
Abstract
The technological evolution of HMDs is responsible for making devices available that are lighter, cheaper and more operational, as well as being aware of the risks of cybersickness. Cybersickness involves a range of symptoms similar to those of motion sickness, which affects a significant number of users and is currently regarded as one of the main obstacles to virtual reality helmets in the market. The focal point of this paper is on merging the fields of knowledge of Neuroscience and Games Design as a strategy for mitigating the symptoms of cybersickness. It sets out the results obtained from an experiment carried out with two groups of volunteers – heavy and low users of games for HMDs. These results underpin the sensory rearrangement theory and point out the kind of design choices that can trigger the symptoms of cybersickness. As a result, it is becoming possible to design games by predicting the design decisions required to overcome the problem of this malady.
You have full access to this open access chapter, Download conference paper PDF
1 Introduction
Virtual reality has formed a part of the everyday lives of human beings since the time of primitive designs and has always been employed as a kind of expression through paintings, cinema, theatre, opera, illusionism and other artistic activities [35]. Technology is being integrated with virtual reality in an attempt to surround the spectator with images through an expanded kind of cinema, CAVE and HMDs [9].
The increase of processing speed and reduction in the size of computer components, are making it increasingly feasible to develop technologies for the improvement of HMDs (Head mounted display). These consist of helmets or glasses that have two screens – one for each eye – that produce images from an application produced by the computer.
Virtual reality with HMD is one of the emerging interactive media that is attracting most attention from the large technology companies [29]. Following considerable financial expenditure and research in the area, Facebook, Google and HTC have invested in the creation of their own virtual reality devices with the aim of launching HMDs as products that can be accessible to the general public.
In technological terms, the consolidation of virtual reality in HMD (with cheaper, lighter and more operational devices) has not been enough to overcome what currently represents one of its most serious challenges - cybersickness, one of the main obstacles to the success of these helmets in the market.
Cybersickness induces an array of symptoms that affect the experience of virtual reality. These symptoms include nausea, sweating, motion sickness, headaches, increased saliva, blurred vision and ocular fatigue [29]. It does not represent a disease but is a natural response of the human body to unaccustomed stimuli, and it affects 50% of those involved in the experience of virtual reality.
There are several theories about the physiological causes of cybersickness, in particular the following: (a) sensory conflict [13, 15,16,17, 19]; (b) postural instability [4, 30] (c) poisoning [5, 24, 36]; and (d) sensory rearrangement [28].
In the domain of virtual reality games, cybersickness is also called virtual reality sickness (VRS) and occurs largely as the conflict between three sensory systems: visual, vestibular and proprioceptive [19]. VRS constrains the planning capacity of the designers of games, who are responsible for deciding about all the features, rules and dynamics of a game. The games currently being designed for this platform show significant reductions in the complexity of these mechanisms and dynamics.
In light of this problem, this paper seeks to combine the field of knowledge of Neuroscience with Games Design, in an attempt to find possible design strategies that are able to mitigate the symptoms caused by cybersickness in games made for virtual reality helmets. This involves setting out the results obtained from an experiment on the experience of games involving virtual reality helmets, which was carried out with two groups of volunteers made up of heavy and low users in the 18–35 age range. The purpose of this experiment was to identify and analyze the planned decisions made for this game and their ability either to increase or reduce the presence of symptoms of cybersickness among the users. As a result, the study sought to point out the main design features of the game that should be avoided when devising games of this nature, as well as assisting in the development of games that are increasingly more aware of the perceptive and cognitive system of the users.
2 Simulator Sickness and Cybersickness: The Main Differences
The condition called Simulator Sickness became well known at the end of the 1950s, when virtual reality was still restricted to training helicopter pilots. Its symptoms were recorded for the first time by Casali and Frank [4], and described as discomfort, drowsiness, pallor, sweating, nausea and occasional vomiting, which were the cause of distraction and impaired the effectiveness of the simulators [18]. In view of its complex and polysymptomatic features, (with significant variations from one person to another which made its diagnosis and treatment difficult), Kennedy and Fowlkes [17] decided to recognize it as a syndrome.
As the scope of its field broadened, with a more extensive use of laboratories and simulators, virtual reality reached the general public and the condition of Simulator Sickness began to be called Cybersickness, since it was no longer confined to the world of simulators. The distinction between both conditions also extended to the kind of technology used. Whereas cases of Simulator Sickness generally involve stationary virtual reality devices, those related to Cybersickness stem from the use of HMDs, in which movements of the user´s head have already been detected [27].
