
Abstract
If it appears strange that that one etiologic agent gives rise to such a diversity of disease, then consider the three major components of any infectious process: (1) the inherent virulence of the agent, (2) the infectious dose, and (3) the patient status. Allergic fungal sinusitis represents the most common form of sinonasal fungal disease. Invasive fungal sinusitis {acute, (<4 weeks) and chronic (>12 weeks)} represents the most serious sinonasal fungal disease, which develops in the setting of neutropenia, or neutrophil dysfunction. Other more rare and exotic sinonasal infectious conditions, or infectious mimickers are also discussed in this chapter.
Access this chapter
Tax calculation will be finalised at checkout
Purchases are for personal use only
References
Ardehali MM, Amali A, Bakhshaee M, Madani Z, Amiri M. The comparison of histopathological characteristics of polyps in asthmatic and nonasthmatic patients. Otolaryngol Head Neck Surg. 2009;140:748–51.
Samter M, Beers Jr RF. Intolerance to aspirin. Clinical studies and consideration of its pathogenesis. Ann Intern Med. 1968;68:975–83.
Samter M, Beers Jr RF. Concerning the nature of intolerance to aspirin. J Allergy. 1967;40:281–93.
Chang JE, White A, Simon RA, Stevenson DD. Aspirin-exacerbated respiratory disease: burden of disease. Allergy Asthma Proc. 2012;33:117–21.
Casale M, Pappacena M, Potena M, Vesperini E, Ciglia G, Mladina R, Dianzani C, Degener AM, Salvinelli F. Nasal polyposis: from pathogenesis to treatment, an update. Inflamm Allergy Drug Targets. 2011;10:158–63.
Yee KK, Pribitkin EA, Cowart BJ, Vainius AA, Klock CT, Rosen D, Hahn CG, Rawson NE. Smoking-associated squamous metaplasia in olfactory mucosa of patients with chronic rhinosinusitis. Toxicol Pathol. 2009;37: 594–8.
Durgam A, Batra PS. Paranasal sinus cholesterol granuloma: systematic review of diagnostic and management aspects. Int Forum Allergy Rhinol. 2013;3:242–7.
Mercan H, Edizer DT, Kilic E, Esen T, Ramazanoglu R, Cansiz H. Osseous metaplasia in a nasal polyp: report of a rare case and review of the literature. Ear Nose Throat J. 2012;91:E4–6.
Ramachandran K, Thomas MA, Denholm RB. Osseous metaplasia of a nasal polyp. J Otolaryngol. 2005;34:72–3.
Srouji S, Kizhner T, Ben David D, Riminucci M, Bianco P, Livne E. The Schneiderian membrane contains osteoprogenitor cells: in vivo and in vitro study. Calcif Tissue Int. 2009;84:138–45.
Lou H, Meng Y, Piao Y, Wang C, Zhang L, Bachert C. Predictive significance of tissue eosinophilia for nasal polyp recurrence in the Chinese population. Am J Rhinol Allergy. 2015;29:350–6.
Yaman H, Alkan N, Yilmaz S, Koc S, Belada A. Is routine histopathological analysis of nasal polyposis specimens necessary? Eur Arch Otorhinolaryngol. 2011;268:1013–5.
Schraven SP, Wehrmann M, Wagner W, Blumenstock G, Koitschev A. Prevalence and histopathology of chronic polypoid sinusitis in pediatric patients with cystic fibrosis. J Cyst Fibros. 2011;10:181–6.
Wu X, Amorn MM, Aujla PK, Rice S, Mimms R, Watson AM, Peters-Hall JR, Rose MC, Peña MT. Histologic characteristics and mucin immunohistochemistry of cystic fibrosis sinus mucosa. Arch Otolaryngol Head Neck Surg. 2011;137:383–9.
Mostafa HS, Fawzy TO, Jabri WR, Ayad E. Lymphatic obstruction: a novel etiologic factor in the formation of antrochoanal polyps. Ann Otol Rhinol Laryngol. 2014;123:381–6.
