
Abstract
This field study embodies S-BPM into organizational development processes, both methodologically, exploring how to capture work knowledge, and with respect to implementation, providing accurate specifications for process support. Eliciting and acquiring knowledge of work procedures have been exploited by means of Value Network Analysis (VNA). It engages stakeholders on elaborating by scenarios of work they have experienced and supports exploring opportunities of change in terms of exchanged deliverables along actor-specific communication structures. VNA roles correspond to subjects and interactional transactions to business objects. The approach has become part of an SOP for organizational development of clinics. We exemplify the development of patient-critical treatment planning in the University Clinic for Radiotherapy-Radiation Oncology.
You have full access to this open access chapter, Download chapter PDF
1 Introduction
The University Clinic for Radiotherapy-Radiation Oncology (ROI) is the Tyrol’s only radiotherapy facility, and thus represents a major part of the regional and national infrastructure in cancer medicine. About 70 % of all cancer patients of the federal state hospital (Landeskrankenhaus Innsbruck) are treated at the University clinic. The complexity of planning cancer treatment is reflected through involving staff from different professions and disciplines. In addition to the medical staff, radio technologists, medical physicists, technicians, biomedical analysts, psycho-oncologists and administrative staff form the planning team for patient treatment. In recent years the number of patients has started to increase significantly, resulting in a corresponding increase of services and treatment capabilities, in terms of both technical resources and personnel.
In order to ensure the professional development of the clinic its director launched an organizational development process after holding a strategy meeting involving its multi-professional management team. Major internal organizational issues were discussed, and a mission statement of the clinic has been released. To sustain it in daily routines, an organizational development project has been started. In addition, establishing specialized tumor group treatment as part of organization’s structural change should be explored. The project’s management team specified two central objectives for the organizational development process :
-
developing task allocation models referring to job profiles, and
-
establishing regular communication patterns. In this context, motivation, job satisfaction, and professional handling of conflicts also played an important role.
The organizational development team of the umbrella organization Tiroler Landeskrankenanstalten GmbH (TILAK) set up a corresponding change project entitled “Reflect ROI” for one year. After refining the existing mission statement involving the extended leadership board, a workplace satisfaction survey was launched. All clinic staff was invited to judge the image and quality of patient management, the satisfaction with the content of work, the social relations (including management), and workplace conflict management.
Figure 3.1 shows the public and internal image including patient performance as judged by the various professional groups at ROI. While the various professional groups rated the image and performance quite highly (as indicated by the dot cloud on the right-hand side), the internal image of physician trainees (leftmost dot) has been perceived quite ambivalently.

Perceived image from outside
With respect to conflict handling, physician trainees questioned openly addressing conflicts and indicated the need for professional support for conflict management (upper and lower circled dots in Fig. 3.2).

Conflicts and their management
With respect to collaboration, again physician trainees did not experience team feeling and indicated the need for improving cooperation with administration and their peers (Fig. 3.3).

Team work
Finally, as indicated in the middle of Fig. 3.4, accomplishing core tasks when being on duty was not organized satisfactorily for physician trainees, besides the lack of cooperation of other ROI units and aligning private and occupational duties.

