
Abstract
The inferior gluteal artery perforator flap, which is vascularized by perforator branches of the inferior gluteal artery (formerly ischiatic artery) is harvested in the gluteal crease. The purpose of this anatomical study was to clarify the anatomical features of this flap and locate the perforators of the inferior gluteal artery destined to the flap, in view to facilitate its surgical removal, as free flap for breast reconstruction.. The authors performed 12 dissections on fresh cadavers, after selective injection of the inferior gluteal artery with a gelled solution. During harvesting the perforators were located which arise from the inferior gluteal artery and perfuse the flap. There are four zones, defined relatively to anatomical landmarks of the region, according to the frequency of perforators. This anatomical study enables to steer the surgical harvesting of this flap in its free shape for breast autologous reconstruction especially given its numerous advantages: a constant volume of fat even in thin patients and minimal donor site morbidity.
Similar content being viewed by others

Keywords
- Breast Reconstruction
- Perforator Flap
- Skin Paddle
- Posterior Superior Iliac Spine
- Autologous Reconstruction
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Breast reconstruction techniques are using an increasing number of autologous flaps. The increasing use of DIEP is the best illustration. However, this latter can only be sampled from patients having an abdominal wall without scars and lends itself to a dermolipectomy. In addition, the gluteal area, with its consistent blubber even on thinner patients, offers the possibility of sampling a perforator flap at the gluteal sulcus, while preserving the underlying muscle. For that reason, the Inferior Gluteal Artery Perforator (IGAP) flap could be an interesting alternative for autologous reconstruction on patients with a deep inferior epigastric perforator DIEP flap contraindication. Very little studies are in the literature through an anatomical dissection to specify its main features. The authors performed a mapping of the perforator branches of this flap, in order to ease its surgery removal.
2 Technique
An anatomical study on 12 gluteal areas was carried out on six fresh cadavers. The gluteal areas were injected by a pigmented gelatinized and radio-opaque solution.
2.1 Injection Technique
The solution injected was made of 50 mL of contrast dye (micropac: barium sulphate microraffine) plus 5 g of edible gelatine plus dye (a bulb of methylene blue). The inferior gluteal artery (IGA) was marked at the level of its emergence point on the pelvic region, and catheterized with a 10 ch probe. A skin incision on the banks of the flap was carried out to assess the good dissemination of the product. In a prime time, the arterial network was washed by lukewarm water, and then injected by the prepared product. The volume injected was determined by the product’s extravasation on the banks. The corpse was then put back in the refrigerator for 24 h. The flap dissection was performed the next day.
2.2 Dissection Technique
2.2.1 Flap Alignment
The authors chose the simple anatomical and reproducible marks; the bone marks of the gluteal area posterior superior iliac spine (PSIS), the ischial tuberosity (I) and the greater trochanter (T) and the skin folds limiting each area inside and at the bottom (median line and the inferior gluteal sulcus) (Fig. 4.1). The paddle was drawn under the shape of a horizontal ellipse following the gluteal sulcus direction, two thirds above and a third below the latter. Its width was rated in order to get a self-closing paddle.

The bone marks of the gluteal area posterior superior iliac spine (PSIS), the ischial tuberosity and the greater trochanter and the skin folds limiting each area inside and at the bottom (median line and the inferior gluteal sulcus)
2.2.2 Paddle and Perforator Dissection
According to the drawing, there is cutting the skin, subcutaneous tissue and fascia. The dissection that started at the level of the inferior bank was carried out in the subfascial plan by marking the lower edge of the gluteus maximus muscle as well as perforators intended for the paddle (Fig. 4.2). The perforators arteries diameter that are greater than or equal to 1 mm (under magnifying lamp), with their concomitant veins were followed through the muscle fascicles, which were spread to allow a deep dissection. The dissection continued under the muscle up to their origin on the IGA. The pedicle was then cut and the flap removed. The descending branch of the IGA and the posterior femoral cutaneous nerve were identified. At the level of the donor site, we have identified all the other perforators intended for the paddle. The latter were cut and marked by pins at the muscle surface.

