in addition to clinical data.
Complications after lung transplantation are:
-
Rejection
-
Bronchial anastomotic insufficiency: mediastinal and perihilar air collections are important for diagnosis.
-
Bronchial anastomotic strictures: can be demonstrated with multislice CT virtual bronchoscopy.
-
Infections: the risk of infection with bacterial and other opportunistic organisms including CMV increases due to immunosuppressive therapy.
-
Risk of malignancy: lympho-proliferative diseases may occur, related to infection by Epstein-Bar virus. The risk of bronchial carcinoma increases in the transplanted lung.
Hyperacute Rejection
Hyperacute rejection occurs immediately after the transplantation, when the transplant tissue is connected to the recipient circulating blood. Hypersensitivity reaction due to blood group or HLA antibodies occurs and subsequent complement activation and deposition leads to necrosis of the transplanted tissue.
Imaging has virtually no role in diagnosis of hyperacute rejection.
Acute Rejection
This occurs after 40 days on average and presents clinically with cough, dyspnea, fever, and decrease in FFV1. The presence of infection must be excluded. Regression of symptoms under steroid therapy is a proof of rejection. High-resolution CT is the imaging method of choice for radiologic diagnosis, findings include:
-
Air trapping
-
Intra-alveolar opacities (ground-glass opacities)
-
Thickened alveolar septa
Chronic Rejection
Chronic rejection commonly starts about 1 year after transplantation; and presents with slowly progressive decrease in FFV1. Findings on high-resolution CT include:
-
Thickened alveolar septa
-
Thickening of the bronchial walls
-
Dilation of the bronchioles
-
Bronchiolitis obliterans
14 Treatment
Acute rejection may be treated with immunosuppressants such as azathioprine, cyclosporine, and steroids. In chronic rejection, treatment is more difficult. Frequently, re-transplantation is necessary.
14 Postoperative Changes
Interventions involving the pleura often, intentionally or not, lead to extensive fibrous formation. Recurrent pneumothorax may be treated with preventive pleurodesis, in which the pleural cavity is sealed.
Pneumonectomy.
Serous fluid and air develop in the operated side after pneumonectomy. This progressively consolidates and the space partially shrinks due to fibrous formation. This leads to gradual mediastinal shift and elevation of the diaphragm with hyperinflation of the remaining lung showing increased translucency.
Lobectomy/Segmentectomy.
Depending on the location and size of the resected segment, changes may be seen on imaging such as hyperinflation of the remaining lung parenchyma, displacement of the diaphragm, mediastinal shift and displacement of the fissures similar to atelectasis. Follow-up is always important to differentiate postoperative cicatricial changes from possible residual or recurrent disease.
Foreign bodies that were missed during surgery must also be diagnosed.
14 Radiation Injury
14 Pathogenesis
The intensity of radiation injury is dependent on the applied dose and choice of the radiation field and concomitant chemotherapy. Acutely it leads to pneumonitis, which may evolve into postradiation fibrosis.
The exact pathogenesis is not clear. Histologically, there is injury to the alveolar membrane with diffusion of intracellular components into the alveolar lumen. Lytic enzymes are activated simultaneously and surfactant formation reactively increased.
14 Clinical Presentation
The patients suffer from dyspnea, cough, and whitish sputum.
14 Imaging
CT shows pneumonitis usually after the end of irradiation, which does not respect lobar or segmental boundaries. There are extensive, ground-glass opacities up to complete consolidation. After healing, significant fibrosis with volume reduction and retraction of surrounding structures are seen. This commonly occurs in para-mediastinal location after radiotherapy of mediastinal lymphoma.
14 Therapy
Treatment consists of high dose corticosteroids and possibly additional antibiotic treatment.
14 Drug-Induced Pulmonary Changes
Many drugs can induce damage to the lungs. Some examples will be described; detailed information is available at the site of the University Hospital of Dijon/France www.pneumotox.com.
The clinical picture fluctuates from an acute course with fever, cough, sputum, oedema, or spasm, to chronic pain. In chronic cases, usually only a small cough occurs.
Acute changes with oedema or infiltrate formation are described, for example, when taking penicillin, sulfonamides, or hydrochlorothiazide. Chronic damage occurs primarily in the treatment with cytostatics.
Drugs with Lung-Damaging Effects
-
Aminorex: pulmonary hypertension
-
Amiodarone: subacute interstitial pneumonitis, eosinophilic infiltrates, fibrosis, COPD
-
ACE inhibitors: eosinophilic infiltrates, subacute interstitial pneumonitis
-
Methotrexate: acute pneumonitis with respiratory failure, subacute interstitial pneumonia, eosinophilic infiltrates, fibrosis
-
Phenytoin: COPD, eosinophilic infiltrates
-
Salbutamol: acute pulmonary oedema
15 Chest Trauma
15 Pneumothorax
15 Pathogenesis
Pneumothorax occurs when air enters the pleural cavity between the visceral and parietal pleural layers due to external or internal causes. The amount of pneumothorax is variable, ranging from a small amount of air visibly surrounding the lung up to a large amount that can cause total collapse of the lung.
Causes of pneumothorax are:
-
Idiopathic: recurrent pneumothorax, often in thin middle-aged women
-
Iatrogenic (central venous catheter insertion, biopsy, thoracocentesis, mechanical ventilation)
-
Underlying disease (emphysema, bullae)
-
After blunt chest trauma or penetrating chest wall injury (stab wounds, fractured ribs)
15 Clinical Presentation
Symptoms range from mild dyspnea to acute respiratory distress with tachycardia and stabbing chest pain. On percussion, there is hyperresonance on the affected side with diminished breath sounds compared to the other side.
15 Imaging
Expiratory chest X-ray shows a fine line running along the ribs (medially displaced visceral pleura) (Fig. 19.103); the pulmonary vessels do not exceed this line. The line cannot be traced beyond the borders of the thorax (in contradistinction to skin folds). The translucency is increased between the line and the borders of the thorax. The heart borders are well seen. In severe cases, the whole hemithorax is translucent and the lung is collapsed and present in the perihilar region.

