
Abstract
Purpose We performed a study to determine the effects and influencing factors of a hypertension health management (HHM) program in elderly residents of Chengguan District in Lanzhou City, Gansu Province, China.
Methods Two hundred seventy-nine elderly residents (aged over 60 years) in Chengguan District were recruited to participate in a virtual nursing home for this study in January 2017. During the following ten months, HHM, including periodic monitoring of blood pressure (BP), health education, and social support, was performed by 11 health management specialists (all with nurse qualification certificates) from Lily Eldercare Center. The BP of all 279 participants was measured every week. Information regarding BP and other records was integrated into the Lily Health Eldercare Cloud Platform, which was supported by an information technology (IT) foundation. The primary outcome measure was BP control at levels lower than 140/90 mmHg. BP levels before and after the intervention were compared.
Results after ten months of intervention, BP was significantly decreased (P < 0.05). Systolic blood pressure (SBP) was reduced by 8.98 ± 15.55 mmHg (1 mmHg = 0.133 kPa), and diastolic blood pressure (DBP) was reduced by 4.86 ± 11.17 mmHg. A significant difference was observed between the proportion of BP control before and after health management (2.58% vs 77.57%, 2 = 23.64, P < 0.05). In addition, the changes in BP values were associated with alcohol consumption, dietary preference, and life satisfaction.
Conclusions At-home healthcare management with BP monitoring provided by Lily Eldercare Center significantly improved BP control in the elderly community in an undeveloped area of China.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
As the leading cause of death globally, noncommunicable diseases(NCDs) were responsible for 38 million (68%) of the world’s 56 million deaths in 2012 [1]. Nearly 80% of these deaths occurred in low- and middle-income countries (LMICs) [2]. Hypertension, defined as a blood pressure (BP) measurement greater than 140/90 mmHg, is the most prevalent modifiable risk factor for cardiovascular disease (CVD). Medical treatment of hypertension reduces cardiovascular morbidity and mortality in the elderly, and all guidelines recommend lifestyle modifications and medical treatment for elderly patients whose BP exceeds prescribed thresholds and who are at moderate or high risk for CVD [3]. Since early detection of hypertension contributes to the prevention and reduction of the onset of CVD [4], determining hypertension risk factors and establishing a real-time, accurate and coordinated BP information network will facilitate the early prevention and effective management of hypertension and improve individual health conditions.
The aging of the population means that the proportion of elderly (≥65 years) individuals is growing rapidly worldwide. The attendant increase in the prevalence of hypertension and other comorbidities is a major concern as the population ages [5]. Although many aspects of hypertension prevention, diagnosis and treatment are shared between young and older people, some issues are unique to the elderly and require attention while caring for the elderly. Establishing community-based elderly care service systems has become one of the major strategies for addressing aging issues. Iranian scientists conducted a comprehensive study of trends in the prevalence, awareness, treatment and control of hypertension. They evaluated the effect of an expanded chronic care model (ECCM) on hypertension control, treatment and self-care [6]. The current Chinese community-based elderly care service system is not integrated, which causes serious fragmentation problems. To address this critical issue, the civic affairs bureau of Chengguan District of Lanzhou City launched a “medical and health integration” initiative that includes an integrated hypertension care model (IHCM) for disadvantaged elderly individuals. The IHCM utilizes the Lily Health Eldercare Cloud Platform information technology (IT) capacity to integrate the elderly, their families, primary care physicians in their community and home-care providers to regularly manage hypertension in the elderly. We formed a multi-disciplinary research team with strong scientific research and engineering expertise and extensive collaboration experience to assess the performance of the IHCM. However, limited evidence exists regarding whether the IHCM is effective, which is a major and vital part of the network.
Therefore, we performed this study to determine the effects and influencing factors of home healthcare management via IT on BP control for the elderly in a low-resource setting in China.
