
Abstract
To obtain insight into the severity of lesions and for better prognostication, it is recommended that a scoring system be applied for GMH-IVH, PVE and PVL. These scoring systems are presented in Appendices 6.1–6.3, respectively.
Access this chapter
Tax calculation will be finalised at checkout
Purchases are for personal use only
References
De Vries LS et al (1992) The spectrum of leukomalacia using cranial ultrasound. Behav Brain Res 49:1–6
Van Wezel-Meijler G et al (1998) Magnetic resonance imaging of the brain in premature infants during the neonatal period. Normal phenomena and reflection of mild ultrasound abnormalities. Neuropediatrics 29:89–96
Volpe JJ (1989) Intraventricular hemorrhage in the premature infant – current concepts. II. Ann Neurol 25:109–116
Further Reading
Groenendaal F et al (2010) Complications affecting preterm neonates from 1991 to 2006: what have we gained? Acta Paediatr 99:354–358
Leijser LM et al (2009) Brain imaging findings in very preterm infants throughout the neonatal period: Part I. Incidences and evolution of lesions, comparison between ultrasound and MRI. Early Hum Dev 85:101–109
Leijser LM et al (2010) Is sequential cranial ultrasound reliable for detection of white matter injury in very preterm infants? Neuroradiology 52:397–406
Miller SP et al (2003) Comparing the diagnosis of white matter injury in premature newborns with serial MR imaging and transfontanel ultrasonography findings. AJNR Am J Neuroradiol 24(8):1661–1669
Van Wezel-Meijler G et al (2011) Ultrasound detection of white matter injury in very preterm neonates: practical implications. Dev Med Child Neurol 53 (suppl4):29–34
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 6.1: Classification of Germinal Matrix – Intraventricular Haemorrhage
Adapted from Volpe (1989):
-
Grade 1: GMH with no or minimal IVH (Fig. 6.1)
Fig. 6.1 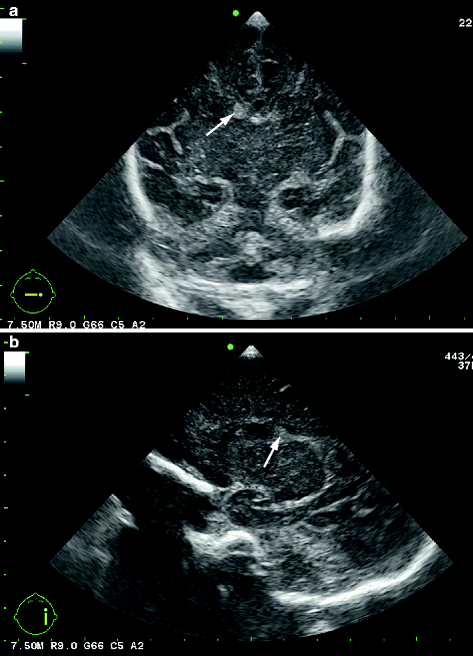
