
Abstract
Mobile phones appear to have become one of the main entertainment features in adolescents’ life, which has also been suggested to be potentially addictive. A shortened version of a scale used to detect this potential addiction, the Mobile Phone Problematic Use Scale (MPPUS-10; Foerster, Roser, Schoeni, & Röösli, 2015) has been extracted from the Mobile Phone Problematic Use Scale for Adolescents (MPPUSA; Lopez-Fernandez, Honrubia-Serrano, & Freixa-Blanxart, 2012). To validate this shortened scale, a cross-national study surveyed 1391 high school students in both Spain and Greece, assessing both socio-demographic variables and self- perceived mobile use dependency. The MPPUS-10 exhibited good factorial validity, good reliability, and similar mid scores in both countries. Results from sub-scale symptomatology showed consistency in elevated levels of craving, withdrawal, and loss of control related to mobile phone use in both countries. This study presents evidence of self-perceived mobile phone dependence in south-European high school students, but more research is needed.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others

Keywords
- Mobile phone dependence
- Smartphone dependence
- Behavioural addiction
- Cross-cultural study
- High school students
1 Introduction
Interacting with mobile phones (such as smartphones) has now become embedded in the lifestyles of students from high schools across the world.
The International Telecommunication Union (ITU) [1] has reported that between 2007 and 2015, mobile-broadband subscriptions increased 12-fold globally. The ITU has recently ranked both Spain and Greece among the higher scoring European nations in the Information and Communication Technologies Development Index (IDI), with Spain ranking 31st (IDI = 7.92) and Greece 34th (IDI = 7.92) out of 40 global economies [1]. This Index is a benchmark for comparing the level of technological development in countries across the world. In the case of Spain and Greece, these two countries are reported to have among the highest domestic mobile minutes and message (SMS) economies (i.e., in 2014, the average domestic mobile minutes per subscription per month were 176 in Greece and 131 in Spain; the average SMSs sent per mobile subscription per month were 31 in Greece and 4 in Spain). In relation to mobile-broadband prices, for a pre-paid handset-based on a 500 MB monthly data allowance, again both countries are ranked in the first economies (Spain: n. 22 with 525 MB and Greece n. 61 with 600 MB). Finally, during 2015, mobile subscriptions per 100 habitants were 107.9 in Spain and 110.3 in Greece. These data exhibit how mobile phones are a widespread technology and highly used in both countries.
Nowadays, it is known mobile phone overuse can psychologically interfere with users’ lives, potentially leading to negative health effects such as dependence-like [2, 3] and addiction symptoms [4]. Problematic Mobile Phone Use (PMPU) has been defined, partly, as a potential behavioural addiction through the use of mobile phones or smartphones. PMPU can cause issues for users when enacted as an excessive form of relationship maintenance, in banned and/or dangerous situations, and during addictive use [5]. These addictive symptoms can include cognitive salience, loss of control, mood modification, tolerance, withdrawal, conflict, and relapse [6]. To assess this potential addiction and its symptoms, the goal standard PMPU scale has been the Mobile Phone Problem Use Scale (MPPUS [2]), originally consisting of twenty-seven items, which has also been adapted to adolescents using twenty-six items (MPPUSA [7, 8]), and recently has been shortened to ten items also for adolescents (MPPUS-10 [9]). Furthermore, although a great part of the research into this potential addiction has a decade of psychometric research, with a number of validated PMPU scales, rarely are these scales exclusively tested within adolescent samples [10], and few times have they been discussed regarding their implications for this age group or secondary school education.
Basically, it has been argued that mobile phones predominantly affect adolescents in their social, affective, and behavioural spheres, impacting their relationship with parents and peers, and interfering with school and leisure activities [11]. However, to the best of the authors’ knowledge, the field of mobile phone dependence has little research investigating its impact on high school students.
