
Abstract
Advancements integrating computers and mobile devices with physiological sensors may increase individual opportunities for stress awareness. Conversely, computers and mobile devices, remain sources of stress, particularly in student populations. Use of these devices can have a negative effect on breathing patterns, which can, in turn, cause or exacerbate stress. This study explores whether breath counting and abdominal breathing activities may be useful to help manage stress induced by computer use. Nine male senior computer science students completed a repeated-measures experimental sequence which included Stroop color-word tasks followed by periods of sitting quietly or periods of conducting one of three breathing activities. The study highlights the possibility that college students may be able to use five-minute breathing activities to effect physiological responses. The study advocates the continued examination of these breathing activity effects on skin conductance (SC), heart rate (HR) and breath ratio. It also suggests that there may be similarity in overall effect on respiration rate (RR) for the three breathing activities used in this study. Future studies with larger sample sizes and demographic diversity may provide better fidelity on suggested relationships. This study expands upon a previously published work in progress [1].
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
- Breath counting
- Abdominal breathing
- Stress
- Stroop color-word task
- Students
- Physiological response
- Meditation
- Kruskal-Wallis H test
1 Introduction
Portable and wearable sensor technology is becoming ubiquitous and enables one to potentially gain greater visibility of one’s own physiological measures [2,3,4,5,6,7,8,9,10]. Integration of physiological sensors with computers, mobile devices and other platforms will continue to expand the possibilities for augmented cognition related to stress monitoring, especially through the use of sensors to monitor skin conductance (SC), heart rate (HR) and respiratory rate (RR) [5, 7, 10,11,12,13,14,15,16,17,18]. As this integration continues, individual users will have enhanced capacity, to monitor, record, and become more aware of their own physiological signals and use this information to make decisions about their health, especially stress management.
2 Theoretical Background
2.1 Students, Stress and Technology
College and university students generally experience high levels of stress [19,20,21,22,23]. Some of this stress may be caused, or intensified by using computers and electronic devices, which in some cases can cause superficial or irregular breathing [24,25,26]. Computers and mobile devices could eventually be used to help remedy this phenomenon, particularly if used to build awareness of breathing and variations in physiological signals, and to enable individuals to make behavioral changes, which is consistent with approaches used in breath-related biofeedback for stress management [27,28,29,30,31,32,33,34].
2.2 Breathing and Stress Management
As noted previously [1], science has thoroughly documented the complex physiological relationship between breathing and stress [35,36,37,38], which is consistent with longstanding knowledge applied in a variety of meditative and other traditions [39,40,41,42]. Since breathing is both reflexive and voluntary, it has the potential to both cause and help manage stress. Breathing activities that have been used with children and students include breath counting [43, 44] and abdominal breathing [19, 32, 45,46,47].
One aspect of using breathing activities for stress management involves enabling individuals do develop an awareness of their own breathing. Breath awareness is used extensively in a variety of meditative practices, including meditative practices applied for stress management [43, 48,49,50,51,52].
2.3 Physiological Measures
From an augmented cognition perspective, the following physiological measures may be particularly useful for monitoring stress levels because sensors that measure these signals are becoming more integrated with computers and mobile devices.
Skin Conductance (SC).
One measure of electrodermal activity (EDA), SC is the change in electrical conduciveness of the surface of the skin caused by eccrine sweat glands secretions. It is measured in microsiemens (μS) and increases in SC are generally related to increased physiological arousal [38, 53, 54].
Heart Rate (HR).
HR is derived from electrocardiogram (ECG) measures by converting the heart period (inter-beat interval - IBI) into beats per minute to quantify cardiac activity. (It can also be determined by counting heart beats.) HR measures are converted to average beats per minute (BPM) and increases in HR can indicate physiological arousal [38, 53, 54].
Respiratory Rate (RR).
RR is the quantification of breathing by counting respiratory cycles. One cycle is comprised of one inhalation and one exhalation [38, 54]. It is measured in average breaths per minute (BrPMFootnote 1).
Breath Ratio.
Breath ratio is a calculated value derived by dividing the standard deviation of the voltage obtained from an abdominal belt sensor by the standard deviation of the voltage obtained from a thoracic belt sensor. Values less than one indicate a thoracic breathing style and values greater than one indicate an abdominal breathing style [55].
2.4 Research Questions
Based on the aforementioned information, the following research questions have emerged as the basis of this study:
-
RQ1:
Can college students use a five-minute breathing activity to regulate physiological responses caused by computer use?
-
RQ2:
Are there significant differences in effect on physiological responses between quiet sitting and the breathing activities of breath counting, abdominal breathing and combined breath counting and abdominal breathing?
2.5 Hypotheses
The research questions are parsed into hypotheses related to specific breathing activities and physiological measures, which will guide data collection and analysis. Since the computer-based task is designed to elicit physiological response, any change in physiological response would be demonstrated by comparing the activity periods immediately following each computer-based task.
-
H1:
Participants can use a five-minute breath counting activity to regulate physiological responses caused by computer use.
-
H1.1:
The breath counting activity will cause a change in participant SC when compared to the quiet sitting activity.