Cybersickness is a condition very similar to Motion SicknessFootnote 1, the symptoms of which include vomiting, sickness, nausea, headaches, increased salivation, fatigue, cold sweats, and pallor [8, 16, 19]. Although, motion sickness and cybersickness have similar symptoms, they are not necessarily the same thing [19]. Motion sickness is caused by movements of the body, while the eyes are focused on a static point; in contrast, cybersickness is caused by the inability to simulate the movements of the body while the eyes follow its movements. On account of this feature, some researchers describe cybersickness as visually induced motion sickness (VIMS).
Cybersickness can also be defined as an affliction that is usually caused by immersing someone in virtual environments, which makes a large number of the users of virtual reality devices suffer from the range of symptoms and types of discomfort described above [29]. Jones et al. [14] list the following factors that can lead to either an increase or mitigation of the causes of cybersickness:
-
1.
System: level of distortion of the image; amplitude of the field of vision; flickering on the screen; mobility of the users provided by mobile platforms; screen frequency; resolution; input delays of the player with regard to head movements; and the upgrading frame speed per second;
-
2.
Personal features and experiences: sex, age, illnesses, degree of postural stability and propensity to motion sickness;
-
3.
Time: duration of the user´s experience in virtual reality;
-
4.
Number of experiences: frequency of the user´s experience with virtual reality;
-
5.
Cinematic features: degrees and levels of user interaction in the virtual reality experience.
Rolnick and Lubow [31] stated that when the user makes an unexpected movement, this represents one of the key factors that cause cybersickness. So et al. [32] suggested that acceleration is one of the main factors that cause cybersickness in a navigation of virtual reality environments with HMDs. Since the vestibular human system, which is responsible for the detection of these kinds of stimuli, does not respond to constant speed, the continuous movements represent fewer sensory conflicts. At the same time, linear or angular accelerations cause greater discomfort, owing to the sensory conflict caused by the fact that the body is stopped. For this reason, shorter accelerations are more comfortable to users than those that are more extensive.
In contrast, Palmisano [27] argues that the developers of software must take care when making representations of movements of the head for people wearing virtual reality helmets, because alterations in the desynchronization of the movements of the head or even delays in response, can lead to cybersickness.
Detecting the exact cause of cybersickness is a difficult task because as well as suffering from polysymptomatic distress, the users have different experiences and react in an individual way to the stimuli. The stimuli can be delayed over a period of minutes or hours and the question of human adjustment is another key factor that can make it hard to determine the exact cause of the problem [15]. Users with a tendency to feel sick in rides at amusement parks or cars, also tend to be more sensitive.
In the past, researchers believed that an improvement in the hardware of VR devices would mitigate the symptoms and allow a better human adjustment [33]. On the other hand, studies such as those of Mon-Williansm, Wann e Rushton [23] argued that an upgrading of the hardware of stereoscopic screens caused an increase of the symptoms.
There is a wide range of methods for measuring and assessing cybersickness, which include the following: galvanic skin response; electroencephalograms; and the Simulator Sickness Questionnaire (SSQ). The SSQ was devised by Kennedy [15], together with other researchers, and was based on the MSQ (Motion Sickness Questionnaire). It covers 3 different categories of symptoms: Nausea; Oculomotor Movements; and Disorientation (Chart 1). Each of these categories has different weights and constants. The weights of the SSQ-N, SSQ-O and SSQ-D categories are multiplied to the value assigned by the participant of the virtual reality experience himself, for each symptom mentioned in the questionnaire, in a scale of 0 to 3 (0.0 = no symptom; 1.0 = few symptoms; 2,0 = moderate symptoms; 3 = many symptoms). The weight of the SSQ-T category is multiplied by the sum of the total number of values obtained from the SSQ-N, SSQ-O and SSQ-D categories. Despite the limitations of a questionnaire, where the users might record symptoms that have not really occurred or even lie, the SSQ is the only method that does not require special equipment and its data are easy to interpret.
3 Cybersickness: The Main Theories
Research in the field of neuroscience has investigated cybersickness by means of the sensory rearrangement theory of [25, 28, 36], through an approximation of neuromechanisms responsible for vection, vertigo and motion sickness [1, 10, 19, 27] and through a hypothetical neural pathway of visual, vestibular and proprioceptive senses [11, 12].
Most of the studies related to cybersickness cite the sensory conflict theory as an explanation of the problem. However, after 1990, new theories were advanced by researchers in the field of psychology. These sought to explain motion sickness as being induced by visual stimuli, knowledge, the theory of postural instability and poisoning. The clash between these theories led to an investigation of the possible neural mechanisms and etiology of cybersickness. To understand the neural mechanisms, it is essential to follow strategies to find possible solutions to the malady.