Taxy JB. Paranasal fungal sinusitis: contributions of histopathology to diagnosis: a report of 60 cases and literature review. Am J Surg Pathol. 2006;30:713–20.
Das A, Bal A, Chakrabarti A, Panda N, Joshi K. Spectrum of fungal rhinosinusitis; histopathologist’s perspective. Histopathology. 2009;54:854–9.
Hedayati MT, Pasqualotto AC, Warn PA, Bowyer P, Denning DW. Aspergillus flavus: human pathogen, allergen and mycotoxin producer. Microbiology. 2007;153:1677–92.
Sandison AT, Gentles JC, Davidson CM. Aspergilloma of paranasal sinuses and orbit in Northern Sudanese. Sabouraudia. 1967;6:57.
Miloshev B. Aspergilloma of paranasal sinuses and orbit in Northern Sudanese. Lancet. 1966;1(7440):746.
Borish L, Rosenwasser L, Steinke JW. Fungi in chronic hyperplastic eosinophilic sinusitis: reasonable doubt. Clin Rev Allergy Immunol. 2006;30:195–204.
Chakrabarti A, Denning DW, Ferguson BJ, Ponikau J, Buzina W, Kita H, Marple B, Panda N, Vlaminck S, Kauffmann-Lacroix C, Das A, Singh P, Taj-Aldeen SJ, Kantarcioglu AS, Handa KK, Gupta A, Thungabathra M, Shivaprakash MR, Bal A, Fothergill A, Radotra BD. Fungal rhinosinusitis: a categorization and definitional schema addressing current controversies. Laryngoscope. 2009;119:1809–18.
Ferguson BJ. Eosinophilic mucin rhinosinusitis: a distinct clinicopathological entity. Laryngoscope. 2000;110:799–813.
Guo C, Ghadersohi S, Kephart GM, Laine RA, Sherris DA, Kita H, Ponikau JU. Improving the detection of fungi in eosinophilic mucin: seeing what we could not see before. Otolaryngol Head Neck Surg. 2012;147:943–9.
Uri N, Ronen O, Marshak T, Parpara O, Nashashibi M, Gruber M. Allergic fungal sinusitis and eosinophilic mucin rhinosinusitis: diagnostic criteria. J Laryngol Otol. 2013;127:867–71.
Nicolai P, Lombardi D, Tomenzoli D, Villaret AB, Piccioni M, Mensi M, Maroldi R. Fungus ball of the paranasal sinuses: experience in 160 patients treated with endoscopic surgery. Laryngoscope. 2009;119:2275–9.
Stammberger H, Jakse R, Beaufort F. Aspergillosis of the paranasal sinuses X-ray diagnosis, histopathology, and clinical aspects. Ann Otol Rhinol Laryngol. 1984;93:251–6.
Odell E, Pertl C. Zinc as a growth factor for Aspergillus sp. and the antifungal effect of root canal sealants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79:82–7.
Senocak D, Kaur A. What’s in a fungus ball? Report of a case with submucosal invasion and tissue eosinophilia. Ear Nose Throat J. 2004;83:696–8.
Rhodes JC, Bode RB, McCuan-Kirsch CM. Elastase production in clinical isolates of Aspergillus. Diagn Microbiol Infect Dis. 1988;10:165–70.
Ibrahim AS, Spellberg B, Walsh TJ, Kontoyiannis DP. Pathogenesis of mucormycosis. Clin Infect Dis. 2012;54:S16–22.
Simão I, Gaspar I, Faustino R, Brito MJ. Rhinoscleroma in a 5-year-old Portuguese child. Pediatr Infect Dis J. 2014;33:774–5.
Botelho-Nevers E, Gouriet F, Lepidi H, Couvret A, Amphoux B, Dessi P, Raoult D. Chronic nasal infection caused by Klebsiella rhinoscleromatis or Klebsiella ozaenae: two forgotten infectious diseases. Int J Infect Dis. 2007;11:423–9.
Chan TV, Spiegel JH. Klebsiella rhinoscleromatis of the membranous nasal septum. J Laryngol Otol. 2007;121:998–1002.