Malposition of a nasogastric tube. Chest X-ray posteroanterior view shows a malpositioned nasogastric tube in the right main bronchus (arrows)

Dislocated pacemaker lead. a Axial CT in lung window shows the broken dislocated lead (arrow). b Scout view of CT

Forgotten guidewire after CVC insertion. Lateral chest radiograph

Postoperative hydropneumothorax. a Chest X-ray posteroanterior view shows left hydropneumothorax with air-fluid level. b Lateral chest radiograph

Left pneumothorax. Chest X-ray posteroanterior view shows the visceral pleural line (arrows)
Tension pneumothorax occurs via a ball and valve mechanism, where air enters the pleural cavity in inspiration but cannot exit during expiration. Thereby, the intrathoracic pressure increases, compromising the respiratory function of the intact lung and the heart activity.
Signs are (Fig. 19.104):

Tension pneumothorax. Chest X-ray posteroanterior view shows large right pneumothorax with midline and mediastinal shift (arrows)
-
Mediastinal shift
-
The diaphragm is flattened on the affected side
-
The diaphragm may become concave on the affected side
15 Treatment
With a small pneumothorax, about a finger width in the chest X-ray, usually no treatment is necessary. On the other hand, tension pneumothorax requires immediate puncture of the pleural space to relief pressure. When necessary, drainage of air is performed by intercostal chest tube drainage or aspiration. A chest tube can be connected into the Heimlich one-way valve or water-seal system. Smaller bore tubes can be used in patients with smaller pneumothoraces. Follow-up is necessary with chest X-ray. Recurrent or nonresponding cases may be treated with thoracoscopic closure of leaks or pleurodesis.
15 Fractures
Rib Fractures.
Rib fractures are common with trauma. Without history of trauma, one should consider pathologic fractures. Besides the fracture itself, associated findings should be carefully sought for in the chest X-ray; including adjacent area of lung injury with haemorrhage, contusion, or ipsilateral pleural effusion. With penetration of one or more ribs through the pleura, pneumothorax or tension pneumothorax may occur. Clinical observation of breathing is important because respiratory movement may be limited by pain or, in the case of multiple rib fractures, an unstable thorax develops.
Vertebral Fractures.
Radiologically, there is loss of height of vertebral bodies, such depressed fractures are best seen in the lateral chest radiograph. Complementary CT must be performed to assess the stability of the posterior vertebral column. The possibility of underlying aetiology for vertebral fractures should be kept in mind (such as osteoporosis, metastases, etc.).
Clavicle/Acromio-Clavicular Joint.
Such fractures are best seen in the posteroanterior chest X-ray. Dislocation of the clavicle may lead to thoracic haemorrhage or pneumothorax.
15 Pulmonary Contusion
15 Definition
Lung contusion is a diffuse haemorrhage caused by traumatic crushing of the lung parenchyma.
15 Diagnosis
On CT, contusion appears as patchy, homogeneous opacities in the lung parenchyma, without air bronchogram, mostly subpleural situated. The opacities do not respect segmental boundaries, and are partially confluent. The radiograph shows diffuse shadowing. The opacities tend to clear after a few days.
15 Injuries of the Bronchial System
15 Pathogenesis and Clinical Presentation
Injury of the tracheobronchial system can be caused by penetrating trauma, a sudden increase in intrathoracic pressure or high-velocity trauma.
Clinically, there are breathing difficulties with dyspnea, cough, or wheezes. Since bronchial injuries are usually observed only in severely injured patients, other clinical signs are usually present.
15 Diagnosis
Direct visualisation of bronchial injury is unusual (80% of injuries are close to the carina). Complete bronchial tear may be seen as discontinuity of the bronchus and caudal displacement of the bronchus in an erect radiograph.
Indirect signs are:
-
Pneumomediastinum or pneumopericardium
-
Pneumothorax
-
Atelectasis
15 Pneumomediastinum
15 Definition and Pathogenesis
Pneumomediastinum is pathologic accumulation of air in the mediastinum due to variable causes (Figs. 19.105 and 19.106). Air enters the mediastinum from perforated alveoli, or from esophageal or tracheobronchial injuries into the mediastinum.

Pneumomediastinum. Chest X-ray posteroanterior view shows linear air-densities in the mediastinum (arrows) and subcutaneous emphysema on the right

Pneumopericardium. Lateral chest radiograph shows pneumopericardium (arrows)
Possible causes include:
-
Trauma (bronchial rupture, penetrating trauma)
-
Iatrogenic (mechanical ventilation, tracheostomy, esophageal dilatation)
-
Inflammatory (mediastinitis, retroperitoneal inflammation, pneumonia)
-
As a complication of tumours
-
Boerhaave syndrome
15 Clinical Presentation
Clinically, it can be difficult to diagnose pure pneumomediastinum. More often, it is a secondary finding in the chest radiograph or CT.
15 Imaging
Thoracic/CT:
-
Thread-like air streaks that outlines mediastinal structures
-
Heart borders are more clear
-
May extend into the neck
15 Injuries of the Aorta
15 Pathogenesis
Aortic injuries are caused by high-speed trauma or penetrating injuries. A common site of injury is the aortic isthmus near the ligamentum arteriosum. Aortic injury can lead to aortic rupture, aortic dissection, or aneurysm formation.
15 Clinical Presentation
The symptoms include chest pain, dyspnea, blood pressure difference between the two arms, and blood pressure instability.
15 Diagnosis
The chest X-ray shows nonspecific signs:
-
Widened upper mediastinum
-
Tracheal shift
-
Enlarged or obscured aortic knob
-
Displacement of the aorto-pulmonary window
CT is the method of choice for diagnosis of aortic injuries:
-
A concealed rupture appears as thin rim of peri-aortic fluid
-
Pseudoaneurysm formation
-
A dissection flap appears as a fine intraluminal line that courses longitudinally, parallel to the aortic wall
Transesophageal echocardiography may be performed as an alternative for diagnosis or with equivocal CT findings.
15 Diaphragmatic Rupture
Diaphragmatic rupture is occasionally seen following trauma. It is sometimes accompanied by other serious injuries such as splenic or liver parenchymal injuries.
15 Clinical Presentation
The presentation depends on the extent of the injury. Small tears may be asymptomatic and are incidentally detected on imaging.
15 Imaging
On chest X-ray, there are only indirect signs:
-
Elevated diaphragm and blurring of the diaphragmatic contour on the affected side
-
Intrathoracic fluid levels or atypical cavities due to herniation of abdominal organs
-
Mediastinal shift
In addition, with unclear results, a barium swallow investigation under fluoroscopy could be used. Small ruptures can be diagnosed by CT.
15 Hernias (also not Traumatic)
Herniation of abdominal contents into the thorax may be due to congenital defect in the muscle, traumatic diaphragmatic tears, or through acquired weakness in the esophageal hiatus.
15 Hiatus Hernias (Figs. 19.107 and 19.108)

