
Abstract
This essay studies the combination of virtual reality (VR) technology and conventional stroke rehabilitation physiotherapy. Specifically, we propose a novel therapeutic device coupled with an immersive VR software environment to foster hand rehabilitation. We first study the current state of the art in VR technology use in medical rehabilitation. Next, we investigate the conventional stroke rehabilitation process to integrate accepted methods of physical therapy into mobile games. The game system’s input device (V-rehab) is an improvement on existing rehabilitation equipment, designed to maximize interaction between user and game. We feature a prototype game system based on sensor hardware and a custom environment running on the Unity3D software platform. Finally, we show results of system testing and discuss the application of VR in stroke rehabilitation.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others



Keywords
1 Introduction
1.1 Research Background and Goals
Stroke is a medical condition in which poor blood flow to the brain results in cell death [1]. China has the highest incidence of stroke in the world. In recent years, the number of stroke survivors has increased with the development and progress of medical technology. However, about 75% of patients still suffer from varying degrees of motor dysfunction, especially hand motor dysfunction, with up to 10% of patients living with severe disability. The primary stroke hand dysfunction defects are buckling contracture, weakened grip, side clips, and other functional loss to palm and fingers [2]. Hemiplegic hand dyskinesia significantly reduces quality of life and increases the economic and psychological burden of patients as well as their families [3].
Prior research has demonstrated that exercise rehabilitation training can not only promote spontaneous nerve function recovery in patients with hemiplegia and help patients to restore central nervous system control and control of limb movement, but it can also prevent atrophy from muscle disuse and improve the recovery of motor function [4]. Physical therapy has become one of the most commonly used methods for rehabilitating motor function in clinical practice. At present, motor-function rehabilitation in patients with hemiplegia is still carried out under the guidance of a therapist, who assists patients with passive or auxiliary exercise training. However, these methods have obvious shortcomings:
-
(1)
Waste of manpower and material resources. Rehabilitation therapists cannot simultaneously guide more than a small number of hemiplegia patients in technique, and this costly and specialized field is impractical in a huge developing country like China;
-
(2)
Rehabilitation training is mechanically tedious: hemiplegic patients rarely participate enthusiastically, which leads to lapses in treatment;
-
(3)
It is very difficult to obtain feedback to gauge the intensity and effectiveness of rehabilitation training [5].
Existing research shows that the introduction of virtual reality technology and games into rehabilitation training is helpful for the rehabilitation of patients with motor dysfunction [6]. This method can provide a variety of feedback during training and reasonable rehabilitation recommendations according to the patient’s specific condition. A virtual environment can greatly increase patients’ initiative to participate in therapy, so as to effectuate rehabilitation [7]. With its three primary characteristics of interaction, imagination, and immersion, VR technology uses a synergistic merger of virtual and real environments to give patients strong sensory stimulation [8], which can greatly improve their enthusiasm for training.
1.2 Research Status
Since late in the twentieth century, researchers have extensively studied virtual reality technology and its application in rehabilitation medicine. In 2001, U.S. researchers developed a five-finger rehabilitation robot. Each fingertip is fixed with a prosthetic which can allow the entire finger to flex and extend [9]. In 2003, researchers at the University of Manchester in the U.K. designed an exoskeleton-based system for physical and occupational hand therapy, which uses a modular design for a four-finger rehabilitation exercise in an interactive VR environment [10]. The American company Rolyan developed and successfully marketed a CPM (Continuous Passive Motion) machine for the rehabilitation of small joints such as those of the wrist and fingers. Kagawa University in Japan developed a rehabilitation device that restores the flexibility of the finger, which allows patients to control the movement of a virtual object by a pre-designed trajectory [11]. Ljubljana University in Slovenia has developed a finger-rehabilitation game system based on a virtual maze, the patient controlling the movement of a ball in the virtual environment by changing the position of the hand [12]. New Jersey Institute of Technology developed a VR-based hand-rehabilitation system for individual motion of the finger and coordinated movement between the fingers. A sensor reads the articulation angle of the finger and shows it in a virtual environment, where different degrees of bending play different piano sounds [13]. Purdue University in the U.S. has also developed rehabilitation equipment to restore patients’ writing ability and guide patients in English writing [14].
