
Abstract
Diagnose Knee osteoarthritis (OA) is a very important task, in this work an automated metrics method is used to predict chronic pain. In early stages of OA, changes into joint structures are shown, some of the most common symptoms are; formation of osteophytes, cartilage degradation and joint space reduction, among others. Using public data from the Osteoarthritis initiative (OAI), a set of X-ray images with different Kellgren Lawrence score (K & L) scores were used to determine a relationship between bilateral asymmetry and the radiological evaluation in K & L score with the chronic knee pain. In order to measure the asymmetry between the knees, the right knee was registered to match the left knee, then a series of similarity metrics; mutual information, correlation, and mean square error were computed to correlate the deformation (mismatch) and K & L score with chronic knee pain. Radiological information was evaluated and scored by OAI radiologist groups, all metric of image registration were obtained in an automated way. The results of the study suggest an association between image registration metrics, radiological K & L score with chronic knee pain. Four GLM models wit AUC \(\> 0.6\) and \(\> 0.7\) accuracy random forest classification model was formed with this information to classify the early bony changes with OA chronic knee pain.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
Osteoarthritis (OA) is one of the most common diseases in the industrialized world. This incapacitating disease brings poor quality of life to many people, turning in a painful task working or even making daily life activities. This disease affects 1 in 10 adults over 60 years, only in the United States [25], OA is the most common manifestation of arthritis. In Mexico, OA is one of the principal causes of medical attention requests.
X-Ray imaging is the first hand information that Diagnosing OA and determining the patient disease stage is critical, medical imaging is one of the techniques used to primary diagnose and staging.
There are several radiological methods to establish the stage in the OA. Expert radiologists evaluate radiological evidence of x-ray images to determine morphological changes such as appearance of osteophytes, structural changes or joint space narrowing (JSN) [1]. This radiological evidence has not been fully studied or associated with the most common symptoms [12, 14, 18, 24]; pain and stiffness [8]. One of the biggest challenges is clearly associate radiological evidence with early symptoms that commonly have late onset, as it is the most common symptom in OA; pain.
Early diagnosis is very important because the knee pain is one of the most disabling symptoms even at early ages. There is a lack of standards in the form of how images are assessed. To attack this problem, OA community has developed a series of clinical questionnaires and some atlas [2, 10, 16, 17] for image evaluation [3, 22]. There are methods such as Kellgren-Lawrence (K & L) [16] that are commonly used by radiologists to evaluate images, but these methods still depend on the judgment of an experienced radiologist, and studies demonstrate that the same image can be evaluated very differently by two or more different radiologists, and even the same radiologist may assess differently the same film at two different times [19, 20].
The development of an automatic method for the evaluation of the images is very important, this way the bias induced by the human factor is reduced, and the patient can be evaluated in an objective way. Using computational methods to evaluate x-ray images can be used as a second opinion and thus achieve an automatic patient early diagnosis of OA. For this reason, a large number of associations makes huge efforts to generate information about the disease in search of finding treatments or even a cure that does not exist now.
The Osteoarthritis Initiative (OAI) has been recollecting thousands of clinical data in OA patients, subjects at risk, and control subjects using validated questionnaires and standardized image assessment procedures. The OAI effort has bring very important information that will enable a better understanding of the disease process. Using x-ray images of the knee available in open databases OAI, the goal of this work is to use computational methods to correlate metrics obtained automatically with chronic pain as the main symptom.
Using image registration techniques [26] allows the alignment of both knees to measure the degree of asymmetry between knees, this asymmetry metrics aim to help find a relationship between the deformation of the bone structure and chronic knee pain.
Three different asymmetry metrics were obtained using the registered knees; Mutual information, Correlation, and Mean Square error in order to explore the relation of the asymmetry between the knees as the chronic pain. Using the automated metrics and the assessed K & L score, the association of the bony structure with the chronic pain is analyzed.
2 Materials and Methods
In this work, a series of images were processed by computational and radiological techniques. All the Materials and Methods are described below.