-
H1.2:
The breath counting activity will cause a change in participant HR when compared to the quiet sitting activity.
-
H1.3:
The breath counting activity will cause a change in participant RR when compared to the quiet sitting activity.
-
H1.4:
The breath counting activity will cause a change in participant breath ratio when compared to the quiet sitting activity.
-
H1.1:
-
H2:
Participants can use a five-minute abdominal breathing activity to regulate physiological responses caused by computer use.
-
H2.1:
The abdominal breathing activity will cause a change in participant SC when compared to the quiet sitting activity.
-
H2.2:
The abdominal breathing activity will cause a change in participant HR when compared to the quiet sitting activity.
-
H2.3:
The abdominal breathing activity will cause a change in participant RR when compared to the quiet sitting activity.
-
H2.4:
The abdominal breathing activity will cause a change in participant breath ratio when compared to the quiet sitting activity.
-
H2.1:
-
H3:
Participants can use a five-minute combined breathing activity (breath counting and abdominal breathing) to regulate physiological responses caused by a computer use.
-
H3.1:
The combined breathing activity will cause a change in participant SC when compared to the quiet sitting activity.
-
H3.2:
The combined breathing activity will cause a change in participant HR when compared to the quiet sitting activity.
-
H3.3:
The combined breathing activity will cause a change in participant RR when compared to the quiet sitting activity.
-
H3.4:
The combined breathing activity will cause a change in participant breath ratio when compared to the quiet sitting activity.
-
H3.1:
Evidence for or against these hypotheses involves a statistically significant change in the mean physiological signal measure between the periods of quiet sitting and the breathing activity periods. If there is a change, it may indicate that the participant is able to use the breathing activity to regulate physiological response, which supports the hypotheses. If there is no change it may indicate that the participant is not able to use the breathing activity to regulate physiological response, or that the breathing activity had no effect - both of which do not support the hypotheses.
2.6 Stroop Effect
The Stroop Effect [56] describes interference that occurs when two inconsistent stimuli are simultaneously presented to an individual and the individual’s response to the designated stimulus is slower (in milliseconds) than when two stimuli are consistent.
Stroop color-word tasks present color words in font colors that match or do not match the color word. Participants are instructed to respond by identifying the font color, not the color-word. Stroop color-word tasks have been employed extensively to study stress and cognitive load [33, 34, 57,58,59,60,61,62,63,64]. As previously noted [1], Stroop tasks are effective laboratory stressors because practice effects only emerge after prolonged exposure [65] and because individual response to interference cannot be controlled [64].
3 Method
The purpose of this study is to investigate the efficacy of university student use of breath counting, abdominal breathing and combined breathing treatments to regulate physiological responses caused by a computer-based task. This study uses a repeated measures design to account for the range of participant physiological variation. Physiological responses were measured and recorded throughout each session across the experimental activity sequence.
3.1 Participants
Nine male university seniors were recruited from a summer computer science course. Participants age ranged from 20–24 years with the average age of 22 years. Participants received extra credit as compensation for their participation and all participants completed the experimental activity sequence. Each participant indicated he was in good health and had normal color vision.
3.2 Activity Sequence
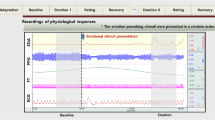
Figure 1 shows the experimental activity sequence. The researcher first recorded baseline physiological measures for each participant during a two and one-half minute period of no activity (Fig. 1, item 1). Next, participants practiced the Stroop color-word task [66] for two and one-half minutes (Fig. 1, item 2). All participants then completed a series of three – two and one-half computer-based Stroop color-word tasks, each immediately followed by five minutes of quiet sitting (Fig. 1, items 3–8b).

Experimental activity sequence with each, two and one-half minute period delineated. Letters a and b after numbers designate the first and second halves of five-minute activities.
After rehearsing a breathing activity that corresponded with their treatment group for two and one-half minutes (Fig. 1, item 9), participants subsequently completed another series of three – two and one-half minute Stroop tasks, each followed by five-minute periods of the breathing activity (Fig. 1, items 10–15b).
Stroop Color-Word Task.
This study uses a modified version of an existing computer-based Stroop color-word task [66] for the specific purpose of eliciting physiological responses. Participants were instructed to complete the task as quickly and accurately as they were able. Each participant completed a total of seven iterations (including a practice period – Fig. 1, items 2, 3, 5, 7, 10, 12 and 14).
In the task, the program displays color words in a font color that matches or does not match the color word. Only four colors are used: red, green, yellow and blue. Items are randomly displayed to participant, half having matching color word and font color and half not. Participants are instructed to respond by pressing the key on the computer keyboard that corresponds with the first letter of the font color (not the color word). The message “Correct. Press SPACE to continue” appears after correct responses. The message “INCORRECT. Don’t rush” is displayed for incorrect responses.
3.3 Treatments
The researcher used restricted random assignment, forcing equal sample sizes to place participants in one of three breathing activity conditions: (a) breath counting, (b) abdominal breathing and (c) combined - both breath counting and abdominal breathing. Each treatment group had three participants (Table 1).
Quiet Sitting.