The dissection that started at the level of the inferior bank was carried out in the subfascial plan by marking the lower edge of the gluteus maximus muscle as well as perforators intended for the paddle
3 Measures
3.1 Study Technique
In addition to the conventional measures carried out with the help of a plastic vernier caliper (Model 700-127 Mitutoyo) whose accuracy is of plus/minus 0.2 mm, photos were taken of the different gluteal areas in a standardized manner (same digital camera with the same settings) and carry out X-ray (standard and computed tomography).
Given the difference in size and of gluteal area’s shape depending on the thickness and the sex of the specimen, all the photographs have been standardized in size (300–500 pixels) and laterality (right side) by using the Software Adobe Photoshop CS3 and Adobe Illustrator CS3 (Adobe Systems, Inc. San Jose, Calif.) aiming to obtain superimposed data in the form of similar tracings in size and orientation (Figs. 4.3, 4.4, 4.5, and 4.6).

Perforators are marked and superimposed in the form of similar tracings in size and orientation
3.2 Studied Criteria
In the course of all our dissections the following criteria was noted:
-
1.
IGA’s origin in relation to the area’s marks.
-
2.
Flap size (length, width and thickness in centimeters).
-
3.
Pedicle length (linked with the paddle at the IGA emergence at the level of the gluteal area) in centimeters and its diameter (at the IGA origin) in millimeters.
-
4.
The perforators (all the perforators located on the area corresponding to the paddle): their number, type (myocutaneous or cutaneous) and their topography.
4 Results
4.1 Inferior Gluteal Artery Origin
At the level of the gluteal area, the point (where IGA emerges from the pelvic cavity) is projected at 0.7 plus/minus 0.2 cm inside the half of the line between PSIS and I (Fig. 4.7).

At the level of the gluteal area, the point (where IGA emerges from the pelvic cavity) is projected at 0.7 ± 0.2 cm inside the half of the line between PSIS posterior superior iliac spine and IGA inferior gluteal artery
4.2 Flap Size
The average dimensions of the paddle skin sampled were between 22.1 and 10.2 cm (edges paddles: between 16 and 9.5 and between 27 and 11.5). The thickness varied according to the corpse’s adiposity and was on average 4 cm.
4.3 Pedicle Length and Diameter
The pedicle average length was 15.8 cm (with edges between 14 and 18 cm). The pedicle average size at his origin was of 2.3 mm for the artery and 2.1 mm for the vein, compliant caliber with a microsurgery.
4.4 Perforators
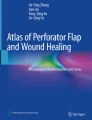
The number of perforators found by the paddle was of 10.3 on average (with edges ranging from 7 to 14) (Fig. 4.8). The perforator caliber could not be noted due to the lack of precision of such measure. Their caliber was however visually satisfactory (>1 mm under magnifying lamp). The perforators were mainly myocutaneous (97.1 %). The three cutaneous perforators found were localized at the level of the medial angle of the skin flap and quickly linked with the IGA origin; they gave short pedicle and therefore less interesting on the surgical plan. In order to establish a mapping of available perforators at the level of the sampling areas of the paddle, we have superimposed tracings of all gluteal areas dissected on which we had marked the perforators (Fig. 4.5). The perforators are localized predominantly at the level of the central part of the skin paddle (2nd 3rd quarters) (Fig. 4.9). This is confirmed also on the standard X-ray and the CT scan sections (Figs. 4.10 and 4.11)

The number of perforators found by the paddle was of 10.3 on average (with edges ranging from 7 to 14)

The perforators are localized predominantly at the level of the central part of the skin paddle (2nd 3rd quarters)

Perforators confirmed on standard x-ray PSIS posterior superior iliac spine, I ischiopubic ramus, T Tuberosity