2.1 Data Acquisition
Public data from OAI was used to develop this work. “OAI is a multi-center, longitudinal, prospective observational study of knee OA. The OAI will establish and maintain a natural history database for osteoarthritis that will include clinical evaluation data, radiological (x-ray and magnetic resonance) images, and a bio-specimen repository from 4796 men and women aged between 45 and 79 years old, enrolled between February 2004 and May 2006” (https://oai.epi-ucsf.org). Bilateral knee x-ray images and the Central Reading of Knee X-rays for K-L Grade, chronic pain information, and Individual Radiographic Features of Knee Datasets were used. Subjects in the study were selected from the database using the baseline K & L score information and chronic pain data.
2.2 Subject Selection
A case/control study using K & L scores to predict pain cohort was used. Using a random process, 50 subjects of this cohort were selected, 10 for each K & L score level (0–4). The selection criteria for the cohort was:
Control subjects were selected under the criteria of:
-
1.
Not presenting pain as a symptom since the baseline visit to 60 month visit;
-
2.
Not presenting a symptomatic status since the baseline visit to 60 month visit;
-
3.
Taking no pain medication from the baseline visit to the 60 month visit.
Case subjects were selected under the criteria of:
-
1.
Not presenting pain as a symptom at baseline visit;
-
2.
Not presenting a symptomatic status at baseline visit;
-
3.
Taking no pain medication at the baseline visit;
-
4.
Develop chronic right knee pain in some time point after baseline and up to 60 month visit.
2.3 Image Processing
Due the high dynamism of the knees, a direct comparison of the left and right image cannot be performed straight forward. An alignment of the images must be carried out prior to the similarity analysis. Three main steps were performed:
-
1.
The knees of the patient are segmented in order to remove unwanted information.
-
2.
An alignment (registration) of the left knee to the right is carried out.
-
3.
A similarity metrics are computed in order to evaluate the relationship of the degree of similarity between knees and the stages of the disease.
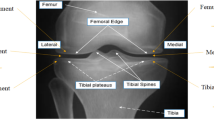
All images were pre-processed manually. During this process, the area of interest in the images was enclosed to prevent unwanted information i.e. (Tags, noise, marks) into the regions. The region of interest (ROI) in the x-ray image was adjusted, this process generates an individual image for each knee, then, the left knee image is horizontally flipped to enable the image registration process, a logarithmic transformation in each pixel is performed to enhance the low intensity pixels in the image [15]. In Fig. 1 shows an example of the ROI used in this research.

Input image, ROI to be used is displayed in a yellow rectangle (Color figure online)
Image Segmentation. All background noise and all image artifacts were removed from the x-ray images using an automated segmentation process. The automatic segmentation of the knee was based on the background noise. This process created a segmentation mask, this mask discards any pixel above a threshold value, this threshold value is unique for each image. Afterwards, the largest connected region of the entire image, went through a hole filling algorithm based on morphological operations to ensure a solid surface extraction. This segmentation process using the mask to extract only the knee bones structure and discard all background.
Image Registration. For the registration process of the left knee into the right knee, the segmentation mask was used as ROI. The left knee image was mirrored and then co-registered with it’s corresponding right knee image.
A B-Spline multi resolution algorithm was used to optimize the Mattes mutual information metric in the bilateral image registration [5]. A deformable B-Spline transform is used, this is based on transforming an image modifying control points contained in a mesh based on a maximization of a similarity measure, this approach often avoids local minimal in the parameter search space and reduces computational time [9, 23], In this multi resolution approach, all images are registered in the lowest resolution, and in the next steps, the transformation parameters are scaled to the higher resolutions and parameter optimization is computed again. The registration algorithm returns a transformation file: T(x,y) that is used to find a point in the left image for each point (x,y) in the right image [4].
Metric Quantification. To establish the relation between the registered image and the target image, three representative measurements were computed, sum of square differences [7], correlation coefficient, mutual information. This set of measurements is wide used in the literature [13] as a measurement of similarity between two images.
The sum of squared differences (SSD) in Eq. 1 assumes that the images are identical at registration, and the implicit assumption that there are no differences between intensity profiles. This metric is sensitive to outliers: small number of voxels having large intensity differences. Where f(x) is the intensity at a position x in an image, m(t(x)) is the intensity at the corresponding point given by the transformation t(x). N is the number of pixels in the region of overlap.