Participants completed a total of three, five-minute quiet sitting tasks, (Fig. 1, items 4a–b, 6a–b, and 8a–b). For quiet sitting, participants were instructed to maintain a comfortable sitting position with their backs straight and refrain from talking.
Breath Counting.
The researcher provided participants in the breath counting treatment group a breath-counting worksheet with the following instructions and verbally reviewed the instructions with each participant:
-
1.
Sit up comfortably with your back straight and both feet on the floor.
-
2.
Breathe comfortably and focus your attention on your breathing.
-
3.
When the time starts, mark the worksheet with the next breath event that occurs: inhale start, inhale end, exhale start, exhale end.
-
4.
Continue to mark the worksheet with each subsequent breath event as it occurs: inhale start, inhale end, exhale start, exhale end.
-
5.
Continue to breathe comfortably.
Abdominal Breathing.
The researcher provided participants in the abdominal breathing treatment group a worksheet with the following instructions and verbally reviewed the instructions with each participant:
-
1.
Sit up comfortably with your back straight and both feet on the floor.
-
2.
Place your dominant hand on the center of your chest and your other hand on the center of your abdomen.
-
3.
Inhale slowly through your nose and permit your abdomen to expand as your diaphragm descends and your lungs fill; while at the same time keeping your chest and upper body as still as you can.
-
4.
Exhale slowly through your nose and permit your abdomen to reduce and move toward your spine as your diaphragm rises and your lungs empty; while at the same time keeping your chest and upper body as still as you can.
-
5.
Keep your eyes open and observe your abdomen as it moves.
-
6.
Focus your attention on the sensations of breathing and when you notice that your mind has wandered, bring your attention back to your breathing sensations.
-
7.
Continue to breathe slowly, deeply and comfortably.
Combined.
The researcher provided and verbally reviewed both instruction sets and worksheets to the participants. The participants completed the breath counting and abdominal breathing activities simultaneously with the following minor modification: participants used their dominant hand to mark the breath counting worksheet and placed the other hand on their abdomen.
Variables.
The independent variable for this study is the treatment group: (a) breath counting, (b) abdominal breathing and (c) combined. The dependent variables are (a) SC, (b) HR, (c) RR and (d) breath ratio.
SC was measured by placing two disposable sensors side-by-side on the medial side of the right foot along the plantar surface of the longitudinal arch [53]. HR was measured by placing one pre-gelled disposable sensor on each of the participants forearms inferior to the antecubital space [53]. RR was measured using two belt sensors: one placed around the middle of the participant’s abdomen and the other around the upper portion of the participant’s thorax [55].
3.4 Procedure
Lab Description.
The lab space is air conditioned and equipped with fluorescent lights and an acoustic tile drop ceiling. It contains two sections, the experimental workstation and the proctor workstation. The experimental workstation is comparable to a standard, 64-in. by 64-in. office cubicle, equipped with a small desk, computer workstation and static chair. The computer is equipped with a 20-in. monitor, standard keyboard and mouse. It is separated from the lab equipment and the proctor workstation by a 64-in. by 72-in. fabric covered partition. The proctor workstation has two displays and two sets of controls. One monitor, keyboard and mouse that mirrors and controls the participant’s experimental workstation and another monitor, keyboard and mouse to view and record the physiological signals.
Instrumentation.
The researcher used BIOPAC MP150 system to collect physiological data. Signals were recorded at 1000 Hz across four channels: channel one – EDA, channel two – electrocardiogram (ECG), channel three – abdominal breathing signal, channel four – thoracic breathing signal. All signals were recorded and prepared with BIOPAC AcqKnowledge software [67].
To determine HR, the researcher used the software to mark and count QRS peaks in the ECG channel. To calculate RR, the researcher used the software to mark the signals from the abdominal and thoracic RR channels at the beginning of each inspiration (inhale) and the beginning of each expiration (exhale). The researcher then used the software to count the markers and divided the count by two to derive one breath cycle (inhale, exhale) and then averaged the RR values from the abdominal and thoracic channels to establish composite RR values.
Experimental Procedure.
This experiment was approved by the university institutional review board (IRB). The experimental session lasted approximately 90 min for each participant. After providing informed consent, participants were seated in the experimental space at the computer workstation. The proctor then applied the sensors and instructed the participant to complete a computer-based demographic survey. Next, the participant started the activity sequence (Fig. 1). After the final breathing activity in the activity sequence, the participant completed a post-activity questionnaire, after which the proctor removed the sensors and debriefed the participant.
4 Results
Due to the small sample size (N = 9) and subsequent small group sizes (n = 3) the researcher applied the Kruskal-Wallis H test [68] (non-parametric ANOVA) in SPSS [69] to compare means of the physiological signals between treatment groups and between selected activities in the experimental protocol.
The researcher compared the physiological data from the following selected activities: (a) baseline, (b) Stroop task before breathing activity exposure, (c) first half of the quiet sitting activity, (d) second half of the quiet sitting activity, (e) Stroop task after breathing activity exposure, (f) first half of the breathing activity and (g) second half of the breathing activity.
