
Abstract
Emerging adulthood, viewed through the lens of life course health development, has the potential to be a very positive developmental stage with postindustrial societies giving adolescents and emerging adults a greater opportunity for choice and exploration but also greater challenges with greater educational and social role requirements. The loss of supports and structures offered by schools, families, and child- and family-oriented health and social services means that the emerging adult must rely more on his/her own resources in a less structured environment. This increased agency in the context of less structure is occurring as the human brain is still developing higher-level capacities such as executive functioning. The person-context interactions during EA are many and complex, leading to multiple different pathways through emerging adulthood. Those with sufficient economic and adult supports as well as personal resources and maturity will be more likely to choose well and embark on a positive trajectory during EA. Those lacking these resources, or those with physical and mental health or intellectual disabilities, may struggle during this period and experience a negative trajectory in the spheres of education, vocation, relationships, and health status. The life course health science of EA requires more detailed and deeper analysis of the relationship between family, peers, and societal supports and personal internal resources in order to help promote successful developmental trajectories during EA.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

1 Introduction to Emerging Adulthood
The path that individuals take from dependency in childhood to independence in adulthood is now a longer and more complicated one than at any other point in history (Arnett 2014). From the mid- to late twentieth century and extending into the twenty-first century, industrial societies have experienced a surge in the concept of individualism and increased salience of self-realization and personal expression (Arnett 1998). Moreover, we have seen a dramatic increase in the number of youth seeking post-high school education, which is required for success as the economy transitions from an industrial to an information-based economy (Rifkin 2011). However, stagnation of wages for low-skilled workers and the lack of work opportunities for youth and young adults, combined with the increased costs of education and independent living, have made the pathway to independence and adulthood prolonged, complex, and varied, creating a new stage in the life course that has been labeled emerging adulthood (EA). While not all life course or developmental scientists agree that emerging adulthood constitutes a new developmental stage , there is agreement that social and economic forces have prolonged entry into adulthood and with significant role and developmental challenges beyond the traditional adolescent years (Cote 2014).
At the beginning of this stage, 17–18 years of age, emerging adults are generally dependent, living with their parents or caretakers, beginning to engage in romantic relationships, and attending high school. At the end of this stage, mid- to late 20s, most emerging adults live independently, are in long-term relationships, and have clear career paths ahead of them. How they traverse this life stage is dependent upon the personal, family, and social resources they possess as they enter this stage of life, dynamic and reciprocal interaction between the emerging adult and their environment, and the supports they receive during this stage. The result is that there are many pathways that youth and young adults pursue through this stage to achieve stable adulthood. For example, 40% do not pursue post-high school education. While 60% entered college immediately after graduating high school, many drop out or interrupt their college education with periods of work. Some 33% in this stage remain unmarried; however, 67% of them achieve stable domestic partners. Importantly, only a minority of emerging adults are employed in full-time jobs, limiting the economic opportunities they experience (U.S. Census Bureau. American Community Survey 2006).
Emerging adulthood is considered to be the volitional years , as it offers the most opportunity for identity exploration in the areas of love, work, and worldviews (Arnett 2000). During this time, individuals begin to develop the characteristic qualities necessary for becoming self-sufficient, engage in mature, committed relationships, assume more adult roles and responsibilities, and obtain a level of education and training that sets the foundation for work during the adult years. Characterizing emerging adulthood as a stage in the life course has proven to be beneficial to explain the social, cognitive, and psychological development that occurs during this stage. Research demonstrating continued brain development into the late 20s provides further justification for viewing emerging adulthood as a stage in the life course (Spear 2000).
2 Conceptual Framework
The Life Course Health Development (LCHD) model posits that myriad factors (e.g., biological, psychological, cultural) on multiple levels (e.g., micro, meso, macro) interact simultaneously in a transactional fashion to influence an individual’s LCHD during each stage to determine a “health developmental” trajectory (see also Halfon and Forrest 2017). The Life Course Health Development (LCHD) model further posits that transitions and pivotal points in an individual’s life have the potential to influence and alter an individual’s developmental pathways. EA is a life stage characterized by changes in person-context cognitive, emotional, physical, and social domains, and the ultimate pathway achieved by the emerging adults during this stage is determined by the ongoing, dynamic, and reciprocal interactions between the individual and their environment. The degree of agency and role exploration that characterizes EA results in the potential for growth in intellectual and emotional functioning (Arnett 2000). EA represents a broad and diverse but fundamentally important area of consideration by virtue of the multiple avenues through which an individual’s developmental trajectories and outcomes may be influenced. Important developmental challenges during EA include the continued formation of identity and values, which occur in the midst of frequent changes in personal relationships, living arrangements, vocational and educational pursuits, and social roles (Shanahan 2000).
No stage in life, other than perhaps infancy, experiences such dynamic and complex changes on the personal, social, emotional, neuroanatomical, and developmental levels. For the 10 years between 18 and 28, the vast majority of emerging adults change living situation, change their primary relationships, complete education or vocational preparation, get married, have children, and transition from adolescent/dependent roles to adult/independent roles. This occurs during often volatile emotional, neurodevelopmental, and social development. Increasing agency occurs at the same time as decreasing institutional and family supports. The theoretical framework developed by Learner and others to create the positive youth development theory nicely explains how the developmental trajectories that emerge during the period of EA are dependent upon multiple influential, bidirectional, person-context coactions. Individuals during emerging adulthood act as co-developers of their own developmental pathways, adaptively responding to different biological, social, cultural, and physical environmental contexts that they influence and are also influenced by (Learner and Overton 2008). Successfully navigating the developmental challenges inherent in EA will likely, in large part, influence the developmental trajectory of adulthood because these challenges ultimately influence the important adult outcomes of independent living, committed intimate relationships, and vocational and educational achievement. Youth and young adults with chronic disease or disabilities face additional challenges (disease management, disease complications, limitations in opportunities, etc.) in the context of these multiple domains of growth and development, which impact their pathway through this stage.
The continued positive trajectory of the emerging adult’s mental health, identity formation, education achievement, social relationships, and other developmental areas is somewhat dependent on the degree to which there are matches or mismatches between the individual and his/her resources and the environmental challenges and supports . If the transition, such as school to work, provides a reasonable and developmentally appropriate challenge and the emerging adult successfully navigates that challenge, then the developmental trajectory of the emerging adult will be enhanced. In contrast, if the same transition lacks supports or is an inappropriate match for the emerging adult’s abilities (e.g., an inadequate vocational program for an emerging adult with a learning disorder or lack of support for chronic disease management) and the emerging adult experiences failure, then the developmental trajectory may be impaired, resulting in significantly less achievement or developmental progression across the lifespan. A major defining characteristic of the stage of EA is that contexts are changing significantly (family to independence or romantic relationships, school to work or disconnected state, dependent living to independent living arrangements). The changes are so significant that emerging adults need substantial supports to navigate the transition successfully. Emerging adults with disabilities or chronic health conditions require more support to maximize their potential development during EA (Table 1).
The above table outlines the seven principles of the Life Course Health Development framework. These principles can be applied to the stage of emerging adulthood in a limited fashion due to the limited research literature focused on this life stage. However, conceptually, using the seven principles to view the stage of emerging adulthood can be instructive and can lead to additional research questions (see end of this article). For example, Principle 5 states that health development expressions are malleable and enable and constrain health development pathways and plasticity. According to Bogin’s reserve capacity hypothesis, prolonged childhood into adolescence and perhaps emerging adulthood leads to greater biologic and social resilience in adulthood, which leads to enhanced fertility and greater longevity (Bogin 2013). Principle 4 states that health development is sensitive to life course timing and social structuring of the environment. As we described above, this is particularly true of emerging adulthood, where the interaction between age, personal development, and environment (peers, schools, social institutions, etc.) leads to multiple pathways to identify formation and academic and social achievement during this stage (Benson and Elder 2011; Benson et al. 2012).
Multiple factors can influence the life course during EA, including factors at the macro-level (historical and societal influences), meso-level (parent-child relationship, family environment, and socioeconomic status), and microlevel (individual cognitive, personality, and emotional development). The timing of these exposures during EA, which we consider a critical or sensitive period in the life course development, can significantly impact adult outcomes. For example, an emerging adult that engages in criminal activity and is convicted of a felony will suffer repercussions that will greatly diminish their chances of achieving success in relationships and work. In the sections that follow, we review the macro-, meso-, and microlevel influences occurring during EA for emerging adults generally. Next we explore the additional challenges faced by those with selected chronic health or developmental conditions including mental illness or substance abuse, diabetes, chronic renal failure, and autism, to serve as case studies of the increased complexity faced by emerging adults with chronic disease. Finally, we finish up with a set of questions and issues that are research priorities for developing an LCHD research agenda on the stage of emerging adulthood.
