
Abstract
The majority of individuals diagnosed with multiple sclerosis (MS) experience a major decline in their abilities due to the progression of MS after five years post-diagnosis. Following this period, they need to learn how to cope with the functional limitations caused by the disease and how to age with MS. The World Health Organization (WHO) and the Consortium of Multiple Sclerosis Centres advise that individuals with MS take control of decisions affecting their wellness and life and self-manage their disease as often as possible. Mobile health technologies provide potential support for disease self-management. There are currently nine MS-specific mobile applications on the market to help individuals with MS manage their health and daily activities. However, none of these apps was tested with their target population. Moreover, many individuals with MS have numerous usability problems with current mobile touchscreen interfaces. Therefore, the existing apps need to be usable by individuals with MS, as well as people aging with this mobility-affecting chronic disease. This research contributed to the state-of-knowledge about the design of mobile interfaces for people aging with MS and tested current mobile interfaces with people with MS and older adults to provide recommendations for the design of mobile interfaces for people aging with MS to further inform the design of the mobile application for individuals aging with MS.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
The majority of individuals diagnosed with multiple sclerosis (MS) experience a major decline in their abilities due to the progression of MS after five years post-diagnosis (Gulick 1998). Following this period, they need to learn how to cope with the functional limitations caused by the disease and how to age with MS. The World Health Organization (WHO) (Organization 2008) and the Consortium of Multiple Sclerosis Centres (Fraser et al. 2009) advise that individuals with MS take control of decisions affecting their wellness and life and self-manage their disease as often as possible.
Mobile health technologies provide potential support for disease self-management (Zulman et al. 2015). There are nine MS-specific applications on the market to help individuals with MS manage their health and daily activities. These mobile applications vary in their functionality and primarily focus on providing basic information about latest research, news, and practical tips on health and wellness, medication adherence, self-reporting of daily activities, moods, and health status, and sharing the data with healthcare providers. However, none of these apps was tested with their target population. Given that many individuals with MS have many usability problems with current mobile technologies (Irwin and Sesto 2009), the existing apps need to be usable by people aging with this mobility-affecting chronic disease.
MS has overlapping symptoms with physical results of aging including decline in muscle strength, problems with balance, weakness, fatigue, reduced sensation, vision impairments, alterations in bowel/bladder function, cognitive impairment, pain, osteoporosis and sleep disturbances (Finlayson 2002; Fleming and Pollak 2005; Stern 2005; Stern et al. 2010). The majority of people with MS reported their physical health limited daily activities and caused them to accomplish less than they wanted (Minden et al. 2004). To accommodate individuals aging with MS with self-management of their disease, this project tested current mobile MS-specific interfaces and reported the recommendations for the design of future mobile touchscreen applications for health and wellness self-management for this user population.
2 Background
Because of the lack of literature on the interaction with mobile touchscreen interfaces for people aging with MS, we are reporting the related work for people with MS-related symptoms, such as a motor, vision, and cognitive impairments, including tremor.
Individuals with ranges of motor disabilities are adopting touchscreen devices, they are using them on a daily basis, and they think that these devices empower them and help them be independent (Anthony et al. 2013). However, they often use customized devices and configurations, suggesting that there is a need for the improvement in accessibility of these devices. Moreover, users with motor impairments experience problems with tapping (Duff et al. 2010; Irwin and Sesto 2012). They were less accurate, slower and had greater dwell times (time that finger remains on the button) than people without motor impairments. In addition, they have problems with small button size (Hurst et al. 2008; Irwin and Sesto 2009), and small size of the screen features (Kurniawan 2008). Moreover, older adults with tremor experience problems with tapping as well (Wacharamanotham et al. 2011). They do not get the same input efficiency and are unsatisfied with mobile technology (Mertens et al. 2010). Older adults with tremor experience problems with tapping as well (Wacharamanotham et al. 2011).
Mobile interfaces are often not accessible to people with vision impairments due to problems with small fonts, small form factors, and small or undifferentiated keys (Dawe 2007; Kane et al. 2008, 2009). Researchers (Bhachu et al. 2008; Leonard et al. 2005; McGookin et al. 2008; Plos and Buisine 2006; Tomioka et al. 2002; Watanabe et al. 2008) found that older adults and visually impaired individuals encounter many problems with mobile interfaces including issues with small size of the devices and screens, small buttons, screens with text difficult to read, complex interface menus, using the gestures, knowing their relative location on the screen, lack of tactile feedback, inconsistent navigation, and audio feedback.