Maguiña C, Cortez-Escalante J, Osores-Plenge F, Centeno J, Guerra H, Montoya M, Cok J, Castro C. Rhinoscleroma: eight Peruvian cases. Rev Inst Med Trop Sao Paulo. 2006;48:295–9.
de Pontual L, Ovetchkine P, Rodriguez D, Grant A, Puel A, Bustamante J, Plancoulaine S, Yona L, Lienhart PY, Dehesdin D, Huerre M, Tournebize R, Sansonetti P, Abel L, Casanova JL. Rhinoscleroma: a French national retrospective study of epidemiological and clinical features. Clin Infect Dis. 2008;47:1396–402.
Wright J. A nasal sporozoon. (Rhinosporididium kinealyi). NY Med J. 1907;86:1149–53.
Justice JM, Solyar AY, Davis KM, Lanza DC. Progressive left nasal obstruction and intermittent epistaxis. JAMA Otolaryngol Head Neck Surg. 2013;139:955–6.
Mukherjee B, Mohan A, Sumathi V, Biswas J. Infestation of the lacrimal sac by Rhinosporidium seeberi: a clinicopathological case report. Indian J Ophthalmol. 2013;61:588–90.
Choudhury M. Rhinosporidium seeberi in nasal smears. Diagn Cytopathol. 2011;39:593–4.
Gichuhi S, Onyuma T, Macharia E, Kabiru J, Zindamoyen AM, Sagoo MS, Burton MJ. Ocular rhinosporidiosis mimicking conjunctival squamous papilloma in Kenya – a case report. BMC Ophthalmol. 2014;14:45.
Mithal C, Agarwal P, Mithal N. Ocular and adnexal rhinosporidiosis: the clinical profile and treatment outcomes in a tertiary eye care centre. Nepal J Ophthalmol. 2012;4:45–8.
Norman WG. Rhinosporidiosis in Texas. Arch Otolaryngol. 1960;72:361–2.
Lasser A, Smith HW. Rhinosporidiosis. Arch Otolaryngol. 1976;102:308–10.
Jimenez JF, Young DE, Hough AJ. Rhinosporidiosis. A report of two cases from Arkansas. Am J Clin Pathol. 1984;82:611–25.
Naik RS, Siddiqui RS, Naik V. Urethronasal rhinosporidiosis. J Indian Med Assoc. 1979;72:238–9.
Herr RA, Ajello L, Taylor JW, Arseculeratne SN, Mendoza L. Phylogenetic analysis of rhinosporidium seeberi’s 18S small-subunit ribosomal DNA groups this pathogen among members of the protoctistan mesomycetozoa clade. J Clin Microbiol. 1999;37:2750–4.
Vilela R, Mendoza L. The taxonomy and phylogenetics of the human and animal pathogen Rhinosporidium seeberi: a critical review. Rev Iberoam Micol. 2012;29: 185–99.
Mc Clatchie S, Warambo MW, Bremner AD. Myospherulosis: a previously unreported disease? Am J Clin Pathol. 1969;51:699–704.
Kyriakos M. Myospherulosis of the paranasal sinuses, nose and middle ear. A possible iatrogenic disease. Am J Clin Pathol. 1977;67:118–30.
Rosai J. The nature of myospherulosis of the upper respiratory tract. Am J Clin Pathol. 1978;69:475–81.
Sindwani R, Cohen JT, Pilch BZ, Metson RB. Myospherulosis following sinus surgery: pathological curiosity or important clinical entity? Laryngoscope. 2003;113:1123–7.
Kaul R, Chander B, Dogra SS. Myospherulosis in the nose: a report of an unusual lesion. Indian J Pathol Microbiol. 2014;57:338–9.
Coulier B, Desgain O, Gielen I. Sinonasal myospherulosis and paraffin retention cysts suggested by CT: report of a case. Head Neck Pathol. 2012;6:270–4.
Syed SP, Wat BY, Wang J. Pathologic quiz case: a 55-year-old man with chronic maxillary sinusitis. Synchronous occurrence of Aspergillosis and myospherulosis. Arch Pathol Lab Med. 2005;129:e84–6.
