
Abstract
This chapter provides an overview of both benign and malignant pleural disorders, starting with the relevant anatomy and physiology. The focus is on the management of pneumothoraces and pleural effusions—conditions that are commonly encountered on a general thoracic surgery service. The pleural cavity is lined by parietal and visceral pleura, which are smooth membranes that are continuous with one another at the hilum and pulmonary ligaments. Parietal Pleura: innermost chest wall layer, divided into cervical, costal, mediastinal and diaphragmatic pleura.
You have full access to this open access chapter, Download chapter PDF
Anatomy and Physiology
-
The pleural cavity is lined by parietal and visceral pleura, which are smooth membranes that are continuous with one another at the hilum and pulmonary ligaments.
-
Parietal Pleura: innermost chest wall layer, divided into cervical, costal, mediastinal and diaphragmatic pleura.
-
Arterial supply and venous drainage: systemic
-
Highly innervated by intercostal nerves responsible for somatic pain sensation when the parietal pleura is subjected to trauma (e.g. tube thoracostomy, thoracotomy) or tumour invasion
-
Phrenic nerve also innervates the mediastinal and diaphragmatic pleura
-
-
Visceral Pleura: layer covering both lungs
-
Arterial supply: systemic and pulmonary; venous drainage: pulmonary
-
Innervated by the autonomic nervous system
-
-
The two layers are separated by a thin layer of pleural fluid, which serves to allow transmission of forces from the chest wall to the lungs during inspiration and expiration.
-
Pleural fluid under normal conditions is about 0.25 mL/kg and is plasma-like consistency [1].
-
Pleural fluid turnover: 0.15 mL/kg/h [2].
-
The production and reabsorption of fluid is dictated by the Staling forces of parietal and visceral pleura capillaries (hydrostatic pressure, plasma oncotic pressure), as well as capillary permeability and the negative intrathoracic pressure. The lymphatics also have a significant ability to reabsorb large protein molecules and fluid. Any disruption or alterations of these mechanisms may lead to a pleural effusion.
-
Fluid moves via a net filtration gradient from the parietal pleura capillaries into the pleura, while fluid is reabsorbed generally by parietal pleural lymphatics.
-
The function of the pleural fluid is to decrease friction between the parietal and visceral pleura during respiration, allow apposition of the lungs to the chest wall and ensure coupling between the lung, chest wall and diaphragm to optimise ventilation.
-
Pneumothorax
Overview
-
Abnormal presence of air within the pleural cavity
-
Results in dissociation of the parietal and visceral pleura leading to a disruption of lung mechanics.
-
Lung compression reduces lung compliance, volumes and diffusion capacity.
Tension Pneumothorax
-
If left untreated, air can accumulate without decompressing adequately, leading to high positive pleural pressures, causing severe lung collapse, and compression of the mediastinum, great vessels and heart, and ultimately haemodynamic compromise.
-
Patients in tension pneumothorax require immediate clinical diagnosis, followed by needle decompression in the second intercostal space at the midclavicular line, followed by tube thoracostomy.
Aetiology (Table 4.1)
-
Spontaneous Pneumothorax: no underlying trauma or iatrogenic cause for pneumothorax
-
Primary Spontaneous Pneumothorax: no known underlying lung disease (Fig. 4.1)
Fig. 4.1. 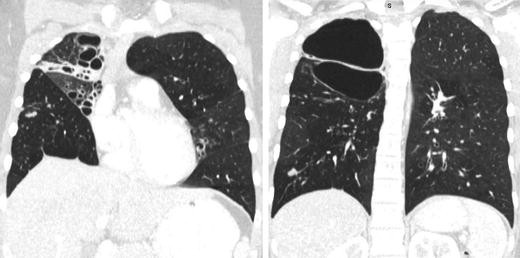
Chest CT of a 27-year-old patient with severe bullous disease. This patient suffered from recurrent primary spontaneous pneumothoraces.
-
Incidence 7.4/100,000 (men) and 1.2/100,000 (women) annually in the USA [3].
-
Caused by rupture of small bleb (bullae) usually in apices of upper or lower lobes, allowing air to leak into the pleural cavity.