Individuals with cognitive impairments encountered numerous problems with user interfaces including overly complex mobile phone menus and interfaces, access to the voicemail, inconsistent display information and navigation, lack of presence of the physical stimuli, cognitive overload, number of distracting elements, the presence of multiple simultaneous tasks, and the level of relevant information (Dawe 2007; Holzinger et al. 2007).
3 Research Study Objectives
There are only nine MS-specific applications on the market to help individuals with MS manage their health, wellness, and daily activities. The existing MS-specific mobile apps were not tested with their target population. Moreover, people with MS have usability problems with current mobile technologies. There is a need to test the usability of these applications by its target user population.
This research contributed to the state-of-knowledge about design of mobile interfaces for people aging with MS, and explored whether the aging with this disease has an effect on usability of mobile applications for people with MS. Since it was hard to recruit participants aging with MS, two groups of participants, older adults and people with MS, participated in the study to assess the effects of aging on usability compared to ones of MS.
The purpose of this research study was to test current mobile interfaces investigate how well the salient design elements in current mobile user interfaces meet the usability requirements of people aging with MS. Specific aims of the study were to evaluate the usability of two current MS health and wellness self-management mobile applications and one health app for the general population to identify the effectiveness of app attributes and provide recommendations for the design of new mobile technologies for the target population.
4 MS-Specific Mobile Applications
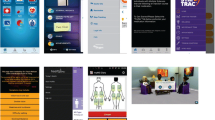
The number of mobile applications designed for people with MS is very limited. The nine applications available to this group of users primarily focus on providing basic information about latest research, news, and practical tips on health, nutrition, and fitness, self-recording of health status and medication adherence, self-recording of daily activities, symptoms, mood, and similar, and/or sharing the data with healthcare providers (See Fig. 1).

Current mobile applications for individuals with MS
Multiple Sclerosis Association of America (MSAA) released a mobile phone application, My MS Manager, for individuals with MS and their caretakers (My MS Manager™ 2012). The app offers tools for health self-reporting, storing medical information, creating charts and reports for treatment, mood, and symptoms, reminder settings, links to educational materials from MSAA and connecting to healthcare providers to share the progress and reports. Similarly, SymTrac was designed to provide health self-reporting tool, which stores the data, reports, and shares the charts with healthcare providers (SymTrac 2014). MS self offers a journal, which is a functionality for self-reporting the moods, thoughts, and health data at one place that can be later easily accessed by the user and shared with the healthcare team. In addition, it provides helpful health-related information, and achievements for using the app (MS self – Multiple Sclerosis (MS) App 2015). My MS Conversations provides an interactive group session with experienced virtual patients on selected topics (My MS Conversations™ 2014). MS Journal is an injection reminder tool for individuals with MS and their caregivers limited to UK market only (MS Journal 2014). Social app MS Buddy (MS Buddy 2016) pairs individuals with MS with another person with MS to chat daily. My Multiple Sclerosis Diary (My Multiple Sclerosis Diary 2015) is another injection reminder mobile app that offers injection location and time set up. MS Attack app (Multiple Sclerosis Attack App 2014) helps users learn about MS symptoms, how these present themselves during the MS attack and provides a location of the UT MS Clinic and the Neuro Eye Center. MySidekick for MS (MySidekick for MS 2012) provides tips for living with MS, manages medicine with reminders, allows users record mood, energy level, activities, sensations, and memory and provides a daily overview, has an email feature that lets users send results to themselves or a caregiver, a memory exercise, a built-in step-tracking feature, and a list of suggested questions for a visit to a doctor.
Existing mobile applications for the individuals with MS were not tested with their end-user group, and there is no evidence that these interfaces meet the usability requirements of this specific population.
5 Methods
We hypothesized that salient features of the interfaces, such as font and button size, use of the spinner, navigation bar and similar, will either act as barriers or facilitators to usability for both groups of participants. These design elements will be used to provide recommendations for the design of apps for people aging with MS, as measured by the number and types of help requests, and further identified and categorized with interview questions.