Phillip V, Becker K, Bajbouj M, Schmid RM. Myospherulosis. Ann Diagn Pathol. 2013;17:383–9.
Lin HW, Handzel O, Faquin WC, Gopen Q. Myospherulosis from antibiotic ointment in the postoperative mastoid space. Am J Otolaryngol. 2010;31:205–88.
Godman GC, Churg J. Wegener’s granulomatosis: pathology and review of the literature. AMA Arch Pathol. 1954;58:533–53.
Klinger H. Grenzformen der Periarteriitis Nodosa. Frankf Z Pathol. 1931;42:455–80.
Wegener F. Ueber generalisierte septische Gefäßerkrankungen. Verh Deut Ges Pathol. 1936;29:202–10.
Wegener F. Ueber eine eigenartige rhinogene Granulomatose mit besonderer Beteiligung des Arteriensystems und der Nieren. Beitr Pathol Anat. 1939;102: 30–68.
Woywodt A, Haubitz M, Haller H, Matteson EL. Wegener’s granulomatosis. Lancet. 2006;367:1362–6.
Feder BJ. A Nazi past casts a pall on name of a disease. The New York Times. 2008. http://www.nytimes.com/2008/01/22/health/22dise.html?_r=1&oref=slogin. Accessed 19 Nov 2014.
Falk RJ, Gross WL, Guillevin L, Hoffman GS, Jayne DR, Jennette JC, Kallenberg CG, Luqmani R, Mahr AD, Matteson EL, Merkel PA, Specks U, Watts RA, American College of Rheumatology; American Society of Nephrology; European League Against Rheumatism. Granulomatosis with polyangiitis (Wegener’s): an alternative name for Wegener’s granulomatosis. Arthritis Rheum. 2011;63:863–4.
Muller K, Lin JH. Orbital granulomatosis with polyangiitis (Wegener granulomatosis): clinical and pathologic findings. Arch Pathol Lab Med. 2014;138:1110–4.
Taylor SC, Clayburgh DR, Rosenbaum JT, Schindler JS. Progression and management of Wegener’s granulomatosis in the head and neck. Laryngoscope. 2012;122:1695–700.
Gajic-Veljic M, Nikolic M, Peco-Antic A, Bogdanovic R, Andrejevic S, Bonaci-Nikolic B. Granulomatosis with polyangiitis (Wegener’s granulomatosis) in children: report of three cases with cutaneous manifestations and literature review. Pediatr Dermatol. 2013;30:e37–42.
Olsen KD, Neel 3rd HB, Deremee RA, Weiland LH. Nasal manifestations of allergic granulomatosis and angiitis (Churg-Strauss syndrome). Otolaryngol Head Neck Surg. 1980;88:85–9.
Devaney KO, Travis WD, Hoffman G, Leavitt R, Lebovics R, Fauci AS. Interpretation of head and neck biopsies in Wegener’s granulomatosis. A pathologic study of 126 biopsies in 70 patients. Am J Surg Pathol. 1990;14:555–64.
Del Buono EA, Flint A. Diagnostic usefulness of nasal biopsy in Wegener’s granulomatosis. Hum Pathol. 1991;22:107–10.
Colby TV, Tazelaar HD, Specks U, DeRemee RA. Nasal biopsy in Wegener’s granulomatosis. Hum Pathol. 1991;22:101–4.
Bajema IM, Bruijn JA. What stuff is this! A historical perspective on fibrinoid necrosis. J Pathol. 2000;191:235–8.
Jennette JC. Nomenclature and classification of vasculitis: lessons learned from granulomatosis with polyangiitis (Wegener’s granulomatosis). Clin Exp Immunol. 2011;164 Suppl 1:7–10.
Chang SY, Keogh KA, Lewis JE, Ryu JH, Cornell LD, Garrity JA, Yi ES. IgG4-positive plasma cells in granulomatosis with polyangiitis (Wegener’s): a clinicopathologic and immunohistochemical study on 43 granulomatosis with polyangiitis and 20 control cases. Hum Pathol. 2013;44:2432–7.