Grade 1 GMH-IVH in a preterm baby (GA 32 weeks, scanned 2 days after birth). (a) Coronal cUS at the level of the frontal horns of the lateral ventricles, showing right-sided GMH (arrow; grade 1 GMH-IVH). (b) Parasagittal cUS through the right lateral ventricle, also showing the small haemorrhage (arrow)
-
Grade 2: IVH (10–50% of the ventricular area on parasagittal view) (Fig. 6.2, see also Fig. 4.7b)
Fig. 6.2 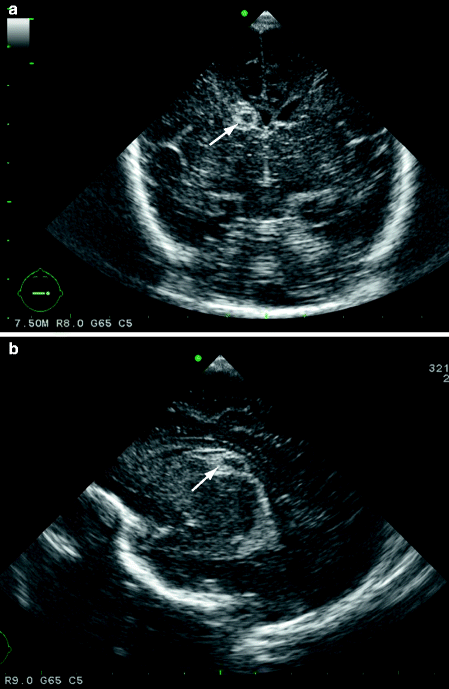
Grade 2 IVH in a very preterm baby (GA 25 + 3 weeks, scanned 3 days after birth). (a) Coronal cUS scan, level of the frontal horns of the lateral ventricles, showing right-sided IVH (arrow). (b) Parasagittal ultrasound scan through right lateral ventricle showing the IVH (arrow)
-
Grade 3: IVH (>50% of the ventricular area on parasagittal view, usually distends the lateral ventricle) (Fig. 6.3)
Fig. 6.3 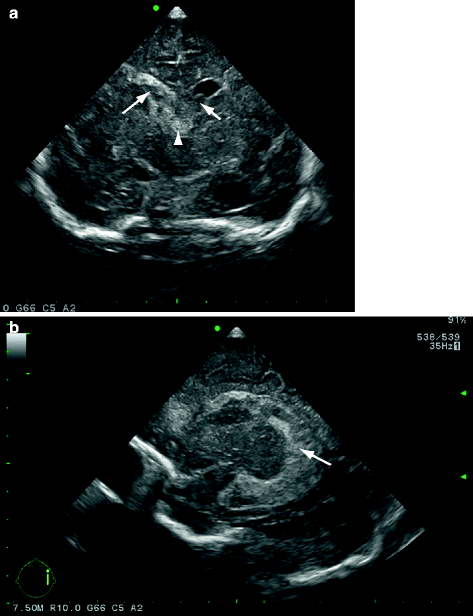
Grade 3 IVH in a near-term neonate born asphyxiated. (a) Coronal cUS at the level of the frontal horns of the lateral ventricles, showing large, right-sided IVH (arrow) and also small left-sided IVH (short arrow) distending the lateral ventricles. Also showing haemorrhage in the 3rd ventricle (arrowhead) and echogenic ventricular lining resulting from haemorrhage. (b) Parasagittal cUS through the right lateral ventricle, showing the large IVH (arrow) which almost completely fills and distends the lateral ventricle
-
Separate notation: PHVD (Fig. 6.4, see also Figs. 4.7c and 4.8)
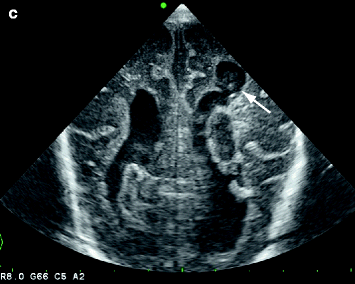
Fig. 6.4 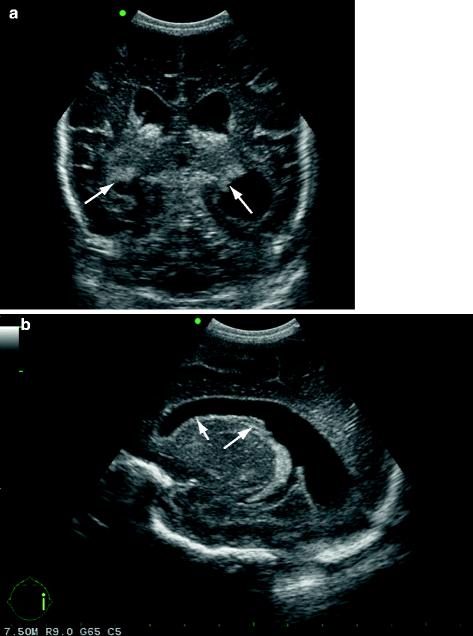
PHVD. Preterm baby, GA 29 + 4 weeks, cUS scan performed at postmenstrual age of 32 weeks. (a) Coronal at the level of the trigones of the lateral ventricles, and (b) Parasagittal through the lateral ventricle, showing remnants of bilateral IVH (arrows), dilatation of the lateral ventricles and echogenic ventricular lining (short arrow in b)