5.1 Participants
Participants were recruited from the CATEA Consumer Network (CCN). A total number of 19 participants were recruited. The group of people diagnosed with multiple sclerosis at least 5 years ago (9 participants, all 9 women, 33–67 years old, mean age 51.11 ± 11.22 years) included participants with ranges of functional limitations. One of them reported no functional limitations, one had balance issues, three had dexterity problems, five had gait issues, one had fatigue, one had numbness in feet, three had mobility issues, one had some pain, three had cognitive issues, one had sensation of the left side of the body, one had vision problem, two of them had foot drop, one had tremors, one can use only one arm a little, and one had lower extremity weakness.
The group of older adults (10 participants, 6 female and 4 male, 65–77 years old, mean age 68.90 ± 3.90 years) consisted of seven participants without any functional limitations, two with mobility issues due to post-polio (they walk with the crutches, and use a power chair), and one with hip problem.
5.2 Test Prototype
In this study, we used an iPhone 6 to test a more realistic everyday use of the three mobile applications. The iPhone 6 has Retina HD display that is 4.7 inches in size with a 16:9 resolution of 1334 × 750 (326 ppi). Two MS health and wellness self-management mobile applications, My MS Manager and MS self, (See Figs. 2 and 3), and iHealth, an integrated mobile health app for the general population (See Fig. 4) were chosen for this study.

My MS Manager (My MS Manager™ 2012)

MS self (MS self – Multiple Sclerosis (MS) App 2015)

iHealth (iHealth 2012)
5.3 Procedure
Participants signed the informed consent form approved by the Georgia Tech Institutional Review Board. They completed a demographic background questionnaire and reported their functional limitations, rated the use of mobile, mobile health, and MS-specific applications, computer and touchscreen experience, and use of the accessibility features on their smartphones. Participants performed three sets of tasks on three chosen mobile interfaces (My MS Manager, MS self, and iHealth). The order of the mobile applications was counterbalanced and randomly assigned to each participant. They were asked to complete each task and ask for help when they cannot find a solution to finish the task. Participants answered a questionnaire rating the UI elements and two interview questions identifying the barriers and facilitators to usability following the completion of each set of tasks. The usability study was video recorded and lasted from 60 to 150 min, depending on the participant. All participants were compensated $20.00 for their time and $5 for the travel to Georgia Tech.
Use of Mobile Health and MS-Specific Apps.
The participants self-reported use of mobile, mobile health, and MS-specific applications ranging from often, frequently, occasionally, very infrequently, to never (See Tables 1 and 2).
Computer and Touch Screen Experience.
The participants self-reported their computer and touchscreen experience on a scale from 1 = none, 2 = novice, 3 = intermediate, 4 = advanced, to 5 = expert. The mean level of computer experience was different between the two groups: the people with MS group (M = 3.89, SD = 1.36), and the older adults group (M = 3.10, SD = 0.57). In addition, the mean of touchscreen experience was different between the two groups as well: the people with MS group (M = 3.67, SD = 0.87), and the group of seniors (M = 3.1, SD = 0.99).
Accessibility Features.
The participants reported the use of the accessibility features on their smartphones. The people with MS had seven participants that reported the use of large text size or zoom, five that used voice over, one that used high contrast or inverted colors, and one that used assistive touch. Out of the group of ten older adults, six reported use of large text size or zoom and one used voice over.
Tasks.
All participants performed three sets of tasks on My MS Manager, MS Self, and iHealth. The tasks on iHealth were short and simple, and therefore the number of tasks for this app increased to seven tasks. The first four tasks on My MS Manager and MS Self were the same (See Table 3). Task 1 (My MS Manager and MS self) will ask participants to open a Journal, create a new entry, fill out the entry with the prescribed data, and make another entry with a different set of data. The second entry will contain different data that require a slight change in navigation. Task 1 in iHealth will ask them to find and open Goals and populate the entry with the prescribed data. Task 2 (My MS Manager) will require participants to open two existing entries from the list. In MS self, they will open History from the Journal entry screen and from there open the two entries from the list. In iHealth task 2, they will find and open Reminder, create a new task and populate it with the prescribed data. Task 3 (My MS Manager) will request participants to open Charts, select a date range, filter chart data, and look up the two selected charts. In MS self, they will select a date range, filter data, generate a report, and look up the two reports. In iHealth task 3, they will navigate the interface to measure their blood pressure using the BPM. Task 4 (My MS Manager and MS self) will require them to open the function and skip it. In iHealth Task 4 they will find and open new manual entry, and populate it with the prescribed data. In task 5 (My MS Manager) they will open Treatments, create a new entry, and fill out the entry with the prescribed data. Task 5 in MS self will require them to Open Fact Cards and look up the Tips for Living Well. In iHealth, they will find the BP results list, delete the entry, and then decide to keep the entry.