3 Macro-level Influences on the Trajectory of Emerging Adulthood
Emerging adulthood, like many other developmental stages, is a period in the life course that is culturally constructed and not universal (Arnett 1998, 2000). Thus, the very existence and trajectory of EA are dependent on macro-level societal expectations and influences. For many years, it was theorized that an individual transitioned from adolescence (which begins in puberty and ends in the late teens) into young adulthood. Over history and cross-culturally, the length of time during which an individual spends in adolescence has been determined by the age at which the person enters marriage or a committed relationship (Schlegel and Barry III 1991, Gilmore 1990). In fact, human life history posits that the life stage of adolescence came into existence about 75,000 years ago due to changes in human societies and cultures associated with pair bonding and living in large groups (Bogin 2013). So massive culture and reproductive change led to a change in life history with the addition of a new period of development. It is theorized by those promoting emerging adulthood as a new life stage that the same kind of massive cultural and reproductive change is happening once again and new social and cultural demands of adult life necessitate a longer and more complex prologue to adult life.
Although the functional outcome of EA, causing a delayed transition to adulthood, appears relatively novel, this practice of prolonging the transition to adulthood may be dated back to early modern English society from the 1500s to 1700s (Ben-Amos 1994). Similar to what generally occurs during EA today, individuals during that era took part in a “life cycle service ” between their late teens and 20s, wherein they would engage in developing important vocational skills (e.g., a trade or craft) and marriage was often postponed until the late 20s for both men and women; adult roles and responsibilities for individuals during that era were provided only gradually, as each individual acquired the desired character qualities deemed appropriate by society (Ben-Amos 1994). It was not until industrialization in America began to emerge in the nineteenth century that the concept of individualism developed and strengthened (Rotundo 1994). The twentieth century marked the first time that an individual could obtain and gain control over the resources that would allow them to choose the timing of major life events and personal expression was valued in society (Modell 1991).
As we move forward into the twenty-first century, individualism in contemporary postindustrial society continues to strengthen, while the age at which individuals marry continues to increase, and individuals increasingly seek to pursue other life course events (Modell 1991; Alwin 1988; Bellah et al. 2007). As a reflection of these trends, recent evidence indicates that contemporary postindustrial society considers marriage status of low importance in the determination of whether or not an individual has reached adulthood; rather, societies in developed countries appear to now consider the acquisition of certain character qualities as the most important indicator of having attained adulthood, the top three character qualities of which include (1) accepting responsibility for oneself, (2) making independent decisions, and (3) assuming financial independence – all of which emphasize an individual’s ability to be self-sufficient (Scheer et al. 1996; Greene et al. 1992; Arnett 1997, 1998).
4 Meso-level Influences of Life Trajectories During Emerging Adulthood
Earlier life experiences and family environment can impact one’s life trajectory from childhood through EA and into adulthood. Longitudinal studies that span early childhood through EA indicate that there is both continuity and discontinuity of healthy and unhealthy paths and outcomes. (Masten et al. 2006, 2005). In this section, we will be discussing the impact of the parent-child relationship, family environment, and other sociodemographic factors, such as socioeconomic status (SES) and its influence in EA.
4.1 Earlier Parent-Child Relationships
The quality of parent-child relationships during EA is, in large part, a function of the history of early parent-child attachment experiences. Attachment theory suggests that positive bonding with an emotionally available adult during early childhood facilitates the development of the child’s capacity to bond with others and respond to stressful events. A history of positive attachment experiences will ultimately provide a foundation for positive interactions with others and foster secure, lasting relationships in EA which subsequently influence the LCHD (Mikulincer M and Shaver PR 2009). whereas insecure attachments can result in mistrust or lack of security and reduced sense of self-efficacy and self-esteem. Simultaneously, social learning theory suggests that styles of family interactions learned in early and middle childhood are carried by emerging adults into adulthood (Whitbeck et al. 1994). Familiar patterns of interaction help individuals deal with new situations and have a significant influence on the emerging adult’s capacity to deal with the multiple changes that occur during EA. Alternatively, inadequate parenting, disrupted family bonds, and poverty are environmental risks for childhood-onset conduct, behavioral and emotional problems, and educational underachievement that can persist into adolescence and emerging adulthood (Moffit and Caspi 2001).
Adverse events experienced in childhood such as parental divorce or alcoholism or the experience of abuse are major risk factors for the leading causes of illness and death as well as poor quality of life in adults in the USA. Disruptions in the parent relationship (e.g., divorce) can have strong, negative effects on the parent-child relationship (Aquilino 1994) causing significant emotional impact throughout the life course. Parental divorce may influence the emerging adults’ ability to form stable romantic relationships and their decision to marry early or may undermine the emerging adult’s financial ability to attend college (Jacquet and Surra 2001, Cherlin et al. 1998).
Importantly, parental acceptance and support for independence have been linked to higher self-esteem, individualism, and feelings of worthiness among emerging adults (Ryan and Lynch 1989). Critical to the emerging adult’s achievement of independence are feeling connected, secure, understood, and loved in their families and having the willingness to call on parental resources for help in making choices in educational, relationship, living, and other changes that confront the emerging adult. Persistent connectedness to parents facilitates rather than undermines ongoing identity development in emerging adulthood (Grotevant and Cooper 1986; Ryan and Lynch 1989).
4.2 Childhood Socioeconomic Status
Socioeconomic status (SES), family supports, and the neighborhood environment all can contribute to the positive or negative life trajectory prior to and during EA (Galobardes et al. 2008; Gilman 2012; Gilman and Loucks 2012). Socioeconomic status has been identified as one of the most important health determinants throughout the life course (Miller et al. 2015). Low financial resources and all the other exposures that go along with poverty – poor schools, chaotic families, exposure to violence, and victimization – limit opportunities for growth or acquisition of other resources that enhance quality of life (Wadsworth et al. 2016; Kim et al. 2015).
In addition to being an important predictor of disease-specific morbidity and mortality in adulthood, early childhood poverty has been associated with lower adult educational attainment (Duncan and Brooks-Gunn 2000). Educational achievement has a major influence on the life trajectory, including financial stability and health in EA and onward throughout adulthood. Seventy percent of emerging adults who grow up in poverty delay enrollment in postsecondary education, in comparison to 40% who grow up in household of higher SES. Furthermore, research has indicated that individuals who delay enrollment past the age of 22 are less likely to ever enroll in postsecondary education and less likely to complete a degree (Feliciano and Ashtiani 2012). The result is that only 22% of young adults from low-income families earn college degrees, while 48% of young adults from higher-income families earn at least an associate’s degree. Earning a college education results in not only higher lifetime earnings but enhancement of multiple aspects of psychosocial development (Evans and Cassells 2014).
However, while SES has been found to be predictive of educational attainment, the impact of poverty can be mitigated by a number of factors such as individual characteristics of self-efficacy and hope . Students from poor families that have high self-efficacy and a similar concept of hope for educational attainment do equally as well in school as their higher SES peers (Osgood et al. 2005). Recent research by Dweck and colleagues indicates that students’ mindsets are critically linked to resilience and achievement and that they can be changed through brief interventions, leading to substantial increases in measures of resilience and achievement (Yeager and Dweck 2012). These studies suggest that in addition to SES, individual characteristics also have a large influence on outcomes of EA and that these characteristics can be influenced through individual interventions. Individual characteristics and development are discussed in the next section.
5 Microlevel Influences on the Trajectories During Emerging Adulthood
As discussed in previous sections, individualism and the qualities of character have become increasingly important in the transition to EA and ultimately reaching full adulthood in postindustrial, developed societies. Studies have shown that the ability to accept responsibility for one’s self, make independent decisions, and assume financial independence are the top three most important factors in becoming an adult (Arnett 2014). In order to achieve individualism and obtain these important qualities of character, one needs to reach some degree of cognitive and psychological maturity, as well as possess some level of resilience. These individual factors are discussed in this section.
5.1 Cognitive Development
One of the identified qualities of character that is important in EA and reaching full adulthood is independent decision-making. While the ability to make independent decisions is a reflection of one’s psychological and moral identity, it also has to do with cognitive maturity and the ability to weigh a variety of considerations before deciding on a choice. Recent neuroscience research indicates that brain development (particularly in the prefrontal cortex) continues well into the third decade of life, ultimately resulting in the integration and coordination of cognitions, emotion and action, and strategic executive control (Luciana et al. 2005). The continuous unfolding and acquisition of specific neurodevelopmental capacities during adolescences and EA influence the acquisition of goal directedness and future orientation that have been observed behaviorally during EA (Dahl 2004; Nelson et al. 2012; Nurmi 1999; Steinberg et al. 2006). As new capacities emerge, they are available to solve problems, delay gratification, and filter unnecessary input. With maturation of these skills, emerging adults are also more capable of reflecting on the influence of their environment and on their internal state, regulate their emotions, and use problem-solving skills to effectively compromise, which is important for the development of meaningful social interactions and personal relationships as well as in the work environment. These skills also support an emerging adult’s capacity for optimally interacting with the health-care system, managing their health-care needs, and making decisions that will influence their long-term health outcomes.