To date, there is a lack of research concerning the role of mobile phones in educational settings (such as high schools) and little is known about mobile phones in adolescents using a cross-cultural approach. Consequently, the objectives of this cross-national study were twofold. First, to compare the validations of a shortened screening tool to detect mobile phone dependence (the MPPUS-10) in Spanish and Greek, and second, to explore the perceived addictive symptoms in relation to mobile phones in adolescent high school students from both countries.
2 Method
2.1 Participants and Procedure
The study surveyed two convenience samples at high schools in both Barcelona (Spain: n = 887) and Athens (Greece: n = 504), at different snapshots of time (2012–2013 in Spain and 2016 in Greece). The sample comprised of 1391 participants (Spain: 49.94% male; age range 12–18 years; Greece: 51.78% male; age range 12–18 years) sampled from high school students that voluntarily agreed to participate. Regarding the Spanish subsample, almost all students had their own mobile phone (79%); similarly, in the Greek subsample, all students possessed a mobile phone. The questionnaire was administered during class time, with the teacher present, and all responses were recorded anonymous.
2.2 Instruments
The survey was administered in each country with a paper-based format and comprised of two sections: (a) socio-demographics, (b) the Short Version of the MPPUSA [7, 8]: the MPPUS-10 [9]. The original version of the MPPUSA was English, as with the original MPPUS [2], previously validated in Spanish [7] and Greek iterations, which were translated using the translation-back translation method [12].
The MPPUS-10 [9] comprises of ten items rated on a Likert scale (ranging from 1 “Not true at all” to 10 “Extremely true”). The total score ranges between 10 and 100, with the highest score being the maximum presence of ‘Mobile phone (dependence) problem use in adolescents’ (see Table 1). The Greek version uses a Likert scale from 4 “Strongly agree” to 1 “Strongly disagree”. The response rate of the MPPUS-10 in each country was 78.4% in Spain and 100% in Greece.
3 Results
The MPPUS-10 scores were in Spain (n = 887), M = 36.97, SD = 22.4 [range from 10–100]; while in Greece (n = 504), M = 20.75, SD = 4.64 [range from 10–40].
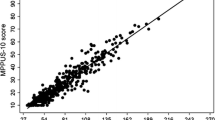
The item analysis of the scale per country is presented in Table 2 and Fig. 1.

Scree plots of MPPUS-10 in Spanish and Greek adolescents (X: eigenvalues, Y: components/factors)
There were slight differences between items regarding behaviors in both countries. The 10-item mobile phone dependence scale had good reliability according to Cronbach’s alpha coefficients (α = .92 for Spain; α = .71 for Greece). The results obtained through an Exploratory Factor Analysis with Principal Component technique were similar in both countries (Spain: KMO = .93; Bartlett’s test: χ2(45) = 6055.98; p < .001; Greece: KMO = .80; Bartlett’s test: χ2(45) = 626.5; p < .001) and both yielded a two factor solution: explaining 70.42% of the total variance in Spain (Factor 1: 60.3% and Factor 2: 10.12%) and 40.5% of the total variance in Greece (Factor 1: 28.08% and Factor 2: 12.43%).
In relation to the association between sociodemographic and self-perceived mobile phone dependence in both countries, several relevant variables showed significant bivariate relationships. Gender was significantly associated with MPPUS-10 total score in Spain (but not Greece), with females being more prone to perceive themselves as dependent on using their phones (t(884) = −2.05, Z = −3.124, p < .05 [Men: M = 35.46, SD = 23.39, Women: M = 38.53, SD = 21.27]), contrasting to the Greek sample (t(502) = −.024, Z = −.52, p = 0.981).
In relation to the self-perceived addictive symptomatology of mobile phones, Spain high school students highlighted craving, withdrawal, loss of control and negative life consequences as primary symptoms, which again contrasted against Greek high school students, reporting relatively little craving, withdrawal, and loss of control symptoms.