2 Methods
2.1 Study Design
We explored the effects and relevant factors of home-care hypertension management on BP control for elderly individuals in Lanzhou City, Gansu Province, which is an underdeveloped area of China. In January 2017, 279 men and women older than 60 years who were low-income permanent residents and had no major disability were identified through official residential records and invited to participate in a virtual nursing home (i.e., a home-care model) organized by the local civic affairs bureau. At the baseline survey, detailed socio-demographic, lifestyle and medical data were collected using a laptop-based questionnaire. In the following ten months, hypertension health management (HHM), including periodic BP monitoring, health education, and social support, was conducted by 11 health management specialists (all with nurse qualification certificates) from the Lily Eldercare Center.
The BP of all 279 participants was measured every week. Two measurements were obtained after participants had remained at rest in a seated position for at least five minutes. If the difference between the two measurements was >10 mmHg for the systolic blood pressure (SBP), a third measurement was made, and the last two measurements were recorded. The mean of the two recorded values was used for analysis. Hypertension was defined as SBP ≥140 mmHg, diastolic blood pressure (DBP) ≥90 mmHg, and/or self-reported treatment of hypertension with antihypertensive medication in the last 2 weeks, according to the Chinese Guidelines on Prevention and Control of Hypertension [7] and the Sixth Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure guidelines [8]. All the records were summarized on the Lily Eldercare Cloud Platform. Control of hypertension was defined as an average SBP less than 140 mmHg and an average DBP less than 90 mmHg. The primary outcome measure was control of BP to levels lower than 140/90 mmHg, and each patient’s BP was compared between before and after the HHM intervention. Questionnaires about lifestyle and a range of physical measurements, including height, weight and BP, were administered at the end of the study. The smoking or drinking habits were recorded according to the patient’s self-report. Smoking was graded as “never”, “light” (≤10 cigarettes/day) and “heavy” (>10 cigarettes/day), in which the latter two were labeled “yes”. Drinking was graded as “never”, “infrequent” (≤twice/week, >1 glass of wine or equivalent each time) and “frequent” (>twice/week), in which the latter two were labeled “yes”. BMI was divided into different groups according to the “Criteria of Weight for Adults” released by the National Health and Family Planning Commission (NHFPC) of China in 2013, which defined four groups according to the following BMI (kg/m2) values: underweight (<18.5), healthy (≥18.5 to <24), overweight (≥24 to <28), and obese (≥28) [9].
2.2 Statistical Analysis
Statistical analysis was performed using the SAS version 9.1.3 service pack 4 (SAS Institute Inc., Cary, NC, USA). Descriptive statistics were used to summarize participant characteristics. Qualitative variables are presented as frequency distributions and percentages, and quantitative variables are summarized as the mean with the standard deviation (SD). The mean SBP and DBP were calculated for each calendar week of the 10-month study period. To analyze the differences between the baseline and the follow-up measurements, t tests and ANOVA were performed for continuous variables, and the χ2 test was performed for categorical variables. All P values represent two-sided tests. For all analyses, a P-value of less than 0.05 was considered statistically significant.
2.3 Ethical Considerations
Ethics approval was obtained from the Ethics Review Committee of the Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China (X170315009). All study participants provided written informed consent.
3 Results
The main characteristics of the study participants are shown in Table 1. More than half the elderly participants were female (68.1%). The overall mean age was 76.83 ± 6.95 years. A total of 28.7% of the participants were overweight, and 5.0% were obese. The monthly mean family income of the elderly participants in the virtual nursing home was only 780 yuan, and the vast majority (67.00%) had only a primary school education level or below, indicating very low education and income levels.
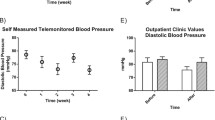
After ten months of HHM, BP values were significantly decreased (P < 0.05). The SBP was decreased by 8.98 ± 15.55 mmHg (1 mmHg = 0.133 kPa), and the DBP was decreased by 4.86 ± 11.17 mmHg. Figures 1 and 2 show the time trends in SBP and DPB, respectively, during the study period.

Trend of systolic blood pressure (SBP) values after health management.

Diastolic blood pressure (DBP) values after health management.
Approximately half (55.6%) of the elderly subjects had uncontrolled high blood pressure (HBP) at the beginning of the study. A significant difference was observed in the proportion of HBP control between baseline and after HHM (38.4%, 2 = 23.64, P < 0.05). The BP control rate was 77.57% after the intervention.