4.1 Between Groups
The Kruskal-Wallis H test suggests statistically significant difference between the three groups for SC, HR, and breath ratio. For SC, χ2(2) = 16.19, p = 0.000 with a mean rank SC score of 4.00 for Group 1, 17.29 for Group 2 and 11.71 for Group 3. For HR, χ2(2) = 13.781, p = 0.001 with a mean HR score of 6.43 for Group 1, 18.00 for Group 2 and 8.57 for Group 3. For breath ratio, χ2(2) = 9.824, p = 0.010 with a mean breath ratio score of 5.43 for Group 1, 12.29 for Group 2 and 15.29 for Group 3. The test did not show a statistically significant difference between the three groups for respiration rate (RR). Table 2 displays these results.
Figure 2 displays box plots for the three physiological measures with statistically significant differences by group. Table 3 contains the corresponding box plot values for each measure by group. Breath ratio values correspond with a breathing style category. Values greater than one indicate a predominately abdominal breathing style. Values less than one indicate a predominately thoracic breathing style.

Plots of statistically significant differences in physiological measures between treatment groups: Group 1 – Breath Counting, Group 2 – Abdominal Breathing, Group 3 – Combined.
4.2 Across Activities
Graphing the mean values SC, HR, RR and breath ratio by group across the activities showed variations, but did not show any visibly consistent patterns for SC, HR and breath ratio. A consistent pattern did seem to emerge in the graph of mean RR for the three groups by activity period (Fig. 3).

Mean respiratory rate (RR) by activity
The Kruskal-Wallis H test suggests a statistically significant difference (Fig. 4) between the selected seven activities and RR, χ2(6) = 16.357, p = 0.012 with a mean rank RR score of (a) 8.67 for baseline, (b) 19.33 for the Stroop activities before exposure to the breathing activity (Stroop 1), (c) 12.17 for the first half of the quiet sitting activities (QSa), (d) 11.67 for the second half of the quiet sitting activities (QSb), (e) 17.00 for the Stroop activities after exposure to the breathing activity (Stroop 2), (f) 4.83 for the first half of the breathing activities (BAa) and (g) 3.33 for the second half of the breathing activities (BAb). Figure 4 shows the box plot of RR values for the seven selected activities and Table 4 contains the corresponding RR box plot values by activity. The Kruskal-Wallis H test did not show any statistically significant difference between the seven selected activities and SC, HR, and breath ratio.

Plots of RR measures across selected activities: baseline measure, Stroop 1 – pre-treatment Stroop tasks, QSa – first half quiet sitting periods, QSb – second half quiet sitting periods, Stroop 2 – post treatment Stroop tasks, BAa -first half breathing activities, BAb -second half breathing activities
5 Discussion
Small sample size precludes any definitive conclusions regarding the results of this study. The results may, however indicate potential relationships that are worth examining in future studies with more participants and with a greater range of participant demographic diversity.
The statistically significant difference between the mean physiological measures of SC, HR and breath ratio, (Fig. 2, Table 3) may lend evidence supporting the hypotheses specific to those particular measures when comparing the three treatment groups. It is also possible that the differences between the mean values was due to physical and physiological differences between individual participants, so further study with more participants has the potential to reveal evidence related to any individual differences.
5.1 Skin Conductance (SC) Between Groups
The statistically significant difference in mean SC between groups may be evidence which supports the hypotheses that the breathing activities for the treatment groups cause a change in SC (H1.1, H2.1 and H3.1). Participants in the breath counting group (group 1) showed a substantially lower ranked mean than the other two treatment groups (abdominal breathing - group 2, and combined - group 3). This could be attributed to individual differences or it is possible that the treatments were responsible for these results.
The abdominal breathing group showed the highest ranked mean score when compared to the other two groups, which could indicate that the abdominal breathing activity caused an increase in SC. Since abdominal breathing was also included in the combined breathing activity group, this could explain why the combined treatment group had a ranked mean score between the breath counting and abdominal breathing treatment groups.
5.2 Heart Rate (HR) Between Groups
The statistically significant difference in mean HR between groups may be evidence which supports the hypotheses that the breathing activities for the treatment groups cause a change in HR (H1.2, H2.2 and H3.2). The abdominal breathing group displayed the highest ranked mean score when compared with the other two groups. This could be due to individual differences or it may indicate that the abdominal breathing activity can cause a general increase in heart rate.
5.3 Breath Ratio Between Groups
The statistically significant difference in mean breath ratio values between groups may be evidence which supports the hypotheses that the breathing activities for the treatment groups cause a change in breath ratio (H1.4, H2.4 and H3.4). Because breath ratio values greater than one indicate a predominately abdominal breathing style and values less than one indicate a predominately thoracic breathing style, the fact that the abdominal breathing group displays the greatest range of ratio scores when compared with the other two groups is consistent with the experimental manipulation.
5.4 Respiratory Rate (RR) Between Groups
The absence of a statistically significant difference between the mean RR may mean that the breathing activities had no effect on RR when comparing treatment groups or that the treatments all had similar effects on RR. The possibility of similar effects for all three treatments may be supported by the similar pattern in mean values by activity (Fig. 3) and the statistically significant difference for RR across activities (Fig. 4).