There is a gap between China and foreign countries in the field of VR rehabilitation research. At present, several universities and the Rehabilitation Research Center in China have researched robots for rehabilitation, but the main focus is on joint rehabilitation and single-function rehabilitation robots. Harbin Institute of Technology has developed a new type of rehabilitation training manipulator for hand movement dysfunction that uses gearing, integrated mechanical sensors and angle sensors to achieve exercise, but at present only a single finger can be trained at a time [15]. Southeast University developed a training device for finger rehabilitation, with both active and passive assistance. Its disadvantage is the lack of real-time feedback and accurate evaluation of technique and progress [16]. In 2007, Harbin Engineering University developed an automatic finger rehabilitation trainer using a micro-DC motor to drive a special curved rod, allowing a patient’s finger to perform mechanical movements according to various preset modes [17]. Hua Zhong University of Science and Technology designed a rehabilitation training robot for improving the ability of patients with joint activities using pneumatic muscle assistance, conducting preliminary experiments in the hospital. Although the immersive quality of its virtual environment was found to be deficient, the system still demonstrated some beneficial effect [18].
1.3 Research Purposes
To summarize, the use of VR technology to help patients in physical rehabilitation is feasible and effective. In the course of this research, we evaluated several VR environments; although each had certain positive qualities in game form and rehabilitation effectiveness, an almost universal problem was that the equipment was too precise and too expensive, not suitable for the general public to use. In addition, despite the era of mobile Internet, there has still been very little research on VR technology to help the rehabilitation of stroke patients on mobile platforms such as smart phones. Smartphones, however, have already reached 57% penetration in China [19]. Mobile games are a potentially convenient and easy-to-use rehabilitation training medium. The purpose of this project was to design a VR game system for hand rehabilitation of stroke patients. Interactive input devices improve existing hand rehabilitation solutions, and virtual reality mobile games offer an innovative immersive healing environment not possible with static mechanical tools. In combination with the scientific principles and methods of hand rehabilitation in stroke patients, this project is devoted to allowing patients to perform hand rehabilitation in easy-to-use and useful games.
There are three main parts to this study: (1) Build a prototype device, (2) Develop and implement the games on mobile platform, and (3) Test the prototype.
The object of this study is to design mobile games based on mobile virtual reality that can help stroke patients recover from hand rehabilitation. According to the prior art, hand movement data of the patient is acquired by using existing hand rehabilitation equipment (for example, the data of the movement direction, the movement distance and the hand grip force are mainly obtained by the three-dimensional motion sensor with a G-sensor). These data are imported into the game system as the input data and the game interface gives the corresponding feedback, so as to complete the interactive process of the game. The specific research contents are as follows:
-
First, investigate the existing virtual reality technology and products for physical rehabilitation, to evaluate their advantages and limitations.
-
Second, study the mechanical aspects of hand rehabilitation therapy to help determine appropriate game motifs to foster hand exercise;
-
Third, research the specific types of target users to understand their pain points in the rehabilitation process;
-
Fourth, select a suitable hand rehabilitation device, optimize its shape, and install sensors to collect movement data of users’ hands;
-
Fifth, develop a mobile application specifically to suit the target users’ behavior.
2 Design Research
2.1 Stroke and Rehabilitation Training
Stroke, also known as cerebrovascular event (CVE), cerebrovascular accident (CVA), cerebrovascular incident (CVI), or brain attack, refers to brain cell death caused by cerebral ischemia. Stroke is divided into two types: one is ischemic stroke caused by vascular obstruction; another is hemorrhagic stroke caused by bleeding. Either ischemic or hemorrhagic stroke can cause brain dysfunction [1]. Common symptoms of stroke include but are not limited to: an inability to move unilateral limbs or the partial paralysis of one side of the body; an inability to understand language or to speak; dizziness; an inability to see one side of the visual field. [20, 21] The symptoms of a stroke can become permanent sequelae.
In 2010, there were about 17 million stroke incidents and 330 million survivors had a history of stroke. Between 1990 and 2010, the incidence of stroke in developed countries dropped by about 10%, while in developing countries it increased by 10%. [22] Stroke was the second most common cause of death in 2013, accounting for 12% of the total (6,400,000 cases) [23], of whom about 3.3 million were due to ischemia stroke deaths and 3.2 million due to hemorrhagic stroke [23]. About half of those who have had a stroke have an average remaining life of no more than one year [4]. Overall, two-thirds of strokes occurred in people over 65 years of age [22].