Hiatus hernia. Chest X-ray posteroanterior view shows a large lucency in the lower mediastinum with intralesional air-fluid level (arrows)

Large hiatus hernia. Lateral chest radiograph showing the herniated stomach (arrowheads) with air-fluid level inside (arrows)
Axial Sliding Hernia
Axial sliding hernia occurs due to an insufficiency of the phrenico-esophageal membrane and an increase in intra-abdominal pressure, so that a portion of the stomach prolapses into the thorax. Hiatus hernias may predispose to esophageal reflux. In many cases, hiatus hernias are asymptomatic.
X-ray:
-
Rounded mass with smooth borders and with fluid levels
-
In the posteroanterior view, it is seen projected behind the heart shadow
-
In the lateral view, it is seen in the retrocardiac space
Barium swallow:
-
Intrathoracic stagnation of the contrast agent
-
Formation of air-fluid levels
Para-Esophageal Hernia
In para-esophageal hernia, portions of the stomach, particularly the cardia, are prolapsed into the thorax beside the oesophagus through the diaphragmatic hiatus (Fig. 19.109). Most are due to congenital defects of the phrenico-esophageal membrane. A para-esophageal hernia often causes postprandial abdominal discomfort. Incarceration of the herniated stomach may occur as a severe complication. Large para-esophageal hernias, where the whole stomach is herniated through the widened hiatus into the thoracic cavity, may be complicated by gastric volvulus producing an “upside-down stomach.”

Para-esophageal hernia. a Axial CT in soft tissue window shows a mass in the lower mediastinum with central lumen (arrows). b CT in lung window
15 Congenital Diaphragmatic Hernia
Bochdalek hernias occur when intra-abdominal organs such as omental fat, abdominal organs, or parts of the intestine herniate through the lumbo-costal triangle. Morgagni hernias occur when the same structures herniate through the sterno-costal triangle.
16 The Mediastinum
The mediastinum contains the heart, the great vessels, the oesophagus, thyroid and nervous structures, all of which may be affected by pathologic changes.
Mediastinal shift may occur due to tension pneumothorax or unilateral phrenic nerve palsy. A fixed shift of the mediastinum can be seen with scoliosis, pneumonectomy, atelectasis, pleural operations, or mass lesions such as pleural effusion or tumours.
16.1 Mediastinal Inflammations
16.1 Pathogenesis
Mediastinal inflammations lead to nonspecific widening of the mediastinal shadow on chest radiography. Inflammations may be acute or chronic. Acute inflammations are often caused by esophageal rupture or iatrogenic after sternotomy or endoscopy.
Mediastinal inflammations are often severe with a high mortality rate, up to 50%.
16.1 Clinical Presentation
Patients with acute mediastinitis present with severe retrosternal pain radiating to the neck, dyspnea, dysphagia, and soft tissue emphysema. In addition, signs of sepsis such as high fever, tachycardia, and tachypnea can develop.
Chronic mediastinal inflammations may be caused by different chronic granulomatous diseases which lead to fibrosis of the mediastinum. Such granulomatous diseases include sarcoidosis or tuberculosis. Primary mediastinal Ormond’s disease is rare. The presentation is usually nonspecific. Only with extensive fibrosis, symptoms occur due to narrowing of the organs in the mediastinum with upper vein stasis, swallowing, and breathing difficulties.
16.1 Imaging
On the chest X-ray or CT, there is widening of the mediastinum with irregular contours, and possibly with pneumomediastinum. On CT, there is obliteration of the mediastinal fat by a diffuse inflammatory reaction. There is often compression of the superior vena cava up to complete occlusion. Fluid collections with marginal contrast enhancement and air-fluid levels indicate the development of mediastinal abscess. Chronic mediastinitis should be differentiated from malignant neoplasms. In selected cases, CT-guided biopsy may be performed to confirm the diagnosis.
16.1 Treatment
Acute mediastinitis is treated by broad spectrum antibiotics or surgical drainage as well as treatment of the cause of the mediastinitis. The treatment of chronic mediastinitis is dependent on the underlying disease. An identifiable focus of infection should be eliminated and specific antibiotics administered.
16.2 Anterior Mediastinal Masses
Lesions in the mediastinum are shown in Figs. 19.110–19.115 .

Mass in the superior mediastinum. Chest X-ray posteroanterior view shows a large homogeneous upper mediastinal mass with smooth margins (arrows)

Mass in the anterior superior mediastinum (arrows). Lateral chest radiograph

Mediastinal mass. Axial CT image in soft tissue window shows a mass originating from the thyroid gland with central calcifications; retrosternal goiter

Goiter. Chest X-ray posteroanterior view shows a calcified mass with tracheal shift (arrows)