The correlation coefficient (CC) is a measure of the linear dependence between two variables X and Y or images, in Eq. 2 is described the CC, where f (x) is the intensity at a position x in the fixed image, and m (t (x)) is the intensity at the corresponding point given by the transformation t (x) in the moving image, the number of pixels in overlapped region is represented by N.
Mutual information (MI) shown in Eq. 3, provides a measure of probabilistic dependence between two intensity distributions. For this research, the ShannonWiener entropy measure H in Eq. 3 is used, this measurement is one well-known used measure of information in image processing, this measurement was originally developed as part of communication theory in the 1940 s [17].
In Eq. 4 H(X,Y) represents the joint entropy, and H(X) the individual entropy of random image X, Y, N stands for the number of intensity levels, and Px (Pxy) is the probability of value X (x,y) in the (joint) probability distribution of variable X (X and Y).
2.4 Statistical Analysis
In a first step, using only the variables obtained by the method of image registration; MI, CORR, and MS, logistic regression as cost function is used for the analysis. A general linear model is generated and analyzed, odds ratio, and the area under the receiver operating characteristic (ROC) curve (AUC) were calculated. The ROC curve was constructed and the curve is a graphical representation of the sensitivity against 1-specificity for a binary classifier system as the discrimination threshold is varied. The outcome variable in this analysis was the left knee chronic pain.
In a second case, the information obtained from the image registration process and the information evaluated for the K & L score is used with logistic regression to generate a new general linear model, ODD, and AUC were calculated for the model. In this case the outcome variable was chronic left knee pain.
Finally, using the variables that had the highest ODD, a known classifier, it is generated using a Random Forest technique. The classifier was run using chronic left knee pain as outcome variable, and 5000 trees as defaults.
All statistical analyzes were performed using statistical software R and its packages [21].
3 Results
Based on the experimental work, the obtained results are presented. First the results obtained from the image registration metrics are shown in Table 1, results on MI, CORR, and MS obtained for each of the levels of K & L of 50 analyzed patients for this work are presented by OA stage.
After obtaining the metrics, linear models were generated using logistic regression as classification function, statistical results and their AUC are presented in the Table 2. In Fig. 2, ROC curves for each model are shown.
Once the ODD ratios were obtained, the 5000 trees random forest classifications presented the results below:
-
CORR. Using the variable with the highest ODD, a 0.7143 accuracy classification was obtained.
-
CORR+K & L. Using the variables in the best GLM models, a 0.6122 accuracy classification was obtained.

ROC curves; (a) GLM1, (b) GLM2, (c) GLM3, (d) GLM4
4 Conclusion
This paper presents for the first time in medical diagnosis the use of automatic asymmetry metrics to associate symptoms such as chronic knee pain. The results shown in the Table 2, demonstrate a behavior similar to models based on a search within tens of variables. The association of changes in the bone structure can be detected by the asymmetry that might be associated with early chronic knee pain.
The set of information obtained automatically, and radiological assessment of an expert improves performance classification of a power regression model.
On the other hand, using the variable that determines a greater risk to the subject of developing the symptoms, and use that variable as a classifier on a random forest, delivers us an accuracy of more than 0.7, that within the standard prediction of pain is above those reported in the work of sorting pain [11].
In works like [18], a cohort with all subjects diagnosed with OA, the AUC obtained is 0.64 using radiological evaluations, and 0.70 using evaluations and K & L scores. In a [6] study, the reported the OR are between 1.95 and 2.11.
In this work, the metrics obtained without a radiologist intervention have a similar performance in prediction and OR.
Pain is one of the most complex to explain symptoms, the fact that morphological characteristics can be associated at least as an early risk factor may help develop a treatment by early diagnosis.
This type of association of pain may be the first step in developing a tool that helps to have a second opinion to decrease the workload of the radiologist, and thus deliver more accurate diagnoses.