Most patients with cerebrovascular disease have different levels of hand dysfunction in the process of functional recovery, which affects their ability to take care of themselves in normal life and their professional ability to return to society. The functional recovery process is begun a few days after onset of cerebrovascular disease. Recovery was most rapid in the first 3 months and was slowed down after 3 months due to disuse syndrome and misapply syndrome. Function recovery of the lower extremity is better than that of upper extremity, while the upper extremity is dominated by flexible, coordinated and skilled exercise. Recovery is not easily achieved, especially the function of the hand. The recovery is usually divided into the following stages:
-
Flaccid paralysis period: Hand, fingers included, is weak and feeble.
-
Fretting period: Fingers have partial active flexion but cannot stretch.
-
Holistic grasping period: Hand can grasp as a whole without finger-straightening extension action but cannot relax.
-
Functional recovery period: Patients can grip with the whole palm, such as cylindrical or spherical objects. Although performance is not fully competent, and the function of the hand is limited, the fingers can scratch voluntarily.
-
Functional period: All grasping patterns are under patient’s control.
2.2 User Interview
Our research method was primarily based on a user interview.
Interviewees: Patients with a stroke experience who are recovering or who have recovered.
Interview form: One-to-one interview
Interview purpose: To understand the basic physical condition of patients during rehabilitation, rehabilitation methods, and psychological and physical demands during the rehabilitation process.
Main questions:
-
Medical history (including age, stroke time, affected part, duration of rehabilitation)
-
Hand rehabilitation training method and auxiliary equipment
-
The family’s role in healing
-
State of mind and emotional state since suffering strokes
-
Lifestyle and exercise before strokes
-
Views and attitudes towards the combination of virtual reality technology and stroke rehabilitation.
The following is an overview of interview records of two stroke patients:
Mr. Zou: In the summer of 2011, Mr. Zou suffered from a stroke, and is now in the later stages of rehabilitation. He can now take care of himself, but his impaired right arm injury is permanent. Mr. Zou was hospitalized for three months after the stroke onset and completed systematic rehabilitation training in the rehabilitation department of the hospital to restore language ability and swallowing ability. He has insisted on daily rehabilitation exercises in the year after his discharge from the hospital, and with the help of his wife has maintained passive exercise training on the muscular atrophy of the right arm (rehabilitation ball, fingerboard, tractor), which he can now lift slowly. During his recovery, Mr. Zou often felt up and down, but has been supported by his family’s tolerance. He has heard of VR technology and showed interest in it,; he expressed willingness to try it if the price is reasonable.
Mr. Zhu: Following a sudden stroke (reversible ischemic neurological deficit) in November 2016, his physical condition has returned to normal with no sequelae now. Hospitalized for a month, he performed daily bed activities and passive exercise with acupuncture and massage under the guidance of doctors’ rehabilitation. After discharge from the hospital, it was very difficult for Mr. Zhu to persist in completing a set of movements hundreds of times without supervision from a doctor. He felt very impatient when his progress did not recover, and eventually spent an additional month to fully restore function. Although the current recovery prognosis is optimistic, Mr. Zhu and his family’s life have still been greatly affected. Since suffering from stroke, he has become more aware of the importance of health. As to the introduction of new technologies, he said that he would accept any kind of technology that can make him recover faster.
In communicating with stroke patients, we learned that patients must remain at home for an extended period during the rehabilitation process, and they usually cannot meet the standard training requirements without the supervision of a doctor. Furthermore, the lack of positive feedback in the process causes patients to suffer some emotional distress. Patients generally regard feedback and incentives as important during the rehabilitation process; our contacts reported that they would appreciate more reward forms in the game design, so that they can get a sense of accomplishment in the game process, as well as to ensure adequate training exercise. Finally, rehabilitation equipment should ensure safety and comfort, and it should be able to be handled by patients independently.
2.3 Competitive Product Analysis
The hardware used by patients for rehabilitation also serves as the operating handset for the game system. In form, this is essentially an improved version of existing mechanical hand rehabilitation equipment. Among the devices that are already available on the market, this article compares their sensitivity to hand motion and aspects of their operation, operationalized as follows:
-
Operation: Hand rehabilitation training methods can be divided into active training and passive training. Active training is exercise through patients’ own muscle flexion and extension, while passive training is hand movement assisted by the equipment via motors or mechanical force devices.
-
Flexibility: The degrees of freedom of hand movement and the number of joints involved (Fig. 1).
Fig. 1. 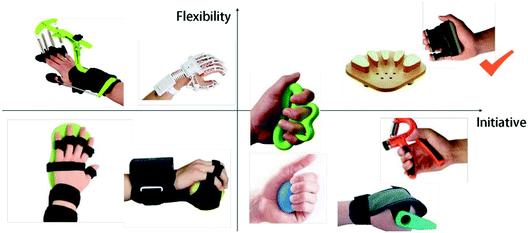
Comparison chart of hand rehabilitation equipment