Evaluating the organization of work
In a follow-up (one-day) workshop representatives from all occupational groups across hierarchical positions developed a vision of the future of the clinic. This vision should be put to operational practice by four working groups (WGs): Optimal Organization, Division of Labor, Professional Profiles, and Communication. All working groups were staffed inter-professionally by clinic members, and accompanied by the project team. The meetings had different formats: workshops, impulses, focus groups, solution development.
Concrete suggestions were discussed in a monthly meeting by the clinic’s internal working group leader with the director of the clinic, and their implementations were always jointly decided upon. In the following we focus on the Organizational Learning part of the project, namely detailing the approach of the working group Optimal Organization from a content and method perspective. It addressed the clinic’s communication and value-orientation along organizational development.
2 Initial Situation
The University Clinic for Radiotherapy-Radiation Oncology (ROI) has been organized in a function-oriented way. Hence, doctors were responsible only for selected aspects of the overall treatment. A closer doctor-patient relationship—such as the one established through initial interviews—was thereby prevented. In addition, the transfer of the patient information was incomplete and led to frequent losses of information. Compensating for these deficiencies still required lots of resources and continuously rebuilding of doctor-patient relationships.
Working along functional units as indicated above has been perceived as “assembly-line work” and created frustration albeit high patient satisfaction with the clinics’ performance according to the survey (see also in Fig. 3.1). However, the need for increasing consistency in medical care has been expressed by patients over and over again.
With regard to assigning physicians and the supervising wards (including his/ her own ward) the allocation of tasks and patient responsibility was not quite clear: Each patient could be in contact with four different units at the same time, according to the functional division of labor at the outpatient department, Linac team, tumor board and ward. This confusion also hindered sufficient time resources for each patient and focused academic work.
The working group had a core of two conductive senior physicians and 11 other members involving all other professions. Such cross-section of the clinic’s staff enabled consensus when formulating the problem statement to be handled in the context of the organizational development project:
Is there an optimal form organizing our work, which contributes to good patient care and high employee satisfaction as well as to an efficient use of resources?
It triggered the specific mandate of the working group:
Developing a model of how the work needs to be organized, ensuring optimal patient care, while improving employee satisfaction at ROI.
This mandate has been implemented by developing different possible variants, and revealing associated advantages and disadvantages by evaluating their consequences of a corresponding implementation. The latter should serve as a basis for optimizing the organizational structure of work.
With respect to methodological and practical know-how the project participants of ROI were neither educated in Organizational Design and Business Process Management, nor familiar with Workflow Management Systems. Hence, the elicitation and representation of work (process) knowledge had to be accompanied by informing activities.
3 Project Implementation
The ROI members of the working group together with the TILAK organizational development team defined the following procedure to achieve the objectives of the project:
-
1.
Documentation of current situation
-
2.
Development of model variants
-
3.
Analysis of the consequences of the models’ implementation
In order to perform these steps subject-oriented and systemic knowledge management methods were used, which were accompanied by an external consultant.
3.1 Documentation of the Current Situation
For the representation of the actual situation with regard to the operational and organizational structure of the University Clinic for Radiotherapy-Radiation Oncology, members of the working group modeled the structures and core processes of their clinic. In two workshops an interactive structure elaboration tabletop system was used. It allowed visualizing work knowledge (structures, processes, and the like) using three differently shaped elements and arbitrary relationships (see Fig. 3.5).

Interactive structure elaboration tabletop system. Adopted from Stary (2014)
After introducing the table and its functionalities, participants developed a common understanding on modeling their work. It supported their visualizing complex processes and structure requirements within a short period of time. A total of 12 models, three structure and nine flow models emerged:
-
Job/workspace structure
-
Overview of workspaces (see Fig. 3.6)
Fig. 3.6 
Structure model: overview of workspaces (upper part original pattern, lower part nodes with their main relationships). Adopted from Stary (2014)
-
Structure of out-patient department
-
Out-patient department process
-
Planning process
-
Linac process (see Fig. 3.7)
Fig. 3.7 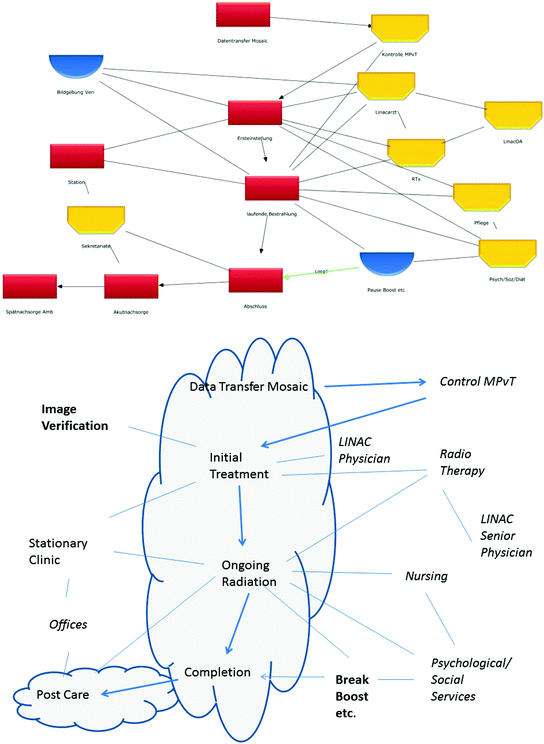
Flow model: Linac (upper part original pattern, lower part nodes with their main relationships)—core process elements are located in the cloud (lower part). Adopted from Stary (2014)
-
Brachytherapy process
-
Ward process
-
Emergency process on weekends and during holidays
-
Blood irradiation/experimental irradiation process
-
Benign diseases/conventional therapy process
-
Procurement process