4 Discussion
The first objective of this cross-national study was to compare the validation of a new shortened screening tool (the MPPUS-10) to detect self-perceived mobile phone dependence, in two adolescent samples studying at Spanish and Greek high schools. The second objective was to explore the reported addictive symptoms that adolescents, from both countries, perceived regarding their own mobile phone or smartphone usage.
Both MPPUS-10 versions showed good internal consistency across both temporal snapshots and geographical regions (i.e., 2012–2013 in Spain and 2016 in Greece), which is comparable to validations of the original shorter version (MPPUS-10, e.g., α = .85 in Switzerland 2013 [9]) and original (longer) versions (the 27-item scale for adults (e.g. α = .93 in Australia 2003 [2]) and 26-item scale for adolescents (e.g. α = .97 in Spain 2012 [7], α = .95 in United Kingdom 2010 [8])). However, the factorial structures were slightly different and not unidimensional, as expected from longer versions investigations [2, 7, 8]; this is likely due to the fact the MPPUS-10 was multifactorial (i.e., with five factors associated to symptoms: loss of control, withdrawal, negative life consequences, craving, and peer dependence [9]). However, in both our subsamples, the MPPUS-10 obtained a two-factor solution (F1: with almost all items, and F2: items related theoretically to withdrawal and loss of control, which could be argued to be craving and conflict addictive symptoms respectively). This could be due to the different snapshots of time, different countries, and cultures in which data was collected, among other potential confounds (e.g., socio-economic level, type of school, pedagogic approach).
In their study, Foerster et al. [9] did not find a threshold for differentiating between problematic and non-problematic adolescent mobile phone users. This supports the idea that problematic mobile phone use is on a continuum, with higher MPPUS-10 scores suggesting a higher likelihood of addictive mobile phone use in high school students. Therefore, based on these findings, little self-perceived dependence seems to exist, and when it does it appears to be more common in girls, but only in Spain [7]. Furthermore, when analyzing descriptive findings related to the addictive symptomatology, only craving, withdrawal and loss of control seem to be prevalent in both countries, with slight differences between cultures [7,8,9]. However, in our study ‘peer dependence’ does not appear to be a factor related to a potential mobile phone use addiction in adolescents. Finally, based on the overall descriptive score in both countries, the MPPUS-10 seems to show an average of ‘mid-self-perceived’ dependence in Spanish and Greek adolescents, attending to also that both countries are high ranked in mobile phone use [1].
Limitations of this cross-national study are the convenience samples used and collecting data in different academic years in both countries (although with the same methodology and instruments, and in same type of high school students). Moreover, future studies must transform the scores into a standardized procedure [13], for effective in-depth comparisons with each item, factor, and symptom, as well as the potential predictors, which have started to emerge in this preliminary and exploratory study.
Future research could also reinforce the validation of this short version for use in schools and educational settings (where adolescents develop their usual activities), in order to detect potential causes and consequences related to a certain degree of dependency on mobile phones (e.g., excessive attachments to others, excessive gaming [5]), or even perhaps a potential addiction to the range of mobile apps offered to adolescents (e.g., WhatsApp, Instagram, Facebook). Moreover, mobile phones are still commonly perceived as negative by high school teachers (who tend to be over 50 years old [14]). More research is needed regarding these professionals in educational settings, in order to collect their own perspectives on these issues. Nevertheless, mobile phones are now a potential tool for informal learning and leisure (as mobile phones, iPod and iPads are also used for improving learning outcomes [15]) and a prevalent communication tool that merits more research, especially in children from our contemporary societies.