3.1 The Sensory Conflict Theory
Since cybersickness has characteristics similar to motion sickness, theories about the causes of both problems have been correlated. This theory was formulated in an attempt to explain the cause of motion sickness and takes account of the sensory conflict between the information that is being processed by the eyes, semicircular canals, otoliths, proprioceptors and somatosensory data, compared with the existing patterns in a neural network of past experiences. The comparison between the two memories leads to inconsistency and causes the symptoms of motion sickness/cybersickness, at the same time that someone experiences an adjustment to these stimuli [13].
The vestibular system is responsible for transmitting information about movement and head orientation so that the brain can process it. This occurs in the inner ear, which contains the receptors responsible for the position of the head. The signals produced by this positioning are converted into neural signals that are transmitted to the nuclei by means of vestibular nerves. These nuclei are situated in the encephalic trunk and their predictions provide information about the movement of the head and its position relative to gravity, the stability of the eyes during the movements of the head, postural adjustment, autonomous functions and awareness [21].
Reason and Brand [28] concluded that there are several kinds of sensory conflict that can cause motion sickness. Although ‘visual without the vestibular’ sensory conflict is widely accepted as the cause of cybersickness, there are other sensory conflicts such as ‘vestibular disorder without vision’, which cause symptoms of motion sickness, that resemble the symptoms of cybersickness (Table 1).
Although this is the most widely accepted theory, researchers such as Riccio [30] and Money [24] argue that sensory conflict does not exist and that the non-redundant multisensory patterns can be regarded as complementary and not conflicting. Moreover, Stroffregen and Riccio [30] and Frank and Casali [4] stated that the sensory conflict theory fails to predict increases in intensity or when the cybersickness will occur and cannot even determine how severe will be the difference between the senses.
3.2 Theory of Postural Instability
Riccio and Stoffregen [30] put forward the theory of postural instability, which regards a stable posture, or rather, balance, as a natural part of human behavior. Having stable posture can be defined as a situation when someone´s uncontrollable movements are restricted to those caused by factors in the surrounding environment. The body naturally seeks postural stability as shown in the example in Fig. 1, and a person attempts to correct the posture of his body by bending. In the situation represented, as the gravity remains low, the posture will be unstable owing to an incorrect visual stimulus. The more unstable the posture, the more prolonged will be the period of instability or adjustment and the more likely will be the occurrence of cybersickness.

Image illustrating an incorrect visual stimulus [29].
For example, in a virtual reality application, not all the information related to gravity is the same as in the real world and hence while the body perceives gravity in one way, the vision is perceiving it in another. In an attempt to keep its balance, the body ends up by inducing the symptoms of cybersickness. It is worth noting that it is for this reason that authors such as Rebenitch [29] state that postural instability has not ceased to be a type of sensory conflict.
3.3 Theory of Poisoning
The theory of poisoning was suggested by Claremont [5] and later formalized by Treisman [36]. Measured from a perspective related to biological evolution, the theory of poisoning seeks a way of explaining the reason why a movement, or illusion of a movement, in the context of virtual reality, can cause nausea and vomiting.
This theory suggests that motion sickness and cybersickness are the result of an evolutionary process, according to which the intake of poison causes an alteration in the vestibular system that causes sickness and makes one disgorge what is in the stomach [5]. Thus, virtual reality will act in a psychological way and make the body think it has ingested some kind of toxic substance and react in an instinctive way, resulting in symptoms of nausea and vomiting. Money [24] regards motion sickness as an evolutionary abnormality that can be found in several other species and is thus not a condition confined to human beings but also recognizable in other animals.
3.4 Theory of Sensory Rearrangement
The theory of sensory rearrangement is described by Reason and Brand [28] and puts forward the idea that the cause of motion sickness originates from sensory inputs that diverge from the “normal”. Unlike the sensory conflict theory, the theory of sensory rearrangement is supported by the question of human adaptability.
Virtual reality makes use of sensory stimuli to create a world that does not exist. Whatever attempts are made to replicate the physical features of reality, the HMDs are still unable to reproduce the physical world as a whole, with fidelity and hence simple alterations, such as changes in the field of vision, type of navigation and even the lack of gravity, can trigger the symptoms of motion sickness.
Those who wear glasses that include prismatic lenses, have symptoms similar to cybersickness when they alter the angle of the lenses. This is due to the need for sensory adaptation.