The changes in BP values were associated with alcohol consumption, dietary preference, and life satisfaction; control of SBP and DBP was significantly improved in the elderly with higher life satisfaction (P = 0.01 and 0.002, respectively), and DBP control was significantly improved in the elderly with no alcohol consumption (P = 0.01) or a light diet (P = 0.04). However, no significant association was detected for smoking, physical exercise, or social relationships, and the results remained unchanged in the subgroup analyses by sex, age and BMI (Table 2).
4 Discussion
Rising BP is an important and common modifiable risk factor for CVD and related diseases, including stroke and chronic kidney disease [10]. Although evidence suggests that lowering BP substantially reduces this risk, strategies to achieve sustained BP control are complex, especially in the elderly. These strategies include modifying a range of behaviors related to health, including attending clinic appointments, taking medication regularly and continuing treatment [11, 12]. In addition to treating hypertension, the physician must treat other modifiable cardiovascular risk factors in patients with or without diabetes mellitus or chronic kidney disease to reduce cardiovascular events and mortality. Moreover, a particular form of hypertension, most prevalent among the elderly, is isolated systolic hypertension (ISH). Hypertension in the elderly should be treated, especially when the SBP exceeds 160 mmHg. Lowering the SBP to less than 150 mmHg confers substantial cardiovascular protection [13].
4.1 Main Findings
The ten-month HHM intervention using IT (with a 0% rate of loss to follow-up) may have been responsible for the downward trend of BP values. The association was stronger in older people with a lighter diet or higher life satisfaction.
An upward trend was observed in SBP (Fig. 1) and DBP (Fig. 2) during the last few weeks, probably due to the decrease in temperature and changes in daily living habitats caused by the seasonal shift. BP is strongly inversely associated with outdoor temperature in Chinese adults across a range of climatic conditions, although access to home central heating appears to remove much of the association during the winter months. Seasonal variation in BP should be considered in the clinical management of hypertension [14]. People perform less physical activity and eat more during colder months; for example, they have increased salt intake (such as from pickled vegetables) and reduced fluid excretion during the cold season, which may be responsible for increases in BP.
The adoption of the Lily Health Eldercare Cloud Platform enabled us to study dynamic changes in the health status of the elderly, especially BP, by conjoined analysis of behavioral data and health indicators drawn from multidimensional data sources. Our study on HHM via IT will help transmit all related data regarding the elderly and share information electronically among primary care physicians, family members and professional caregivers. This will contribute to the further improvement of the elder-oriented integrated hypertension care model.
4.2 Strengths and Limitations
Despite these strengths, there are several limitations of our current study. First, given the confounding factors, a control group should be included to increase the statistical power. Second, the follow-up time should be increased. Lastly, additional participants need to be recruited in similar areas of China. Further good-quality studies are needed to validate our results.
4.3 Implications
This study provides a feasible, effective and integrated hypertension care model for establishing the IT-based Lily Health Eldercare Cloud Platform. It will play a key role in elderly health and research policy and provide a suitable model for implementing appropriate hypertension management measures at the provincial and national levels.
5 Conclusions
Our study provided empirical evidence regarding the effectiveness of home healthcare management for hypertension via IT. The intervention provided by the Lily Eldercare Center resulted in significant improvements in BP control in elderly individuals in a Chinese underdeveloped community, especially in non-drinkers, those with higher life satisfaction, and those with a light diet.