Task 6 (iHealth) will ask them to find and look up BP trends and lists. In task 7 (iHealth) they will find and open My Diary, open lunch, search for the specific meal, select it, open activity, select a specific one, and set up time for practice. UI elements used in each task for all three mobile health applications are listed in Table 3.
5.4 Data Collection and Analysis
Effectiveness.
The task completion rates (i.e., the percentage of completed tasks) and the user success rate (i.e., the percentage of tasks completed correctly without asking for help) were recorded.
Participants were asked to complete each task and ask for help when they could not find the solution to finish the task. Counting help requests was used as a filter for errors, allowing only important errors to pass through. The number of times participants requested help was recorded, and the frequency of help requests was reported (i.e., the number of help requests divided by the number of participants per group). The researcher described each help request that occurred during the testing and recorded it as a specific problem. The help requests were coded based on their general nature (e.g., navigation, instructions, selection, etc.). Based on the number and frequency of these types of help requests, the weak points (i.e., barriers) of the interface were prioritized. The frequency of help requests by type of functional ability, depending on the ability required to perform the step, was reported as well.
The category of cognitive issues included the problems participants had with the Instructions, Navigation, Location, Spinner, Button active area, Selection, and Mistakes. Leveling the hand while using the blood pressure monitor (BPM) in iHealth was coded as Instructions since the interface provided the directions for measuring the blood pressure. Navigation issues included the following: adding the new task, going back and forth, skipping, deleting, generating the report, and updating the task. Location problems related to finding the specific features or sub-features, such as Goals and Reminder in iHealth, Achievements and Report in MS Self, Journal in both MS Self and My MS Manager, and similar. Problems with the use of the spinner were coded as Spinner. Adding a comment in MS Self and My MS Manager, pressing + to navigate, tapping to add, tapping >+ part of the button to navigate were coded as Button active area. Selecting mood and symptoms in MS Self, exacerbations and mood in My MS Manager, day rating in My MS Manager, charts in MS Self, disability level in My MS Manager, every day in iHealth, 90 days within the Chart feature in MS Self, as well as deselect any of the options were a part of the Selection problems. When participants did not enter required date, we coded that as a mistake. Problems with the touchscreen, tapping twice, unresponsive screen, and button size were coded as dexterity issues. Visual problems included issues with the contrast, which was mostly due to the very low contrast on “Done” button in iHealth app (See Table 4).
Barriers and Facilitators.
14 design elements were rated by the participants using the Likert scale from 1 = strongly disagree, to 5 = strongly agree. Two open-ended interview questions were used to further identify barriers and facilitators.
All the recorded video files (19 participants × 3 mobile health interfaces = 57 files) were used to confirm the nature of the specific problems participants encountered.
6 Results
All participants (n = 19) completed all three trials (3 mobile health interface designs × 19 participants = 57 completed trials). The total study time lasted from 1 to 2.5 h.
6.1 Effectiveness
Task completion rates for all participants and all tasks were 100%. Out of a total number of completed tasks (19 participants × 17 tasks = 323 tasks), 39 tasks (12.07%) were completed successfully without asking for help (i.e., the user success rate). 284 tasks (87.93%) required at least one help request (See Table 5). 1 participant with MS did not ask for help while performing all the tasks on all 3 apps, 1 participant with MS and 1 older adult did not request help while performing all the tasks on MS Self, and 1 older adult did not ask for help while completing the tasks on My MS Manager and iHealth apps.
Out of a total of 339 help requests, people with MS asked 112, and older adults 227 times for help. Help requests related to cognitive abilities accounted for a majority of problems, with 107 being asked by people with MS and 217 asked by older adults. There was only 1 help request by people with MS-related to dexterity problems, and 10 by older adults. Visual issues accounted for 4 help requests by people with MS, and none by older adults. Among the cognitive issues, the biggest number of help requests came from the problems with navigation and finding the interface features and sub-features for both groups of participants (See Table 5). The frequency of help requests allows for a comparison between the two groups of participants.