Perforators confirmed on CT scan
5 Discussion
In 1975, Fujino was the first to use the gluteal area as a donor site for a breast reconstruction by using a myocutaneous gluteal flap [1]. In 1983, Shaw [2] insisted on the use of this flap in case of TRAM contraindication. The inferior gluteal flap was described initially in its myocutaneous shape to rebuild a breast in 1978 by Le Quang [3]. The inferior gluteal myocutaneous flap has been included in a wider range by Paletta et al. in 1989 [4] but seemed to create sequelae at the level of the supplying area. And then, Allen, in 1993 [5], introduced the perforator gluteal flap (Superior Gluteal Artery Perforator Flap “SGAP Flap”) for breast reconstructions, in order to preserve the underlying muscle and avoid the functional sequelae. Then, the technique was enhanced. Blondeel in 1999 suggested breast reconstructions with sensate SGAP flap [6]. And in 2002, Higgins described the first Inferior Gluteal Artery Perforator flap “ IGAP Flap”, as a means of coverage of ischial pressure sores [7]. Finally, in 2006 Allen et al. [8] reported the use of this flap in breast reconstruction, by sampling it in the gluteal sulcus to reduce not only the pain but also scars.
In recent years, the evolution in breast reconstruction is more and more using autologous tissue [9–11]. And since the advent of perforator flap they are booming, relying on their growing use of DIEP, or the more recent superior and inferior gluteal perforator flap which represented the first alternative for some surgeons to DIEP [8, 12, 13]. The interest of these perforator flaps in breast reconstruction is no longer doubtful [6, 10–23]. Indeed, in addition to their cosmetic satisfactory and durable results, they would also help to reduce the rate of complications, the length of hospital stay or even the global cost of autologous breast reconstruction [24, 25]. Compared to other processes, the inferior gluteal flap seems to have certain strengths [8, 13, 21]. It brings a volume of autologous tissue satisfactory, with a pedicle long enough to allow proper positioning of the paddle and different possibilities of anastomotic (internal thoracic artery or axillary artery) [8], while leaving little sequelae at the level of the donor site: the muscle is preserved and the sciatic nerve is protected, unlike the myocutaneous flap [5, 8] and finally, the scar in gluteal sulcus does not disrupt the aesthetic unit of the buttock unlike the SGAP flap [26]. In addition, this flap could be used even on thinner patients, since the buttocks volume is relatively constant unlike the abdominal panicle [21].
The potential indications of this flap would therefore be the breast reconstructions on patients who desire or require an autologous reconstruction, with a contralateral breast of medium volume non-ptosis [11] and a sufficient gluteal volume, when the abdomen is low or unusable [8, 21]; low BMI, liposuction history [27] or abdominal surgery, or among those which the DIEP or TRAM have already been used [8], or candidates for a bilateral reconstruction [28], or simply who choose this flap to avoid an abdominal scar and a hairiness ascension, particularly among the young nulliparous with a harmonious belly [8]. Not easy as it sounds, the sampling technique seems to be comparable in challenge with the one of other perforator flaps used in reconstructive surgery. And if the surgery duration could be one of its disadvantages [21], the prior anatomy knowledge of this flap before its achievement could help to save precious time before initiating the micro surgical time. If the perforator flaps are led to become the standard techniques in autologous breast reconstruction [24], the gluteal perforator flap remains, however, less studied than the other. In the literature there are very few anatomical studies of this flap [29, 30] and still a less number of studies having a practical impact on its use in breast reconstruction. Either it is about anatomical studies of its pedicle shape for a use in the coverage of ischial pressure sores [31, 32], or studies that are limited to the vascular anatomy of the region by X-ray explorations without however being specific to the exclusive territory of the IGA [33–35], or even of anatomical dissections focusing primarily on the relationship between the descending IGA branch and the posterior femoral cutaneous nerve which must be preserved during the sampling, and which does not seem to cause any problems at the time of the perforator flap sampling in its free shape [36].
The objective of the study was therefore to clarify the anatomical features of this flap that is less studied. Also, we have been able to describe its sampling technique and to define areas where the perforators, originating from the IGA and intended for the flap paddle, were the most frequently found.
Because, although currently, the evolution of X-ray explorations allows a localization more reliable of perforators in preoperative [34, 35], these reviews developed and sometimes expensive are however not of current practice in all centers [37], without mentioning their potential risks (radiation, allergy to iodine..). This is why we believe that this repartition of perforators in four sectors, perfectly reproducible on a patient in operating position (because it was made in accordance with fixed anatomical marks), would allow to save a precious time before we begin the microsurgery. Actually, this simple drawing of perforating sectors frequency may guide the search for perforators in operating room or in preoperative by Doppler, when it is possible [8, 37, 38].
In the rare anatomical dissections traced in the literature, the topography of the IGA perforator were lacking precision and was not based on specific marks. Ahmadzadeh et al. [29] noted a concentration of perforators on a line in the middle third of the gluteal region beside the gluteal sulcus. This is confirmed in our diagram prepared with more accuracy and reproducibility. Mu et a. [30] have found a majority of perforators of wide caliber in the para-ischial side and central of the gluteal muscle without distinguishing between those who were originating from the IGA or on the SGA. Mapping of perforators has been made from a selective injection of the IGA (Fig. 4.12), which means that all the perforators listed originated from this artery. Other studies of the vascular anatomy of the region lacked precision or specificity and did not determine with certainty the origin of these perforating vessels [35, 39]. Similarly, if the X-ray studies were able to identify the perforators of a very small diameter (0.3 mm) and therefore report a more important number of perforators [35], this has no practical impact. These perforators are too small to be chosen as flap feeding arteries. In our study, we restricted ourselves to perforators with a macroscopically satisfactory diameter (>1 mm), and we have listed that those were being projected at the level of the skin paddle which were, therefore, interesting from surgical point of view.