Mass in the upper mediastinum. Chest X-ray posteroanterior

Thymic tumour. Axial CT in soft tissue window shows an extensive, diffuse infiltration in the anterior mediastinum with displacement of vessels: malignant lymphoma
16.2 Thyroid Masses
16.2 Definition and Pathogenesis
Enlargement of the thyroid gland, which can extend to the superior anterior mediastinum, may have different etiologies (. Figs. 19.112 and 19.113 ). Most cases are due to multinodular goiter, or less commonly thyroid neoplasms. Thyroid masses usually cause deviation and deformation of the trachea.
16.2 Diagnosis
Chest X-ray
The chest radiograph shows nonspecific widening of the mediastinal shadow, with possible displacement of the trachea.
CT:
-
Smooth, well-defined contrast-enhancing mass
-
Rounded, hypodense areas in the presence of adenomas
-
Calcifications are possible
16.2 Parathyroid Tumours
Parathyroid tumours usually present with clinical symptoms of hyperparathyroidism. Normally, the parathyroid glands are located posterior to the thyroid gland, but ectopic location down to the aortic arch is possible. The glands are often only very small structures; with less contrast-enhancement on CT than that of the adjacent thyroid tissue. Sonography is also commonly used for diagnosis of parathyroid lesions.
Tumours of the Anterior Mediastinum
-
Thyroid tumours (goiter, carcinoma)
-
Thymus-associated tumours (thymoma, thymic carcinoma, hyperplasia)
-
Teratoma, cysts (e.g., dermoid/epidermoid)
-
Mesenchymal tumours
16.2 Thymus-Associated Masses
Chest X-ray shows indirect signs such as widening of the upper mediastinum or narrowing of the retrosternal space. CT shows a wedge-shaped, soft tissue density mass in the anterior, superior mediastinum, adjacent to the aortic arch.
Causes of thymus-associated masses include (Fig. 19.115):
-
Thymic hyperplasia after severe systemic disease
-
Follicular hyperplasia associated, in two thirds of cases, with myasthenia gravis
-
Thymoma:
-
Usually solid, well-defined, lobulated mass in the anterior superior mediastinum
-
Calcifications and local infiltrative growth are possible
-
On MRI, thymic tumours are hyperintense on T2-weighted sequences
-
On T1-weighted sequences, they are isointense to muscles
-
Specific diagnosis is done by biopsy
-
-
Thymus cysts:
-
May be congenital or acquired
-
Acquired cysts can grow up to 10 cm in diameter
-
Attention must be paid when diagnosing thymic cysts because germ cell tumours (seminomas) may contain cysts
-
-
Infiltration of the thymus may occur with Hodgkin’s disease, non-Hodgkin’s lymphoma, and leukemia
-
Other tumours: Thymolipoma, carcinoid
16.2 Germ Cell Tumours
These tumours present variable imaging pictures, mostly well-defined and smoothly marginated. The clinical course is also variable; some are asymptomatic, and others present with early local compression symptoms or with secondary infection.
16.3 Middle Mediastinal Masses
16.3 Vascular Variants and Lesions
-
Aortic aneurysms:
-
Dilatation of the ascending aorta may be caused by degenerative or inflammatory processes, trauma, or congenital defect (e.g., Marfan syndrome)
-
Dilatation of the ascending aorta > 4 cm is considered pathologic
-
Suspicious findings on chest X-ray with displaced mediastinal lines warrant confirmation of diagnosis by CT or echo-cardiography
-
On CT, aneurysmal dilatation could be accurately diagnosed and quantified, in addition; dissection and mural thrombus could be detected
-
ECG-triggered CT is indicated for the specific evaluation of the ascending aorta
-
-
Aberrant right subclavian artery:
-
Congenital variant involving the origin and course of the right subclavian artery
-
The artery originates directly from the descending aorta and crosses to the right side behind the oesophagus
-
May cause dysphagia (dysphagia lusoria)
-
-
Aortic arch variants:
-
Numerous variants are reported
-
Commonly associated with other cardiac congenital anomalies, such as Fallot’s tetralogy, pulmonary atresia
-
A right aortic arch is characterised on X-ray by a right-sided aortic knob instead of the usual left-sided one. The trachea may be slightly shifted to the left
-
Double aortic arch
-
High position of the aortic arch
-
-
Left superior vena cava
16.3 Bronchogenic Cysts
See Sect. 19.5.2
16.3 Pericardial Cysts
A pericardial cyst is a thin-walled, fluid-filled cyst with no connection to the pericardial cavity. It is most commonly located in the cardio-phrenic angle and has no clinical significance.
16.3 Chest X-Ray and CT
Radiographically, a pericardial cyst appears as a well-circumscribed, rounded structure in contact with the heart, rarely with calcifications. On CT, it appears as a well-circumscribed, rounded structure, with fluid density.
MRI:
-
The signal intensity can vary depending on the contents of the cyst
-
T2-weighted sequence: high signal intensity
-
T1-weighted sequence: variable signal intensity depending on the protein content, marginal enhancement after contrast administration
-
Proton-density weighted sequence: intermediate signal intensity, lower than that on the T1-weighted sequence
Tumours of the Middle Mediastinum
-
Lymphoma
-
Tumours originating from the oesophagus (e.g., leiomyoma),
-
Neuromas (phrenic nerve, the vagus nerve)
-
Thyroid tumours
16.3 Lymph Node Enlargement
Mediastinal lymph node enlargement may be caused by neoplasms such as Hodgkin’s disease, non-Hodgkin lymphoma, leukemia, and metastasis; or granulomatous diseases such as sarcoidosis, amyloidosis, and Wegener’s disease, or reactive due to infectious diseases such as tuberculosis, fungal infections, viral and mycoplasma pneumonias.
16.3 Chest X-ray
The picture on chest X-ray is dependent on the location of the enlarged lymph nodes:
-
Widening of the right paratracheal stripe with enlarged right paratracheal lymph nodes
-
Displacement of the azygous shadow laterally with enlarged azygous lymph nodes
-
Convex opacity in the aorto-pulmonary window or total opacity of the aorto-pulmonary window in the lateral view
-
Widened mediastinum
-
Infra-carinal opacity with displaced azygo-esophageal line
-
Lobulated hilar enlargement
CT:
Lymph nodes on CT with short-axis diameter of 10 mm or more are considered pathologic. They present as hypodense, mostly well-defined nodular structures. Sometimes, the lymph nodes become confluent, and appear as a bulky mass, where individual nodes cannot be distinguished from each other. Central necrosis with fluid density areas without significant contrast enhancement is possible and may be observed with fungal infections, tuberculosis, and lymphoma. Marked enhancement is seen in well-perfused metastases, from lung carcinoma or renal cell carcinoma, and in Castleman’s disease.
It is important to describe accurately the location and size as well as the presence of calcifications in the lymph nodes. With unclear findings and/or an unknown primary tumour, CT-guided biopsy may be indicated.
MRI:
-
T1-weighted sequence: low signal intensity, similar to muscle tissue
-
Contrast-enhanced T1-weighted sequence: high signal intensity due to contrast enhancement simulates fat signal, therefore fat suppression is recommended
-
T2-weighted sequence: high signal intensity
16.3 Tracheal Tumours
16.3 Pathogenesis
Primary tumours of the trachea are rare. Secondary invasion of the trachea from tumours of adjacent organs is more common (e.g., bronchi, larynx).
Benign tracheal tumours include pleomorphic adenomas, papillomas, hamartomas, and chondromas. Malignant tumours of the trachea are most commonly squamous cell carcinoma, followed by adenoid cystic carcinoma.
16.3 Clinical Presentation
The course is usually slowly progressive; symptoms start only with narrowing of the lumen by about two thirds, and then include dyspnea, cough, wheezes, and bloody sputum. These symptoms are often misdiagnosed as asthma or bronchitis.
16.3 Chest X-Ray
Chest radiography rarely shows direct signs of tracheal tumours. Sometimes deformity of the tracheal contour is seen.
CT:
-
Intraluminal mass
-
Benign tumours appear as smoothly bordered lesions, usually limited by the tracheal cartilage
-
Hamartomas are characterised by the presence of intralesional fat
-
Malignant lesions are characterised by infiltration of the surrounding tissue
-
Virtual bronchoscopy is helpful for evaluation of the extent and for preoperative planning
16.4 Posterior Mediastinal Masses
16.4 Neurogenic Tumours
16.4 Definition
Neurogenic tumours are tumours that arise from nerve cells and nerve sheath tissue. The most common tumours include schwannomas, neurofibromas, neuroblastomas, paragangliomas, and ganglioneuromas.
16.4 Clinical Presentation
Patients are often asymptomatic; symptoms include radicular pain. Growth into the spinal canal leads to spinal cord compression symptoms.
16.4 Imaging
Chest X-ray reveals a well-circumscribed, homogeneous opacity, paravertebral in location. Adjacent sclerosis is an indication of a benign process, while rib destruction is suspicious of a malignant tumour.
On CT, benign tumours appear as soft tissue density masses with smooth borders located in the posterior mediastinum. Malignant tumours are characterised by heterogeneous density, irregular borders, infiltrative growth pattern, and intense enhancement with increased vascularity. The relation to the spinal canal must be demonstrated, and a complementary MRI may be necessary if intraspinal extension is suspected.
On MRI, there is better differentiation between the tumour and surrounding muscle tissues due to difference in signal intensity on both T1- and T2-weighted images. Enhancement after gadolinium administration depends on the composition of the tumour and the degree of vascularisation.
16.4 Extramedullary Haematopoiesis
Extramedullary haematopoiesis occurs in patients with sickle cell anemia, thalassemia, or other severe anemias. Extramedullary haematopoiesis presents as asymptomatic, elongated masses, paraspinal in location and bilateral. Only large masses are detectable on conventional radiography.
In most cases, extramedullary haematopoiesis can only be seen by CT. They appear as well-circumscribed, soft tissue density masses, with smooth borders and with significant contrast enhancement.
On MRI, extramedullary haematopoietic tissue has higher signal intensity than the surrounding muscles on T2-weighted images. There is significant enhancement after gadolinium administration on T1-weighted images.
Tumours of the Posterior Mediastinum
-
Schwannomas
-
Neuroblastomas
-
Pheochromocytomas
-
Tumours originating from the oesophagus
16.4 Oesophagus
Achalasia, esophageal tumours (Fig. 19.116), esophageal diverticula, or hernia are possible causes of posterior mediastinal masses.