When a movement is planned, and the copy of sensory stimulation caused by the brain is compared with the actual stimulation prompted by one of the senses, the brain initiates a sensory rearrangement and produces new information for future movements in accordance with what is occurring (Fig. 2).

Cerebral sensory model of the estimated states in which a general control reaches a state in which the efference copy is withdrawn. This copy is compared with the complete sensory response in multiple regions of the brain [6].
The cerebellum plays a key role in the creation of internal models that are designed to control the arms, legs and other parts of the body. It has neurons called Purkinje fibers, and these acts to stabilize the movements of the head. In recent research in the field of neuroscience, Oman and Cullen [25] suggest that there is a connection between the neurons of the vestibular nucleus in the encephalic trunk and the integrated sensory network of the brain. Researchers such as Dennison [6] state that this connection might be the key to finding the origins of the symptoms of cybersickness.
4 Cybersickness in Virtual Reality Games of HMDs
Cybersickness is a condition that affects the whole process of producing a virtual reality game. According to Carmack [2], cybersickness is one of the main problems facing the virtual games industry in its desire to adopt a greater degree of virtual reality. Other researchers like Mammen et al. [22] think that cybersickness should be viewed as a part of the enjoyment but in a way that does not spoil the experience of the game.
The high latency of the user´s head movements is mentioned as one of the main causes of cybersickness. This was found in old generations of HMD and made it difficult to produce games for the general public. However, even after a significant improvement in virtual reality technology, to the point of almost eradicating the problems of latency, there are still many reported cases of players suffering from cybersickness [29].
The recent virtual reality helmets have corrected several of the problems caused by the old versions; however, the problems cannot only be attributed to technology. A large proportion of the problems that cause cybersickness in virtual reality are linked to the application design [26].
Virtual reality helmets such as Oculus Rift and Playstation VR are intended to provide the user with an experience of virtual reality, while comfortably seated [20]. This position is suited to sessions of the game that last a long time, and reduce the dangers caused by falls.
However, before the designers can provide the player with a satisfactory experience while seated, they must introduce innovations for the time when the navigation of this experience is planned. Shooting games like DOOMFootnote 2 and QUAKEFootnote 3, which make use of cameras with an inner focus lens, require the users to make constant backwards and sideways movements, which are prone to lead to cybersickness. Another factor that impairs the experience of the games of this nature is the need to rotate the virtual body of the user, so he can interact with what takes place in the part behind his field of vision. This requires a physical rotation or the use of an input in a gamepad, which will make the digital camera of the game move.
In other words, most of the experiences of virtual reality games are spoilt by attempts to prevent sensory conflict, since they result in limited navigations or require a great deal of physical space for locomotion. This is also the case with games created for the Vive virtual reality helmet produced by HTC, which employs INAV (In-place Navigation Technique). The game captures the movements of the body by means of sensors and reproduces them from translations to rotations, as a means of embedding the user in the virtual world. However, the rotation of the user´s body through a joystick, allows the camera of the game to move without the user having to move his head and this causes a great disparity between the visual and vestibular information and hence cybersickness.
Another outcome from the creation of virtual reality games lies in the limitations cybersickness causes to the level design, as in the example of the version of virtual reality SUPERHOTFootnote 4. Whereas the version for personal computers and video games allows users to cross over the levels by navigating with a joystick, to carry out the translation and rotation movements, the virtual reality version of the game had all the levels redesigned, so that no navigation of any kind was necessary during each of the levels. The player can only move his body in a way that can allow him to hide from, or shoot at, the enemies spread out in his field of vision.
This makes it clear that despite all the advances in hardware and software technology, until now cybersickness has remained a significant problem in the development of virtual reality games. The fact that it involves both technical constraints and the creative process, makes it difficult to achieve progress in this area.
5 The Experiment
This research study carried out an experiment with the aim of finding possible design strategies that could mitigate the symptoms caused by cybersickness in virtual reality games made for helmets. This involved a sample of two groups of volunteers made up of heavy-users and low-users, in the age range of 18–35. The experiment detected, analyzed and interpreted the design decisions found in the game that was tested and determined whether they were able to increase or reduce the incidence of symptoms of cybersickness among the users.
5.1 Game for the Virtual Reality Helmet
The platform selected for the application of the prototype was the Samsung Galaxy S7 smartphone together with the HMD Samsung Gear VR. With a resolution screen of 2560 × 1440 and processing capacity sufficient to maintain an upgrading rate of 60 fps, the cellular device is coupled to the HMD by an entry micro-USB, capable of receiving information from the gyroscope and the accelerometer of the helmet.