However, the preceding paragraph assumes that the individual has experienced optimal neurodevelopment up to the point that they enter the stage of EA. Studies have demonstrated that exposure to chronic stress during childhood (e.g., poverty) or experiencing adverse childhood events (e.g., child maltreatment, neglect, parental divorce, parental substance abuse) may cause detrimental impact to the developing brain. For example, repeated exposure to stressful events has been associated with structural differences in specific brain regions (i.e., amygdala, hippocampus, and prefrontal cortex), which are in turn associated with functional differences in learning, memory, and aspects of executive functioning. Furthermore, preliminary studies go on to suggest that there may be sensitive periods of brain development with increased susceptibility to the effects of stress and adverse events. These environmentally induced modulations in neurodevelopment can impact an individual’s cognitive development and their capacity to develop the necessary skills and relationships that will enable them to thrive.
An emerging adult, who has experienced chronic stress or adverse events earlier in childhood and adolescence and is cognitively immature, is more likely, through adverse interaction with their environment, to suffer secondary effects such as school failure, risky/impulsive behaviors, accidental injury, criminal activity, or substance misuse or overuse. These behaviors may in turn interfere with the ongoing development of an optimal pathway to adulthood. Feelings of isolation and rates of substance abuse in individuals often peak during this period as emerging adults are faced with the stresses of having to navigate societal structures that are not adequately informed or equipped to address the needs of an emerging adult population – all while their brains have yet to reach full maturation (Spear 2000). An impulsive emerging adult fueled by alcohol and despair is at high risk for suicide. It is thus apparent that multiple factors related to an individual’s cognitive and emotional development may intersect and interact to multiply the likelihood of adverse or positive health outcomes in EA. It is crucial for service providers to recognize the level of cognitive maturation an emerging adult possesses and tailor their interventions and supports based on this.
5.2 Identity Formation
Identity formation is a major developmental activity during EA. Identity development , occurs in a number of dimensions: (1) psychological dimension, or ego identity via a sense of temporal-spatial continuity and its concomitants; (2) the personal dimension, or a behavioral and character repertoire that differentiates the individuals; and (3) the social dimension, or recognized roles within a community. These components come together during the stage of identity formation (adolescence and EA) and stabilization (EA and young adulthood), and once the identity is considered stable, this is when a relatively firm sense of ego identity is developed, behavior and character become stabilized, and community-sanctioned roles are acquired (2002).
Identity formation during adolescence was thought to be a critical milestone in adolescence; however, it has been recognized that in certain societal contexts, identity formation continues beyond adolescence. In the postindustrial society, with the prolongation of educational and vocational attainment, prolongation of identity exploration in the three main areas of love, work, and worldviews into the 20s has become the norm. Identity formation is critical in EA, as it has direct implications on psychological and moral identity and in achieving the three qualities of character deemed as important in the transition to adulthood.
5.3 Resilience in Emerging Adulthood
Resilience is an individual’s capacity to adapt to change in healthy and flexible ways during stressful events (Catalano et al. 2004). Resilience can be measured in various ways, including internal adaption (e.g., well-being, happiness, or self-concept) or external adaption (academic achievement, relationship development) to adverse circumstances, such as how well a person navigates and achieves the developmental tasks presented by the external world (e.g., educational achievement, stable work/career, marriage, etc.). Resiliency in adolescence and young adulthood is higher among youth with higher intellectual resources, optimistic future orientation, the presence of caring relationships with positive adult role models, and opportunities to succeed and serve the community. Emerging adulthood is a particularly important stage in the life course to understand resilience because the important changes in functional capacity, educational achievement, and social roles are large and varied and have a significant influence on life course outcomes.
Key individual characteristics that predict resilience during EA are goal-directed motivation and planfulness about the future. In addition, adult support and mentorship are important factors that help promote resilience (Miller GE 2015; Masten et al. 2005; Arnett 2005). Furstenberg, Brooks-Gunn, and others studied young women who became pregnant during adolescence and found that a small proportion with positive adult relationships had dramatic change in trajectory for the better (Furstenberg 2002). Masten, studying a cohort of low-income youth (beginning at ages 8–12) over a 20-year period, found that a number of factors predict competence in EA including higher intellectual capacity, higher parenting quality, and higher SES (Masten and Coatsworth 1998). When they examined resilience between the 10- and 20-year follow-up, they found that youth doing well in EA was predicted from doing well 10 years earlier. In the context of high adversity, childhood IQ was particularly an important moderator and predictor of resilience. During EA, individuals who were doing well from high-adversity backgrounds had significant personal resources in intelligence and personal competence and a history of receiving high-quality parenting (Masten et al. 2004).
6 Trajectories During Emerging Adulthood for Emerging Adults with Chronic Health Condition
Chronic health conditions can significantly impact the developmental trajectory of emerging adults during this life stage. Many types of chronic conditions, including those that impact physical, intellectual, or emotional functioning, may undermine the assumption of adult roles by the emerging adult, undermine success in school, impair the transition to work, and make living independently more of a challenge. Eighteen percent of youth aged 12–17 in the USA are defined as having a special health-care need , meaning they have a chronic physical, medical, emotional, or developmental condition that requires a more intensive use of health-care and related services. Emerging adults with chronic conditions are at risk for a number of problems during transition to adulthood, including experiencing gaps in needed medical and related services and gaps in health insurance (Lotstein et al. 2008, Reiss et al. 2005). Below we review the impact of several specific chronic conditions on the growth trajectory during emerging adulthood.
6.1 Autism Spectrum Disorders (ASDs)
For youth with autism spectrum disorders (ASDs) and their families, the transition from adolescence to emerging adulthood is a time of uncertainty and loss of entitlement to many services that were available while in the public school system under the Individuals with Disabilities Education Act (IDEA). In comparison to childhood, young adults with autism often experience a dearth of appropriate supports and opportunities. Leaving high school is associated with deterioration in ASD symptom presentation, increase in maladaptive behaviors, and worsening family functioning (Taylor and Seltzer 2010, 2011a, b). Many persons with ASD are able to work successfully within the community (Garcia-Villamisar et al. 2000; Mawhood and Howlin 1999); however, the majority experience difficulty securing meaningful employment (Eaves and Ho 2008; Howlin et al. 2004; Newman et al. 2011). A recent study indicated that only 58% have ever worked for pay. In addition, it was found that only one in five individuals ever lived independently (Roux et al. 2015). Even among those employed, their jobs tended to be low level and low income (Cimera and Cowan 2009; Eaves and Ho 2008; Howlin et al. 2004). Jobs often ended prematurely because of social or behavioral difficulties or other work-related difficulties (Mawhood and Howlin 1999).
Young adults on the autism spectrum are reported to experience difficulties in assuming other important adult roles and responsibilities, including attaining postsecondary education and living independently (Roux et al. 2015). A number of studies (Billstedt et al. 2005; Gillespie-Lynch et al. 2012; Howlin et al. 2004) have found that having an IQ of around 70 seemed to be a critical cutoff point for better outcome (e.g., level of independence). A number of comorbid conditions can complicate the trajectory for youth with intellectual disability through adolescence and EA, such as seizure disorder, which substantially increase in prevalence from childhood through adolescence into adulthood. Adults with ASD and related conditions are more vulnerable to anxiety and depression which can require specific treatments (Skokauskas and Gallagher 2010; White et al. 2009). The majority of young adults with ASD remain dependent on parents for support in living, recreation, and occupational situations. The availability of appropriate resources, services, and supports for the individuals with ASD and their families is key for successful transition into adulthood and better outcomes throughout adult life. The following elements are important for high-quality transition services and associated with improved young adult outcomes: (1) individualized services that reflect the strengths of the individual, (2) positive career development and early work experiences, (3) collaboration and interagency involvement, (4) family supports and expectations, (5) fostering self-determination and independence, (6) social and employment-related skill instruction, and (7) establishment of job-related supports. Therefore, outcomes for emerging adults with ASD could be improved if social and institutional supports available through adolescence continued into adulthood.
6.2 Type 1 Diabetes Mellitus (DM)
The study of emerging adults with type 1 DM has elucidated the potential challenges facing emerging adults with diabetes and other chronic health conditions that have significant self-management burden. Emerging adults with type 1 diabetes face extensive behavioral demands in order to maintain their health, including the necessity for precisely scheduled daily insulin injections, blood glucose monitoring, dietary monitoring, regular physical exercise, and the management of DM-related complications. In early adulthood, frequent changes in roles, living situations, educational routines, jobs, friendships, and romantic relationships are common and can undermine the routines and the resolve needed to maintain metabolic control (Anderson and Wolpert 2004).
The developmental tasks of emerging adulthood may be at odds with maintaining the intensive self-care that is required of those with type 1 diabetes and vice versa. For example, the tasks of establishing autonomy and prevailing egocentrism may be associated with the emerging adult not wanting to follow medical advice or advice of his or her family (Masten et al. 1995). Heightened concern for peer acceptance or the establishment of intimate relationships is characteristic of this period of development. Emerging adults may be reluctant to admit to their significant others that they have type 1 diabetes or any other chronic condition that puts them at risk for being rejected (Madsen et al. 2002). Moreover, the major cognitive developmental milestone during the stage of emerging adulthood is the ability to think abstractly (Erikson 1994). Those who have not yet reached this developmental milestone may struggle with taking responsibility to maintain good disease management understanding the consequences of poor disease management. Lastly, increased rates of drinking, illicit drug use, or other high-risk behaviors may disrupt the emerging adults’ lifestyle and negatively impact self-care management of diabetes, resulting in (Madsen et al. 2002) lack of control of diabetes and the resulting physical and mental consequences of hypo- or hyperglycemia, which undermine emerging adults’ abilities to perform in school, maintain relationships, or keep employment.