(a, b) Mapping of perforators has been made from a selective injection of the IGA, which means that all the perforators listed originated from this artery
The drawing of this mapping has been done in a context close to the operative context, in an operative position and on a drawing paddle that is similar to a breast reconstruction. This localization of perforators has been carried out in a precise and reliable way, since the perforators, visually marked, have been marked directly on the surface corresponding to the skin paddle while the radiological studies although they provide a rich and complete iconography, are often supported by a radio surgery correlation [35]. Regarding the type of perforators, the majority of those found in the study were myocutaneous, confirming what has already been reported in other studies [29]. In practical application, apart from the drawing of the gluteal sulcus which will be in a standing position in vivo, all other chosen marks are reproducible and fixed marks, namely, the bone marks tangible in the gluteal area (PSIS, ischial tuberosity and trochanter). The paddle is drawn under the shape of a horizontal ellipse along the axis of the gluteal sulcus. It is considered appropriate to the position, two third above and a third below the fold in order to obtain a new fold in a symmetrical position linked to the contralateral fold. Its upper limit is marked in such a way as to include the perforators selected in the paddle. Its major axis follows the fold and its minor axis is determined in terms of the skin that is necessary for the breast reconstruction and tissue available on the donor site (self-closing).
The incision of the paddle perimeter arrives in depth up to muscular plan. The flap sampling started in the bottom and outside. The dissection is done in the sub-facial plan. Indeed, carrying the fascia, would ensure a greater vascular security, without compromising the underlying muscle [8]. In contrast with the sampling of the DIEP where we must leave the aponeurosis and thus ensure a parietal reinforcement, this could have parietal complications despite its minimal break [40]. The grease is cut into a bevel in the flap’s upper and lower parts, in order to include the maximum of tissue in the flap and refining the skin banks of the donor site. The sided perforators are preferred because they allow the obtaining of a longer pedicle and therefore a flap easier to position on the receiving area. When the pedicle chosen fits in the center of the flap, this would not facilitate its implementation in place and it is imperative to try to get a pedicle of sufficient length despite the challenges of additional sampling and sometimes the larger diameter of the vessels near their origin. It is sometimes possible to find a second or even a third perforator which joins the first (Fig. 4.13) flap that will be even better infused [8]. Once again, where the perforator(s) is/are found, dissection is continued through and under the muscle up to obtain a pedicle of length and diameter sufficient for its microsurgery use, according to the diameter of the recipient vessels. Through all our dissections, we have managed to avoid prejudicing the posterior femoral cutaneous nerve which walks with the inferior gluteal vessels.