The interface used for the interaction with the prototype was the wireless joystick which comes with the 2017 version of Gear VR. The control has six different buttons. Only the Button located in the region of the thumb was used for the experiment, which apart from being pressable, selects the touch position on the surface (Fig. 3).

Samsung Gear VR and its joystick.
The video processing capacity (GPU) of the cell device has limitations during the development process of the application. Adjustments are necessary, as well as a reduction in the consumption of the device resources to keep the rate at 60 fps. There is a need for this to avoid any lowering of the application performance and hence, resulting in symptoms of cybersickness.
The engine Unity 3D game was used for designing the game employed in the experiment, together with the official library, which is provided free of charge to developers on the official page of the Oculus Company. Small alterations were made to the codes of the basic library to adapt the movements of the character in a way that could avoid the physical movements of the player, particularly when handling curves (Fig. 4).

Alteration of the Updated method of the OVRController.cs script, found in the basic library of Oculus VR.
5.2 The User´s Experience
The application of the experiment took place in five stages: (a) the first involved a survey of information related to the physical condition and health of the user; (b) the second is devoted to the random assignment of participants in the sequence of the game being played, before the beginning of the experience; (c) the third consisted of putting on the virtual reality helmet for the calibration and adjustments; (d) the fourth covered the virtual reality experience. This was carried out in a session lasting a total of 30 min, −10 min being devoted to being immersed in ‘Level 1’ of the game; a 10 min interval; and 10 min for immersion in ‘Level 2’ of the game. We emphasize here the random order for the beginning of the experience at ‘Level 1’ or ‘Level 2’, as indicated in Item ‘b’ and described in Item 4.2.3; (e) the fifth corresponds to the application of the Simulator Sickness Questionnaire (SSQ).
Participants
The participants were all native Brazilians who are residents of the urban regions of the State of Sao Paulo, and came from several professional areas. The experiment comprised 24 male participants and this sample was divided into two groups: 12 low users and 12 heavy users of digital games. The criterion for categorizing and dividing the respective groups took account of the level of experience the users had of virtual reality games for helmets: none, little [low-users] or considerable [heavy users].
The Simulator Sickness Questionnaire
In making an assessment of the symptoms of cybersickness, the experiment relied on the Simulator Sickness Questionnaire, devised by Kennedy et al. [15]. This questionnaire has been adopted for most of the investigative studies of cybersickness. A review of the literature by Carvalho [3] revealed that between 40 and 50 studies have used it as an assessment method.
The 16 items listed on the left show the potential symptoms of the user during the experience of virtual reality. Added to these are three categories that show the possible causes of each of the symptoms mentioned. These are: Nausea; Oculomotor; and Disorientation. The scores are shown through each of the following abbreviations: SSQ-N, SSQ-O, SSQ-D, SSQ-T (Total) (Table 2).
Stages of the method
-
(a)
In the first stage of the experiment, the users answered short questions related to their physical condition and health, in particular any possible history of cardiac problems or in the vestibular system such as labyrinthitis.
-
(b)
In the second stage, a random allocation of the order of the game (‘Sequence A’ or ‘Sequence B’) was made to begin the experience in the virtual reality helmet. At this time, the amount of information given to the user was restricted with the aim of avoiding making any suggestions.
In ‘Sequence A’ of the game, the player began his navigation from Level 1, followed by Level 2; while in ‘Sequence B’, the player began his experience at Level 2, so as to follow Level 1 afterwards in a reverse order. The purpose of altering the design of these levels was to determine the possible effects on the checked results that originated from the sequence in which the features of the game were displayed to the user and hence find out the possible symptoms of cybersickness related to them (Table 3).
-
(c)
In the third stage, the participant put on the virtual reality helmet and was given instructions about how to move and control the avatar in the space of the game. At this time, the user was also told to avoid moving his body during the curves; the aim of this was to encourage him to use the control as an interface for interaction. In addition, the player was requested to memorize the effects of the experience on his body and note the differences between the two levels, in particular with regard to possible symptoms caused by cybersickness.
-
(d)
The fourth stage covers the experience of the user in two levels of the game. The experience at each level lasts 10 min with an interval between them of the same length of time. The order for the beginning of ‘Level 1’ or ‘Level 2’ is random.
Throughout this stage, the participant is questioned about the occurrence of any symptom related to cybersickness, and about what aspect of the game he thinks is responsible for triggering it. It is worth mentioning that the user is granted the right to abort the experiment at any time, especially if the symptoms of cybersickness too much to bear.