As has been demonstrated in other chronic childhood conditions, the transition from pediatric- to adult-centered medical care for youth with DM is associated with a decline in DM control (Busse et al. 2007; Oeffinger et al. 2006). Adverse health-related outcomes documented in the young adult population with diabetes include a decline in disease self-care behaviors and an increased risk for diabetes-related complications (Bryden et al. 2001; Fredericks et al. 2010; Yeung et al. 2008). In addition, emerging adults with diabetes are at higher than average risk for psychosocial morbidity including social delays and isolation, impaired social competence, and emotional problems such as depression (Helgeson et al. 2007). As in the case in ASD, additional support for an emerging adult with DM during the transition to adult medical care has been shown to help decrease the adverse outcomes seen with usual practice. For example, DM transition programs that include introductions to new adult care providers or intensive care coordination have been found to be protective (Holmes-Walker et al. 2007).
6.3 Chronic Kidney Disease
Chronic kidney disease (CKD) is a condition characterized by disease progression, significant cardiovascular morbidity, growth failure, neurocognitive impairment, and impaired quality of life changes (Sarnak 2003; Copelovitch et al. 2011; Gerson et al. 2006; McKenna et al. 2006). CKD is divided into five stages based on glomerular filtration rate, with stage 1 being the mildest form and stage 5 the worst form, also called end-stage kidney disease (ESKD ), requiring renal replacement therapy (dialysis or transplant) (Hogg et al. 2003). The prevalence of pediatric CKD is unknown as it may be silent in early stages. The prevalence of pediatric ESKD is 15 cases per million population (Saran et al. 2015). African-Americans and Latinos are disproportionately affected by CKD in part due to a higher incidence of glomerular conditions (Ferris et al. 2006). While the 10-year survival for adolescent-onset ESKD is 80–85% (much higher than adult-onset ESKD patients), this still represents a 30-fold increase in mortality compared to the general US adolescent population. Survival is better for younger adolescents, males, Caucasians, Asians, and transplant recipients (2006). However, emerging adults with CKD achieve adult milestones (e.g., employment, marriage) less frequently than their healthy peers (Bartosh et al. 2003).
The burden of care directly correlates with the stage of CKD . Based on the mean number of unique medications , those with CKD stages 1–4 take 6.2 ± 4 of medications, those with peritoneal dialysis (CKD 5) take 8.5 ± 2 medications, those with kidney transplant (CKD 5) take 9.7 ± 4.2 medications, and those on hemodialysis (CKD 5) take 11.3 ± 2.1 (So et al. 2011). The complexity of care also include procedures such as self-catheterization several times per day, fluid and dietary restrictions, blood pressure measurements daily, and injections (erythropoiesis-stimulating agents once to thrice weekly, growth hormone daily, or insulin several times per day). The life course of pediatric-onset CKD-ESKD varies by etiology and age at onset of this condition, but once they reach ESKD, most patients share the same comorbidities (hypertension, anemia, acidosis, metabolic bone disease, and growth delay). Patients with greater level of CKD have a decreased sense of self-worth, perceive a poor future, and feel limited in their physical and psychosocial capacities to have the same potential and opportunity as their healthy peers.
While most children and adolescent patients with ESKD will receive a kidney transplant , they likely will experience dialysis prior to receiving an organ. The most common cause of kidney transplant rejection in adolescents and emerging adults is treatment nonadherence (Andreoni et al. 2013). Adherence among adolescents is compromised by poor understanding and poor consequence recognition leading to an inconsistent commitment to the treatment regimens. Once the kidney transplant is lost, patients return to dialysis and likely will not receive another kidney transplant for many years. As in adult patients, cardiovascular disease (CVD) accounts for a majority of deaths in patients with pediatric-onset CKD, but unlike adults, pediatric-onset CKD patients rarely demonstrate symptomatic atherosclerosis (Shroff et al. 2011). Lastly, survivors of pediatric-onset CKD are at greater risk for malignancies and posttransplant diabetes mellitus (Koukourgianni et al. 2010).
Patients who transfer to adult-focused services without transition preparation and support appear to be at greater risk to lose their kidney transplant (Watson 2000, 2005). The international societies of internal medicine and pediatric nephrology have published position statements and policies to promote health-care transition preparation (Watson 2005; Watson et al. 2011). Strategies to increase patient autonomy, health-care transition, and self-management are needed to achieve successful outcomes at the time of transfer to adult-focused providers.
6.4 Mental Health and Substance Use
Emerging adulthood is a time of increased experimentation with tobacco, drugs, and alcohol (Schulenberg et al. 2004; Schulenberg and Maggs 2002), increasing from rates of 12.2% in adolescence to 40.2% in young adulthood for cigarette smoking, from 10.7% to 41.9% for binge drinking, from 11.2% to 20.3% for illicit drug use, and from 2.6% to 14.9% for heavy alcohol use. While cigarette, alcohol, and drug use are normative during adolescence and emerging adulthood, a number of factors predict excessive use rather than experimentation including genetic (e.g., family history of alcohol abuse), biological (e.g., early puberty timing), family (e.g., low parental monitoring), school (e.g., low grade average, school failure), peer (e.g., peer substance use), and youth personality and psychopathology (e.g., depression) factors (Cicchetti 1999). However, the pattern of use/abuse of these substances is influenced by the experience during the stage of EA. For example, increasing responsibility, work, and marriage all are associated with decreased use of these substances (Masten et al. 1999; Bachman et al. 2014). Again, there is great heterogeneity in the trajectories followed by individuals with regard to substance use during this period, all influenced by the multiplicity of factors listed above.
Among young adults, 13.7% experience serious mental illness such as major depressive disorders, schizophrenia, and bipolar disorder (AmericanPsychiatricAssociation 2013). The neuropsychological pathology that has onset during EA has many of the predisposing factors related to family adversities, such as social disadvantage, divorce, dysfunctional parenting, multiple family changes/moves, and peer group choices. The expanded independence and self-reliance during EA may be difficult to handle for youth with preexisting emotional or social challenges or poor attachment. The decrease in supports from school or family during EA may be even further destabilizing, leading to increased emotional and interpersonal difficulties. Young people with serious mental health conditions have difficulty with impulse control and self-regulation (Walker and Gowen 2011). Their apparent immaturity reflects a delay in social and emotional development and undermines progress toward goals in education, relationships, independence in health, and health-care management.
Three-quarters of lifetime cases of mental, emotional, and behavioral disorders begin by age 24 (Kessler et al. 2005). In emerging adults with social, emotional, and behavioral disorders, much higher risk is associated with onset in early adolescence versus onset in late adolescence (Mofitt and Caspi 2001). Dysfunctional family environments and participation in deviant peer group increase the likelihood of early-onset delinquency followed by a long trajectory of social, emotional, and behavioral problems. Youth with later onset of social, emotional, and behavioral problems are more commonly from relatively healthy family backgrounds and more likely to desist from delinquency by age 23 (Roisman et al. 2004). Similar patterns can be seen for major psychiatric disorders such as depression, with early-onset mood disorders being representative of more severe recurrent forms of mood disorders arising from increased severity and complexity of family and biologic risk factors (Fergusson and Woodward 2002) and later-onset disorders reflecting lower levels of risk factors in childhood.
7 Protective and Risk Factors That Impact Emerging Adulthood
The supports, opportunities, and experiences that occur during the stage of EA greatly influence the ultimate outcome of this stage and the ensuing life trajectory into young adulthood. As discussed in this chapter, critical influences during EA include mentoring relationships, socioeconomic supports, and educational and vocational opportunities. Emerging adulthood typically is accompanied by an increase in agency/independence and decrease in social and institutional support (e.g., schools and family), such that most individuals have more choice in day-to-day activities and life decisions. This increase in choice may result in greater success which will likely contribute to well-being. However, increased freedom can result in poor choices (e.g., drug use, criminal activity) that have a negative impact on the developmental trajectory as well (Schulenberg and Maggs 2002; Schulenberg et al. 2004). For example, many relationships and other aspects of life are so unstable during EA that important and powerful negative experiences can occur such as date rape, school failure, and substance addiction. These experiences can have a lasting, if not lifetime, detrimental impact on the developmental and mental health trajectory of the emerging adult. Similarly, many potential powerful positive influences can occur during this period in life (e.g., marriage, educational achievement, mentoring) that can enhance the developmental and mental health trajectory. Therefore, experiences both distal (early childhood) and proximal (during emerging adulthood) can influence, either positively or negatively, the developmental and mental health trajectory of the emerging adult (Miller et al. 2015).