-
Separate notation: concomitant periventricular echodensity (including location and extent), referred to as “IPE” (intraparenchymal echodensity), representing PVHI (Fig. 6.5)
Fig. 6.5 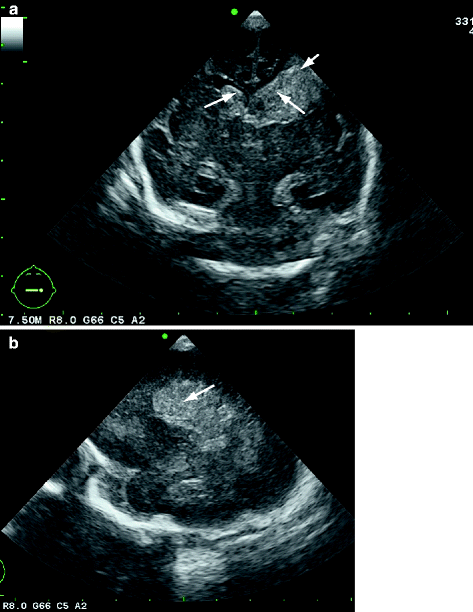
Grade 3 IVH with IPE. Preterm neonate, GA 28 weeks with initially normal cUS scans but large IVH developing 2 days after birth and IPE visible on the third day of life. (a) Coronal cUS at the level of the frontal horns of the lateral ventricles, showing bilateral IVH (grade 3) (arrows), complicated by a left-sided IPE, representing PVHI (short arrow). (b) Parasagittal cUS, showing the large IPE in the left fronto-parietal area (arrow). (c) Coronal cUS at the level of the trigone of the lateral ventricles: after 3 weeks a porencephalic cyst (arrow) developed in the area of the IPE. Remnants of the IVH are still visible in the lateral ventricles






Appendix 6.2: Classification of Periventricular White Matter Echodensity (PVE)
Adapted from van Wezel-Meijler et al. (1998):
-
Grade 0 PVE: normal echogenicity of the periventricular white matter (the echogenicity of the periventricular white matter being less than that of the choroid plexus) (Fig. 6.6, see also Figs. 3.3, 3.5, 4.2, 4.6a, b, 4.7a)
Fig. 6.6 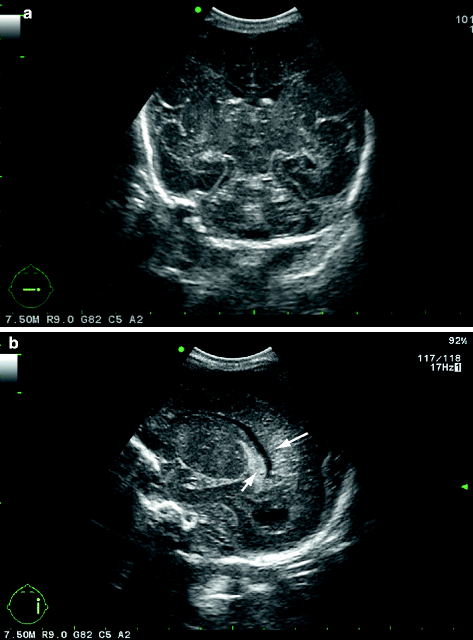
Preterm neonate, GA 28 weeks (same infant as in Fig. 6.5), having normal cUS scan on the first day of life without haemorrhage and with normal echogenicity of the periventricular white matter (arrow in b), being homogeneous and of lower echogenicity than the choroid plexus (short arrow in b). (a) Coronal scan at the level of the bodies of the lateral ventricles. (b) Parasagittal scan through the right lateral ventricle
-
Grade 1 PVE: moderately increased echogenicity of the periventricular white matter, the affected region (or smaller areas within the affected region) being (almost) as bright as the choroid plexus (Figs. 6.7 and 6.8 see also Figs. 3.6, 4.5c, 5.1f)