-
(e)
The fifth and final stage occurs soon after the end of the experience, which the player has of both levels of the game and involves the user being given the questionnaire (SSQ) to fill in. The experience at each level is recorded by the user in separate Tables. As well as the Table, the form includes a section for information regarding the identity of the volunteer, as well as space for possible comments about the experience he has undergone.
5.3 Results and Discussions
The data collected from the Simulator Sickness Questionnaire was divided into the following categories: SSQ-N [Nausea]; SSQ-O [Oculomotor]; SSQ-D [Disorientation]; and SSQ-T [Total]. The scores of each participant were calculated in accordance with the guidelines indicated by the referred method. Graph in Fig. 5 shows the results obtained from all the participants of the experiment, who were classified as ‘Heavy Users’ and ‘Low Users’.

Results of the SSQ: a comparison between ‘heavy users’ and ‘low users’.
The comparison between the results obtained for the group of ‘Heavy Users’ and ‘Low Users’, give evidence of a striking difference between the scores for all the categories, that observed in the SSQ-D category being the most significant: with 17.05 for the low users and 34.22 for the heavy users. SSQ-T also showed a significant difference: with 26.80 for the low users and 42.38 for the heavy users.
On the basis of these results, it is possible to identify, analyze and interpret the main design decisions that increase the symptoms of cybersickness, in each of the sequences A and B, and particularly, for each group (Table 4).
-
(A)
The main difference in the performance of heavy users and low users
The differences observed in the results obtained for the groups of heavy users and low users suggest that the low users have more symptoms related to cybersickness, especially with regard to the SSQ-D [Disorientation] category.
These results strengthen the theory of sensory rearrangement, put forward by Reason and Brand [28]. This means the players who are heavy users of digital games end up by having efference copies for situations that are repeated in environments reproduced by virtual reality helmets – for example, through the rotation of the camera by using leveraged analogical skills in joysticks. This very common technique in video games is used in the experiment and has proved to be one of the main causes of the disorientation experienced by the participants. Other uncommon factors among the low users such as irregular movements when climbing stairs or involuntary movements of the head of the avatar, are also commonly found among heavy users, a fact which leads the more experienced users to adapt more quickly to the stereoscopic screen of the HMD.
-
(B)
Cybersickness originating from luminous stimuli
The comments of the participants referred to which of the design decisions that are common in video and computer games, lead to an increase in the symptoms of cybersickness, when applied to virtual reality games.
The strong light in the corridor (Fig. 6), used as a kind of distraction to prevent the player from noticing a hidden key, features as one of the main complaints of the participants in the experiment as being associated with symptoms of cybersickness. A smaller number of users also noted the difference of the lighting in the inner environment and the outer environment, which was exposed to the skybox as a cause of these symptoms. In both situations – the sudden change in the intensity of the lighting caused a significant increase in cybersickness.

Source of shining light in Level 1 of the game designed and applied in the experiment
-
(C)
Cybersickness caused by the movement of climbing stairs: conflicts between the experience and efferent copies
Another result observed was the difference between people who had symptoms of cybersickness when they climbed or went down ramps or stairs. According to Dorado and Figueroa [7], ramps lead to better results with regard to mitigating cybersickness when compared with those obtained from people using stairs with natural movements (Fig. 7).
Fig. 7. 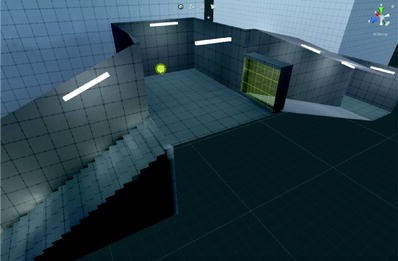
Ramp and staircase at a moment in the game designed and applied to the experiment

This result provided evidence that the action of climbing stairs with natural movements causes instability in the movements of the camera. The link between instability and this situation is uncommon in the vestibular system of the human beings, which already has efferent copies of vertical movements related to ‘climbing stairs’, stored in its nervous system. In an experience with virtual reality helmets, the vestibular system is not stimulated during this kind of movement. This means it is not feasible to make an ideal comparison between the situation experienced by the player and the existing reafference, which leads the user to suffer from symptoms of cybersickness.
6 Conclusion
Cybersickness has arisen as a limiting factor for the creation of games that require greater complexity in the handling of the avatar (virtual character) of the player. In light of this, when compared with computer games and videogames, games for virtual reality helmets are being simplified.