Abbreviations
- IHCM:
-
Integrated Hypertension Care Model
- HHM:
-
Hypertension Health Management
- IT:
-
Information Technology
- SBP:
-
Systolic Blood Pressure
- DBP:
-
Diastolic Blood Pressure
- BMI:
-
Body Mass Index
References
World Health Organization.: GLOBAL STATUS REPORT on noncommunicable diseases (2014). ISBN: 978 92 4 156485 4. http://www.who.int/nmh/publications/ncd-status-report-2014/en/
World Health Organization.: Global status report on non-communicable diseases. 2010, Geneva: World Health Organization (2010)
Pimenta, E., Oparil, S.: Management of hypertension in the elderly. Nat. Rev. Cardiol. 9(5), 286–296 (2012). https://doi.org/10.1038/nrcardio.2012.27
Wang, A., An, N., Chen, G., Li, L., Alterovitz, G.: Predicting hypertension without measurement: a non-invasive, questionnaire-based approach. Expert Syst. Appl. 42(21), 7601–7609 (2015). https://doi.org/10.1016/j.eswa.2015.06.012
Turgut, F., Yesil, Y., Balogun, R.A., Abdel-Rahman, E.M.: Hypertension in the elderly: unique challenges and management. Clin. Geriatr. Med. 29(3), 593–609 (2013). https://doi.org/10.1016/j.cger.2013.05.002
Eghbali-Babadi, M., Khosravi, A., Feizi, A., Sarrafzadegan, N.: Design and implementation of a combined observational and interventional study: trends of prevalence, awareness, treatment and control hypertension and the effect of expanded chronic care model on control, treatment and self-care. ARYA Atheroscler. 13(5), 211–220 (2017)
Committee for Revision of Chinese Guidelines for Prevention and Treatment of Patients with Hypertension. Chinese guidelines for prevention and treatment of patients with hypertension. Chin. J. Hypertens. 134, 2–41 (2005). (in Chinese)
The sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Arch. Int. Med. 157, 2413–2446 (1997)
China NHaFPCotPsRo.: Criteria of weight for adults. File No WS/T 428–2013 (2013)
Lim, S.S., Vos, T., Flaxman, A.D., Danaei, G., Shibuya, K., Adair-Rohani, H., et al.: A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet 380(9859), 2224–2260 (2012)
Viswanathan, M., Golin, C.E., Jones, C.D., Ashok, M., Blalock, S.J., Wines, R.C.M., et al.: Interventions to improve adherence to self-administered medications for chronic diseases in the United States: a systematic review. Ann. Int. Med. 157(11), 785–795 (2012)
Gwadry-Sridhar, F.H., Manias, E., Lal, L., Salas, M., Hughes, D.A., Ratzki-Leewing, A., et al.: Impact of interventions on medication adherence and blood pressure control in patients with essential hypertension: a systematic review by the ISPOR medication adherence and persistence special interest group. Value Health 16(5), 863–871 (2013)
Piotrowicz, K., Kucharska, E., Skalska, A., Kwater, A., Bhagavatula, S., Gasowski, J.: Pharmacological management of hypertension in the elderly–certitudes and controversies. Curr. Pharm. Des. 20(38), 5963–5967 (2014)
Lewington, S., Li, L., Sherliker, P., Guo, Y., Millwood, I., Bian, Z., Whitlock, G., Yang, L., Collins, R., Chen, J., Wu, X., Wang, S., Hu, Y., Jiang, L., Yang, L., Lacey, B., Peto, R., Chen, Z.: China Kadoorie Biobank study collaboration. Seasonal variation in blood pressure and its relationship with outdoor temperature in 10 diverse regions of China: the China Kadoorie Biobank. J. Hypertens. 30(7), 1383–1391 (2012)
Acknowledgments
We thank Pingyue Jin, School of Public Health, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China for assisting with the design, planning, organization and performance of the study.
This study was supported by a grant from the National Natural Science Foundation of China (grant number: 71661167004).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Ethics declarations
No conflict of interest.
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Zhu, Z., Li, J., Jie, Y., Liu, Y. (2018). The Effect of Hypertension Health Management (HHM) Using IT for the Elderly: A Case Study in an Underdeveloped Area of China. In: Zhou, J., Salvendy, G. (eds) Human Aspects of IT for the Aged Population. Applications in Health, Assistance, and Entertainment. ITAP 2018. Lecture Notes in Computer Science(), vol 10927. Springer, Cham. https://doi.org/10.1007/978-3-319-92037-5_15
Download citation
DOI: https://doi.org/10.1007/978-3-319-92037-5_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-92036-8
Online ISBN: 978-3-319-92037-5
eBook Packages: Computer ScienceComputer Science (R0)