It is sometimes possible to find a second or even a third perforator which joins the first flap that will be even better infused
Scheufler et al. [31] were particularly interested in the study of marks of this nerve in order to preserve it for the flap’s future use in its pedicled shape and possibly sensate to the coverage of pelvic sores. Zenn and Millard [41] have recently been able to prove that we could preserve at least a portion of the nerve in 94.5 % of gluteal myocutaneous flap dissections. This close relationship between the descending branch of the IGA and the nerve is particularly detrimental during the use of the flap in its pedicled shape and thus can restrict its rotation angle. This report seemed to us less restrictive at the time of perforator free flap sampling. Moreover, through a broad anatomical study (118 corpses), Windhofer et al. [36] have shown that we could remove safely a cutaneous or fasciocutaneous flap at this area without losing sensitivity in the upper side of the thigh. Furthermore, in the rare cases reported on which the nerve is cut off, hypoesthesia of the upper side of the thigh is rarely inconvenient [26, 28].
At the end of the harvesting, the possibility was confirmed of achieving this flap while restoring all the area’s ad integrum anatomy (preserving the gluteal muscle anatomy that protects the sciatic nerve and closing the donor site with a scar in the gluteal sulcus) (Figs. 4.14 and 4.15). If the position change in intraoperative could extend the duration of the intervention, during our dissections, the sampling of the flap seems perfectly compatible with a job in double team, in lateral decubitus. The first team would sample the flap while the second would prepare the receiving vessels at the axillary hollow [8]. The main limitations of our study are linked to an anatomical study on corpses. First of all, the gluteal sulcus drawing has been performed in a ventral decubitus and not in a standing position as it would be in vivo. The authors were not able to judge the in vivo quality of tissue to be transferred, such as the fat density at this level and its consequences on the breast steadiness to rebuild, or the texture compatibility and the skin color.

At the end of the harvesting, the possibility was confirmed of achieving this flap