Practical supports during EA provided by families include financial support for education, transportation, independent living, health insurance, and other necessities. The primary determinant of parental support are the level of parental resources. Emerging adults with wealthier parents and those with fewer siblings receive more financial support for education (Steelman and Powell 1991). Divorced parents provide less financial support than parents with intact marriages (Cooney and Uhlenberg 1992). Support from families by parents and grandparents during EA is also provided in the form of guidance or advice, information, and emotional support. Parents of emerging adults may also help the emerging adult negotiate the health-care system, formulate and carry out educational and vocational goals, and acquire leases for apartments and even provide advice for intimate relationships. In short, continued social and financial connection to parents with adequate emotional and financial resources can be a very significant factor in the positive life trajectory during emerging adulthood (Aquilino 2005). Previous studies have found a high correlation between improved EA outcomes and adolescent hope in the future (Bennett 2014). Hope is a form of personal capital that protects youth from social, emotional, and behavioral disorders and correlates with and predicts the rates of many outcomes, including academic achievement, delay of initiation of early sexual activity, and lower likelihood of violent behavior. Hope requires a sense of self-efficacy and knowledge of alternate outcomes. Hope is reflected in adolescent and young adult goals as they reflect and make ongoing assessments of their current and future selves. Individual goals and aspirations relate to the sense of control an individual feels in relation to a particular domain.
Positive youth development (PYD) programs are approaches that provide supports to adolescents and emerging adults to achieve social, emotional, behavioral, and moral competence, foster self-efficacy, a clear and positive identity, and belief in the future; and reinforce pro-social norms (Catalano et al. 2004). Positive development approaches involve a paradigm shift from targeting the risk factors to enhancing the assets and protective factors. The emphasis on hope, empowerment, and well-being resonates with youth and mental health professionals. The PYD approach outlined above suggests that effective programs to support EA would include an individualized approach supporting young people to identify and move toward personally meaningful goals. This begins with envisioning a positive future identity (“Who do I want to become?”). Pursuing goals promotes a sense of purpose, and making progress toward those goals contributes to building feelings of efficacy, empowerment, and self-determination, enhancing the individual’s ability to act as the primary causal agent in pursuing personally meaningful goals (Silbereisen and Lerner 2007).
A PYD perspective further suggests that youth and emerging adults will benefit from learning specific strategies for increasing and maintaining interpersonal support from positive peers, family, providers, and people in the community (Guerra and Bradshaw 2008). Young people can learn specific steps and skills that can help them increase the quality and the extent of their interpersonal networks, as well as the amount of emotional, instrumental, and informational support available to them. Using a PYD perspective suggests that the development of assets is an important recovery-oriented outcome in and of themselves, as well as a mediator of longer-term outcomes related to education, employment, mental health, and general quality of life. Indeed, a review of the available research on community-based programs and interventions for EA reveals a common focus on personal asset building (Lerner 2014). Also consistent with the PYD perspective is that many of the programs and interventions include a focus on changing the meso-environment of youth so that it encourages young people to develop or express strengths and assets.
8 Services and Supports
As we better understand the limits of and issues related to EA, it is imperative that we review and revise policy and current social and medical services and supports so they optimally address the current and future needs of individuals during this life stage. Current medical, mental health, and social service delivery models are geared toward either child or adult populations. In other words, individuals generally seek child-serving services between the ages of 0 and 18, and they are subsequently transferred directly to adult-serving services. However, the various biobehavioral and sociocultural factors discussed above make this direct transition from child to adult-centered care ill-suited for optimally addressing the nuances and challenges that individuals may face during EA. For example, an adult-centered medical doctor may regularly treat patients with fixed habits and lifestyles, who may already suffer from a variety of chronic health conditions. However, many such chronic health conditions in adults represent a culmination of experiences from an individual’s earlier years, which may not yet be apparent during EA. It is thus strongly recommended that EA service providers reorient themselves using a prevention-based paradigm and familiarize themselves with the possible antecedents to social, emotional, and medical conditions so that they may make health-care or social service recommendations to minimize risk factors and to maximize strengths and assets to facilitate development along optimal health trajectories. EA presents a unique opportunity for service providers to intervene and influence an individual’s LCHD before significant social, emotional, and medical pathology fully develops, utilizing existing knowledge of the skills and capacities associated with EA to inform services and interventions.
In addition to training service providers to reorient their approach to care and become more sensitive to antecedents of chronic health conditions in adulthood, the multifactorial nature of the LCHD model suggests that it would be important for service providers to consider horizontal (i.e., cross sector) and longitudinal (i.e., across the lifespan) service integration. Specifically, the current model posits that myriad factors (e.g., biological, psychological, cultural) on multiple levels (e.g., micro, meso, macro) interact simultaneously in a transactional fashion to influence an individual’s LCHD and overall health trajectory. However, most current training models which emphasize specialization in their independent fields and opportunities for cross-disciplinary case conceptualization and collaboration with regard to service delivery – particularly with respect to preventive care, which may be of special importance when considering EA as a sensitive period of development – tend to be rare. Such specialization in service delivery may result in service fragmentation. Additionally, adult service providers generally do not work in tandem with child service providers as individuals transition from one care setting to the next, consequently resulting in potential gaps in service delivery and care, which may be exacerbated as individuals work to rebuild rapport with their new service providers. Moreover, health, mental health, social service, and education professionals rarely collaborate to create comprehensive models across the EA stage. Clearly, the current service delivery infrastructure does not adequately support the needs and challenges unique to emerging adult populations. It is thus important to recognize emerging adults as a unique population requiring additional and specialized skills of service providers and the creation of specific pathways for transition which support continuity of care.
The larger sociopolitical and cultural contexts may also facilitate or create challenges which impact service and intervention efforts directed at emerging adults. The majority of individuals in developed nations transitioning through EA, for instance, may be classified as “digital natives ,” individuals who have been brought up in environments where exposure to digital technology may be normative and who are therefore familiar with computers and the Internet. As emerging adults increasingly turn to digital and mobile solutions to support and enhance their daily routines, it behooves service providers to creatively explore ways of engaging emerging adult populations using technology. Use of social networks, such as Instagram, Twitter, and Facebook, to advance primary prevention efforts, increase awareness of public health issues, and provide basic health and psychological education affords service providers the opportunity to outreach to unprecedented numbers and populations. Use of text messaging may also be effective as a way of engaging with digital native emerging adult populations and promoting engagement and adherence by emerging adults or to promote youth development programs. Also, as service providers keep pace with technological advancements, they may even begin to explore novel methods of service delivery and intervention using digital or Internet-based platforms, which may increase “buy-in” and potentially preventive service utilization, among digitally native emerging adult populations. For example, service providers might potentially leverage the data that digitally native emerging adults might collect as part of the “quantified self” movement (e.g., pedometer information, weight, blood pressure, etc.) in an effort to inform their ongoing care efforts.
On the other hand, due to clinical billing practices and regulations , as well as patient privacy concerns and regulations (e.g., Health Insurance Portability and Accountability Act, HIPAA), current service delivery models often tend to operate in a fragmented and siloed fashion, which in turn may limit the ability of service providers to develop a holistic treatment plan to address each individual’s needs. Further complicating this fragmentation is the restricted access to health records once an individual turns 18 years of age, when parents who may have been primarily responsible for managing their child’s health-care needs no longer are able to access their child’s medical records (unless explicit permission is granted by the child, who is now an emerging adult). Depending on each family’s cultural context and the relationship between the emerging adult and his or her parents, this transition may be a cause for significant stress and/or strife between family members as they work to renegotiate previously familiar boundaries. Mothers of children with diabetes, for example, have indicated feeling increased stress as their children transitioned from pediatric to adult care, particularly if they perceived that their children were not managing their health-care condition as well as they had been when it was previously under greater parent control (Allen et al. 2011). Such stress might result in familial conflict and dysfunction which could subsequently interfere with the emerging adult’s willingness or ability to adequately access services. One potential solution to overcoming the issue of patient privacy may be to implement public health programs and tools to educate and empower individuals with respect to managing and taking an active role in their own care. However, it is important to underscore the need for larger, overall systems to change in order to support service providers in working together with individuals and their families to ensure continuity and comprehensiveness of services and health-related information during the transition.
Finally, the implementation of health-care policies may have important implications for service and intervention delivery with an emerging adult population. With the introduction of the Patient Protection and Affordable Care Act of 2010 (ACA), for example, individuals may now remain on their parents’ health insurance plans until they turn 26 years of age. While this theoretically affords emerging adults the opportunity to develop the necessary skills for interacting with the health-care system and managing their own care, research indicates that emerging adults frequently perceived themselves as being at lower risk for health problems and the financial burden of health insurance as lacking in value. Consequently, emerging adults may opt for high-deductible catastrophic insurance which generally costs less compared to other health insurance plans, but translates to fewer opportunities for interaction with the health service sector and fewer opportunities for service providers to intervene early during an individual’s LCHD trajectory prior to the onset of chronic adult disease. Importantly, research indicates that despite preventive maintenance health visits being mandatory under the ACA, emerging adults were less likely to request health maintenance visits. Thus, it may be important for public health efforts to determine the underlying factors associated with this diminished utilization of health services by emerging adults and subsequently develop health literacy programs to promote prevention mindedness and service utilization in emerging adults.