In order to ensure the rationality of the rehabilitation equipment, the choice of equipment refers to the existing hand rehabilitation equipment and is evaluated by the scientific program of hand rehabilitation. To offer the user a greater sense of interactivity and fully autonomous exercises during the rehabilitation process, the device should to have higher initiative and sensitivity and should be able to precisely record data for each finger press. Therefore, we chose a device with four pressure elements that users will need to press with the four fingers.
The selection of a virtual reality gaming platform was based on two considerations, one being the cost of purchasing head-mounted devices, and the second being the compatibility of the device for different phone size and system version. In order to allow use of these devices on a variety of mobile phones and to make this stroke rehabilitation system affordable, we chose the cheaper, more compatible Google cardboard and Google Daydream as a basic platform; users may choose a higher-cost platform according to economic situation, but we decided on this as a baseline (Fig. 2).

Comparison chart of existing virtual reality devices
To operate a VR game, the user opens the virtual reality game application in the smartphone and inserts the phone into a Google Cardboard or Google Daydream visor. The content displayed in front of the user will change via the phone camera and sensing by the phone or visor’s built-in gyroscope as the user moves his or her head. Figure 3 shows a user following the game interface training introduction to interact with the game scene.

Use of Google Daydream
3 System Design
This project used the Unity3D game software development platform with the “Google Cardboard SDK for Unity” plug-in to develop mobile virtual reality games. Our mobile game system structure is shown in Fig. 4.

Game system structure
3.1 Hardware Design
As shown in Fig. 5, the game system is divided into three parts: users, hand equipment, and mobile VR games. The user’s finger movement is captured and recorded by the pressure sensor in the handgear, and the data is read by the Bluno module and transmitted to the handset program via Bluetooth. After the mobile program receives the input data, the system responds and changes the corresponding scene in the screen and feedbacks to the user. These form the complete interactive process for our system.

Technical path diagram
Because pressure is the main action in stroke rehabilitation training, a pressure sensor was deemed as the best choice for input sensing. The pressure sensor we chose was the FSR402 Resistive Film Pressure Sensor, which converts the pressure applied on the FSR sensor film area into a change in resistance to obtain pressure information. The higher the pressure, the lower the resistance, allowing it to be used at 0 g–10 kg pressure to meet our design needs. It is small enough and light enough to be used in equipment with high experience requirements (Fig. 6).

FSR402 Resistive Film Pressure Sensor
Based on the requirements of our project, we needed a device to communicate with the Arduino microcontroller and mobile phone. The Bluno Bluetooth module suited our requirements as the communication unit between our mobile gaming and hardware device (Fig. 7).

Bluno Nano
We implemented a hardware device consisting of an Arduino microcontroller, a Bluno Bluetooth module, and pressure sensors. Four pressure sensors serve as the proximal interface for the user; they receive the user’s movement information directly. In the game, we defined the meaning of each of the four finger presses, each representing different actions in the user’s view. The function of the pressure sensor is to converts finger pressure into an electrical signal through the resistance effect described above, and to send the data to the microcontroller via pins connected to the Arduino.
The Arduino microcontroller program will rapidly poll the four pressure sensors. After acquiring this information in each polling cycle, the microcontroller will know which fingers made a pressing action, and with how much force. Then the microcontroller will package the pressure sensor information and send it to the Bluetooth module for further processing.
Bluno receives the packaged signal from the microcontroller and uses Bluetooth to send the package to the mobile phone. It should be noted that before the first use there is a procedure for pairing the Bluno Bluetooth module with the phone’s Bluetooth device; only after this pairing process can data be exchanged.
After the mobile device receives this data packet, it will decode it according to the reverse process of that of the microcontroller and restore it to the original data of the four pressure sensors. By analyzing these data, the mobile game program can know what operations the user has performed and make corresponding modifications to the program interface according to these operations to provide feedback. Because the electronic components used to implement this process are relatively mature products and our products do not require a large data stream, the program is highly responsive (Fig. 8).

Handset hardware combination
3.2 Handset Shape Prototype
Because the handset it is hand-held equipment, we needed to ensure that all electronic components such as hand-pressure devices, sensors, control panels, batteries, switches, and other devices will fit into the product, and that the product can be held by the average-sized hand and comfortably fit the shape of the hand (Fig. 9).

Shell of handset
For handset design, we designed hand lines based on ergonomics principles suiting ease and comfort for users (Fig. 10).