The various elements were used with different meanings. In the structure model (see Fig. 3.6, the lower part shows excerpted text items with their main relationships), rectangle elements describe workspaces with direct patient reference. Semicircular elements represent workspaces which in part are already contained in the rectangle elements. They refer to planning as an essential element of radiotherapy. Hexagonal elements define workspaces without reference to patients, elaborating on the rectangle units. In this context, device management and the front office of the various work units were specified. The connections between the rectangle and hexagonal elements indicate the cooperation between the units. Once a semicircular element is connected, a ‘has-part’ or ‘recruits from’ relationship has been set. The structure model of all workspaces was used subsequently as a framework for the selection of the processes to be modeled.
In the follow-up (process) models, e.g., Fig. 3.7 (the lower part shows excerpted text items with their main relationships and the patient-relevant process in the cloud), rectangle elements define main process steps or top-level starting points triggering procedures. Semicircular elements specify major equipment or operators supplying additional information for the process. Hexagonal elements represent functions to be included in the course of patient-oriented planning, or responsible organizational units. Undirected connections represent bidirectional collaboration between groups of actors and responsibilities of persons for process steps. For in- stance, Linac physicians and radio technologists collaborate when being responsible for the initial setting for a patient at the Linac. Directed links enable mapping the sequence of process steps to the elaborated structure.
The application of the structure elaboration tabletop system revealed that professional groups such as physicians who are used to make decisions under time pressure in clinical practice, are highly active when the workshop participants were asked to model their work practice. The other professionals joined them once the initial elements had been identified, depending on the addressed actors and their process knowledge. The members of the working group evaluated the four processes “Linac”, “out-patient department”, “planning”, and “performance profile” in terms of critical success factors. They identified strengths, weaknesses, ideas for solutions to open problems, questions, and potential for improvement. These results formed the basis for the development of model variants. As each of the process models in the stakeholder-genuine notation included actor- and IT system-specific information elements as well as lines of communication, the most relevant input for subject-oriented representation had been provided.
3.2 Development of Model Variants
In order to develop and analyze appropriate models for optimizing the organization of work regarding patient care, use of resources, and employee satisfaction, two more workshops were conducted. At the beginning of the first workshop, the working group agreed on two favorable variants:
-
optimization of (existing) function-based process organization
-
organizing work according to tumor groups
For analysis and refinement of the two variants the participants split into two groups, each moderated by the TILAK organizational development team and an external consultant. In a first step the necessary functions/roles, tasks and tools were documented in a network of organizational activities utilizing HoloMapping (cf. vernaallee.com). The same symbol colors were used as for the structure elaboration on the tabletop system, namely hexagonal for functions/roles, rectangle for tasks, semicircular for work equipment and committees.
In addition, solid arrows (Tangibles ) visualized the information and knowledge exchange required for the fulfillment of tasks, whereas dashed arrows (Intangibles ) between the individual elements visualized experience knowledge and action-guiding values. Particularly controversial or dysfunctional exchange relationships were drawn in a dedicated color like the value-creating and neutral relationships (see Figs. 3.8 and 3.9).

HoloMap representing function-oriented organizational form. Adopted from Stary (2014)

