
Abstract
Intestinal atresia is a common cause of neonatal intestinal obstruction. Laparoscopic-assisted repair is a favorable approach given the ease with which the small bowel may be externalized; it offers several benefits compared to the traditional laparotomy including decreased pain, smaller incisions, and quicker recovery. This chapter gives an overview of intestinal atresia and outlines the preoperative evaluation, operative techniques, postoperative management, and outcomes of laparoscopic-assisted repair.
Introduction
Epidemiology
Intestinal atresia is defined as congenital obstruction of the small or large bowel due to abnormal intrauterine development. It is generally considered a sporadic disease, although rare familial cases have been reported [1]. There is an association with prematurity, with males and females being equally affected [2]. Most commonly this phenomenon occurs in the small intestine (jejunum and ileum), with an incidence ranging from 1 in 1500 to 12,000 live births. Large bowel involvement is less common and occurs in about 1 in 40,000 live births [2]. The overall mortality rate of jejuno-ileal atresia is reported 11 %, mostly due to associated anomalies and more frequently in patients with type IIIB or type IV atresias [4].
Pathophysiology
Small and large bowel atresia is presumed to be the result of an intrauterine ischemic insult to the midgut during the 10 to 12th week of gestation, when the intestines return to the coelomic cavity. The affected segment of bowel undergoes necrosis resulting in bowel discontinuity [4]. Several studies have replicated this phenomenon by performing ligation of mesenteric blood vessels in animals [5–7]. There is a low association with other organ abnormalities, given the isolated vascular compromise and late occurrence in relation to organogenesis [8]. However, multiple reports of diagnosis of intestinal atresia in the setting of gastroschisis and Hirschsprung’s disease exist.
Classification of Intestinal Atresia (Fig. 26.1)

Types of intestinal atresia. From Sinha CK, et al. Intestinal Atresia. In: Handbook of Pediatric Surgery, Sinha CK, Davenport M, eds. Springer; 2010, pg. 97. Reprinted with permission.
Intestinal atresia is classified into four categories. Type I is the least common of the four, in which the serosa and muscularis layers of the intestine remain intact. In contrast to the other types of atresia, there is no discontinuity in the bowel and a slight decrease in diameter of the bowel distal to the atresia is the only abnormality visible external to the intestine. The obstruction in this type of atresia is due to a diaphragm of mucosa or submucosa, which occludes the lumen of the bowel. Intestinal stenosis, a condition in which the bowel lumen is merely narrowed and not completely obstructed, is associated with Type I deformities and managed similarly. In Type II intestinal atresia, no layers of the bowel wall are in continuity and a fibrous band connects the proximal and distal segments of intestine. The most common intestinal atresia is type III and it is divided into two subtypes. Type IIIA is similar to Type II; however, no fibrous band connects the segments of bowel in discontinuity. Type IIIB is also known as the apple peel or Christmas tree deformity. Both bowel and mesentery are in complete discontinuity allowing the distal bowel to corkscrew around its mesenteric arterial supply, giving it an apple peel appearance. Type IV atresia is a combination of multiple Type II and IIIA segments of atresia. Multiple areas of discontinuous bowel segments are involved, some of which are connected by fibrous bands (“chain of lake” appearance) [3]. This atresia is likely a result of multiple insults to the small bowel vasculature, such as embolic debris [9].
Preoperative Evaluation
History
Although typically diagnosed in the early postnatal stage, diagnosis of intestinal atresia with prenatal ultrasound is possible in about 30–40 % of cases. This allows planning for the delivery at an appropriate facility [4, 10]. Prenatal ultrasound can detect findings associated with intestinal atresia, such as dilated echogenic loops of bowel greater than 7 mm in internal diameter and ascites, during the late second trimester and onward [1, 4, 10–12] (Fig. 26.2). Polyhydramnios are present in about 15–20 % of cases [3]. In general, proximal obstructions are more easily detected prenatally because bowel loops are more extensively dilated and polyhydramnios is more significant [4].
Presentation

Dilated loops of bowel seen on prenatal ultrasound. From Couture A. Bowel Obstruction in Neonates and Children. In: Baud C, et al. Gastrointestinal Tract Sonography in Fetuses and Children: Springer; 2008, pp 131–251. Reprinted with permission.