This paper investigates the close alliance between the design of games and the fields of neuroscience by seeking to understand the crucial importance of overcoming cybersickness. When carried out from the perspective of the operational sensorimotor and cognitive systems of the user, (and from the neurophysiological mechanisms that cause cybersickness), a planning strategy can open up secure ways of exploring the design of games for HMDs, by providing evidence of design features that are able to maintain the navigational complexity for the users through different levels of the game, while at the same time, mitigating the symptoms of cybersickness.
This potential capacity is borne out by the results obtained from the application of the experiment set out here and can be carried out with both heavy users and low users of games for virtual reality helmets. The main results and benefits for the mitigation of the symptoms caused by cybersickness emerge from the following design decisions:
-
Avoiding the use of ladders in designing the “levels”;
-
Avoiding sharp contrasts in the lighting when applied to different settings and effects;
-
Taking account of the sensory adaptation of the user in designing different levels. In other words, situations capable of causing cybersickness should only be shown to the player after he/she has fully adapted to the virtual reality interface;
Ensuring the design of games involving a complex navigation system are aimed at heavy users, since their previous experiences with regard to interaction in virtual reality systems, strongly corroborates the fact that they are able to make a faster and more effective sensory adaptation to the interface of this game.
It should be noted that currently cybersickness represents one of the most limiting factors for high investment in the development of complex games for HMDs. This fact puts in the shade the current games for HMDs, which are designed for traditional platforms.
In view of this, the future development of this research study seeks to carry out and apply new experiments aimed at broadening the range of design solutions described here. In this way an attempt will be made to overcome the symptoms caused by cybersickness, in both low and heavy users of games for virtual reality helmets.
Thus, it is believed that by following the recommendations for this purpose in a systematic way, a significant contribution can be made to the games industry for everyone concerned.
Notes
- 1.
It is characterized by the intolerance to the movement resulting from a sensory conflict between the vestibular, visual and proprioceptive systems. This results in a physiological response related to the stimuli of unfamiliar movements [28].
- 2.
Games published by Bethesda Softworks and designed by Id Software. First launched on 13th May 2016.
- 3.
Game first launched on 5th December 1999 published and developed by Id Software.
- 4.
Independent distributed and developed by SUPERHOT Team. Its virtual reality version has been released in 6th December 2016, while its PC version has been released 25th February of 2016.
References
Brandt, T.: Vertigo: its multisensory syndromes, n. 2 (1999)
Carmack (2014). https://www.youtube.com/watch?v=nqzpAbK9qFk
Carvalho, M.R., Da Costa, R.T., Nardi, E.A.: Simulator Sickness Questionnaire: Tradução e adaptação transcultural. Jornal brasileiro de psiquiatria 60(4), 247–252 (2011)
Casali, J.G., Frank, L.H.: Manifestation of visual/vestibular disruption in simulators: severity and empirical measurements of symptamotology. In: AGARD Conference, n. 433, pp. 11–18 (1988)
Claremont, C.A.: The psychology of sea-sickness. Psyche 11, 86–90 (1931)
Dennison, M.: Motion sickness in virtual environments, p. 101. Tese (Doutorado) em Psicologia, California (2017)
Dorado, J.L., Figueroa, P.A.: Ramps are better than stairs to reduce Cybersickness in applications based on a HMD and a gamepad. In: IEEE Symposium on 3D user Interfaces, Minneapolis, pp. 29–30 (2014)
Ehrlich, S.D.: Motion Sickness. Pennstate Hershey (2014). http://pennstatehershey.adam.com/content.aspx?productId=107&pid=33&gid=000110
Grau, O.: A arte virtual: Da ilusão à imersão. UNESP e Senac, São Paulo (2007)
Hettinger, J., Berbaum, K.S., Kennedy, R.S., Dunlap, W.P., Nolan, M.D., et al.: Vection and simulator sickness. Mil. Psychol. 2, 171–181 (1990)
Ji, J.J., So, R.H.Y., Cheung, T.F., Howarth, P., Stanney, K.: A search for possible neural pathways leading to visually induced motion sickness. Vision 2, 131–134 (2005)