Leiomyoma of the oesophagus. a Contrast swallow examination shows spindle-shaped compression of the oesophagus with narrowing of the lumen. b Contrast-enhanced MRI shows the soft tissue tumour (arrows)
16.4 Achalasia
Chest X-ray shows a nonspecific appearance of the enlarged, air-filled oesophagus. For further investigation, a barium swallow can be performed.
16.4 Esophageal Tumours
Esophageal tumours are normally not visible in plain radiographs. Barium swallow is the imaging modality of choice. They are uncommonly shown by CT as circumscribed esophageal wall thickening.
16.4 Diverticula
The Zenker diverticulum is a Pulsions diverticulum with protrusion of mucosa and submucosa through a left-sided muscle gap above the M. cricopharyngeus. Clinically, there is difficulty in swallowing, regurgitation of food residues, and pain in ulcerations. Chest X-ray occasionally shows a shadow with fluid level, the barium swallow is indicated for definitive diagnosis.
The epiphrenic diverticulum is a pulsations diverticulum, located about 10 cm above the cardia in the distal oesophagus. Diagnosis is made by barium swallow whereby small diverticulum may mimic ulcerations.
Causes of mediastinal calcifications
-
Goiter, thyroid cysts
-
Teratoma
-
Thymoma
-
Calcified tracheal rings
-
Pericardial calcifications
-
Calcified cardiac valves
-
Atherosclerosis (coronary arteries, aortic arch)
17 Pleura and Chest Wall
17.1 Pleura
17.1 Pleural Effusion
17.1 Pathogenesis
Pleural effusion is accumulation of fluid in the pleural cavity due to various etiologies (Fig. 19.117). Possible causes include:

Limits of detection of pleural effusion
-
Transudate (Table 19.37):
Table 19.37 Differentiation transudate vs. exudate -
Heart failure
-
Hypoproteinemia (nephrotic syndrome)
-
Hepatic cirrhosis
-
-
Exudate:
-
Infections (tuberculosis, viruses, Parapneumonic)
-
Malignancies (lung cancer, metastases, Hodgkin’s disease, mesothelioma)
-
Pulmonary embolism
-
Autoimmune diseases
-
Pancreatitis
-
-
Haemothorax/chylothorax:
-
Iatrogenic: after biopsy, surgery
-
Traumatic
-
Malignancies
-
17.1 Clinical Presentation
A larger effusion can lead to dyspnea. Percussion reveals dullness that increases laterally (Ellis-Damoiseau line) and decreased tactile fremitus. On auscultation, there are diminished breath sounds over the effusion.
17.1 Imaging
Free pleural effusion collects in the most dependent region of the thoracic cavity. In the standing position, fluid collects in the costo-phrenic recess. Smaller effusions can be diagnosed in the lateral radiograph first, because the fluid collects in the more dependent posterior aspect. Fluid becomes visible on lateral X-ray from an amount of about 150 ml. There is first blunting of the costo-phrenic angle, with a visible level, that rises laterally with increased amount of fluid. Loculated effusions may accumulate in interlobar fissures to appear as spindle-shaped opacities or sometimes simulate nodules. It is possible to identify effusions of only a few milliliters using decubitus views with a horizontal beam. Sonography can detect effusions from 50 ml.
Supine radiographs for patients in intensive care units often show effusions of only about 500 ml or more. The fluid accumulates posteriorly, and is demonstrated as shadowing of the basal lung zones with poor definition of the diaphragm and cardiac borders. Complementary sonography may be performed for suspected cases.
In the presence of haemorrhagic pleural effusion, malignancy should be suspected.
17.1 Treatment
The cause of effusion should be treated first, for example left-sided heart failure. Aspiration or tube drainage (ultrasound or CT-guided) may be performed for recurrent effusions.
Special forms of pleural effusion
-
Loculated effusion: fluid accumulates between visceral pleural layers in the interlobar fissures and appears as spindle-shaped mass, sharply demarcated against lung tissue. Loculated effusions may change with a change in the patient’s position. CT or sonography can differentiate loculated fluid from solid masses.
-
Subpulmonary effusion: fluid accumulates between the lung base and the diaphragm, and does not rise laterally as usual. The appearance simulates an elevated diaphragm on chest X-ray. An indirect sign for differentiation is the large distance between the gastric bubble and the diaphragm.
-
Lamellar effusion: shallow collections of fluid between the lung surface and visceral pleura.
17.1 Broncho-Pleural Fistula
Bronchopleural fistula is defined as communication between the pleura and the bronchial system. It can be iatrogenic; following partial or complete lung resection, post-traumatic, postinfection, or due to ruptured large bullae.
Clinically, it presents with persistent pneumothorax or hydro-pneumothorax and sometimes soft tissue emphysema after drainage insertion. High-resolution CT is the modality of choice, although it is not always possible to localise the defect.
17.1 Pleuritis
Pleuritis is an acute or chronic inflammation of the pleura, usually in combination with other pulmonary processes such as pneumonia, bronchitis, tuberculosis, and tumours. Several forms could occur. In case of serous pleuritis, exudate is secreted into the pleural cavity. Dry pleuritis is characterised by fibrin deposits. Other forms include purulent, tuberculous, and haemorrhagic forms.
17.1 Clinical Presentation and Diagnosis
Patients present with breath-related, unilateral chest pain. There is a friction rub with in- and expiration. Chest X-ray shows an elevated diaphragm on the affected side and a small pleural effusion.
17.1 Treatment
Important is the treatment of the underlying disease. Symptomatic treatment is with paracetamol.
17.1 Malignant Mesothelioma
17.1 Definition and Pathogenesis
Malignant pleural mesothelioma is a tumour that originates from the pleura, and has a strong relation to prolonged exposure to asbestos. Men > 50 years are mostly affected. Only a small proportion of people exposed to asbestosis will develop malignant mesothelioma. The prognosis is poor with a median survival time of 12 months.
17.1 Clinical Presentation
The presentation is nonspecific with shortness of breath, pain, and cough, and the disease is often first diagnosed in an advanced stage, which worsens the prognosis.
17.1 Imaging
Chest X-ray:
-
Pleural effusion
-
Localised nodular opacities of the pleura
-
Mediastinal shift towards the affected side due to volume reduction is possible
-
In advanced stages: rib destruction, mediastinal lymph nodes
CT:
-
The tumour extension is better shown
-
Pleural mass infiltrating the lung, chest wall, or the diaphragm
-
Complete infiltration of the pleura, visible as diffuse pleural thickening is possible
-
Enlarged lymph nodes (parasternal)
When mesothelioma is suspected, CT-guided percutaneous biopsy or thoracoscopy should be performed for final diagnosis.
Tumour staging is presented in Table 19.38.
17.1 Treatment
Early tumours could be treated by surgical resection, pleuro-pneumonectomy, after adjunctive chemotherapy. In advanced stages, only chemotherapy is possible.
17.1 Benign Pleural Tumours
Benign mesotheliomas originate from the visceral pleura. Tumours composed of fibrous tissue are termed pleural fibroma. Solitary lesions are treated surgically and recurrences are rare. Pleural lipomas are uncommon tumours; they can be easily diagnosed by CT because of the density values.
17.1 Empyema
17.1 Pathogenesis
Empyema is an infected pleural effusion, which often occurs in association with bacterial pneumonia. Other causes include sepsis, lung abscess, broncho-pleural fistula, iatrogenic, neoplastic or post-traumatic processes. The course passes through three stages; an exudative phase, a purulent phase, and then fibrosis.
17.1 Clinical Presentation
Symptoms and signs of pleural empyema may be masked by the underlying disease. There is usually, however, fever, local chest pain, cough, and night sweats.
17.1 Imaging
Chest X-ray is generally insensitive for possible infection of a pleural effusion. The radiographic opacity of pleural effusion shows only the approximate amount of effusion.
On CT, the aetiology could be delineated. Other signs include thickened pleura and significant enhancement of the pleura after contrast administration. Furthermore, tube drainage could be inserted guided by CT.
17.1 Treatment
When the empyema is not yet organised, it can be percutaneously drained. Otherwise, surgical intervention is necessary. Fibrinolysin could be injected. Lastly, empyema could be evacuated thoracoscopically.
17.2 Chest Wall
17.2 Subcutaneous Emphysema
17.2 Definition and Pathogenesis
Subcutaneous or soft tissue emphysema is accumulation of air from the lungs or pleural cavity in the surrounding soft tissue, such as muscles and fat. This may occur in association with pneumothorax, mechanical ventilation, or malposition of drainage.
17.2 Clinical Presentation
Clinically it is felt as crepitus and may cause soft tissue swelling and skin stretching.
17.2 Diagnosis
Chest X-ray shows fine, delicate radiolucent lines over the soft tissue of the chest wall and neck, with a feathery appearance. Air may outline the fibers of the pectoral muscles. Sometimes the presence of underlying pneumothorax is masked by the subcutaneous emphysema on X-ray. CT shows air density in between the facial planes of the subcutaneous tissue. The extent of the process is best evaluated with lung window CT images (. Fig. 19.118 ).

Soft tissue emphysema. a Chest X-ray supine view. b CT in lung window shows extensive air in the skin and soft tissues
17.2 Tumours
The most common chest wall tumours include:
-
Tumours originating from ribs or cartilage (see Chap. 36)
-
Soft tissue tumours
-
Primary neoplasms: lipoma, haemangioma, lymphangioma, fibroma, melanoma
-
Secondary malignancies: lung cancer, mesothelioma, metastases
17.2 Other Diseases
17.2 Tietze Syndrome
Is defined as nonsuppurative pain and tenderness of the costal cartilages or the sterno-costal junctions, of unknown aetiology. The chest X-ray is usually normal. On MRI, there is occasionally thickening of cartilage with abnormal signal intensity and increased contrast-enhancement.
17.2 Chest Wall Calcifications
Generally, calcifications are not uncommon on chest X-ray and can have numerous causes. Calcifications within the soft tissue must be differentiated from those only projected on the chest wall. A subcutaneous haematoma or granuloma may appear as a rounded, finely calcified structure (Fig. 19.119). Soft tissue sarcomas or osteosarcomas often show calcifications. Calcified lymph nodes may be seen in the axilla or intrathoracic in the hilar regions or aorto-pulmonary window. The costochondral junctions are often partially or totally calcified in old age. Intrapulmonary calcified foci are often seen with tuberculosis or histoplasmosis, as postinflammatory granulomas. Varicella pneumonia can leave multiple, small, punctate calcifications. Calcified pulmonary metastases from osteosarcomas, mucinous adenocarcinomas, and papillary thyroid carcinomas are also possible.