Overall, the largest number and frequency of help requests come from the problems with the navigation and locating the pages for both groups of participants.
6.2 Barriers and Facilitators
14 design elements were rated on a scale from 1 = strongly disagree, to 5 = strongly agree. Value 3 was inserted when the participants responded with n/a for the specific rating. The average rating was reported for all three apps and both user groups (See Tables 6 and 7).
Overall, MS Self had the highest ratings in both user groups, and seniors rated all three apps lower than the individuals with MS did. Main barriers identified by both user groups were the instructions, text size, and prompt messages. In addition, older adults identified a size of touch buttons, physical ease of use, single tap, color contrast, skipping content, icons, navigation, finding main menu, ease of use, touch buttons, swiping, and scrolling as barriers to usability.
Two interview questions confirmed the previous findings and identified additional barriers and facilitators (See Table 8).
Both groups of participants identified navigation, especially navigating back to a homepage, as a problem on all three apps. Both user groups had issues with finding the specific pages on iHealth and people with MS encountered this problem on My MS Manager. It was not evident when they completed the task, they needed additional instructions for using the apps, it was not clear if they saved an entry, and font and button sizes were too small for most of the users on all three apps. Older adults had problems with color contrast on all three interfaces, and issues with scrolling on iHealth and My MS Manager. Among the facilitators identified, the found emoticons on MS Self to be usable, color contrast on My MS Manager was good enough, MS Self and My MS Manager were found to be simple and intuitive to some users, and use of blood pressure cuff on iHealth was found to be very useful. In addition, among the barriers and facilitators identified, we found some design elements that were present in both categories. Moreover, there were some inconsistencies between the ratings of the design elements and the answers to the interview questions participants made. For example, both user groups rated highly how easy it was to understand when the task was completed, but when asked to identify the barriers to usability, individuals with MS reported task completion for all three apps, and seniors reported it for My MS Manager. We relied more on the answers to the interview questions because of the detailed explanations from the participants and the nature of the open-ended questions.
7 Conclusion
As individuals with MS age, they will experience the usability problems with mobile user interfaces that an aging population faces in addition to the issues they already have due to this chronic disease. Therefore, we identified the barriers and facilitators to usability that both groups of participants face, to develop recommendations for the design of mobile applications for individuals aging with MS.
7.1 Design Recommendations
From the findings from the frequency of help requests, the design elements ratings, and the interview questions, we summarized and prioritized the barriers and facilitators for both user groups, and drew the following main conclusions for recommendations for the design of mobile health and wellness applications for individuals aging with MS:
-
Navigation needs to be clear, intuitive, easy to understand, and consistent. Participants found hard to go back and forth from page to page because the way to navigate to different pages was not consistent (e.g., slide, hamburger menu, button, etc. were used randomly). One participant complained about the lack of next and back buttons. Several participants mentioned the lack of directions, instructions, and help to assist users with the navigation to specific pages within the interface and especially the homepage. Almost all participants had problems with the navigation back to the homepage. Fisk et al. (2009) recommended that navigation assistance (e.g. help, review buttons) should be provided for understanding how to navigate to specific points in the system. This includes navigation to not only the homepage but any relevant page. Moreover, seamless use should be provided to users with a back button, next button, and similar. Be consistent with the ways of the navigation from page to page. Provide more than one way to go to different pages while keeping the consistency.
-
Locating pages needs to be easy and intuitive. Many participants had problems with finding certain pages within the interface, especially in iHealth app. They had problems finding where to record all the entries and where to find the blood pressure monitor feature. Many participants had issues with finding the homepage from any other page. The researchers (Fisk et al. 2012) recommend organizing information within natural or consistent groupings (e.g. group related information and have most frequent operations highest on the menu structure) to allow a user to easily find needed piece of information and related page. Indicate clearly where the user currently is at any point in time. The sequences of actions should be available and visible in the interface, and the user should not be expected to remember them. Make it clear how to navigate to all main point of the interface from the homepage, and how to go back to homepage from any other page.