The limitations of this study are mainly the number of patients enrolled in the study, although medical standards comply with 20 patients minimum.
For future work, the number of patients which metrics are performed will be increased. The association with chronic pain will be complemented by other scales known as WOMAC pain and KOOS. To obtain a robust model is to combine it with some other type of clinical or radiological variables may obtain a biomarker for OA.
References
Altman, R., Asch, E., Bloch, D., Bole, G., Borenstein, D., Brandt, K., Christy, W., Cooke, T., Greenwald, R., Hochberg, M., et al.: Development of criteria for the classification and reporting of osteoarthritis: Classification of osteoarthritis of the knee. Arthritis Rheum. 29(8), 1039–1049 (1986)
Altman, R.D., Gold, G.: Atlas of individual radiographic features in osteoarthritis, revised. Osteoarthritis Cartilage 15, A1–A56 (2007)
Bellamy, N.: Validation study of womac: A health status instrument for measuring clinically-important patient-relevant outcomes following total hip or knee arthroplasty in osteoarthritis. J. Orthop. Rheumatol. 1, 95–108 (1988)
Celaya-Padilaa, J.M., Rodriguez-Rojas, J., Trevino, V., Tamez-Pena, J.G.: Local image registration a comparison for bilateral registration mammography. In: IX International Seminar on Medical Information Processing and Analysis, pp. 892210–892210. International Society for Optics and Photonics (2013)
Celaya-Padilla, J., Martinez-Torteya, A., Rodriguez-Rojas, J., Galvan-Tejada, J., Treviño, V., Tamez-Peña, J.: Bilateral image subtraction and multivariate models for the automated triaging of screening mammograms. BioMed Res. Int. 2015 (2015)
Creamer, P.: Osteoarthritis pain and its treatment. Curr. Opin. Rheumatol. 12(5), 450–455 (2000)
Crum, W.R., Hartkens, T., Hill, D.: Non-rigid image registration: theory and practice. Br. J. Radiol. (2014)
Dekker, J., Boot, B., van der Woude, L.H., Bijlsma, J.: Pain and disability in osteoarthritis: a review of biobehavioral mechanisms. J. Behav. Med. 15(2), 189–214 (1992)
Diez, Y., Oliver, A., Lladó, X., Freixenet, J., Martí, J., Vilanova, J.C., Marti, R.: Revisiting intensity-based image registration applied to mammography. IEEE Trans. Inf. Technol. Biomed. 15(5), 716–725 (2011)
Duryea, J., Li, J., Peterfy, C., Gordon, C., Genant, H.: Trainable rule-based algorithm for the measurement of joint space width in digital radiographic images of the knee. Med. phys. 27(3), 580–591 (2000)
Galván-Tejada, J.I., Celaya-Padilla, J.M., Treviño, V., Tamez-Peña, J.G.: Multivariate radiological-based models for the prediction of future knee pain: Data from the OAI. Comput. Math. Methods Med. 2015, 1–10 (2015)
Glass, N., Torner, J., Law, L.F., Wang, K., Yang, T., Nevitt, M., Felson, D., Lewis, C., Segal, N.: The relationship between quadriceps muscle weakness and worsening of knee pain in the most cohort: a 5-year longitudinal study. Osteoarthritis Cartilage 21(9), 1154–1159 (2013)
Guo, Y., Sivaramakrishna, R., Lu, C.C., Suri, J.S., Laxminarayan, S.: Breast image registration techniques: A survey. Med. Biol. Eng. Comput. 44(1–2), 15–26 (2006)
Hochman, J., Davis, A., Elkayam, J., Gagliese, L., Hawker, G.: Neuropathic pain symptoms on the modified paindetect correlate with signs of central sensitization in knee osteoarthritis. Osteoarthritis Cartilage 21(9), 1236–1242 (2013)
Jourlin, M., Pinoli, J.C.: Logarithmic image processing: The mathematical and physical framework for the representation and processing of transmitted images. Adv. Imaging Electron Phys. 115, 129–196 (2001)