Restoring all the area’s ad integrum anatomy (preserving the gluteal muscle anatomy that protects the sciatic nerve)
On the technical point of view, There was no real difficulty to dissect and to coagulate small branches in depth, near the pedicle origin. In addition, the fact that the flap study has been performed on corpses of old persons, with arterial disease and sometimes pelvic pressure sores, compromises significantly the blood supply of the area and the flap, reflected then in an inadequate injection of all the perforators and would suggest that the number of perforators would be more important among young women candidates for breast reconstruction.
The average length of pedicle found by the study (15.8 cm) is greater than the length of pedicle in the cases described in surgical sampling of this flap (8–11 cm) [8]. This is explained by the fact that, by working on corpses, there was no restriction to dissect the pedicle deep and closer to its origin. While during practice, this represented the whole challenge of the sampling, due to the number of collateral to dissect and tie at this level. If the pedicle dissection is moved forward, in practice, it is enough to stop at a sufficient length for the connection.
The average diameter of the vessels at their origin is slightly different in terms of the data found in the clinical cases described. Quite similar for the arteries (2.3 mm/2 mm) with a difference due essentially to cutting level, which was more proximal in the study. This difference is more significant for the veins (2.1 mm/3 mm) [8]. This is probably explained by the poor venous return on the corpses and therefore a partial filling of veins by the gelatinized solution, the diameter measured seems then smaller. Our measures remain however, closer with the in vivo data, comparatively to other anatomical studies [29].
Conclusions
Sampling of one or several perforators of the IGA, the Inferior Gluteal Perforator flap offers a pallet of size and texture satisfactory to reconstruct an average breast without ptosis, with less aesthetic sequelae. Through this anatomical study, the authors were able to achieve a mapping of its perforators, allowing us to guide the search in pre and intraoperative and thus easing its sampling. It is a useful prelude to the practical use of this flap which would require however to be completed by a clinical study.
The gluteal perforator flap seems to the authors to be an additional technique in the arsenal of the plastic surgeon who is interested in breast reconstruction. The autologous reconstruction and the weakness of sequelae of the donor site would be its main strengths. It could be an interesting alternative when the other techniques have already been used, contraindicated or simply refused by the patients.
References
Fujino T, Abe O, Enomoto K (1981) Primary reconstruction of the breast by free myocutaneous gluteal flap. Int Adv Surg Oncol 4(1):127–143
Shaw WW (1998) Superior gluteal free flap breast reconstruction. Clin Plast Surg 25(2):267–274
Le-Quang C (1992) Secondary microsurgical reconstruction of the breast and free inferior gluteal flap. Ann Chir Plast Esthet 37(6):723–741
Paletta CE, Bostwick J, Nahai F (1989) The inferior gluteal free flap in breast reconstruction. Plast Reconstr Surg 84(6):875–883
Allen RJ (1998) The superior gluteal artery perforator flap. Clin Plast Surg 25(2):293–302
Blondeel PN (1999) The sensate free superior gluteal artery perforator (S-GAP) flap: a valuable alternative in autologous breast reconstruction. Br J Plast Surg 52(3):185–193
Higgins JP, Orlando GS, Blondeel PN (2002) Ischial pressure sore reconstruction using an inferior gluteal artery perforator (IGAP) flap. Br J Plast Surg 55(1):83–85
Allen RJ, Levine JL, Granzow JW (2006) The in-the-fold inferior gluteal artery perforator flap for breast reconstruction. Plast Reconstr Surg 118(2):333–339
Patenotre P, Duquennoy-Martinot V, Capon N, Dumortier R, Pellerin P (2001) Reconstruction mammaires par lambeaux fessiers inferieurs libres. À propos de 34 cas chez 30 patientes. Ann Chir Plast Esthet 46(2):103–111
Rozen WM, Rajkomer AK, Anavekar NS, Ashton MW (2009) Post-mastectomy breast reconstruction: a history in evolution. Clin Breast Cancer 9(3):145–154
Howard MA, Mehrara B (2005) Emerging trends in microsurgical breast reconstruction: deep inferior epigastric artery perforator (DIEP) and the superior gluteal artery perforator (SGAP) flaps. Int J Surg 3(1):53–60
Matar N, Quilichini J, Bosc R, Benjoar MD, Lantieri L (2010) Reconstruction mammaire par lambeau de superior gluteal artery perforator (SGAP) sans changement d’installation. About eight cases. Ann Chir Plast Esthet 55(6):539–546
Granzow JW, Levine JL, Chiu ES, Allen RJ (2006) Breast reconstruction with gluteal artery perforator flaps. J Plast Reconstr Aesthet Surg 59(6):614–621
Blondeel PN, Morris S, Hallock G, Neligan P (2005) Perforator flaps: anatomy, technique and clinical applications. Quality Medical Publishing, Inc, Saint Louis
Saint-Cyr M, Schaverien MV, Rohrich RJ (2009) Perforator flaps: history, controversies, physiology, anatomy, and use in reconstruction. Plast Reconstr Surg 123(4):132e–145e