Author information
Authors and Affiliations
Appendices
Self Study
-
1.
Which statement is true?
-
(a)
Rhinophyma is caused by von Frisch bacilli.
-
(b)
Myospherulosis is caused by mycoplasma.
-
(c)
Chronic invasive fungal sinusitis is the only condition in which fungal sexual reproduction occurs.
-
(d)
Invasive fungal hyphae are observable on hematoxylin and eosin stained slides.
-
(a)
-
2.
Which statement/statements is/are true?
-
(a)
Allergic mucin is composed of degranulated eosinophils, Charcot Leydin crystals, and fungal hyphal fragments.
-
(b)
Antrochoanal polyps arise at the posterior choanae, and prolapse anteriorly through the nares, and are histologically characterized by a “strange emptiness” and bizarre fibroblasts.
-
(c)
Iron-like signaling is characteristic of a fungal ball.
-
(d)
a, b, c
-
(e)
a and c
-
(a)
Answers
-
1.
Which statement is true?
-
(a)
Rhinophyma is characterized by pronounced sebaceous hyperplasia, cystically dilated ducts filled with keratin and sebum, vasodilatation in the upper and middle dermis, and perivascular/perifollicular inflammation (Fig. 2.21 self study).
Fig. 2.21 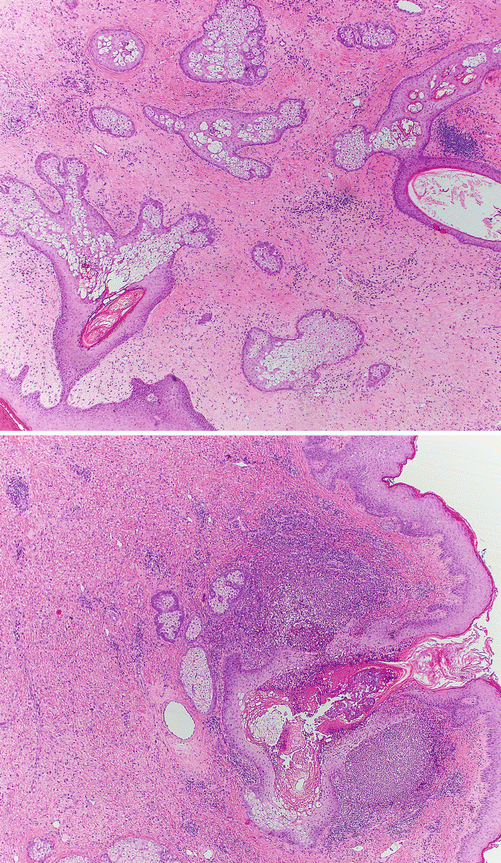
Self study
-
(b)
Myospherulosis is a non-infectious inflammatory reaction to agents such as exogenous lipids (e.g., petroleum, lanolin), vitamin E, or traumatized adipose tissue, resulting in the histological hallmark of pseudofungal “spherules”.
-
(c)
Sexual reproduction can be seen in a fungus ball, in the form of fruiting heads.
-
(d)
Invasive fungal hyphae are observable on hematoxylin and eosin stained slides – CORRECT. After systemic therapy, silver stains are necessary to observe hyphae.
-
(a)
-
2.
Which statement/statements is/are true?
-
(a)
Fungal hyphal fragments are not necessarily present in allergic mucin.
-
(b)
Antrochoanal polyps arise in the maxilla and can protrude through the posterior choanae.
-
(c)
Iron-like signaling is characteristic of a fungal ball. CORRECT. Iron-like radiographic signaling reflects the iron, manganese, and calcium content of fungal hyphae.
-
(a)

Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Brandwein, M.S. (2016). Sinonasal Tract: Nonneoplastic. In: Textbook of Head and Neck Pathology. Springer, Cham. https://doi.org/10.1007/978-3-319-33323-6_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-33323-6_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-33321-2
Online ISBN: 978-3-319-33323-6
eBook Packages: MedicineMedicine (R0)