Average gestational age at birth of infants with intestinal atresia is 36–37 weeks [4, 13]. The presentation varies according to the location of the obstruction. Patients with proximal obstructions most frequently present with bilious emesis in the first 24–48 h, while abdominal distension is the primary feature of distal lesions and vomiting is a late symptom [4]. A focused physical exam can reveal findings suggestive of volume depletion, such as dry mucous membranes, sunken fontanelles, and decreased skin turgor. These infants are at high risk for aspiration and should be monitored closely for signs of respiratory compromise. After the initial exam, serial abdominal exams should be performed to assess progression of the obstruction and monitor for signs of perforation with peritonitis. Diagnosis of intestinal stenosis is more demanding. Patients will show more subtle symptoms associated with a partial obstruction and often present later with failure to thrive. No laboratory studies are indicative of intestinal atresia or stenosis; however, it is important to monitor and correct electrolyte and acid–base disturbances.
Initial Management
Once an intestinal obstruction is suspected, initial management consists of holding feeds, fluid resuscitation with electrolyte replacement, correction of acid–base disturbances, and gastric decompression with an orogastric or nasogastric tube to suction. Parenteral antibiotics are indicated if there is concern for sepsis. After these initial steps are taken, further workup including imaging studies can be carried out to determine the level and cause of obstruction. Supine and decubitus plain X-rays are the first imaging studies performed. Expected findings include dilated gas filled loops of small bowel and absence of distal air. Although non-specific, these radiographic findings frequently establish the diagnosis in combination with the clinical exam [4]. If there is concern for volvulus, malrotation, or a partial obstruction, an upper GI study should be obtained. Water-soluble contrast enema can be indicated in selected cases prior to surgical repair to exclude concomitant colonic atresia. It is important to note that in the setting of pneumoperitoneum, shock, or peritonitis, these imaging studies should not delay surgical treatment (Fig. 26.3).

Abdominal X-ray at 24 h of life in infant with jejunal atresia. Proximal dilated loops of small bowel are seen with no gas in distal bowel. From Couture A. Bowel Obstruction in Neonates and Children. In: Baud C, et al. Gastrointestinal Tract Sonography in Fetuses and Children: Springer; 2008, pp 131–251. Reprinted with permission.
Operative Technique
Special Considerations
Early operative repair is preferred in order to decrease the risk of the perforation or necrosis of the bowel and aspiration pneumonia. There are several important considerations that should be made prior to surgery: Hirschsprung’s disease can mimic intestinal atresia and should be ruled out with rectal suction biopsies in suspected cases [14]. Intestinal atresia can also occur alongside gastroschisis, which can significantly change the course of repair of the atresia. Surgical options include primary repair of the atresia during closure of the abdominal wall or a more conservative approach, involving abdominal wall closure with or without stoma and secondary repair.
Preoperative Management
Prior to surgery, all patients should be managed with gastric decompression via an orogastric or nasogastric tube and intravascular fluid resuscitation with correction of electrolyte and acid–base disturbances. Necessary laboratory studies include type and screen, complete blood count, basic metabolic panel, and coagulation profiles. Water-soluble contrast enema should be considered to confirm patency of the colon [4]. Determining the appropriate timing of surgery requires balancing the advantages of optimization from a respiratory, cardiac, and metabolic perspective with the risks of delayed repair, such as vomiting, aspiration, sepsis, and parenteral nutrition [15].
Instruments
In the operating room, basic laparoscopic instruments, a bowel stapler, suction, and a suction biopsy kit will be necessary.
Steps
-
1.
Position the infant in supine position at the lower end of the operating table (or in transverse position). An orogastric tube should have already been placed preoperatively to decompress the stomach.
-
2.
The surgeon stands at the patient’s feet with the assistant to his left and scrub nurse to his right. Monitors are placed on either side at the head of the table.
-
3.
Using an intra- or infraumbilical incision, access the peritoneal cavity via the open Hassan technique. Place a 11-mm trocar and establish a pneumoperitoneum of 8–10 mmHg.
-
4.
The authors use the 10-mm Storz Hopkins telescope with in-built 5-mm working channel to explore the peritoneal cavity and confirm the diagnosis. This telescope combines a 0-degree fiberoptic camera with a single working channel which allows single site exploration. Place the patient in Trendelenburg or reverse Trendelenburg position to facilitate intra-abdominal exposure.
-
5.
Once the atresia is identified, it can be exteriorized through the umbilical incision to complete the procedure in a standard open fashion. Proximal and distal small bowel should be marked with two antimesenteric stay sutures to maintain orientation. Alternatively, exploratory laparoscopy can be omitted and the procedure can be performed by exteriorizing small bowel through a limited inferior periumbilical incision. Run the bowel to evaluate for distal patency and rule out additional segments of atresia. Injection of normal saline allows to assess for distal patency of the small intestine [4] (Fig. 26.4).