9 Recommendations for Research Priorities
The following is a list of issues in life course research that are critical for better understanding the positive supports and challenges that influence the trajectory of development of emerging adults organized along the macro-, meso-, micro-framework.
Macro Issues
-
What community supports in emerging adulthood enhance health development into adulthood and improve outcomes for an emerging adult with specific health, mental health, and developmental conditions? Is there an “early intervention model” to optimize outcomes for EA? What model should be used for an emerging adult with chronic health, mental health, and developmental conditions?
-
What are the historical, economic, and cultural influences on the meaning of EA, adaption, and maladaptation to the stage and expectations for normative transitions? How have these changed over time? How are they different for an emerging adult with social, health, mental health, and developmental problems?
-
How have the delays in marriage/relationship commitment impacted adult life trajectories?
-
What are the racial and ethnic differences for how these factors interact to support development during EA?
-
How has the information economy and the increased demands for education impacted the life course for youth in upper, middle, and lower socioeconomic strata? Are there regional variations in these outcomes and how can they be improved?
Meso Issues
-
Earlier childhood development and family environment are predictors of adult outcomes, but it is unclear how optimizing health development can be achieved with supports during EA.
-
What is the interaction between health and social system supports, family supports, youth abilities, cognitive and psychological maturity, and EA outcomes for an emerging adult with and without mental or physical disabilities?
-
How can the different support systems be integrated to provide seamless services to youth and emerging adults with significant physical, mental health, or intellectual disabilities?
-
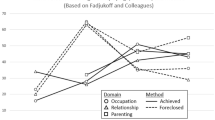
Using the model below from the work of Masten et al. (2005), how do these different resources, supports, and personal characteristics interact to promote optimal development during EA? (Fig. 1)
Fig. 1 
Moving toward resilience : a model of positive change in emerging adulthood

-
What factors promote resilience for youth during EA who lack family supports?
-
What is the role of extended families in support for EA?
-
How can studies of conditions and processes that influence development during EA inform educational/vocational/EA support policies?
-
How can data be gathered across this stage in the lifespan given that emerging adults leave school and have many changes in living arrangements, education, relationships, and work?
Micro Issues
-
To what degree is cognitive, social, physical, moral, and spiritual development mediated during emerging adulthood? How are these developmental pathways impacted by chronic health, mental health, and developmental conditions?
-
How can we optimize the person-context match to promote development during EA with and without chronic health, mental health, and developmental conditions?
-
What is the impact of positive turning points in EA compared to early life stages on life trajectories into adulthood?
-
During EA, exploration of new experiences is normative. Is more exploration better or worse and for which activities is it better or worse? How is this equation different for an emerging adult with chronic health, mental health, and developmental conditions?
-
Do emerging adults with particular health conditions, such as diabetes, spina bifida, solid organ transplant, or cancer survivorship, experience sharply downward trajectories during EA, and what supports are effective to prevent these sharply downward trajectories?
-
How does brain development progress during EA? What is the impact of brain development on the factors that influence the developmental trajectory during EA such as executive control (planfulness, future orientation), motivation, self-efficacy, and hope?
References
Allen, D., Channon, S., Lowes, L., Atwell, C., & Lane, C. (2011). Behind the scenes: The changing roles of parents in the transition from child to adult diabetes service. Diabetic Medicine, 28(8), 994–1000.
Alwin, D. F. (1988). From obedience to autonomy changes in traits desired in children, 1924–1978. Public Opinion Quarterly, 52, 33–52.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. Arlington: American Psychiatric Publishing.
Anderson, B. J., & Wolpert, H. A. (2004). A developmental perspective on the challenges of diabetes education and care during the young adult period. Patient Education and Counseling, 53, 347–352.
Andreoni, K. A., Forbes, R., Andreoni, R. M., Phillips, G., Stewart, H., & Ferris, M. (2013). Age-related kidney transplant outcomes: Health disparities amplified in adolescence. JAMA Internal Medicine, 173, 1524–1532.
Aquilino, W. S. (1994). Impact of childhood family disruption on young Adults’ relationships with parents. Journal of Marriage and the Family, 56, 295–313.
Aquilino, W. S. (2005). Impact of family structure on parental attitudes toward the economic support of adult children over the transition to adulthood. Journal of Family Issues, 26, 143–167.
Arnett, J. J. (1997). Young People’s conceptions of the transition to adulthood. Youth & Society, 29, 3–23.
Arnett, J. J. (1998). Learning to stand alone: The contemporary American transition to adulthood in cultural and historical context. Human Development, 41, 295–315.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55, 469.
Arnett, J. J. (2005). The developmental context of substance use in emerging adulthood. Journal of Drug Issues, 35, 235–254.
Arnett, J. J. (2014). Emerging adulthood: The winding road from the late teens through the twenties. New York: Oxford University Press.
Bachman, J. G., O’malley, P. M., Schulenberg, J. E., Johnston, L. D., Bryant, A. L., & Merline, A. C. (2014). The decline of substance use in young adulthood: Changes in social activities, roles, and beliefs. New York: Psychology Press.
Bartosh, S. M., Leverson, G., Robillard, D., & Sollinger, H. W. (2003). Long-term outcomes in pediatric renal transplant recipients who survive into adulthood. Transplantation, 76, 1195–1200.
Bellah, E. R. N., Bellah, R. N., Tipton, S. M., Sullivan, W. M., Madsen, R., Swidler, A., Sullivan, W. M., & Tipton, S. M. (2007). Habits of the heart: Individualism and commitment in American life. Berkeley: University of California Press.
Ben-Amos, I. K. (1994). Adolescence and youth in early modern England. New Haven: Yale University Press.
Bennett, A. (2014). Finding hope in hopeless environments. International Journal of Child Health And Human Development, 7, 313.
Benson, J. E., & Elder, G. H. (2011). Young adult identities and their pathways: A developmental and life course model. Developmental Psychology, 47, 1646–1657.
Benson, J. E., Johnson, M. K., & Elder, G. H. (2012). The implications of adult identity for educational and work attainment in young adulthood. Developmental Psychology, 48(6), 1752.
Billstedt, E., Gillberg, C., & Gillberg, C. (2005). Autism after adolescence: Population-based 13-to 22-year follow-up study of 120 individuals with autism diagnosed in childhood. Journal of Autism and Developmental Disorders, 35, 351–360.
Bogin, B. (2013). Chapter 2, Childhood, adolescence and longevity: A chapter on human Evolutionary life history. In B. Hewlett (Ed.), Adolescent identify: Evolutionary, cultural and developmental perspectives. New York: Routledge.
Brody, G. H., et al. (2013). Is resilience only skin deep? Rural African Americans’ socioeconomic status–related risk and competence in preadolescence and psychological adjustment and Allostatic load at age 19. Psychological Science. doi:10.1177/0956797612471954.
Bryden, K. S., Peveler, R. C., Stein, A., Neil, A., Mayou, R. A., & Dunger, D. B. (2001). Clinical and psychological course of diabetes from adolescence to young adulthood a longitudinal cohort study. Diabetes Care, 24, 1536–1540.
Busse, F., Hiermann, P., Galler, A., Stumvoll, M., Wiessner, T., Kiess, W., & Kapellen, T. (2007). Evaluation of patients’ opinion and metabolic control after transfer of young adults with type 1 diabetes from a pediatric diabetes clinic to adult care. Hormone Research in Pædiatrics, 67, 132–138.
Catalano, R. F., Berglund, M. L., Ryan, J. A., Lonczak, H. S., & Hawkins, J. D. (2004). Positive youth development in the United States: Research findings on evaluations of positive youth development programs. The Annals of the American Academy of Political and Social Science, 591, 98–124.
Cherlin, A. J., Chase-Lansdale, P. L., & Mcrae, C. (1998). Effects of parental divorce on mental health throughout the life course. American Sociological Review, 63(2), 239–249.
Cicchetti, D., et al. (1999). A developmental psychopathology perspective on drug abuse. Drug abuse: Origins & interventions (pp. 97–117). Washington, DC: American Psychological Association, xxiii, 492 pp.
Cimera, R. E., & Cowan, R. J. (2009). The costs of services and employment outcomes achieved by adults with autism in the us. Autism, 13, 285–302.
Cooney, T. M., & Uhlenberg, P. (1992). Support from parents over the life course: The adult Child's perspective. Social Forces, 71, 63–84.
Copelovitch, L., Warady, B. A., & Furth, S. L. (2011). Insights from the chronic kidney disease in children (Ckid) study. Clinical Journal of the American Society of Nephrology, 6, 2047–2053.
Cote, J. E. (2014). The dangerous myth of emerging adulthood: An evidence-based critique of a flawed developmental theory. Applied Developmental Science, 18(4), 177–188.
Dahl, R. E. (2004). Adolescent brain development: A period of vulnerabilities and opportunities. Keynote address. Annals of the New York Academy of Sciences, 1021, 1–22.