Ergonomic dimensions of human hand
Depending on the size of the hand and the features of the product, our design was most concerned with the fit of the thumb muscle to the handset, as this contributes most to the degree of comfort the when users hold the product.
The following is the modeling iteration process:
-
Stage 1:
The initial model (Fig. 11) used an ellipsoid as the main form with the original four finger pressing parts of the same length. Our primary goal was to achieve a good fit between the thumb muscles with the handset.
Fig. 11. 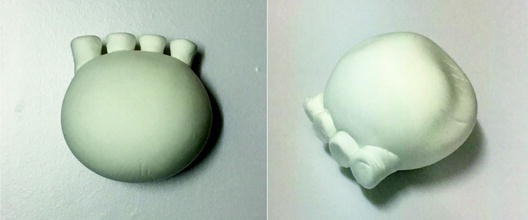
Preliminary model no. 1
-
Stage 2:
In the second model (Fig. 12) we made more adjustments in the curve of the arc which took into account the state of the full finger press given differing heights of each of the four fingers. Thus, the length of each button is adjusted according to different height. At the same time, the hand grip has also been changed to a greater curvature, making an overall shape resembling a bear’s paw.
Fig. 12. 
Preliminary model no. 2
-
Stage 3:
After confirming the design of the finger portion and the design of the bottom surface, we made the bottom line clearer on the original model. At the same time, the buttons were enlarged, resulting in a slightly mellower whole shape. Meanwhile, corresponding concavities and convexities were added to the hand-fitting area, so that the handset fits the natural contours of the palm.
-
Stage 4:
The previous model had a rather inelegant appearance, so we made a few further adjustments.


The shape of the finger areas was improved to make it more abstract and give up the rounded shape; we also performed better blending on the palm-contact surfaces, making the shape more concise and clear. The final model is shown in following figure (Figs. 13, 14 and 15).

Digital model no. 1

Digital model no. 2

V-rehab model rendering
4 Game Design
4.1 Design Platform
Our plan is to guide and encourage patients to carry out rehabilitation training, through the development of a human-computer interaction device in the form of a mobile game that includes virtual reality, sensing, networking. There are two main reasons for choosing a mobile phone as the platform: (1) As one of the fastest-growing platforms in the past decade, mobile phones have become fully integrated into people’s lives and work, so using a cell phone as a rehabilitation device should feel quite natural to many patients. (2) There has been comprehensive recent development of mobile devices and virtual reality technologies. For example, Google Cardboard can display the content in a split-screen in the mobile phone to produce a stereoscopic effect by the parallax of the two eyes. Reference to these relatively mature products allows us to move our product quickly through the technology development phase, to facilitate our human-computer interaction analysis and experiments.
Virtual reality is a new and emerging discipline that communicates and interacts with users through a variety of sensors, and ultimately simulates realistic, real-time three-dimensional environments. There are a number of aspects characterizing virtual reality technology, including: (1) Presence refers to the user’s feeling as the protagonist in the simulated environment. The test of the ideal simulation environment measures the extent to which it is difficult for the user to distinguish between reality and fantasy. (2) Autonomy refers to the degree to which objects in the virtual environment act according to the laws of physical movement in the real world. (3) Multi-perception refers to the auditory, tactile, motor perception, and even taste, smell, perception and other senses besides visual perception. (4) Interactivity refers to the extent to which the user may manipulate objects in the simulated environment and receive feedback.
Virtual reality technology was applied to medicine soon after its development and maturity. In the treatment of some patients, a relatively special environment is necessary, often calling for higher cost, and yet the solutions still lack realism. Virtual reality technology offers a channel that can be adapted to the specific needs of users as well as providing satisfactory realism. When properly implemented, virtual reality technology when implemented can provide significant help to the medical field, in particular at-home therapy. In our project, due to the need to provide stroke patients with a environment sufficiently real to guide them in various kinds of rehabilitation training without becoming being tedious, we felt virtual reality was a good choice.
4.2 Game Content
Stroke rehabilitation patients’ hand movement ability is impaired, so our game design needed to take full account of the patient’s finger movement, in careful combination with the hand acupressure rehabilitation equipment. To do so, it is necessary to fully mobilize the motion of the four fingers during game operation. We devised the game settings in an attempt to achieve optimally effective finger movement according to the sequence and frequency of practical finger rehabilitation exercises. In the game design, we developed two styles of game scenes based on user characteristics of different genders and ages.
Scene 1: “Aircraft War” features explosions and realistic effects, incudes awards or penalty.
Game scene: Simulation of shooting down enemy planes in an actual first-person shooting confrontation. The player’s perspective is to drive a tank equipped with a machine gun. An enemy set in the game will send out a low-flying fighter to prevent the player from moving forward and will cast bombs at the right place to injure the player. Players must operate the tanks and use the machine guns to shoot as many enemy planes as possible to crash them, one point for each. The game scene is as shown (Fig. 16).