HoloMap representing an organization of work according to tumor groups. Adopted from Stary (2014)
The collected hot spots (subscribed exchange relationships) of both forms of organization were formulated as critical success factors in each subgroup. Then, corresponding solution ideas were created and documented in tables—see, e.g., Table 3.1.
In order to further analyze the effect of the (critical) exchange relationships on sender and receiver or the entire organization, each deliverable was according to the Value Network Analysis (VNA) (cf. vernaallee.com). In addition to the already carried out Holomapping and exchange analysis (i.e. analysis of structures of the represented actor network), the VNA includes an Impact and Value Creation analysis for both, the communication-oriented reflection of the impact of values of existing exchange relations/activities, and value creation opportunities for individual participants and the overall organization of work. In the Impact Analysis , stakeholders identify which “deliverables” (=exchange/services) flow between the (critical) roles. A table is created for each role (see Table 3.2). It is listed therein which role receives inputs, from whom it receives these inputs, what activities are triggered at the respective role, and what effect on the used work equipment is experienced. In addition, corresponding intangible impacts, costs, risks and benefits are recognized.
Table 3.2 shows some data entries for the tumor board (role). The physician needs to specify for each incoming transaction of the Tumorboard (see rows of the table) the activities triggered by the input, the effort created by the input to the work flow for each actor, the immaterial (Intangible) effects on them, and the general costs and risks associated with the input. In this way, results that are not adequately achieved are questioned with respect to the usefulness of each deliverable.
The first data entry in the table exemplifies the input ‘patient information’ to the ‘Tumor Board’. It is delivered by the Assigning physician for decision making in the Tumorboard, based on the quality of received information. Currently the Tumorboard experiences a lack of information due to missing data. Planning overhead is high since the board does not issue demands for the missing information. Consequently, the risk of incorrect decision making is high. On the contrary, the benefit of complete information would be high, since it forms the basis for further work (treatment planning).
In the Value Creation Analysis (see Table 3.3) all outgoing transactions are discussed for each role, including the receiver and the value added. It needs to be documented by what activity a possible increase in value, e.g., a possible solution for a problem when organizing work, can be achieved. As in the Impact Analysis, also costs, risks and benefits arising from the respective outputs are documented.
For each role and output the following questions need to be answered: What intention (value) becomes visible with this output? What activities can be set to increase the value of this output from my side (enhancement from my perspective as an acting agent)? To which actor is my output delivered (as a sender)? What are the effort, risks, and benefits when creating additional value?
In our example, patient information should be delivered to the Tumorboard for a tele conference on time, based on the activities of the Assigning physician. Then therapeutic decisions could be based on complete information. The teleconference should demand full information from assigning physicians. A checklist for teleconferencing for assigning physicians could help to reduce additional search activities when completing the patient file which in turn could result in increased employee satisfaction.
Given the tables, fundamental subject-oriented model elements become available, namely subjects and messages. For instance, the Tumorboard and Assigning physician (Zuweiser) represent subjects. All incoming messages are identified naming the tangible deliverables in the table when filling in inputs in the course of the Impact Analysis (Table 3.2). All outgoing messages are listed in the course of the Value Creation Analysis (Table 3.3). They correspond to the tangible transactions with other subjects.
3.3 Analysis of the Consequences of Model Implementations
Detailing and systemically analyzing the two suitable variants for the implementation of an optimal form of organization at the University Clinic for Radiotherapy-Radiation Oncology showed that certain patterns of work behavior had been established over time. It also became evident that these patterns could be addressed independently of whether the current situation would be kept or not. They affected:
-
Organization of tumor boards
-
Completeness of assignments (Assigning physician)
-
Staff shortages
-
Incomplete performance measurement (number of patients)
-
Adherence to deadlines
-
Procedure of the afternoon meeting
Although organizing the work according to tumor groups would imply switching physicians at the interface Out-patient Department/Linac from the perspective of patients (which needs to be resolved separately), this shift would bring substantial benefits for the continuity of patient care and employee satisfaction. These issues were discussed in one of the monthly coordination meetings and redirected to the working group for detailing solution proposals.
Many of the inputs have been already elicited in the course of the Value Network Analysis or resulted from processing critical success factors of the HoloMap. In order to clarify medical staffing, the current staff allocation and the process of planning, including the highly debated service exchange, were again modeled on the structure elaboration tabletop system. Required changes could be derived from this session. In general, it was found that physicians have to be on-site for successful task accomplishment, in particular when the work is organized according to tumor groups.
In addition to the organization-independent optimization issues, the change to focused work areas (tumor groups) promised the following advantages:
-
Strengthening doctor-patient relationships
-
Clarification of ROI profile due to designated work areas
-
Provision of dedicated contact persons for patients, stationary units, and assigning physicians
-
Improvement of training
-
Simplification of planning absences, primarily when self-organizing them in each group
-
Clarification of responsibilities for tumor board representatives, case manager, and their substitutes
-
Promotion of special skills of individual employees
-
Improvements in recruiting patients for studies
-
Development of scientific priorities
-
Continuity of support and documentation of study patients
-
Increasing efficiency when introducing innovations
-
Increased continuity in caretaking of patients with combined tele-brachytherapy or combined photon-neutron therapy
-
Better integration and representation of part-time employees in a group.
4 Going Live
The trigger for implementing changes was the director asking the group leaders and the TILAK organizational development team to develop a business plan containing all necessary implementation steps. They critically reviewed the developments in healthcare with respect to
-
the structure of the task force according to tumor types
-
the composition of the focused working units
-
the required functions and tasks for each group
-
classifying medical staff
-
a planning procedure concerning the absence of doctors
-
clarifying organizational details and context, such as planning Linac slots, room layout, and late night services
-
providing contact persons for all occupational groups
-
training rotations
The implementation concept (being part of the business plan) included changes in physician staffing and patient assignment. Implementation should be supported by focus groups and specific case managers for each tumor group. The implementation also required some IT adaptations.
The business plan was presented to the management team of the University Clinic for Radiotherapy-Radiation Oncology. It agreed on a certain date for switching to the implementation of the novel concept. As a result, a further project, namely implementation support of the focus groups, was set up by the organizational development team of TILAK. This project comprised both all communication-related and all technical-organizational preparations for implementation. It also established the monthly reflection of the implementation status involving the focus group leaders and the management team of the clinic, allowing re-re-planning when required.
In the course of the implementation support project a short survey involving all staff members of the clinic was conducted. It focused on their expectations and barriers concerning the implementation. It is planned to repeat this survey one year after introducing the focus groups and establishing the tumor groups.
As an effective means of documentation and interaction with the IT department, subject-oriented models have been prepared, as exemplified by change requests by physicians to the operation manager in Fig. 3.10. The (re-)engineering process of the interactive application is done in collaboration with staff users and the TILAK organizational development team.