-
Task completion needs to be evident and bold so that users know they have accomplished their tasks and they can continue with the subsequent activities. Most of the participants had problems with the task completion because they did not get any feedback that their entries have been saved and that they have completed the entry successfully. Some participants even suggested that they should get a message saying “Saved” or similar. Users should be given the satisfaction of accomplishment and completion, a sense of relief, and an indicator to prepare for the next group of actions, no matter where they are (Shneiderman 1987). After users save any data, provide them with the information that their records have been saved and secured.
-
Provide specific and clear instructions for every step of the actions. Most of the participants had problems with the lack of instructions during their navigation and use of the interface. They wanted instructions that user can refer to when using the mobile applications. Some participants had problems with the existing instructions and wanted simplified directions with the use of icons, and instructions that are more evident. Researchers (Fisk et al. 2009) found that technical language used in instructions and help systems might be difficult for older adults as their educational attainment levels may be lower than that of younger adults. Reading level of text material needs to be kept at grade 10 or below. Provide clear and understandable instructions for every task that can be completed and allow users to disable these instructions.
-
Font, buttons, and icons size (screen characters and targets) should be large enough to be usable by the end-users. Screen characters and targets should be conspicuous and accessible (e.g., font size should be 12-point and higher, icons should be large enough to select easily) (Fisk et al. 2012). Use at least 12-point x-height serif or sans serif fonts (e.g., Arial, Helvetica, Times Roman), preferably 14-point and bigger (Kascak et al. 2013a, b). Avoid cursive and decorative fonts and use of all uppercase letters since it slows down reading. In mixed-case situations, uppercase text attracts more attention than lowercase ones. Buttons on the mobile touchscreen interfaces should be at least 9.6 mm diagonally (e.g., 44 × 44 pixels on iPad) (Parhi et al. 2006).
-
Color contrast needs to be very high to allow for ease of use and legibility of information. Many participants, especially older adults encountered problems with the color contrast, which was not high enough on some pages and when they had to select “Done” button on iHealth app. Researchers (Fisk et al. 2012) suggest providing at least 50:1 contrast (e.g. black text on white background). Make sure that color discriminations can be made easily by signaling important information using short wavelength (blue-violet-green) contrasts, using black on white or white on black text, avoiding colored and watermarked backgrounds for display of text (Fisk et al. 2012). At least the contrast ratio of 4.5:1, and preferably contrast ratio of 7:1 should be used, based on the WCAG 2.0 recommendations.
-
Avoid use of scrolling and spinner. Many participants experienced problems with scrolling, and especially with the spinner. The majority of older adults could not understand how to use the spinner, had problems to select with it and made similar mistakes from one spinner to the other one. Scrolling text should be avoided because it is difficult to process (Fisk et al. 2012). If necessary to use, use slow scrolling rate. Avoid use of the spinner. Replace it with the keyboard with large keypads.
8 Discussion
In this research project, we evaluated the usability of two current MS health and wellness self-management mobile applications and one health app for the general population to identify the effectiveness of app attributes and provide recommendations for the design of new mobile technologies for the target population.
Cognitive, vision and motor performance declines with age. The results of our study imply that seniors performed worse than individuals with MS. Thus, we recommend making mobile applications more usable by simplifying its design and considering this a vital factor for design and development of mobile applications for older adults and people aging with MS. In addition, we provided a set of the design recommendations to assist with the future development of health and wellness mobile interfaces for people aging with MS. These recommendations present the main considerations when designing for this specific population. The navigation, locating the homepage and other pages within the interface, task completion, instructions, appropriate size of the fonts, buttons, and icons, high color contrast, and avoiding the use of scrolling and the spinner represent the most important design elements that need to be considered for the development of mobile interfaces for population of people aging with MS.