Since the Stroop, quiet sitting and breathing activities all involve minimal levels of physical activity, it is possible that RR may not be a salient indicator of stress for individual participants for tasks performed while seated in front of a computer. It is also possible that individual differences and small sample size masked any statistically significant RR variation.
5.5 Respiratory Rate (RR) Across Selected Activities
The presence of a statistically significant difference in RR across the selected activities (Fig. 4, Table 4) may show a generally positive and similar effect of the breathing activities in reducing RR when comparing the baseline, Stroop, and quiet sitting composite activity periods. Both Stroop composite activity periods showed the two highest ranked values when compared to other activities, which is consistent with the used of the computer-based Stroop color-word task as a laboratory stressor. The two segments of the breathing activity period composites had the two lowest ranked values and were below baseline measures, which may show that the breath activities have a greater effect on RR when compared to the quiet sitting task. The composite baseline and the two segments of the sitting quietly composite activity periods have similar rankings falling between the Stroop activities and the breathing activities. This may show a near equivalence between baseline measure and quiet sitting, which can be expected due to activity similarity.
6 Potential Implications
Towards gathering evidence related to the first research question, it does appear that some college students may be able to use breathing activities to mitigate changes in RR due to computer use. At this time, there is no evidence in this study to indicate that college students are able to use the breathing activities to mitigate changes in SC, HR and breath ratio measures due to computer use but these potential relationships might still be considered in future studies.
Towards gathering evidence related to the second research question, it appears that there could be significant differences between SC, HR and breath ration values for the three treatment groups. It is worth noting that the abdominal breathing activity appeared to be related to an increase of both mean SC and HR values. Typically increases in SC and HR values are generally consistent with physiological arousal [53], but it is also possible that the abdominal breathing activity was physically stimulating when compared to the overall sedentary nature of the experimental protocol, or that individual differences in physiological response could explain these differences.
This pilot study highlights potential relationships that may exist between breathing activities and participant SC, HR and breath ratio. It also may show potential relationships between RR and seven of the activities selected from the experimental activity sequence. In addition to examining these potential relationships, future studies should take into account other variables such as heart rate variability (HRV), individual stress levels and participant prior experience with breathing activities. Additionally, since physiological measures within an individual are not independent, multilevel modeling or hierarchical linear modeling statistical analysis approaches may be more appropriate for analyzing data from larger population samples.
Notes
- 1.
The acronym BPM appears in medical and scientific literature to refer to both breaths per minute for RR and beats per minute for HR. This study uses the acronym BrPM to clearly distinguish breaths per minute from beats per minute (BPM).
References
Brumback, H.K.: Investigation of breath counting, abdominal breathing and physiological responses in relation to cognitive load. In: Schmorrow, Dylan D., Fidopiastis, Cali M. (eds.) AC 2017. LNCS (LNAI), vol. 10284, pp. 275–286. Springer, Cham (2017). https://doi.org/10.1007/978-3-319-58628-1_22
Abbott, D., Shirali, Y., Haws, J.K., Lack, C.W.: Biobehavioral assessment of the anxiety disorders: current progress and future directions. World J. Psychiatry. 7, 133–147 (2017). https://doi.org/10.5498/wjp.v7.i3.133
Treskes, R.W., van der Velde, E.T., Barendse, R., Bruining, N.: Mobile health in cardiology: a review of currently available medical apps and equipment for remote monitoring. Expert Rev. Med. Devices 13, 823–830 (2016). https://doi.org/10.1080/17434440.2016.1218277
Torrado, J.C., Gomez, J., Montoro, G.: Emotional self-regulation of individuals with autism spectrum disorders: Smartwatches for monitoring and interaction. Sensors 17, 1–29 (2017). https://doi.org/10.3390/s17061359