Sample subject behavior diagram : change request by Physicians to Operation Manager. Adopted from Stary (2014)
5 Conclusive Summary
From guiding the change processes several lessons became evident:
-
Rather than starting with a modeling session to analyze a situation of an organization or to capture stakeholder needs a goal setting procedure should be established. It gives an organizational unit and their members the chance to consolidate and formulate objectives that need to be graspable and transparent throughout a change project.
-
Rather than applying a predefined notation for articulating mental models and stakeholder needs an open format should be used allowing all stakeholders to express themselves according to their preferences and capabilities.
-
Rather than optimizing process for a group let the involved stakeholders develop alternatives and variants. Help them to identify relevant measures and schemes, such as success factors, as they have the relevant experience and domain knowledge for evaluation.
With regard to the methods used for the elaboration and analysis of the existing and envisioned situation, the interactive and haptic instrument of the tabletop system enabled a wide and active participation of the members of various professional groups without any special knowledge of work process modeling methods. In addition, the choice of this setting facilitated incorporating all occupational groups and their perspectives, regardless of hierarchy or position in professional groups. It allowed for profound, immediate involvement of different groups of employees. Despite lack of prior knowledge, the parties rapidly came to work with the structure elaboration technique, and developed a coherent and sustainable modeling logic.
The subsequent analysis of the models using VNA (Value Network Analysis) opened up reflecting on causal relationships of certain problems from the perspective of communication. In some cases, they could move to the center far-reaching effects of local problems on the entire organization as well as the effects of values guiding activities. The participants were able to visualize in this way what patterns are effective in their organization for functional activities or when difficulties occur. Thus, the identified hot spots could be processed step by step using the tabletop system and solutions could be developed in terms of added value for the clinic. Here, too, it turned out, in particular by observing four workshops, that the members of the working group could become familiar with the selected method very quickly. However, it should be noted that a moderation of the group is required, both in the use of structural elaboration tabletop system and when processing a HoloMap, i.e., performing value network analyses. It helps on the one hand keeping the focus on the content and the method, and on the other hand triggering questions for reflection, in order to direct participants towards problem solving.
The developed critical success factors provided a well-defined framework for quality assurance in the context of implementing a new organization of work at the clinic. Overall, the organization could profit from its knowledge about their accuracy and meet existing and emerging challenges successfully. It occurred in a way that the decision for selecting a specific organizational form could be based on relevant patterns of communication and underlying values, in addition to factual arguments. Hereby, subject-orientation provides focusing on acting parties and their interaction in terms of work-relevant deliverables. Besides a high-level view, role-specific behaviors can be specified accurately through S-BPM models.
References
Stary Ch (2014) Non-disruptive knowledge and business processing in knowledge life cycles—aligning value network analysis to process management. J Knowl Manage 18(4):651–686
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is distributed under the terms of the Creative Commons Attribution Noncommercial License, which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Copyright information
© 2015 The Author(s)
About this chapter
Cite this chapter
Augl, M., Stary, C. (2015). Communication- and Value-Based Organizational Development at the University Clinic for Radiotherapy-Radiation Oncology. In: Fleischmann, A., Schmidt, W., Stary, C. (eds) S-BPM in the Wild. Springer, Cham. https://doi.org/10.1007/978-3-319-17542-3_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-17542-3_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-17541-6
Online ISBN: 978-3-319-17542-3
eBook Packages: Computer ScienceComputer Science (R0)