Suspected pulmonary granuloma. a Chest X-ray posteroanterior view shows a nodule in the left lower lung zone with high density. b Lateral chest radiograph shows rounded calcification projected over the heart shadow. c Axial CT in the lung window shows calcification in a left ventricular aneurysm
Pleural calcification may occur after empyema or haemothorax. Exposure to asbestos leads to large linear and irregular plaque-like pleural calcifications.
18 Lung Interventions
18.1 Regional Chemotherapy of the Lung
The techniques of regional chemotherapy of the lung can be divided into Transpulmonary chemoembolisation (TPCE) and Transbronchial chemoembolisation.
18.1 Transpulmonary Chemoembolisation (TPCE)
The incidence of bronchial carcinoma has increased rapidly in the last decades. It is nowadays the commonest malignancy worldwide. Lung cancer is the commonest malignant disease in the USA, both in men and women. The average age of incidence is between 65 and 75 years. The commonest pathologic type is squamous cell (34%), followed by large-cell carcinoma (28%) and then adeno-carcinoma and bronchioalveolar (20%), small cell carcinoma (17%), and mixed pathologic types (1%). TPCE is a new alternative treatment for unresectable lung cancer.
18.1 Principle of TPCE
The principle of TPCE is catheter insertion in the pulmonary artery to gain access for arterial inflow to the tumour. High-dose cytostatic drug can be injected directly into the involved lung region; and systemic side effects can be greatly reduced.
18.1 Technique of TPCE
Transvenous cannulation of the pulmonary artery by a 5-F Headhunter catheter and angiography of the pulmonary arterial system is performed. The tumour-supplying segmental artery is catheterised using the Headhunter catheter. Afterwards, a balloon catheter (diameter 7 mm, length 110 mm) is placed in the selected segmental artery. Depending on the size, the location, and the supplied area of the artery, the catheter tip is advanced into the pulmonary artery over a guidewire. The catheter is blocked to cancel out arterio-venous shunts. Afterwards, cytostatics and up to 10 ml of Lipiodol and microspheres are slowly injected under fluoroscopic guidance until stasis of blood flow.
18.1 Results
TPCE may be performed to improve the prognosis of non-small cell lung cancer in stages II and III, as neoadjuvant treatment, combined chemo-radiotherapy, and postoperative. For advanced stages, TCPE may be performed as palliative treatment.
Palliative TPCE is helpful to control refractory local manifestations of lung cancer and lung metastases, particularly for colorectal and breast cancer and other hypervascular metastases of different primary tumours. TCPE can be combined with other interventional therapies such as thermal ablation or laser-induced thermotherapy and the results are very promising.
Two important factors influence the results of TPCE:
-
First, balloon catheter vessel occlusion is necessary in order to prevent spread of embolisation material and avoid the potential complications due to venous contamination through arterio-venous shunts.
-
Second, the super-selective application of chemotherapy, the use of Lipiodol, which acts as a vehicle for cytotoxic drugs and the use of microspheres to delay the elimination of cytostatic drugs.
18.1 Bronchial Artery Embolisation
Bronchial artery embolisation is an established treatment for haemoptysis, because of its high early success rate. Several studies support the use of bronchial artery embolisation in cystic fibrosis patients with acute and chronic haemoptysis.
18.1 Technique
The procedure is usually performed via a femoral access. Selective angiography of the intercostal and bronchial arteries is first performed to identify the source of bleeding. Information from previous bronchoscopy or CT is valuable for rapid localisation of the site of bleeding. The location, size, number, and morphology of the bleeding arteries must be documented during angiography.
On selective bronchial arteriography, the direct sign of bleeding is extravasation of contrast medium. Indirect signs of bleeding include local hypervascularity, arterial hypertrophy, and pulmonary arterio-venous shunts. Haemoptysis with a bleeding rate of > 30 ml/hour should be angiographically positive.
The second step is embolisation using various embolic agents. Some authorities advise performing a complete angiography of the thoracic vascular anatomy including thoracic aortography and selective arteriography of the subclavian artery after embolisation of bronchial arteries.
18.1 Results
The aetiology of haemoptysis and the morphologic changes of the bleeding vessels show great heterogeneity. Published results reported up to 90% success in treating nontumoural haemoptysis. However, recurrence is also commonly seen, especially in the presence of neoplasms because of neovascularisation with weak immature vascular walls and effects of tumour invasion.
Embolisation may be performed with platinum coils. Coils occlude relatively proximal to the source of bleeding, and therefore some authorities are against the use of coils because they prevent re-embolisation of distal sources of bleeding.
18.1 Complications
Several complications were reported including severe chest pain, dysphagia, bronchial necrosis, diaphragmatic paralysis, and spinal ischemia associated with paraplegia. Recent studies show that using nonionic contrast media and the modern DSA system dramatically decreased the complication rates in the hands of an experienced interventionist.
Guidelines for pulmonary/bronchial embolisation (German Society of Radiology)
-
Bronchial artery embolisation:
-
Emergency embolisation for life-threatening haemoptysis if surgical intervention is contraindicated. Curative in cases of vascular malformations. Otherwise, usually palliative because the underlying cause is not treated.
-
Highly indicated for severe haemoptysis (200–500 ml/day).
-
May be performed for haemoptysis associated with tuberculosis, bronchiectasis, cystic fibrosis, lung abscess, pneumoconiosis, aspergilloma, bronchial carcinoma, vascular malformations.
-
Before bronchial arteriography, a local bleeding vessel, that could be endoscopically treated, should be ruled out.
-
-
Pulmonary artery embolisation:
-
Solitary and multiple arterio-venous fistula, > 3 mm, even in asymptomatic patients, due to the risk of paradoxic cerebral emboli.
-
Congenital vascular malformations, commonest with hereditary telangiectasia.
-
Pre-operative embolisation.
-
18.2 Thermal Ablation
18.2 Radiofrequency Ablation (RFA)
Radiofrequency ablation (RFA) is a thermoablative procedure. RFA has gained high acceptance for treatment of liver tumours due to its minimally invasive nature, the low treatment-related morbidity, and the high local efficacy. RFA is currently an alternative therapeutic option in the treatment of lung and kidney tumours and in the symptomatic treatment of bone and soft tissue tumours.
18.2 Principles of RFA
Ablation of tumours by RF is based on increasing the local temperature focused on the solid tumour portions to induce irreversible cellular injury by coagulation necrosis. However, ablative energy also leads to tissue dehydration and water vaporisation, which in turn cause an increase in tissue impedance up to inhibition of further current flow.
18.2 Indications for RFA
The current indications for RFA of lung tumours include:
-
Patients with early-stage primary lung cancer (non-small cell) without lymph node metastasis, who are not candidates for surgery as a result of medical comorbidity.
-
Patients with potentially curable pulmonary metastases who are not candidates for surgical resection of metastases
-
As part of palliative care in patients with primary or metastatic lung tumours, for example for relief of intractable pain
18.2 RFA Technique
The RF needle electrode is placed in the tumour under (CT) imaging guidance, and one or more grounding electrodes are applied on the skin surface (typically on the thighs). The system is connected to the RF generator which generates an alternating current flow between the electrodes. This causes oscillation of ions in the ablation field and thus heating of the tissue by means of friction. This effect increases with increasing the applied energy. The highest energy disposition is in the immediate surroundings of the needle electrode, with increasing distance; depending on the needle electrode, the energy is no longer sufficient to induce tissue damage.
18.2 Mechanism of RFA
A cytotoxic effect has been demonstrated at temperatures of > 42°C. Death of malignant cells is achieved after 8 min at 46°C, 2 min at 51°C, and at 70°C there is immediate cellular death. The exact mechanism of temperature-induced cellular damage is not fully understood. Immediate cellular damage is based on protein-coagulation of cytosolic and mitochondrial enzymes. Besides direct cytotoxic effects in this phase, other intracellular processes are also induced, for example “heat-shock proteins,” which refers to antigen presentation on the cell surface after ablation, and possibly play a role in activation of the immune response. Temperatures above 60°C lead to coagulation necrosis, and temperatures of about 90–100°C lead to tissue charring and carbonisation.
The ablated volume depends on both heat conduction by local RF energy applied and heat convection from the circulating blood. In the lung, RF energy is efficiently deposited because the high blood flow has a heat sink effect and the surrounding air has an insulating effect.
18.2 Results
The criteria for evaluating the success of ablation are currently not standardised. Early detection of residual tumour tissue is critical for the prognosis and allows early interference with re-ablation. For this reason, optimisation of the postablation evaluation is desirable. Contrast-enhanced CT and MRI are currently the modalities of choice. Criteria for successful ablation include size changes, but this may be insensitive in the first three months after ablation because many tumours will show an initial increase in size due to surrounding tissue reaction. Another approach depends on attenuation measurements in contrast-enhanced CT. Functional imaging with FDG PET and PET CT in the early phase after RF ablation has higher sensitivity and specificity in the assessment of ablation results.
18.2 Lung Metastases
Percutaneous RF ablation could be a possible alternative to surgical resection of potentially curable metastases. Indications are similar to surgical metastasectomy, complete eradication of the primary tumour and either absent or treatable extrapulmonary metastases. In addition, a complete RF ablation of all metastases is judged as technically possible.
Palliative Indications of RFA in Lung Tumours.
RF ablation may be used for treatment of intractable tumour-associated pain in the lung and chest wall.
18.2 Complications
The possible post-ablation complications include pain and mild fever, but they require only symptomatic treatment. Occasionally, pleural effusion is seen after ablation of tumours near the pleura. Minimal haemoptysis may occur, but massive haemoptysis requiring treatment is uncommon. Pneumothorax is a common complication, but is usually limited and only in a small percentage is chest tube insertion necessary.
18.3 Laser-Induced Thermotherapy of the Lung
For percutaneous laser ablation, miniaturised applicators have been developed, which can be placed by direct puncture in the tumour. In contrast to laser ablation of liver tumours, there are significant technical problems that discourage MRI control of the intervention (pneumothorax, dislocation risk, necessary lateral or prone position); therefore CT is regarded as the modality of choice for insertion of applicators and control of the intervention.
The advantages of LITT in the lungs are the induction of larger ablation volumes and increased rate of complete tumour ablations due to the lower cooling effects by adjacent vessels and the lack of an impedance problem. The limitation of the thermal ablation of LITT is based on the phenomenon of carbonisation of tissues close to the electrode.