Massey MF, Spiegel AJ, Levine JL, Craigie JE, Kline RM, Khoobehi K, Erhard H, Greenspun DT, Allen RJ Jr, Allen RJ Sr, Group for the Advancement of Breast Reconstruction (2009) Perforator flaps: recent experience, current trends, and future directions based on 3974 microsurgical breast reconstructions. Plast Reconstr Surg 124(3):737–751
Granzow JW, Levine JL, Chiu ES, Allen RJ (2006) Breast reconstruction using perforator flaps. J Surg Oncol 94(6):441–454
Weiler-Mithoff E, Hodgson EL, Malata CM (2009) Perforator flap breast reconstruction. Breast Dis 16:93–106
Boyd JB, Gelfand M, Da Lio A, Shaw W, Watson JP (2009) Comparison of superior gluteal artery musculocutaneous and superior gluteal artery perforator flaps for microvascular breast reconstruction. Plast Reconstr Surg 123(6):1641–1647
Heitmann C, Levine JL, Allen RJ (2007) Gluteal artery perforator flaps. Clin Plast Surg 34(1):123–130
Beshlian KM, Paige KT (2008) Inferior gluteal artery perforator flap breast reconstruction. Am J Surg 195(5):651–653
Acosta R, Smit JM, Audolfsson T, Darcy CM, Enajat M, Kildal M, Liss AG (2010) A clinical review of 9 years of free perforator flap breast reconstructions: an analysis of 675 flaps and the influence of new techniques on clinical practice. J Reconstr Microsurg 27(2):91–98
Tseng CY, Lipa JE (2010) Perforator flaps in breast reconstruction. Clin Plast Surg 37(4):641–654
Allen R, Guarda H, Wall F, Dupin C, Glass C (1997) Free flap breast reconstruction: the LSU experience (1984–1996). J La State Med Soc 149(10):388–392
Kaplan JL, Allen RJ (2000) Cost-based comparison between perforator flaps and TRAM flaps for breast reconstruction. Plast Reconstr Surg 105(3):943–948
Hugon S, Schoofs M (2006) Compte rendu du XXIXe congrès du GAM. Société française de microchirurgie, le 31 mars et le 1er avril 2006. Bruxelles. Ann Chir Plast Esthet 51(6):547–550
De Frene B, Van Landuyt K, Hamdi M, Blondeel P, Roche N, Voet D, Monstrey S (2006) Free DIEAP and SGAP flap breast reconstruction after abdominal/gluteal liposuction. J Plast Reconstr Aesthet Surg 59(10):1031–1036
Levine JL, Miller Q, Vasile J, Khoobehi K, Craigie J, Wise MW, Allen RJ (2009) Simultaneous bilateral breast reconstruction with in-the- fold inferior gluteal artery perforator flaps. Ann Plast Surg 63(3):249–254
Ahmadzadeh R, Bergeron L, Tang M, Morris SF (2007) The superior and inferior gluteal artery perforator flaps. Plast Reconstr Surg 120(6):1551–1556
Mu LH, Yan YP, Luan J, Fan F, Li SK (2005) Anatomy study of superior and inferior gluteal artery perforator flap. Zhonghua Zheng Xing Wai Ke Za Zhi 21(4):278–280
Scheufler O, Farhadi J, Pierer G, Levin LS, Erdmann D (2006) The infragluteal perforator flap. Handchir Mikrochir Plast Chir 38(6):390–397
Scheufler O, Farhadi J, Kovach SJ, Kukies S, Pierer G, Levin LS, Erdmann D (2006) Anatomical basis and clinical application of the infra- gluteal perforator flap. Plast Reconstr Surg 118(6):1389–1400
Saint-Cyr M, Schaverien M, Arbique G, Hatef D, Brown SA, Rohrich RJ (2008) Three- and four-dimensional computed tomographic angiography and venography for the investigation of the vascular anatomy and perfusion of perforator flaps. Plast Reconstr Surg 121(3):772–780
Newman TM, Vasile J, Levine JL, Greenspun DT, Allen RJ, Chao MT, Winchester PA, Prince MR (2010) Perforator flap magnetic resonance angiography for reconstructive breast surgery: a review of 25 deep inferior epigastric and gluteal perforator artery flap patients. J Magn Reson Imaging 31(5):1176–1184
Rozen WM, Ting JW, Grinsell D, Ashton MW (2011) Superior and inferior gluteal artery perforators: in vivo anatomical study and planning for breast reconstruction. J Plast Reconstr Aesthet Surg 64(2):217–225
Windhofer C, Brenner E, Moriggl B, Papp C (2002) Relationship between the descending branch of the inferior gluteal artery and the posterior femoral cutaneous nerve applicable to flap surgery. Surg Radiol Anat 24(5):253–257
Hallock GG (2009) A primer of schematics to facilitate the design of the preferred muscle perforator flaps. Plast Reconstr Surg 123(3):1107–1115
Pérez de la Fuente T Bennett, González González I, Calderón Muñoz F (2008) The IGAP flap for ischial pressure sore reconstruction in tetraplegic patients. Int J Surg 6(6):e1–e3
Song WC, Bae SM, Han SH, Koh KS (2006) Anatomical and radiological study of the superior and inferior gluteal arteries in the gluteus maximus muscle for musculocutaneous flap in Koreans. J Plast Reconstr Aesthet Surg 59(9):935–941
Gill PS, Hunt JP, Guerra AB, Dellacroce FJ, Sullivan SK, Boraski J, Metzinger SE, Dupin CL, Allen RJ (2004) A 10-year retrospective review of 758 DIEP flaps for breast reconstruction. Plast Reconstr Surg 113(4):1153–1160
Zenn MR, Millard JA (2006) Free inferior gluteal flap harvest with sparing of the posterior femoral cutaneous nerve. J Reconstr Microsurg 22(7):509–512
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
El Omari, M., Casoli, V., Pinsolle, V. (2016). Inferior Gluteal Artery Perforator Flap: Anatomic Study. In: Shiffman, M. (eds) Breast Reconstruction. Springer, Cham. https://doi.org/10.1007/978-3-319-18726-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-18726-6_4
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18725-9
Online ISBN: 978-3-319-18726-6
eBook Packages: MedicineMedicine (R0)