References
Anthony, L., Kim, Y., Findlater, L.: Analyzing user-generated youtube videos to understand touchscreen use by people with motor impairments. Paper Presented at the Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (2013)
Bhachu, A.S., Hine, N., Arnott, J.: Technology devices for older adults to aid self management of chronic health conditions. Paper Presented at the Proceedings of the 10th International ACM SIGACCESS Conference on Computers and Accessibility (2008)
Dawe, M.: Understanding mobile phone requirements for young adults with cognitive disabilities. Paper Presented at the Proceedings of the 9th International ACM SIGACCESS Conference on Computers and Accessibility (2007)
Duff, S.N., Irwin, C.B., Skye, J.L., Sesto, M.E., Wiegmann, D.A.: The effect of disability and approach on touch screen performance during a number entry task. Paper Presented at the Proceedings of the Human Factors and Ergonomics Society Annual Meeting (2010)
Finlayson, M.: Health and social profile of older adults with MS: findings from three studies. Int. J. MS Care 4(3), 139–151 (2002)
Fisk, A.D., Rogers, W.A., Charness, N., Czaja, S.J., Sharit, J.: Designing for Older Adults: Principles and Creative Human Factors Approaches. CRC Press, Boca Raton (2009)
Fisk, A.D., Rogers, W.A., Charness, N., Czaja, S.J., Sharit, J.: Designing for Older Adults: Principles and Creative Human Factors Approaches. CRC Press, Boca Raton (2012)
Fleming, W.E., Pollak, C.P.: Sleep disorders in multiple sclerosis. Paper Presented at the Seminars in Neurology (2005)
Fraser, R., Johnson, E., Ehde, D., Bishop, M.: Patient self-management in multiple sclerosis. Consortium of Multiple Sclerosis Centers White Paper. CMSC, USA (2009)
Gulick, E.E.: Symptom and activities of daily living trajectory in multiple sclerosis: a 10-year study. Nurs. Res. 47(3), 137–146 (1998)
Holzinger, A., Searle, G., Nischelwitzer, A.: On some aspects of improving mobile applications for the elderly. In: Stephanidis, C. (ed.) UAHCI 2007. LNCS, vol. 4554, pp. 923–932. Springer, Heidelberg (2007). doi:10.1007/978-3-540-73279-2_103
Hurst, A., Hudson, S.E., Mankoff, J., Trewin, S.: Automatically detecting pointing performance. Paper Presented at the Proceedings of the 13th International Conference on Intelligent User Interfaces (2008)
iHealth (2012). https://ihealthlabs.com/. Accessed 3 Nov 2016
Irwin, C.B., Sesto, M.E.: Timing and accuracy of individuals with and without motor control disabilities completing a touch screen task. In: Stephanidis, C. (ed.) UAHCI 2009. LNCS, vol. 5615, pp. 535–536. Springer, Heidelberg (2009). doi:10.1007/978-3-642-02710-9_59
Irwin, C.B., Sesto, M.E.: Performance and touch characteristics of disabled and non-disabled participants during a reciprocal tapping task using touch screen technology. Appl. Ergon. 43(6), 1038–1043 (2012)
Kane, S.K., Bigham, J.P., Wobbrock, J.O.: Slide rule: making mobile touch screens accessible to blind people using multi-touch interaction techniques. Paper Presented at the Proceedings of the 10th International ACM SIGACCESS Conference on Computers and Accessibility (2008)
Kane, S.K., Jayant, C., Wobbrock, J.O., Ladner, R.E.: Freedom to roam: a study of mobile device adoption and accessibility for people with visual and motor disabilities. Paper Presented at the Proceedings of the 11th International ACM SIGACCESS Conference on Computers and Accessibility (2009)
Kascak, L., Rebola, C.B., Braunstein, R., Sanford, J.A.: Icon design to improve communication of health information to older adults. Commun. Des. Q. Rev. 2(1), 6–32 (2013a)
Kascak, L., Rébola, C.B., Braunstein, R., Sanford, J.A.: Icon design for user interface of remote patient monitoring mobile devices. Paper Presented at the Proceedings of the 31st ACM International Conference on Design of Communication (2013b)
Kurniawan, S.: Older people and mobile phones: a multi-method investigation. Int. J. Hum.-Comput. Stud. 66(12), 889–901 (2008)
Leonard, V.K., Jacko, J.A., Pizzimenti, J.J.: An exploratory investigation of handheld computer interaction for older adults with visual impairments. Paper Presented at the Proceedings of the 7th International ACM SIGACCESS Conference on Computers and Accessibility (2005)