Kellgren, J., Lawrence, J.: Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 16(4), 494 (1957)
Kellgren, J., Lawrence, J.: Atlas of Standard Radiographs: The Epidemiology of Chronic Rheumatism, vol. 2. Blackwell Scientific, Oxford (1963)
Kinds, M.B., Marijnissen, A.C., Bijlsma, J.W., Boers, M., Lafeber, F.P., Welsing, P.M.: Quantitative radiographic features of early knee osteoarthritis: Development over 5 years and relationship with symptoms in the check cohort. J. Rheumatol. 40(1), 58–65 (2013)
Kornaat, P.R., Ceulemans, R.Y., Kroon, H.M., Riyazi, N., Kloppenburg, M., Carter, W.O., Woodworth, T.G., Bloem, J.L.: MRI assessment of knee osteoarthritis: knee osteoarthritis scoring system (koss)inter-observer and intra-observer reproducibility of a compartment-based scoring system. Skeletal Radiol. 34(2), 95–102 (2005)
Pathria, M., Sartoris, D., Resnick, D.: Osteoarthritis of the facet joints: Accuracy of oblique radiographic assessment. Radiology 164(1), 227–230 (1987)
Ripley, B.D.: The R project in statistical computing. MSOR Connections 1(1), 23–25 (2001)
Roos, E.M., Lohmander, L.S.: The knee injury and osteoarthritis outcome score (koos): From joint injury to osteoarthritis. Health Qual. Life Outcomes 1(1), 64 (2003)
Rueckert, D., Sonoda, L.I., Hayes, C., Hill, D.L., Leach, M.O., Hawkes, D.J.: Nonrigid registration using free-form deformations: application to breast MR images. IEEE Trans. Med. Imaging 18(8), 712–721 (1999)
Shimura, Y., Kurosawa, H., Sugawara, Y., Tsuchiya, M., Sawa, M., Kaneko, H., Futami, I., Liu, L., Sadatsuki, R., Hada, S., et al.: The factors associated with pain severity in patients with knee osteoarthritis vary according to the radiographic disease severity: a cross-sectional study. Osteoarthritis Cartilage 21(9), 1179–1184 (2013)
White, D.K., Tudor-Locke, C., Felson, D.T., Gross, K.D., Niu, J., Nevitt, M., Lewis, C.E., Torner, J., Neogi, T.: Do radiographic disease and pain account for why people with or at high risk of knee osteoarthritis do not meet physical activity guidelines? Arthritis Rheum. 65(1), 139–147 (2013)
Zitova, B., Flusser, J.: Image registration methods: A survey. Image Vis. Comput. 21(11), 977–1000 (2003)
Acknowledgment
“The OAI is a public-private partnership comprised of five contracts (N01-AR-2-2258; N01-AR-2-2259; N01-AR-2-2260; N01-AR-2-2261; N01-AR-2-2262) funded by the National Institutes of Health, a branch of the Department of Health and Human Services, and conducted by the OAI Study Investigators. Private funding partners include Merck Research Laboratories; Novartis Pharmaceuticals Corporation, GlaxoSmithKline; and Pfizer, Inc. Private sector funding for the OAI is managed by the Foundation for the National Institutes of Health. This manuscript was prepared using an OAI public use data set and does not necessarily reflect the opinions or views of the OAI investigators, the NIH, or the private funding partners.”
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this paper
Cite this paper
Galván-Tejada, J.I., Galván-Tejada, C.E., Celaya-Padilla, J.M., Delgado-Contreras, J.R., Cervantes, D., Ortiz, M. (2016). Automated Image Registration for Knee Pain Prediction in Osteoarthritis: Data from the OAI. In: Martínez-Trinidad, J., Carrasco-Ochoa, J., Ayala Ramirez, V., Olvera-López, J., Jiang, X. (eds) Pattern Recognition. MCPR 2016. Lecture Notes in Computer Science(), vol 9703. Springer, Cham. https://doi.org/10.1007/978-3-319-39393-3_33
Download citation
DOI: https://doi.org/10.1007/978-3-319-39393-3_33
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-39392-6
Online ISBN: 978-3-319-39393-3
eBook Packages: Computer ScienceComputer Science (R0)