-
80 % of patients will demonstrate emphysema-like changes on CT scan [4].
-
Occur most commonly in thin tall young male patients. Smoking and atmospheric pressures changes are also risk factors [5].
-
-
Secondary Spontaneous Pneumothorax: known underlying lung disease.
-
Incidence 6.3/100,000 (men) and 2.0/100,000 (women) annually in the USA [3].
-
Underlying disease causing rupture and air leak
-

Clinical Presentation
-
Pleuritic chest pain and dyspnea (most common)
-
Physical examination may be normal if the pneumothorax is <25 %.
-
Decreased breath sounds, hyperresonance on the affected side (not always present)
-
Subcutaneous emphysema
-
Tension pneumothorax also presents with tracheal deviation to the contralateral side, severe respiratory distress and haemodynamic instability.
-
Rarely: pneumomediastinum or pneumopericardium (Hamman’s sign)
-
-
Diagnosis is established by an upright chest X-ray (Fig. 4.2). If clinical signs of tension physiology are evident, X-ray confirmation should be omitted and immediate decompression should ensue.
Fig. 4.2. 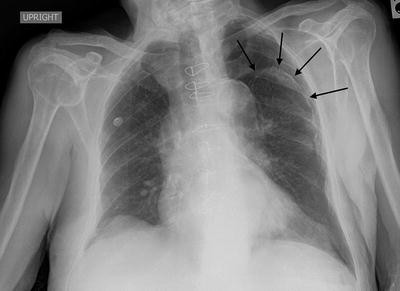
Patient presenting with a traumatic pneumothorax after blunt trauma to the chest. Black arrows denote the outline of the collapsed lung.
-
Expiratory view accentuates the separation of the parietal and visceral pleura.
-
Pneumothorax in supine patients accumulates into the dependent regions of the anterior and subdiaphragmatic pleura and may be detected as a deep sulcus sign.
-
Although CT scan is the gold-standard for diagnosis, it is not necessary for the majority of patients with first-episode spontaneous pneumothorax since it does not change the management.
-
Ultrasound is also an accurate, rapid and non-invasive test, yet requires operator experience.
-

Management
-
The aetiology largely dictates both immediate and definitive management.
-
Observation:
-
Reserved for asymptomatic patients with a small pneumothorax who are unlikely to have an ongoing air leak. Follow-up radiography should be obtained within 24–48 h to document improvement.
-
Supplemental oxygen can help decrease the alveolar pressure of nitrogen in the body, thus creating a gradient to reabsorb the air from the pleura (mostly composed of nitrogen) into the alveoli and tissues.
-
Conservative management re-expands the lung at an average rate of 2.2 %/day with a 79 % success rate [8].
-
Failure for the pneumothorax to resolve may lead to fibrothorax (fibrous entrapment of the lung).
-
-
Aspiration:
-
A small cannula can be used to aspirate pleural air, with a success rate of 75 and 40 % for a primary and secondary spontaneous pneumothorax, respectively. This technique is rarely used.
-
Can be attached to a Heimlich one-way valve or a three-way stop-cock with a large syringe [9].
-
-
Percutaneous Catheters:
-
Small-calibre tube thoracostomy can be performed percutaneously via the Seldinger technique and attached to either a Heimlich one-way valve or suction.
-
Use is limited to a spontaneous pneumothorax with limited respiratory symptoms.
-
-
Tube Thoracostomy:
-
Large-bore chest tubes are the standard-of-care for treatment of traumatic pneumothoraces, unstable patients, persistent or large air leaks and associated effusions or haemothoraces.
-
Clamping of the tube is controversial. If performed, a follow-up chest radiograph should be done in several hours to assess for re-accumulation.
-
Outpatient management is acceptable with the use of a Heimlich one-way valve [10].
-
Complications of chest tube insertion include: injury to the lung, intercostal vessels, or great vessels, misplacement in the fissures or outside the pleural cavity, infection, and re-expansion pulmonary edema caused with rapid re-expansion leading to increase in capillary permeability.
-
-
The appropriate initial management option should be tailored to the expected size of the air leak.