Fig. 26.4. 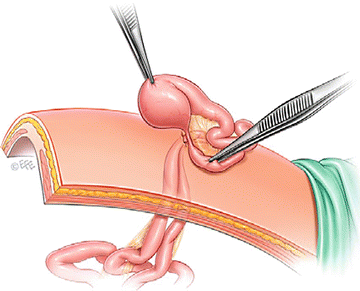
Exteriorized loops of bowel. From Schier F, Turial S. Laparoscopy in children. 2nd ed. Heidelberg: Springer; 2013: 126–7. Reprinted with permission.
-
6.
Depending on location and level of the atresia, the proximal segment can be significantly dilated. Assess caliber discrepancy and consider resection (in cases of high jejunal atresia) or tapering of the proximal obstructed segment.
-
7.
Using a GIA bowel stapler, resect the atretic portion(s) of bowel. Tapering enteroplasty can be achieved by antimesenteric longitudinal bowel resection using a 5 mm GIA stapler.
-
8.
Reanastomose the bowel ends in a single-layer hand-sewn technique to create an end-to-oblique anastomosis using 4–0 or 5–0 absorbable suture (polyglactin or polydioxanone) in an interrupted seromuscular fashion. Alternatively, a stapled side-to-side, functional end-to-end anastomosis, using a 5 mm GIA stapler can be considered. Close the mesenteric defect with fast absorbable suture (Fig. 26.5).
Fig. 26.5. 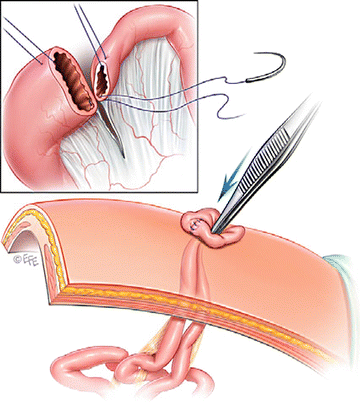
Fashioning the anastomosis and return of the bowel to the abdominal cavity. From Schier F, Turial S. Laparoscopy in children. 2nd ed. Heidelberg: Springer; 2013: 126–7. Reprinted with permission.
-
9.
Return the bowel to the abdominal cavity. Consider replacing the umbilical port and laparoscope for one final check.
-
10.
Remove the trocar. Close the fascial defect at the umbilical port with absorbable suture.
-
11.
Perform suction biopsy of the rectum if suspicion for Hirschsprung’s disease is given [15, 16].


Pearls/Pitfalls
There are several principles to keep in mind when performing this procedure. When the bowel is exteriorized through the umbilical port, avoid exteriorizing more loops of bowel than are necessary. Bowel edema developing during the procedure can make reducing the bowel through the small umbilical incision difficult [17]. When the proximal segment of small bowel is severely dilated, resection or tapering of the dilated bowel may be necessary to reduce the risk of ineffective peristalsis. Resection is preferred to imbrication when tapering due to risk of recurrence and need for revision with plication. However, when multiple segments of atresia are present, care should be taken to preserve intestine length. Adequate bowel length is considered to be at least 30 cm of jejunum and ileum with an intact ileocecal sphincter, but ideally more than 75 cm [4].
Postoperative Care
Postoperative Management
Postoperative management is focused on nutritional support. Nasogastric decompression is continued until bowel function has returned. Once bowel function returns, oral feeding is begun. However, parenteral nutritional support is continued until goal calories are achieved with oral intake. Postoperative ileus can take as long as 9 days with most patients being discharged between postoperative days 9–16 [4, 15, 16].
Complications
Complications include anastomotic leak, adhesions, and small bowel obstruction in the first year of life, reoperation for bowel dilatation, prolonged parenteral nutrition, and malabsorptive syndromes, such as short bowel syndrome [13]. An anastomotic leak rate similar to that seen in laparotomy can be expected since the anastomosis is fashioned extracorporeally. Current studies suggest the rate of small bowel obstruction in the first year of life after laparotomy is about 12 % [4]. This rate is expected to decrease in laparoscopic-assisted repair.