Plane war
Game Operation: A total of five operational dimensions; four fingers control the movement (forefinger controls fire, middle finger controls moving to the left, fourth finger controls moving forward, little finger controls moving to the right.), head rotation controls firing direction.
Under such a dynamic and stimulating environment, patients can train the pressing force of the four fingers, and it can also assist in training the hand to grasp the equipment. Through the control of frequency and azimuth of flying planes, we can guide users to press four fingers at a certain frequency and fully exercise their finger joints and muscles.
Scene 2: “Harvest Forest” is a more leisurely game offering players a more relaxed and pleasant experience.
Game scene: Players wander in the forest according to the established route, along the way catching falling fruit from the trees with a basket. The basket must be placed at one of four possible places to catch the fruit, which is controlled by four fingers. Players need to catch as much fruit as possible, each catch earning a gold coin (Fig. 17).

Harvest forest
Game operation: The four buttons on the handset correspond to the four locations where the fruit falls. Press one button and the basket in the scene will quickly move to the corresponding position to catch the falling fruit.
The patient can fully exercise the joints and muscles on the hand while controlling the basket using four fingers, and at the same time the frequency and location of the fruit drop are programmed to meet the rhythm and frequency of finger rehabilitation exercises, so as to help patients complete the finger exercises per the program of therapy and avoid muscle or joint damage caused by improper exercise during the game.
4.3 Application Design
Aside from the game portion of the application, there are also device connection and data recording modules present in the mobile application. As for the connection module, the mobile application will automatically search for the user’s V-rehab equipment via Bluetooth. After matching the equipment, the user may select a game and then follow instructions to put the mobile into a Google Cardboard or Google Daydream headset. The user may now perform rehabilitation training in the panoramic game (Fig. 18).