Ji, J.J., So, R.H.Y.: Visually induced motion sickness: an insight from neuroscicences. In: First International Symposium on Theoretical Issues in Ergonomics Science, San Diego, pp. 18–21 (2004)
Johnson, D.M.: Introduction to and review of simulator sickness research. Research report (U.S. Army Research Institute for the Behavioral and Social Sciences), Fort Rucker (2005)
Jones, M.B., Kennedy, R.S., Stanney, K.M.: Toward systematic control of Cybersickness. Presence: teleoperators and virtual environments, vol. 13, Massachusetts, pp. 589–600 (2004)
Kennedy, R.S., Lane, N.E., Berbaum, K.S., Lilienthal, M.G.: Simualtor sickness questionnaire: an enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 3(3), 203–220 (1993)
Kennedy, R.S., Lanham, S., Drexler, J.M.: A comparison of incidences, symptom profiles, measurement techniques and suggestions for research. Presence 6, 638–644 (1997)
Kennedy, S.R., Fowlkes, J., Berbaum, K.S., Lilienthal, M.G.: Use of motion sickness history questionnaire for prediction of simulator sickness. Aviat. Space Environ. Med. 63, 588–593 (1992)
Kolasinski, M.E.: Simulator Sickness in Virtual Environments, p. 68 (1995)
LaViola, J.: A discussion of cybersickness in virtual environments. ACM SIGCHI Bulletin 32, 47–56 (2000)
Luckey Patcher. https://www.youtube.com/watch?v=-YCBadIVro8&list=PLckFgM6dUP2hc4iy
Lundy-Ekman, L.: Neurociência: Fundamentos para a Reabilitação, 2nd edn. Elsevier, Rio de Janeiro (2004)
Mammen, S.V., Knote, A., Adenhofer, S.: Cyber sick but still having fun. In: VRST 2016 Proceedings of the 22nd ACM Conference on Virtual Reality Software and Technology, New York, pp. 325–326 (2016)
Mon-Williams, M., Wann, J.P., Rushton, S.: Design factors in stereoscopic virtual-reality displays. Soc. Inf. Disp. 3, 207–210 (1995)
Money, K.E.: Motion and Space Sickness. CRC Press, Boca Raton (1990)
Oman, M.C., Cullen, E.K.: Brainstem processing of vestibular sensory exafference: implications for motion sickness etiology. Exp. Brain Res. 232(8), 2483–2492 (2014)
Porcino, M.T., Clua, E., Trevisan, D., Vasconcelos, C.N., Valente, L., et al.: Minimizing cyber sickness in head mounted display systems: design guidelines and applications. In: IEEE 5th International Conference on Serious Games and Applications for Health (SeGAH), Perth (2017). ISSN 978–1-5090-5482-4
Palmisano, S., Mursic, R., Kim, J.: Vection and cybersickness generated by headand- display motion in the Oculus Rift. Displays 46, 1–8 (2017)
Reason, J.T., Brand, J.J.: Motion Sickness. Academic Press, London (1975)
Rebenitch, L., Owen, C.B.: Review on cybersickness in applications and visual displays. Virtual Real. 20, 101–125 (2016)
Riccio, G., Stroffegen, T.: An Ecological Theory of Motion Sickness and Postural Instability. Ecol. Psychol. 3, 195–240 (1991)
Rolnick, A., Lubow, R.E.: Why is the driver rarely motion sick? the role of controllability in motion sickness. Ergonomics 34, 867–879 (1991)
So, R.H.Y., Lo, W.T., Ho, A.T.K.: Effects of navigation speed on motion sickness caused by an immersive virtual environment. Hum. Factors 43(Edição 3), 452–461 (2001). The Journal of the Human Factors and Ergonomics Society, Hong Kong
Stanney, K., Salvendy, G.: Aftereffects and sense of presence in virtual environments: formulation of a research and development agenda. Int. J. Hum. Comput. Interact. 10, 135–187 (1998)
Talban, R.J., Cardulo, F.M.: Neural mechanisms of motion sickness. J. Med. Invest. 41, 44–59 (2001)
Tori, R., Kirner, C.: Fundamentos de realidade virtual. In: Fundamentos e tecnologia de realidade virtual e aumentada. Belém: VIII Symposium on virtual reality. Cap. 1, pp. 2–22 (2006)
Treisman, M.: Motion sickness: an evolutionary hypothesis. Science 197, 493–495 (1977)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Moreno, F., Zuanon, R. (2018). Game Design and Neuroscience Cooperation: Perspectives to Cybersickness Reduction in Head Mounted Displays Experiences. In: Duffy, V. (eds) Digital Human Modeling. Applications in Health, Safety, Ergonomics, and Risk Management. DHM 2018. Lecture Notes in Computer Science(), vol 10917. Springer, Cham. https://doi.org/10.1007/978-3-319-91397-1_26
Download citation
DOI: https://doi.org/10.1007/978-3-319-91397-1_26
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-91396-4
Online ISBN: 978-3-319-91397-1
eBook Packages: Computer ScienceComputer Science (R0)