Radiofrequency ablation of metastases from renal cell carcinoma. a Axial CT image in lung window with patient in decubitus position showing the RF needle inserted in a metastatic lesion in the upper left lobe. b The RF needle inserted in a different lesion caudal to the first one

Lung metastases. a Transpulmonary chemoembolisation (TPCE) of the right lung. The catheter is seen in the right pulmonary artery. b Axial CT image in lung window shows partially necrotic lesion in the right lower lung lobe after TPCE. c Radiofrequency ablation with needle inserted in the lesion in the right lower lobe. d Axial T2-weighted MR image immediately after ablation shows heterogeneous halo surrounding the lesion due to necrosis. e Follow-up contrast-enhanced MR image after 6 months shows shrinking in size of the lesion with no enhancement

Liver metastases from colorectal carcinoma. 47-year-old patient with liver metastases from colorectal carcinoma. MSCT after LITT shows hypodense areas of necrosis with surrounding relatively hyperdense areas of hyperemia
References
Chrispin AR, Norman AP Pediatr Radiol 1974; 2:101–107
Diederich, Am J Roentgenol; Kersjes 1999, Radiology
Freyschmidt J, Galanski M. Handbook of Diagnostic Radiology: Thorax. Berlin, Heidelberg: Springer 2003
International Statistical Classification of Diseases and Related Health Problems-10 (2006)
Pistolesi et al. Switzerland medical Wochenschrift 1993; 123(11) 464.472
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Proschek, P., Vogl, T.J. (2016). Chest and Mediastinum. In: Vogl, T., Reith, W., Rummeny, E. (eds) Diagnostic and Interventional Radiology. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-44037-7_19
Download citation
DOI: https://doi.org/10.1007/978-3-662-44037-7_19
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-44036-0
Online ISBN: 978-3-662-44037-7
eBook Packages: MedicineMedicine (R0)