Application interface
After the user completes the game, the application can record the progress results, including the number of repetitions of the exercise, duration of the exercise, finger flexibility and indicator completion percentage. The condition of rehabilitation can be intuitively displayed in the data recording module, achieving the effect of supervision and providing incentives. At the same time, the user’s family members can also familiarize themselves with the patient’s training situation through the application and give positive encouragement to the patient’s progress.
4.4 Test and Optimization
After developing the basic game system prototype, including the improved hand rehabilitation device prototype and the mobile phone virtual reality game prototype, we tested the game system and used the results to draft a plan for improving the design. The test was divided into two parts, one being the test of comfort level when the user grasps the equipment and presses the buttons; the other being the test of the smoothness of the game scene with the device.
Hardware testing:
Subjects: Subject A, male, 22 years old, completely healthy with no injuries to his hand. Subject B, male, 22 years old, suffered a ligament strain in hand a month previous. Current hand rehabilitation has reached 80%, fingers are not as flexible as they used to be in fine motor function but are able to do simple press and hold.
Test tasks: (1) Grasp the handset, hold one minute; (2) Press the buttons on the handset with the index finger, middle finger, fourth finger and little finger in the order, do ten groups of this movement at a constant speed.
Test Record: Recorded the pressure intensity of the first and the tenth group of the finger press of two volunteers. Asked the two volunteers about the comfort of the handset, and also asked about the softness and smoothness of the equipment surface felt by the hand. Asked the degree of fatigue of the hand after holding the equipment for a long period of time.
Test results: Subject A: The difference of finger press intensity between the first group and the tenth group was within the 0.5F (since the device measures capacitance, F or farads is the unit of pressure in the Arduino), which can be regarded as almost no fatigue; Subject was satisfied with the comfort of the handset and fairly satisfied with the texture of the surface. Subject reported no significant fatigue after an extended period grasping the handset. Subject B: The difference of finger press intensity between the first group and the tenth group was about 1.2F. Subject was satisfied with the comfort of the handset and the texture of the surface. Subject reported feeling as though the equipment was a little heavy after gripping it for an extended period.
Improvement proposals: There is still a difference in muscle endurance between hand-impaired and healthy people. In order to minimize the burden on the user’s hand so that the patient does not feel tired after prolonged use, the shell and components of the hand equipment should be made of lighter materials.
Game scene testing:
Subjects: Subject C, male, 50 years old, completely healthy with no injuries to his hand. Subject D, male, 59 years old, suffered a sudden stroke about one year before (reversible ischemic neurological function defect) and current physical condition is basically restored to normal. Since leaving the hospital, Subject D has been insisting on rehabilitation exercises at home, including the use of equipment to restore finger flexibility and arm strength.
Test tasks: (1) start the game “harvest forest” with Google Cardboard; (2) In the harvest forest, hold the equipment and complete the game of about 90 s.
Test Record: Record the number of fruits that two volunteers have caught in the game. Ask two volunteers about the head burden they feel when wearing the device, the clarity of the field of vision, the degree of dizziness when turning the head, the smoothness of the response while operating the equipment, and an appraisal of the game tasks.
Test results: Subject C: Equipment felt slightly heavy. Satisfied with visual clarity of the screen but felt a bit of dizziness when moving head. The screen gives very smooth feedback for the finger press, and the operations conforms to intuition. Subject D: Equipment felt slightly heavy. Felt a sense of dizziness when moving head. The feedback of the scene is adequately smooth during the game. The linkage effect of the other three fingers except the index finger is apparent, and this leads to the misoperation from time to time.
Improvement proposals: 90 s per round of intensive operation may bring heavy burdens to the users, such as causing dizziness and hand fatigue. One way to improve is to shorten the round of time, such as from 90 s to 60 s per round. The second way is to increase the number of frames so as to reduce dizziness.
5 Summary and Improvement
This work combines the emerging virtual reality technology with the hand rehabilitation training of patients needing stroke rehabilitation by studying the existing technology. We developed virtual reality games on the Android platform and focused on the user experience of existing products.
We conducted thorough research on existing VR technologies and games for medical rehabilitation and have reached two conclusions: First of all, the proactiveness of patient training increased by applying VR technology to medical rehabilitation. Secondly, a number of domestic and foreign universities, as well as research companies, have developed prototypes of the relevant products. Thirdly, a personal computer is necessary for the display in existing products, and for treatment users need to purchase expensive equipment, such as Kinect somatosensory equipment. This has increased the cost of rehabilitation to some extent and is not suitable for patients with ordinary conditions to enjoy gamification of rehabilitation. Migrating such therapeutic products to smartphone devices make the product available to a more diverse population.
Subsequently, the article conducted a detailed investigation of stroke conditions, rehabilitation methods and patients undergoing rehabilitation, and interviewed two patients in the later rehabilitation phase to derive basic product positioning and design aims. In the research of the prior art, we make a detailed comparison of current hand-rehabilitation products and existing virtual reality head-mounted devices, finally settling on a finger-pressure device as the hardware improvement target while using Google Cardboard and Google Daydream as the head-mounted device.