Duncan, G. J., & Brooks-Gunn, J. (2000). Family poverty, welfare reform, and child development. Child Development, 71, 188–196.
Eaves, L. C., & Ho, H. H. (2008). Young adult outcome of autism Spectrum disorders. Journal of Autism and Developmental Disorders, 38, 739–747.
Erikson, E. H. (1994). Identity: Youth and crisis. New York: Ww Norton & Company.
Evans, G. W., & Cassells, R. C. (2014). Childhood poverty, cumulative risk exposure, and mental health in emerging adults. Clinical Psychological Science, 2(3), 287–296.
Feliciano, C., & Ashtiani, M. (2012). Postsecondary educational pathways of low-income youth: An analysis of add health data. Irvine: Uc/Accord.
Fergusson, D. M., & Woodward, L. J. (2002). Mental health, educational, and social role outcomes of adolescents with depression. Archives of General Psychiatry, 59, 225–231.
Ferris, M. E., Gipson, D. S., Kimmel, P. L., & Eggers, P. W. (2006). Trends in treatment and outcomes of survival of adolescents initiating end-stage renal disease care in the United States of America. Pediatric Nephrology, 21, 1020–1026.
Fredericks, E. M., Dore-Stites, D., Well, A., Magee, J. C., Freed, G. L., Shieck, V., & James Lopez, M. (2010). Assessment of transition readiness skills and adherence in pediatric liver transplant recipients. Pediatric Transplantation, 14, 944–953.
Furstenberg, F. F. (2002). How it takes thirty years to do a study. In Looking at lives: American longitudinal studies of the twentieth century (pp. 37–57).
Galobardes, B., Lynch, J. W., & Smith, G. D. (2008). Is the Association between childhood socioeconomic circumstances and cause-specific mortality established? Update of a systematic review. Journal of Epidemiology and Community Health, 62, 387–390.
Garcia-Villamisar, D., Ross, D., & Wehman, P. (2000). Clinical differential analysis of persons with autism in a work setting: A follow-up study. Journal Of Vocational Rehabilitation, 14, 183–185.
Gerson, A. C., Butler, R., Moxey-Mims, M., Wentz, A., Shinnar, S., Lande, M. B., Mendley, S. R., Warady, B. A., Furth, S. L., & Hooper, S. R. (2006). Neurocognitive outcomes in children with chronic kidney disease: Current findings and contemporary endeavors. Mental Retardation and Developmental Disabilities Research Reviews, 12(3), 208–215.
Gillespie-Lynch, K., Sepeta, L., Wang, Y., Marshall, S., Gomez, L., Sigman, M., & Hutman, T. (2012). Early childhood predictors of the social competence of adults with autism. Journal of Autism and Developmental Disorders, 42, 161–174.
Gilman, S. E. (2012). The successes and challenges of life course Epidemiology: A commentary on Gibb, Fergusson and Horwood (2012). Social Science & Medicine, 75, 2124–2128.
Gilman, S. E., & Loucks, E. B. (2012). Invited commentary: Does the childhood environment influence the Association between every X and every Y in adulthood? American Journal of Epidemiology, 176, 684–688.
Gilmore, D. D. (1990). Manhood in the making: Cultural concepts of masculinity. New Haven: Yale University Press.
Greene, A., Wheatley, S. M., & Aldava, J. F. (1992). Stages on Life’s way Adolescents’ implicit theories of the life course. Journal of Adolescent Research, 7, 364–381.
Grotevant, H. D., & Cooper, C. R. (1986). Individuation in family relationships. Human Development, 29, 82–100.
Guerra, N. G., & Bradshaw, C. P. (2008). Linking the prevention of problem behaviors and positive youth development: Core competencies for positive youth development and risk prevention. New Directions for Child and Adolescent Development, 2008, 1–17.
Halfon, N., & Forrest, C. B. (2017). The emerging theoretical framework of life course health development. In N. Halfon, C. B. Forrest, R. M. Lerner, & E. Faustman (Eds.), Handbook of life course health-development science. Cham: Springer.
Helgeson, V. S., Snyder, P. R., Escobar, O., Siminerio, L., & Becker, D. (2007). Comparison of adolescents with and without diabetes on indices of psychosocial functioning for three years. Journal of Pediatric Psychology, 32, 794–806.
Hogg, R. J., Furth, S., Lemley, K. V., Portman, R., Schwartz, G. J., Coresh, J., Balk, E., Lau, J., Levin, A., & Kausz, A. T. (2003). National Kidney Foundation’s kidney disease outcomes quality initiative clinical practice guidelines for chronic kidney disease in children and adolescents: Evaluation, classification, and stratification. Pediatrics, 111, 1416–1421.
Holmes-Walker, D., Llewellyn, A., & Farrell, K. (2007). A transition care Programme which improves diabetes control and reduces hospital admission rates in young adults with type 1 diabetes aged 15–25 years. Diabetic Medicine, 24, 764–769.
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry, 45, 212–229.
Jacquet, S. E., & Surra, C. A. (2001). Parental divorce and premarital couples: Commitment and other relationship characteristics. Journal of Marriage and Family, 63, 627–638.
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of Dsm-iv disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 593–602.
Kim, P., Neuendorf, C., Bianco, H., & Evans, G. W. (2015). Exposure to childhood poverty and mental health symptomatology in adolescence: A role of coping strategies. Stress and Health, 32, 494–502.
Koukourgianni, F., Harambat, J., Ranchin, B., Euvrard, S., Bouvier, R., Liutkus, A., & Cochat, P. (2010). Malignancy incidence after renal transplantation in children: A 20-year single-Centre experience. Nephrology Dialysis Transplantation, 25, 611–616.
Lerner, R. M. (2014). Developmental science, developmental systems, and contemporary theories of human development. In Handbook of child psychology. New York: Wiley and Sons.
Lotstein, D. S., Inkelas, M., Hays, R. D., Halfon, N., & Brook, R. (2008). Access to care for youth with special health care needs in the transition to adulthood. Journal of Adolescent Health, 43, 23–29.
Luciana, M., Conklin, H. M., Hooper, C. J., & Yarger, R. S. (2005). The development of nonverbal working memory and executive control processes in adolescents. Child Development, 76, 697–712.
Madsen, S. D., Roisman, G. I., & Collins, W. A. (2002). The intersection of adolescent development and intensive intervention: Age-related psychosocial correlates of treatment regimens in the diabetes control and complication trial. Journal of Pediatric Psychology, 27, 451–459.
Masten, A. S., & Coatsworth, J. D. (1998). The development of competence in favorable and unfavorable environments: Lessons from research on successful children. American Psychologist, 53, 205.
Masten, A. S., Coatsworth, J. D., Neemann, J., Gest, S. D., Tellegen, A., & Garmezy, N. (1995). The structure and coherence of competence from childhood through adolescence. Child Development, 66, 1635–1659.
Masten, A. S., Hubbard, J. J., Gest, S. D., Tellegen, A., Garmezy, N., & Ramirez, M. (1999). Competence in the context of adversity: Pathways to resilience and maladaptation from childhood to late adolescence. Development and Psychopathology, 11, 143–169.
Masten, A. S., Burt, K. B., Roisman, G. I., Obradovic, J., Long, J. D., & Tellegen, A. (2004). Resources and resilience in the transition to adulthood: Continuity and change. Development and Psychopathology, 16, 1071–1094.
Masten, A. S., Roisman, G. I., Long, J. D., Burt, K. B., Obradović, J., Riley, J. R., Boelcke-Stennes, K., & Tellegen, A. (2005). Developmental cascades: Linking academic achievement and externalizing and internalizing symptoms over 20 years. Developmental Psychology, 41, 733.
Masten, A. S., Burt, K. B., & Coatsworth, J. D. (2006). Competence and psychopathology in development. D. Cicchetti, C. Dante, & J. Donald (Eds). Developmental psychopathology: Risk, disorder, and adaptation (Vol. 3, 2nd ed., pp. 696–738). Hoboken: John Wiley & Sons Inc, xvi 944 pp.
Mawhood, L., & Howlin, P. (1999). The outcome of a supported employment scheme for high-functioning adults with autism or Asperger syndrome. Autism, 3, 229–254.
Mckenna, A. M., Keating, L. E., Vigneux, A., Stevens, S., Williams, A., & Geary, D. F. (2006). Quality of life in children with chronic kidney disease—Patient and caregiver assessments. Nephrology Dialysis Transplantation, 21, 1899–1905.
Mikulincer, M., & Shaver, P. R. (2009). The attachment and behavioral systems perspective on social support. Journal of Social and Personal Relationships, 26(1), 7–19.
Miller, G. E., Yu, T., Chen, E., & Brody, G. H. (2015 Aug 18). Self-control forecasts better psychosocial outcomes but faster epigenetic aging in low-Ses youth. Proceedings Of The National Academy Of Sciences., 112(33), 10325–10330.
Modell, J. (1991). Into One’s own: From youth to adulthood in the United States, 1920–1975. Berkeley: University of California Press.
Moffitt, T. E., & Caspi, A. (2001). Childhood predictors differentiate life-course persistent and adolescence-limited antisocial pathways among males and females. Devcelopment and Psychopathology, 13, 355–375.