Ertin, E., Stohs, N., Kumar, S., Raij, A., al’Absi, M., Shah, S.: AutoSense: unobtrusively wearable sensor suite for inferring the onset, causality, and consequences of stress in the field. In: Proceedings of the 9th ACM Conference on Embedded Networked Sensor Systems, pp. 274–287. ACM, New York (2011). https://doi.org/10.1145/2070942.2070970
Kennedy, A.P., Epstein, D.H., Jobes, M.L., Agage, D., Tyburski, M., Phillips, K.A., Ali, A.A., Bari, R., Hossain, S.M., Hovsepian, K., Rahman, M.M., Ertin, E., Kumar, S., Preston, K.L.: Continuous in-the-field measurement of heart rate: Correlates of drug use, craving, stress, and mood in polydrug users. Drug Alcohol Depend. 151, 159–166 (2015). https://doi.org/10.1016/j.drugalcdep.2015.03.024
Picard, R.W.: Automating the recognition of stress and emotion: from lab to real-world impact. Multimed. IEEE. 23, 3–7 (2016). https://doi.org/10.1109/MMUL.2016.38
Ferreira, E., Ferreira, D., Kim, S., Siirtola, P., Roning, J., Forlizzi, J.F., Dey, A.K.: Assessing real-time cognitive load based on psycho-physiological measures for younger and older adults. In: 2014 IEEE Symposium on Computational Intelligence, Cognitive Algorithms, Mind, and Brain (CCMB), pp. 39–48. IEEE (2014). https://doi.org/10.1109/CCMB.2014.7020692
Bin, M.S., Khalifa, O.O., Saeed, R.A.: Real-time personalized stress detection from physiological signals. In: 2015 International Conference on Computing, Control, Networking, Electronics and Embedded Systems Engineering (ICCNEEE), pp. 352–356 (2015). https://doi.org/10.1109/ICCNEEE.2015.7381390
Ming-Zher Poh, N.C., Swenson, R.W., Picard, R.W.: A wearable sensor for unobtrusive, long-term assessment of electrodermal activity. IEEE Trans. Biomed. Eng. 57, 1243–1252 (2010). https://doi.org/10.1109/TBME.2009.2038487
Gravenhorst, F., Muaremi, A., Tröster, G., Arnrich, B., Gruenerbl, A.: Towards a mobile galvanic skin response measurement system for mentally disordered patients. In: Proceedings of the 8th International Conference on Body Area Networks, pp. 432–435. ICST (Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering), ICST, Brussels (2013). https://doi.org/10.4108/icst.bodynets.2013.253684
Kappeler-Setz, C., Gravenhorst, F., Schumm, J., Arnrich, B., Tröster, G.: Towards long term monitoring of electrodermal activity in daily life. Pers. Ubiquit. Comput. 17, 261–271 (2011). https://doi.org/10.1007/s00779-011-0463-4
Al-Khalidi, F.Q., Saatchi, R., Burke, D., Elphick, H., Tan, S.: Respiration rate monitoring methods: a review. Pediatr. Pulmonol. 46, 523–529 (2011). https://doi.org/10.1002/ppul.21416
Hernandez, J., Morris, R.R., Picard, R.W.: Call center stress recognition with person-specific models. In: D’Mello, S., Graesser, A., Schuller, B., Martin, J.-C. (eds.) ACII 2011. LNCS, vol. 6974, pp. 125–134. Springer, Heidelberg (2011). https://doi.org/10.1007/978-3-642-24600-5_16
Muaremi, A., Arnrich, B., Tröster, G.: Towards measuring stress with smartphones and wearable devices during workday and sleep. BioNanoScience 3, 172–183 (2013). https://doi.org/10.1007/s12668-013-0089-2
Picard, R.W., Healey, J.: Affective wearables. Pers. Technol. 1, 231–240 (1997). https://doi.org/10.1007/BF01682026
Healey, J.A., Picard, R.W.: Detecting stress during real-world driving tasks using physiological sensors. IEEE Trans. Intell. Transp. Syst. 6, 156–166 (2005). https://doi.org/10.1109/TITS.2005.848368
Zhai, J., Barreto, A.: Stress detection in computer users based on digital signal processing of noninvasive physiological variables. In: Conference Proceedings: Annual International Conference of the IEEE Engineering in Medicine and Biology Society, pp. 1355–1358 (2006). https://doi.org/10.1109/IEMBS.2006.259421
Paul, G., Elam, B., Verhulst, S.: A longitudinal study of students’ perceptions of using deep breathing meditation to reduce testing stresses. Teach. Learn. Med. 19, 287–292 (2007). https://doi.org/10.1080/10401330701366754
American College of Health Association: American college health association-national college health assessment II: Reference group executive summary. American College of Health Association, Hanover (2017). http://www.acha-ncha.org/docs/NCHA-II_SPRING_2017_REFERENCE_GROUP_EXECUTIVE_SUMMARY.pdf
Feldt, R.C.: Development of a brief measure of college stress: the college student stress scale. Psychol. Rep. 102, 855–860 (2008). https://doi.org/10.2466/pr0.102.3.855-860
Stallman, H.M., Hurst, C.P.: The university stress scale: measuring domains and extent of stress in university students. Aust. Psychol. 51, 128–134 (2016). https://doi.org/10.1111/ap.12127
Bamber, M.D., Schneider, J.K.: Mindfulness-based meditation to decrease stress and anxiety in college students: a narrative synthesis of the research. Educ. Res. Rev. 18, 1–32 (2016). https://doi.org/10.1016/j.edurev.2015.12.004