Fig. 6.7 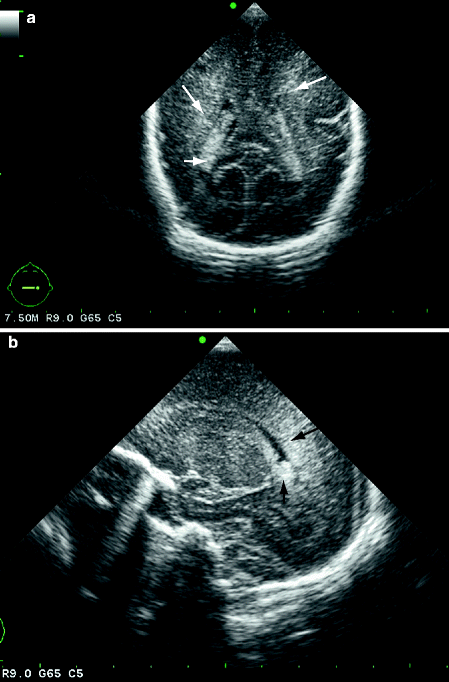
Grade 1 PVE. Preterm neonate, GA 27 + 2 weeks. (a) Coronal cUS at the level of the trigone of the lateral ventricles. (b) Parasagittal cUS through the left lateral ventricle. The echogenicity of the periventricular white matter (arrows) is mildly increased, being almost equal to that of the choroid plexus (short arrow)
-
Grade 2 PVE: seriously increased echogenicity, the affected region (or smaller areas within the affected region) being brighter than the choroid plexus (Fig. 6.9, also see Figs. 4.5d, e, 5.1b, 5.2b)
Fig. 6.8 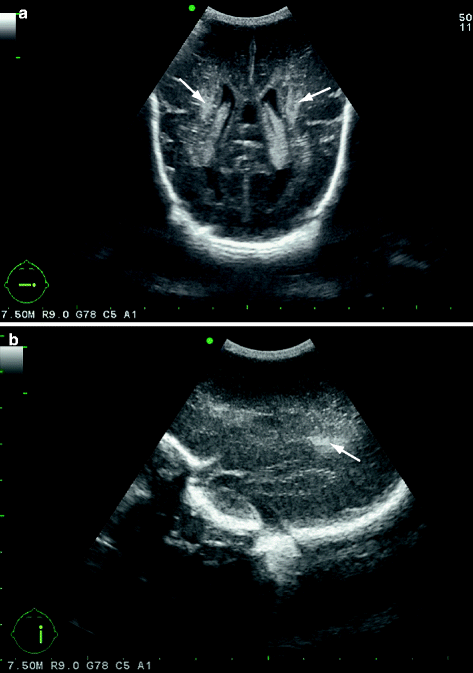
Inhomogeneous grade 1 PVE. Preterm neonate, GA 26 + 2 weeks. (a) Coronal cUS at the level of the trigones of the lateral ventricles. (b) Parasagittal cUS. The echogenicity of the periventricular white matter is inhomogeneously increased (arrows)
-
Separate notation: homogeneous, inhomogeneous (For inhomogeneous PVE see Figs. 4.5d, e, 5.1b, f, 5.2b, 5.3a, 6.9)
Fig. 6.9 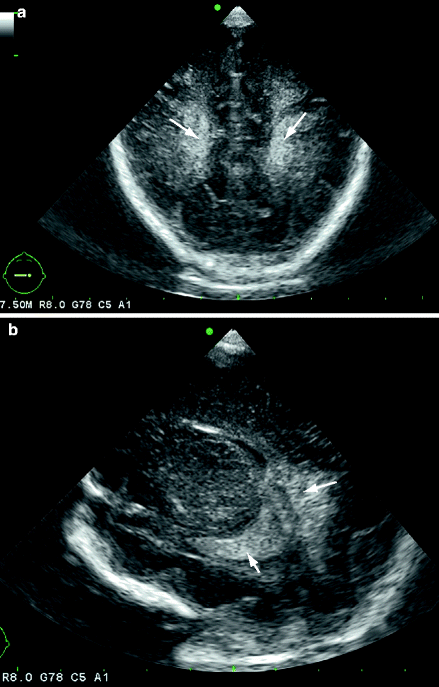
Inhomogeneous grade 2 PVE. Preterm neonate, gestational age 31 + 2 weeks. (a) Coronal cUS at the level of the parieto-occipital lobes. (b) Parasagittal cUS. The echogenicity of the periventricular white matter is seriously and inhomogeneously increased (arrows), exceeding to that of the choroid plexus (short arrow). This infant later developed cystic PVL (Fig. 6.11)




Appendix 6.3: Classification of Periventricular Leukomalacia
According to de Vries et al. (1992):
-
Grade 1: transient PVE persisting for ≥7 days
-
Grade 2: transient PVE evolving into small, localised fronto-parietal cysts (Fig. 6.10)
Fig. 6.10 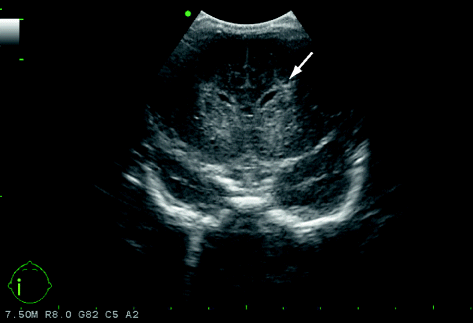
Grade 2 PVL. Preterm neonate, gestational age 27 + 2 weeks. Initially normal cUS scans. cUS performed 4 weeks after birth showing a small, single cystic lesion (arrow) in the frontal periventricular white matter on the left side