Outcomes
The procedure is well tolerated with laparoscopic repair averaging an operative time of 48 min and with incisions measuring approximately 1–2.5 cm. Patients are at no increased risk of bleeding and typically do not require transfusion of blood products. Compared to the conventional open approach the decreased size of the incision offers a marked cosmetic benefit while the extracorporeal portion of the procedure allows open anastomosis without the morbidity of a traditional laparotomy incision [15]. Laparoscopic-assisted repair may also have increased benefits by reducing the risk of small bowel obstructions in the first year of life due to decreased formation of adhesions [18].
Summary
-
Intestinal atresia is one of the most common causes of intestinal obstruction in neonates.
-
The ability to exteriorize the small bowel in infants makes laparoscopic-assisted repair a safe and feasible technique for surgeons trained in laparoscopy.
-
Laparoscopic-assisted technique offers safe repair of intestinal atresia and appears to reduce discomfort, improve cosmesis, and reduce the risk of adhesive postoperative small bowel obstruction.
References
Kumaran N, Shankar KR, Lloyd DA, Losty PD. Trends in the management and outcome of jejuno-ileal atresia. Eur J Pediatr Surg. 2002;12:163.
Dalla Vecchia LK, Grosfeld JL, West KW, et al. Intestinal atresia and stenosis: a 25-year experience with 277 cases. Arch Surg. 1998;133:490–6.
Iacobelli, BD, Zaccara A, SpiydakisI, et al.. Prenatal counseling of small bowel atresia: watch the fluid! Prenat Diagn. 2006;26:214
Burjonrappa S, Crete E, Bouchard S. Comparative outcomes in intestinal atresia: a clinical outcome and pathophysiology analysis. Pediatr Surg Int. 2011;27(4):437–42.
Louw JH. Resection and end-to-end anastomosis in the management of atresia and stenosis of the small bowel. Surgery. 1967;62:940.
Tibboel D, van der Kamp AW, Molenaar JC. The effect of experimentally induced intestinal perforation at an early developmental stage. J Pediatr Surg. 1981;16:1017.
Grosfeld JL, Ballantine TV, Shoemaker R. Operative management of intestinal atresia and stenosis based on pathologic findings. J Pediatr Surg. 1979;14:368.
Sweeney B, Surana R, Puri P. Jejunoileal atresia and associated malformations: correlation with timing of in-utero insult. J Pediatr Surg. 2001;36:774–6.
Komuro H, Amagai T, Hori T, et al. Placental vascular compromise in jejunoileal atresia. J Pediatr Surg. 2004;39:1701–5.
Basu R, Burge DM. The effect of antenatal diagnosis on the management of small bowel atresia. Pediatr Surg Int. 2004;20:177–9.
Phelps S, Fisher R, Partington A, Dykes E. Prenatal ultrasound diagnosis of gastrointestinal malformations. J Pediatr Surg. 1997;32:438.
Ghose I, Mason GC, Martinez D, et al. Hyperechogenic fetal bowel: a prospective analysis of sixty consecutive cases. BJOG. 2000;107:426.
Burjonrappa SC, Crete E, Bouchard S. Prognostic factors in jejuno-ileal atresia. Pediatr Surg Int. 2009;25(9):795–8.
Seo T, Ando H, Watanabe Y, et al. Colonic atresia and Hirschsprung’s disease: importance of histologic examination of the distal bowel. J Pediatr Surg. 2002;37, E19.
Li B, Chen W, Wang S, Liu S, Li L. Laparoscopic-assisted surgery for neonatal intesintal atresia and stenosis: a report of 35 cases. Pediatr Surg Int. 2012;28:1225–8.
Abhyankar A, Mukhtar Z. Laparoscopy-assisted surgery for neonatal intestinal atresia: single-center experience. Asian J Endosc Surg. 2011;4(2):90–3.
Schier F, Turial S. Laparoscopy in children. 2nd ed. Heidelberg: Springer; 2013. p. 126–7.
Holcomb GW, Georgeson K, Rothenberg S. Atlas of pediatric laparoscopy and thoracoscopy. Philadelphia: Saunders/Elsevier; 2008. p. 9–13, 49.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Mamolea, C., Yung, J.B., Seifarth, F.G. (2017). Laparoscopic Approach to Intestinal Atresia. In: Walsh, D., Ponsky, T., Bruns, N. (eds) The SAGES Manual of Pediatric Minimally Invasive Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-43642-5_26
Download citation
DOI: https://doi.org/10.1007/978-3-319-43642-5_26
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43640-1
Online ISBN: 978-3-319-43642-5
eBook Packages: MedicineMedicine (R0)