Lin, I.-M., Peper, E.: Psychophysiological patterns during cell phone text messaging: a preliminary study. Appl. Psychophysiol. Biofeedback. 34, 53–57 (2009). https://doi.org/10.1007/s10484-009-9078-1
Peper, E., Harvey, R., Tylova, H.: Stress protocol for assessing computer-related disorders. Biofeedback 34, 57–62 (2006)
Rosen, L., Carrier, L.M., Miller, A., Rokkum, J., Ruiz, A.: Sleeping with technology: Cognitive, affective, and technology usage predictors of sleep problems among college students. Sleep Health 2, 49–56 (2016). https://doi.org/10.1016/j.sleh.2015.11.003
Edwards, L.: Combining biofeedback and mindfulness in education. Biofeedback 44, 126–129 (2016). https://doi.org/10.5298/1081-5937-44.3.01
Fehring, R.J.: Effects of biofeedback-aided relaxation on the psychological stress symptoms of college students. Nurs. Res. 32, 362–366 (1983)
Briz-Ponce, L., Juanes-Méndez, J.A., García-Peñalvo, F.J. (eds.): Handbook of research on mobile devices and applications in higher education settings. IGI Global, Hershey (2016)
Moss, D.: The house is crashing down on me: integrating mindfulness, breath training, and heart rate variability biofeedback for an anxiety disorder in a 71-year-old caregiver. Biofeedback 44, 160–167 (2016). https://doi.org/10.5298/1081-5937-44.3.02
Wang, S.-Z., Li, S., Xu, X.-Y., Lin, G.-P., Shao, L., Zhao, Y., Wang, T.H.: Effect of slow abdominal breathing combined with biofeedback on blood pressure and heart rate variability in prehypertension. J. Altern. Complement. Med. 16, 1039–1045 (2010). https://doi.org/10.1089/acm.2009.0577
Peper, E., Miceli, B., Harvey, R.: Educational model for self-healing: eliminating a chronic migraine with electromyography, autogenic training, posture, and mindfulness. Biofeedback 44, 130–137 (2016). https://doi.org/10.5298/1081-5937-44.3.03
Prinsloo, G.E., Derman, W.E., Lambert, M.I., Rauch, H.G.L.: The effect of a single session of short duration biofeedback-induced deep breathing on measures of heart rate variability during laboratory-induced cognitive stress: a pilot study. Appl. Psychophysiol. Biofeedback 38, 81–90 (2013). https://doi.org/10.1007/s10484-013-9210-0
Prinsloo, G.E., Rauch, H.G.L., Lambert, M.I., Muench, F., Noakes, T.D., Derman, W.E.: The effect of short duration heart rate variability (HRV) biofeedback on cognitive performance during laboratory induced cognitive stress. Appl. Cogn. Psychol. 25, 792–801 (2011). https://doi.org/10.1002/acp.1750
Fried, R.: The Psychology and Physiology of Breathing: In Behavioral Medicine, Clinical Psychology, and Psychiatry. Springer, New York (1993). https://doi.org/10.1007/978-1-4899-1239-8
Timmons, B.H., Ley, R. (eds.): Behavioral and Psychological Approaches to Breathing Disorders. Plenum Press, New York (1994)
Chaitow, L., Gilbert, C., Bradley, D. (eds.): Recognizing and Treating Breathing Disorders: A Multidisciplinary Approach. Churchill Livingstone Elsevier (2014)
Cacioppo, J.T., Tassinary, L.G., Berntson, G.G. (eds.): Handbook of Psychophysiology. Cambridge University Press, Cambridge (2017)
Bhikkhu, Ā. (ed.): Mahāsatipaṭṭhānasuttaṁ (DN 22): The long discourse about the ways of attending to mindfulness (2011). http://www.ancient-buddhist-texts.net/Texts-and-Translations/Satipatthana/Satipatthana.pdf
Ali-Shah, O.: The Rules or Secrets of the Naqshbandi Order. Tractus Books, Reno (1998)
Eifring, H. (ed.): Meditation in Judaism, Christianity and Islam: Cultural Histories. Bloomsbury Academic, New York (2013)
Therā, N.M.: Satipaṭṭhāna sutta [MN 10: The Discourse on the Establishing of Mindfulness]. In: The Buddha and His Teachings. Buddhadhamma Foundation (1980). http://www.bps.lk/olib/bp/bp102s.pdf
Britton, W.B., Lepp, N.E., Niles, H.F., Rocha, T., Fisher, N., Gold, J.: A randomized controlled pilot trial of classroom-based mindfulness meditation compared to an active control condition in 6th grade children. J. Sch. Psychol. 52, 263–278 (2014). https://doi.org/10.1016/j.jsp.2014.03.002
Hooker, K.E., Fodor, I.E.: Teaching mindfulness to children. Gestalt Rev. 12, 75–91 (2008)
Sellakumar, G.K.: Effect of slow-deep breathing exercise to reduce anxiety among adolescent school students in a selected higher secondary school in Coimbatore. India. J. Psychol. Educ. Res. 23, 54–72 (2015)
Terai, K., Shimo, T., Umezawa, A.: Slow diaphragmatic breathing as a relaxation skill for elementary school children: a psychophysiological assessment. Int. J. Psychophysiol. 229 (2014). https://doi.org/10.1016/j.ijpsycho.2014.08.897
Fonseca, D., Montero, J.A., Guenaga, M., Mentxaka, I.: Data analysis of coaching and advising in undergraduate students. an analytic approach. In: Zaphiris, P., Ioannou, A. (eds.) LCT 2017. LNCS, vol. 10296, pp. 269–280. Springer, Cham (2017). https://doi.org/10.1007/978-3-319-58515-4_21