In V-rehab’s hardware design, sensors and Bluno (a combination of Arduino and Bluetooth module) were used for functional prototypes. Pressure sensors perceive hand-movement and Bluno reads the data and packages and transmits it to the mobile game via Bluetooth communication as a “handle” for the game. As for the shape prototype, applied ergonomic considerations and made it accommodate all electronic equipment. After several iterated improvements, we designed an attractive and comfortable handset which can accommodate intelligent hand rehabilitation equipment. In terms of game design, two game scenarios were designed that considered the characteristics of different patient groups. In combination with the four-finger operation of the hand rehabilitation equipment, corresponding game operation settings were designed so that the four fingers were trained according to standard therapeutic practice.
Finally, after developing the prototype of the game system, we invited several volunteers to conduct user tests. We divided the volunteers into two groups: those whose hands exercise functionally and half-hand-impaired people. The user tests aimed to judge whether the game system is suitable for hand-impaired people to use. The test was divided into two parts, testing the handset and testing the gaming experience. Combined with the user’s performance and attitudes, this paper proposes an improvement solution for both components, and this can be further studied in the future.
This article is an attempt to apply virtual reality to stroke rehabilitation training. The rehabilitation target is limited to the hand, specifically the restoration of the gripping and squeezing functions of affected fingers. Stroke rehabilitation requires training of many body functions, especially for the hand in restoring grip, wrist rotation, and other aspects. It can further be improved by exploring the game design for rehabilitation of other body functions of stroke patients. For this experiment, we only developed a simple action game scene with a simple plot. Developers can design more complex scenarios and scenes in order to understand the characteristics of patients with stroke and help them recover. In addition, this study did not establish a complete recovery evaluation mechanism due to time constraints. Thus, comprehensively assessing the recovery effects for patients playing virtual reality games wearing head-mounted equipment is beyond the scope of this paper. Future research can verify the effect of virtual reality technology for rehabilitation of stroke patients with fuller attention to recovery assessment methods. In conclusion, our design is a small attempt to solve the traditional problems with new technologies. With the development of medical technology and virtual reality technology, virtual reality will undoubtedly continue to provide options for medical treatment.
References
What is a Stroke? National Heart, Lung, and Blood Institute, 26 March 2014. Accessed 26 Feb 2015
Gabriele, W., Renate, S.: Work loss following stroke. Disabil. Rehabil. 31(18), 1487–1493 (2009)
Tierney, N.W., Crouch, J., Garcia, H., et al.: Virtual reality in gait rehabilitation. MODSIM World (2007)
Riwu, L., Maoen, L., Shihai, P., et al.: Mandatory exercise therapy in the treatment of stroke hemiplegia clinical application. Cardiovasc. Cerebrovasc. Dis. Prevent. Control 7(2), 97–98 (2007)
Dongrui, Z., Geng Yanjuan, X., Lisheng, Z.X., Guanglin, L.: Design and implementation of virtual reality hand rehabilitation training system. Integr. Technol. 2(4), 33–40 (2013)
Saposnik, G., Mamdani, M., Bayley, M., et al.: Effectiveness of virtual reality exercises in stroke rehabilitation (EVREST): rationale, design, and protocol of a pilot randomized clinical trial assessing the Wii gaming system. Int. J. Stroke 5(1), 47–51 (2010)
Levanon, Y.: The advantages and disadvantages of using high technology in hand rehabilitation. J. Hand Ther. 26(2), 179–183 (2013)
Saposnik, G., Levin, M.: Virtual reality in stroke rehabilitation: a meta-analysis and implications for clinicians. Stroke 42(5), 1380–1386 (2011)
Uurda, J.P.R., Vroohhoven, R.H.: Robot-assisted surgical systems new era in laparoscopic surgery. Ann. Roy. Coll. Surg. Engl. 84, 223–226 (2003)
Sarakoglou, I., Tsagarakis, N.G., Caldwell, D.G.: Occupational and physical therapy using a hand exoskeleton based exerciser. In: IEEE/RSJ International Conference on Intelligent Robots and Systems, pp. 2973–2978 (2004)
Guo, S., Song, Z., Song, G.: Development of a self-assisted rehabilitation system for the upper limbs based on virtual reality. In: Proceedings of 2007 IEEE International Conference on Mechatronics and Automation, pp. 1452–1457 (2007)
Bardorfer, A., Munih, M., Zupan, A., et al.: Upper limb motion analysis using haptic interface. IEEE/ASME Trans. Mechatron. 6(1), 253–260 (2001)
Adamovich, S.V., Fluet, G.G., Mathai, A.: Incorporating hapic effects into three-dimensional virtual environment to train the hemiparetic upper extremity. IEEE Trans. Neural Syst. Rehabil. Eng. 17, 512–519 (2009)
Kim, Y.K., Yang, X.: Hand writing rehabilitation in the haptic virtual environment. In: IEEE International Workshop on Haptic Audio Visual Environments and Their Applications, pp. 161–164 (2006)
Liu, H.: Hand injury rehabilitation manipulator structure design and analysis. Harbin Institute of Technology Library, Harbin (2007)
Zhou, S., Gong, Z.: Discussion on the definition of virtual reality. Comput. Simul. 23(9), 219–222 (2006)
Yu, J., Qian, J., Shen, Y., et al.: A finger rehabilitation device mechanism and control experiments. Chin. J. Tissue Eng. Res. Clin. Rehabil. 14(30), 5596–5601 (2010)
Zhang, J.: Research on finger rehabilitation system based on virtual reality technology, Huazhong University of Science and Technology, Wuhan (2012)
Pew Research Center: Spring 2015 Global Attitudes Survey, Q71&Q72 (2015)
Donnan, G.A., Fisher, M., Macleod, M., Davis, S.M.: Stroke. Lancet. 371(9624), 1612–1623 (2008)
What are the Signs and Symptoms of a Stroke? National Heart, Lung, and Blood Institute, 26 March 2014. Accessed 27 Feb 2015
Cotran, R.S., Kumar, V., Fausto, N., Robbins, S.L., Abbas, A.K.: Robbins and Cotran Pathologic Basis of Disease. Elsevier Saunders, St. Louis (2005). ISBN 0-7216-0187-1
Who is at Risk for a Stroke? National Heart, Lung, and Blood Institute, 26 March 2014. Accessed 27 Feb 2015
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Yu, J., Jiang, R., Feng, Y., Yuan, M., Kang, Y.I., Gu, Z. (2018). Mobile VR Game Design for Stroke Rehabilitation. In: Rau, PL. (eds) Cross-Cultural Design. Applications in Cultural Heritage, Creativity and Social Development. CCD 2018. Lecture Notes in Computer Science(), vol 10912. Springer, Cham. https://doi.org/10.1007/978-3-319-92252-2_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-92252-2_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-92251-5
Online ISBN: 978-3-319-92252-2
eBook Packages: Computer ScienceComputer Science (R0)