McGookin, D., Brewster, S., Jiang, W.: Investigating touchscreen accessibility for people with visual impairments. Paper Presented at the Proceedings of the 5th Nordic Conference on Human-Computer Interaction: Building Bridges (2008)
Mertens, A., Jochems, N., Schlick, C.M., Dünnebacke, D., Dornberg, J.H.: Design pattern TRABING: touchscreen-based input technique for people affected by intention tremor. Paper Presented at the Proceedings of the 2nd ACM SIGCHI Symposium on Engineering Interactive Computing Systems (2010)
Minden, S.L., Frankel, D., Hadden, L.S., Srinath, K., Perloff, J.N.: Disability in elderly people with multiple sclerosis: an analysis of baseline data from the Sonya Slifka Longitudinal Multiple Sclerosis Study. NeuroRehabilitation 19(1), 55–67 (2004)
MS Buddy (2016). http://www.healthline.com/health/multiple-sclerosis/ms-buddy
MS Journal (2014). http://tensai-solutions.com/app/ms-journal/. Accessed 27 Oct 2014
MS self – Multiple Sclerosis (MS) App (2015). http://www.moveoverms.org/multiple-sclerosis-app-ms-self/
Multiple Sclerosis Attack App (2014). https://itunes.apple.com/us/app/multiple-sclerosis-attack/id883546897?mt=8
My MS Conversations™ (2014). https://play.google.com/store/apps/details?id=com.syandus.ms_patiented_01&hl=en. Accessed 29 Jun 2015
My MS Manager™ (2012). http://mymsaa.org/manage-your-ms/mobile/. Accessed 11 Dec 2014
My Multiple Sclerosis Diary (2015). https://play.google.com/store/apps/details?id=com.appxient.mymsdiary&hl=en
My Sidekick for MS (2012). https://www.abovems.com/. Accessed 2 June 2015
World Health Organization. Atlas: Multiple Sclerosis Resources in the World 2008 (2008)
Parhi, P., Karlson, A.K., Bederson, B.B.: Target size study for one-handed thumb use on small touchscreen devices. Paper Presented at the Proceedings of the 8th Conference on Human-Computer Interaction with Mobile Devices and Services (2006)
Plos, O., Buisine, S.: Universal design for mobile phones: a case study. Paper Presented at the CHI 2006 Extended Abstracts on Human Factors in Computing Systems (2006)
Shneiderman, B., Plaisant, C.: Designing the user interface: strategies for effective human-computer interaction. ACM SIGBIO Newsl. 9(1), 6 (1987). Addison-Wesley
Stern, M.: Aging with multiple sclerosis. Phys. Med. Rehabil. Clin. N. Am. 16(1), 219–234 (2005)
Stern, M., Sorkin, L., Milton, K., Sperber, K.: Aging with multiple sclerosis. Phys. Med. Rehabil. Clin. N. Am. 21(2), 403–417 (2010)
SymTrac (2014). http://www.symtrac.com/. Accessed April 2014
Tomioka, K., Kato, S., Mooney, A., Nussbaum, M., Smith-Jackson, T.: A study on accessibility of cellular phones for users with disabilities. Paper Presented at the Proceedings of Universal Design Japan Conference (2002)
Wacharamanotham, C., Hurtmanns, J., Mertens, A., Kronenbuerger, M., Schlick, C., Borchers, J.: Evaluating swabbing: a touchscreen input method for elderly users with tremor. Paper Presented at the Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (2011)
Watanabe, T., Miyagi, M., Minatani, K., Nagaoka, H.: A survey on the use of mobile phones by visually impaired persons in Japan. In: Miesenberger, K., Klaus, J., Zagler, W., Karshmer, A. (eds.) ICCHP 2008. LNCS, vol. 5105, pp. 1081–1084. Springer, Heidelberg (2008). doi:10.1007/978-3-540-70540-6_162
Zulman, D.M., Jenchura, E.C., Cohen, D.M., Lewis, E.T., Houston, T.K., Asch, S.M.: How can eHealth technology address challenges related to multimorbidity? Perspectives from patients with multiple chronic conditions. J. Gen. Intern. Med. 30(8), 1063–1070 (2015)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this paper
Cite this paper
Ruzic, L., Sanford, J.A. (2017). Usability of Mobile Consumer Applications for Individuals Aging with Multiple Sclerosis. In: Antona, M., Stephanidis, C. (eds) Universal Access in Human–Computer Interaction. Design and Development Approaches and Methods. UAHCI 2017. Lecture Notes in Computer Science(), vol 10277. Springer, Cham. https://doi.org/10.1007/978-3-319-58706-6_21
Download citation
DOI: https://doi.org/10.1007/978-3-319-58706-6_21
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-58705-9
Online ISBN: 978-3-319-58706-6
eBook Packages: Computer ScienceComputer Science (R0)