Dvořáková, K., Kishida, M., Li, J., Elavsky, S., Broderick, P.C., Agrusti, M.R., Greenberg, M.T.: Promoting healthy transition to college through mindfulness training with first-year college students: pilot randomized controlled trial. J. Am. Coll. Health 65, 259–267 (2017). https://doi.org/10.1080/07448481.2017.1278605
Lichtenstein, B.: The mindfulness imperative: how the pedagogical principles of mindfulness provide the foundation for biofeedback. Biofeedback 44, 121–125 (2016). https://doi.org/10.5298/1081-5937-44.3.07
Kabat-Zinn, J.: Mindfulness-based stress reduction (MBSR). Constr. Hum. Sci. 8, 73–107 (2003)
Gold, E., Smith, A., Hopper, I., Herne, D., Tansey, G., Hulland, C.: Mindfulness-based stress reduction (MBSR) for primary school teachers. J. Child Fam. Stud. 19, 184–189 (2010)
Goldin, P.R., Gross, J.J.: Effects of mindfulness-based stress reduction (MBSR) on emotion regulation in social anxiety disorder. Emotion 10, 83–91 (2010). https://doi.org/10.1037/a0018441
Potter, R.F., Bolls, P.D.: Psychophysiological Measurement and Meaning: Cognitive and Emotional Processing of Media. Routledge, New York (2012)
Stern, R.M., Ray, W.J., Quigley, K.S.: Psychophysiological Recording. Oxford University Press, Oxford (2000)
Peper, E., Groshans, G.H., Johnston, J., Harvey, R., Shaffer, F.: Calibrating respiratory strain gauges: what the numbers mean for monitoring respiration. Biofeedback 44, 101–105 (2016). https://doi.org/10.5298/1081-5937-44.2.06
Stroop, J.R.: Studies of interference in serial verbal reactions. J. Exp. Psychol. Gen. 121, 15 (1934/1992). https://doi.org/10.1037/0096-3445.121.1.15
MacLeod, C.M.: Half a century of research on the Stroop effect: An integrative review. Psychol. Bull. 109, 163–203 (1991). https://doi.org/10.1037/0033-2909.109.2.163
Karthikeyan, P., Murugappan, M., Yaacob, S.: Descriptive analysis of skin temperature variability of sympathetic nervous system activity in stress. J. Phys. Ther. Sci. 24, 1341–1344 (2012). https://doi.org/10.1589/jpts.24.1341
Karthikeyan, P., Murugappan, M., Yaacob, S.: Analysis of Stroop color word test-based human stress detection using electrocardiography and heart rate variability signals. Arab. J. Sci. Eng. 39, 1835–1847 (2014). https://doi.org/10.1007/s13369-013-0786-8
Karthikeyan, P., Murugappan, M., Yaacob, S.: A review on stress inducement stimuli for assessing human stress using physiological signals. In: 2011 IEEE 7th International Colloquium on Signal Processing and its Applications, pp. 420–425 (2011). https://doi.org/10.1109/CSPA.2011.5759914
Wallén, N.H., Held, C., Rehnqvist, N., Hjemdahl, P.: Effects of mental and physical stress on platelet function in patients with stable angina pectoris and healthy controls. Eur. Heart J. 18, 807–815 (1997)
Crabb, E.B., Franco, R.L., Caslin, H.L., Blanks, A.M., Bowen, M.K., Acevedo, E.O.: The effect of acute physical and mental stress on soluble cellular adhesion molecule concentration. Life Sci. 157, 91–96 (2016). https://doi.org/10.1016/j.lfs.2016.05.042
Gwizdka, J.: Using Stroop task to assess cognitive load. In: Proceedings of the 28th Annual European Conference on Cognitive Ergonomics, pp. 219–222. ACM, New York (2010). https://doi.org/10.1145/1962300.1962345
Renaud, P., Blondin, J.-P.: The stress of Stroop performance: physiological and emotional responses to color–word interference, task pacing, and pacing speed. Int. J. Psychophysiol. 27, 87–97 (1997). https://doi.org/10.1016/S0167-8760(97)00049-4
Gul, A., Humphreys, G.W.: Practice and colour-word integration in Stroop interference. Psicológica Rev. Metodol. Psicol. Exp. 36, 37–67 (2015)
Yang, E.Z.: Stroop effect - an xhtml 1.0 strict Javascript based interactive program. http://ezyang.com/stroop/. Accessed 6 Feb 2017
BIOPAC Systems Incorporated: AcqKnowledge data acquisition and analysis software. BIOPAC Systems Incorporated, United States (2014). https://www.biopac.com/product/acqknowledge-software/
Kruskal, W.H., Wallis, W.A.: Use of ranks in one-criterion variance analysis. J. Am. Stat. Assoc. 47, 583–621 (1952)
IBM SPSS Statistics. International Business Machines Corporation (2017)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Brumback, H.K. (2018). Can University Students Use Basic Breathing Activities to Regulate Physiological Responses Caused by Computer Use? A Pilot Study. In: Schmorrow, D., Fidopiastis, C. (eds) Augmented Cognition: Users and Contexts. AC 2018. Lecture Notes in Computer Science(), vol 10916. Springer, Cham. https://doi.org/10.1007/978-3-319-91467-1_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-91467-1_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-91466-4
Online ISBN: 978-3-319-91467-1
eBook Packages: Computer ScienceComputer Science (R0)