-
Grade 3: PVE evolving into extensive periventricular cystic lesions (Fig. 6.11)
Fig. 6.11 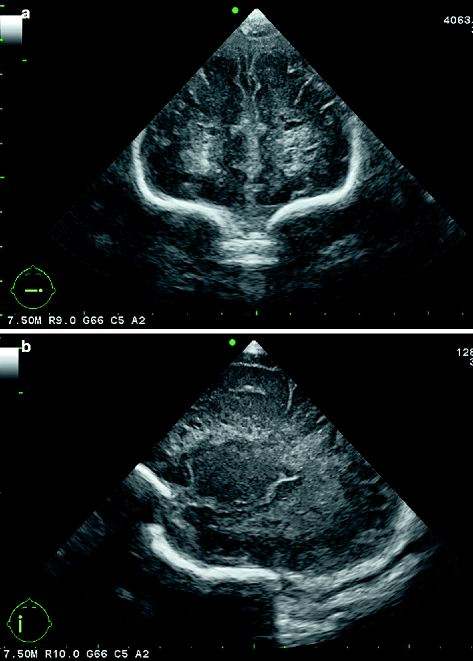
Grade 3 cystic PVL. Preterm neonate, gestational age 31 + 2 weeks, same child as in Fig. 6.9. cUS performed 5 weeks after birth. (a) Coronal at the level of the frontal lobes. (b) Parasagittal. There are cystic lesions in the fronto-patietal periventricular white matter
-
Grade 4: densities extending into the deep white matter evolving into extensive cystic lesions (Fig. 6.12)
Fig. 6.12 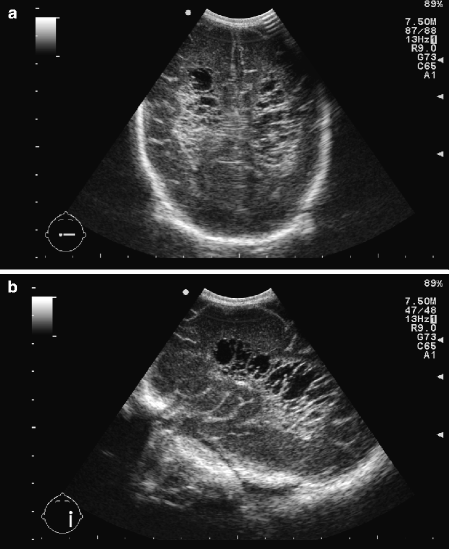
Ultrasound scan in a premature infant who gradually, over a period of weeks, developed extensive leukomalacia (PVL grade 4), showing cystic lesions extending into the deep white matter. This baby was one of monochorionic twins; the pregnancy had been complicated by severe twin-to-twin transfusion syndrome. (a) Coronal view at the level of the parieto-occipital lobes. (b) Parasagittal view



It should be noted that the incidence of “classic” PVL where this classification refers to has importantly declined over the last decade and that there has been a shift towards a more subtle, diffuse form of white matter injury (so-called diffuse white matter injury). For the detection of diffuse white matter injury, MRI is needed as it is not reliably depicted by cUS (see also Chapter 5).
Rights and permissions
Copyright information
© 2012 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Meijler, G. (2012). Scoring Systems. In: Neonatal Cranial Ultrasonography. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-21320-5_6
Download citation
DOI: https://doi.org/10.1007/978-3-642-21320-5_6
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-21319-9
Online ISBN: 978-3-642-21320-5
eBook Packages: MedicineMedicine (R0)