Nelson, C. A., Thomas, K. M., & De Haan, M. (2012). Neuroscience of cognitive development: The role of experience and the developing brain. Hoboken: John Wiley & Sons.
Newman, L., Wagner, M., Knokey, A.-M., Marder, C., Nagle, K., Shaver, D., & Wei, X. (2011). The post-high school outcomes of young adults with disabilities up to 8 years after high school: A Report from the National Longitudinal Transition Study-2 (Nlts2). Ncser 2011–3005. Washington, DC: National Center For Special Education Research.
Nurmi, J.-E. (1999). 15 self-definition and mental health during adolescence and young adulthood. In J. Schulenberg, J. L. Maggs, & K. Hurrelmann (Eds.), Health risks and developmental transitions during adolescence (p. 395). New York: Cambridge University Press.
Oeffinger, K. C., Mertens, A. C., Sklar, C. A., Kawashima, T., Hudson, M. M., Meadows, A. T., Friedman, D. L., Marina, N., Hobbie, W., & Kadan-Lottick, N. S. (2006). Chronic health conditions in adult survivors of childhood cancer. New England Journal of Medicine, 355, 1572–1582.
Osgood, D. W., Ruth, G., Eccles, J. S., Jacobs, J. E. & Barber, B. L. (2005). Six paths to adulthood: Fast starters, parents without careers, educated partners, educated singles, working singles, and slow starters. na.
Reiss, J. G., Gibson, R. W., & Walker, L. R. (2005). Health care transition: Youth, family, and provider perspectives. Pediatrics, 115, 112–120.
Rifkin, J. (2011). The Thired industrial revolution. New York: St. Martin’s Press.
Roisman, G. I., Aguilar, B., & Egeland, B. (2004). Antisocial behavior in the transition to adulthood: The independent and interactive roles of developmental history and emerging developmental tasks. Development and Psychopathology, 16, 857–871.
Rotundo, E. A. (1994). American manhood: Transformations in masculinity from the revolution to the modern era. New York: Basic Books.
Roux, A. M., Shattuck, P. T., Rast, J. E., Rava, J. A., & Anderson, K.,. A. (2015). National autism indicators report: Transition into young adulthood. Philadelphia: Life Course Outcomes Research Program/A.J. Drexel Autism Institute/Drexel University.
Ryan, R. M., & Lynch, J. H. (1989). Emotional autonomy versus detachment: Revisiting the vicissitudes of adolescence and young adulthood. Child Development, 60(2), 340–356.
Saran, R., Li, Y., Robinson, B., Ayanian, J., Balkrishnan, R., Bragg-Gresham, J., Chen, J., Cope, E., Gipson, D., & He, K. (2015). US renal data system 2014 annual data Report: Epidemiology of kidney disease in the United States. American Journal of Kidney Diseases: The Official Journal of the National Kidney Foundation, 65, A7.
Sarnak, M. J. (2003). Cardiovascular complications in chronic kidney disease. American Journal of Kidney Diseases, 41, 11–17.
Scheer, S. D., Unger, D. G., & Brown, M. B. (1996). Adolescents becoming adults: Attributes for adulthood. Adolescence, 31, 127.
Schlegel, A., & Barry Iii, H. (1991). Adolescence: An anthropological inquiry. New York: Free Press.
Schulenberg, J. E., & Maggs, J. L. (2002). A developmental perspective on alcohol use and heavy drinking during adolescence and the transition to young adulthood. Journal of Studies on Alcohol, Supplement No. 14, 54–70.
Schulenberg, J. E., Sameroff, A. J., & Cicchetti, D. (2004). The transition to adulthood as a critical juncture in the course of psychopathology and mental health. Development and Psychopathology, 16, 799–806.
Shanahan, M. J. (2000). Pathways to adulthood in changing societies: Variability and mechanisms in life course perspective. Annual Review of Sociology, 26, 667–692.
Shroff, R., Weaver, D. J., & Mitsnefes, M. M. (2011). Cardiovascular complications in children with chronic kidney disease. Nature Reviews Nephrology, 7, 642–649.
Silbereisen, R. K., & Lerner, R. M. (2007). Approaches to positive youth development. Los Angeles/London: Sage.
Skokauskas, N., & Gallagher, L. (2010). Psychosis, affective disorders and anxiety in autistic Spectrum disorder: Prevalence and Nosological considerations. Psychopathology, 43, 8–16.
So, T.-Y., Bradley Layton, J., Bozik, K., Farrington, E., Gipson, P. E., Gibson, K., Primack, W., Conley Iii, W., Gipson, D. S., & Ferris, M. (2011). Cognitive pharmacy services at a pediatric nephrology and hypertension clinic. Renal Failure, 33, 19–25.
Spear, L. P. (2000). The adolescent brain and age-related behavioral manifestations. Neuroscience & Biobehavioral Reviews, 24(4), 417–463.
Steelman, L. C., & Powell, B. (1991). Sponsoring the next generation: Parental willingness to pay for higher education. American Journal of Sociology, 96(6), 1505–1529.
Steinberg, L., Dahl, R., Keating, D., Kupfer, D. J., Masten, A. S., & Pine, D. S. (2006). The study of developmental psychopathology in adolescence: Integrating affective neuroscience with the study of context. In D. Cicchetti & D. Cohen (Eds.), Handbook of developmental psychopathology (Vol. 2, pp. 710–741). New York: Wiley.
Taylor, J. L., & Seltzer, M. M. (2010). Changes in the autism behavioral phenotype during the transition to adulthood. Journal of Autism and Developmental Disorders, 40, 1431–1446.
Taylor, J. L., & Seltzer, M. M. (2011a). Changes in the mother–child relationship during the transition to adulthood for youth with autism Spectrum disorders. Journal of Autism and Developmental Disorders, 41, 1397–1410.
Taylor, J. L., & Seltzer, M. M. (2011b). Employment and post-secondary educational activities for young adults with autism Spectrum disorders during the transition to adulthood. Journal of Autism and Developmental Disorders, 41, 566–574.
Wadsworth, M. E., et al. (2016). Poverty and the development of psychopathology. In: M. E. Wadsworth, G. W. Evans, K. Grant, J. S. Carter, & S. Duffy (Eds.), Development and psychopathology.Volume Four. Risk, resilience, and intervention, Ch 8 (pp. 215–237). Hoboken: John Wiley & Sons.
Walker, J. S., & Gowen, L. K. (2011). Community-based approaches for supporting positive development in youth and young adults with serious mental health conditions. Portland: Research and Training Center for Pathways to Positive Futures, Portland State University.
Watson, A. R. (2000). Non-compliance and transfer from Paediatric to adult transplant unit. Pediatric Nephrology, 14, 469–472.
Watson, A. R. (2005). Problems and pitfalls of transition from Paediatric to adult renal care. Pediatric Nephrology, 20, 113–117.
Watson, A. R., Harden, P., Ferris, M., Kerr, P. G., Mahan, J., & Ramzy, M. F. (2011). Transition from pediatric to adult renal services: A consensus statement by the international society of nephrology (Isn) and the international pediatric nephrology Association (Ipna). Pediatric Nephrology, 26, 1753–1757.
Webster, B. H., Jr., & Bishaw, A. (2006). U.S. Census Bureau, American Community Survey Reports, ACS-02, Income, Earnings, and Poverty Data From the 2005 American Community Survey. Washington, DC: U.S. Government Printing Office.
Whitbeck, L., Hoyt, D. R., & Huck, S. M. (1994). Early family relationships, intergenerational solidarity, and support provided to parents by their adult children. Journal of Gerontology, 49, S85–S94.
White, S. W., Oswald, D., Ollendick, T., & Scahill, L. (2009). Anxiety in children and adolescents with autism Spectrum disorders. Clinical Psychology Review, 29, 216–229.
Yeager, D. S., & Dweck, C. S. (2012). Mindsets that promote resilience: When students believe that personal characteristics can be developed. Educational Psychologist, 47(4), 302–314.
Yeung, E., Kay, J., Roosevelt, G. E., Brandon, M., & Yetman, A. T. (2008). Lapse of care as a predictor for morbidity in adults with congenital heart disease. International Journal of Cardiology, 125, 62–65.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
This chapter is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, duplication, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made. The images or other third party material in this chapter are included in the work's Creative Commons license, unless indicated otherwise in the credit line; if such material is not included in the work's Creative Commons license and the respective action is not permitted by statutory regulation, users will need to obtain permission from the license holder to duplicate, adapt or reproduce the material.
Copyright information
© 2018 The Author(s)
About this chapter

Cite this chapter
Wood, D. et al. (2018). Emerging Adulthood as a Critical Stage in the Life Course. In: Halfon, N., Forrest, C., Lerner, R., Faustman, E. (eds) Handbook of Life Course Health Development . Springer, Cham. https://doi.org/10.1007/978-3-319-47143-3_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-47143-3_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-47141-9
Online ISBN: 978-3-319-47143-3
eBook Packages: MedicineMedicine (R0)