References
International Telecommunication Union [ITU]: Measuring the Information Society Report 2016. ITU, Geneva (2016). https://www.itu.int/en/ITU-D/Statistics/Documents/publications/misr2016/MISR2016-w4.pdf. Accessed 07 Feb 2017
Bianchi, A., Phillips, J.G.: Psychological predictors of problem mobile phone use. CyberPsychol. Behav. 8(1), 39–51 (2005)
Km, W., Park, B.-W., Lee, K.C.: Measuring smartphone dependence: a first step with emphasis on factor analytic evidence. Inf. – Int. Interdiscip. J. 14, 3031–3047 (2011)
Kwon, M., Lee, J.-Y., Won, W.-Y., Park, J.-W., Min, J.-A., Hahn, C., Gu, X., Choi, J.-H., Kim, D.-J.: Development and validation of a smartphone addiction scale (SAS). PLoS One 8(2), e56936 (2013). https://doi.org/10.1371/journal.pone.0056936
Billieux, J., Maurage, P., Lopez- Fernandez, O., Kuss, D.J., Griffiths, M.D.: Can disordered mobile phone use be considered a behavioral addiction? An update on current evidence and a comprehensive model for future research. Curr. Addict. Rep. 2, 156–162 (2015)
Griffiths, M.: A “components” model of addiction within a biopsychosocial framework. J. Subst. Use 10(4), 191–197 (2005)
Lopez-Fernandez, O., Honrubia-Serrano, M.L., Freixa-Blanxart, M.: Adaptación española del ‘Mobile Phone Problematic Use Scale’ para población adolescente. Adicciones 24, 123–130 (2012)
Lopez-Fernandez, O., Honrubia-Serrano, M.L., Freixa-Blanxart, M., Gibson, W.: Prevalence of problematic mobile phone use in British adolescents. Cyberpsychol. Behav. Soc. Netw. 17, 91–98 (2013)
Foerster, M., Roser, K., Schoeni, A., Röösli, M.: Problematic mobile phone use in adolescents: derivation of a short scale MPPUS-10. Int. J. Public Health 60(2), 277–286 (2015)
Lopez-Fernandez, O.: Problematic internet and mobile phone use in adolescents in Barcelona and London. Doctoral thesis, University of Barcelona, Barcelona, Spain (2013). http://www.tdx.cat/handle/10803/126442. Accessed 11 Mar 2017
Choliz, M.: Mobile phone addiction: a point of issue. Addiction 105, 373–374 (2010)
Brislin, E.W.: Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1(3), 185–216 (1970)
Lopez-Fernandez, O., Losada-Lopez, J.L., Honrubia-Serrano, M.L.: A proposed method for the study of predictors for detecting excessive use of technology: problematic internet and mobile phone usage in adolescents. Aloma 33(2), 49–58 (2015)
O’Bannon, B.W., Thomas, K.: Teacher perceptions of using mobile phones in the classroom: age matters! Comput. Educ. 74, 15–25 (2014)
Martin, F., Ertzberger, J.: Here and now mobile learning: an experimental study on the use of mobile technology. Comput. Educ. 68, 76–85 (2013)
Acknowledgments
The authors would like to thank to Niki Davis (Professor University of Canterbury, New Zealand) for contacting both researchers to do this paper and the World Conference on Computers in Education 2017. To the Chair of the IPC for IFIP WCCE 2017, Don Passey, for the opportunity to present it and the reviewers of this paper. Finally, to Professor Christopher Dawes and Lucy Justice (Research assistants at Nottingham Trent University) for proof-reading this paper.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 IFIP International Federation for Information Processing
About this paper

Cite this paper
Lopez-Fernandez, O., Nikolopoulou, K. (2017). Measuring Mobile Phone Dependence in Spanish and Greek High School Students Using a Short Scale: Validating Both Adaptations. In: Tatnall, A., Webb, M. (eds) Tomorrow's Learning: Involving Everyone. Learning with and about Technologies and Computing. WCCE 2017. IFIP Advances in Information and Communication Technology, vol 515. Springer, Cham. https://doi.org/10.1007/978-3-319-74310-3_12
Download citation
DOI: https://doi.org/10.1007/978-3-319-74310-3_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-74309-7
Online ISBN: 978-3-319-74310-3
eBook Packages: Computer ScienceComputer Science (R0)