-
Conservative options include observation, needle aspiration, and small-bore tube thoracostomy connected to an underwater seal. For persistent or larger air leaks, large-bore chest tubes with underwater seal connected to wall suction can be used, with surgery and/or pleurodesis as last resorts [11].
-
Recurrence after spontaneous pneuothorax is 30 % after the first episode, with the majority occurring within 2 years [12]. Independent risk factors for recurrence include: pulmonary fibrosis, age >60 years, increased height/weight ratio [13]. Recurrence rate increases after each episode.
-
Surgery:
-
Guidelines recommend waiting at least 3–5 days for resolution of a spontaneous pneumothorax before considering definitive surgical management [14].
-
A bullectomy can be performed preferably via a VATS approach with a success rate >95 % [15]. Other options including open thoracotomy and axillary approaches.
-
Indications for bullectomy [14]:
-
After the second spontaneous primary pneumothorax
-
After the first spontaneous primary pneumothorax in patients with high-risk professions, or patients exposed to significant changes in atmospheric pressures
-
After the first spontaneous secondary pneumothorax
-
-
-
Pleurodesis:
Pleural Effusions
-
An abnormal collection of fluid in the pleural space
-
Can be transudative (low protein) or exudative (high protein).
-
-
Benign pleural effusions are twice as common as malignant pleural effusions [18] (Table 4.2).
Table 4.2. Benign pleural effusions with incidence in the USA [18].
Pathophysiology [19]: See Chap. 4: Pleural Disorders (Anatomy and Physiology)
-
Increased pulmonary capillary pressure (CHF, renal failure)
-
Increased pulmonary capillary permeability (pneumonia)
-
Decreased intrapleural pressure (atelectasis)
-
Decreased plasma oncotic pressure (hypoalbuminemia)
-
Increased pleural permeability (infection, inflammation)
-
Obstruction of pleural lymphatic drainage (malignancy)
-
Fluid from other sites or cavities (peritoneum, retroperitoneum)
-
Rupture of thoracic vessels (haemothorax, chylothorax)
-
Drugs [18]
Work-Up (Table 4.3)
-
Serum Laboratory: blood count and differential (high white count suggests infection, bleeding, malignancy), serum electrolytes, urea, creatinine, liver function tests and liver enzymes, albumin, lactate dehydrogenase, lipase, cardiac enzymes, electrocardiogram
-
Imaging:
-
Chest X-ray (presence of >250 mL pleural fluid [20])
-
Complicated pleural infections are suggested by abnormal pleural indentation that does not correspond to the effects of gravity on pleural fluid.
-
-
Ultrasound: can identify small effusions and loculations, and can guide thoracocentesis, drain placement and pleural biopsy.
-
CT scan: best imaging study to characterise size, location, presence of loculations and underlying cause of pleural effusions (Fig. 4.3). It can also guide chest drain placement for complicated effusions/empyema.
Fig. 4.3. 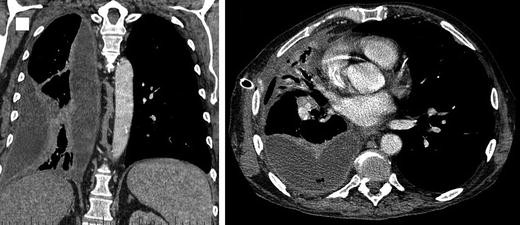
Patient presenting with a parapneumonic effusion that progressed to advanced stage of empyema.
-
Signs of pleural infection include pleural thickening, pleural space air (gas-forming organisms), and the split pleura sign in empyema (pleural fluid encased by distinct thickened visceral and parietal pleura) [21].
-
-
-
Pleural Fluid Sampling: unless the cause of the effusion is known (i.e. CHF) the pleural fluid should be sampled.
-
Pleural Fluid Characteristics [22]:
-
Straw colour (normal, transudate)
-
Turbid/purulent (empyema)
-
Blood (trauma, malignancy, parapneumonic)
-
Enteric content (esophageal rupture)
-
Bile (bilothorax)
-
-
Pleural Fluid Analysis: the following tests should be utilised to characterise the effusion [18, 19]:
-
pH (<7.2 useful for identifying complicated infected effusions)
-
LDH (should be measured in pleural fluid and serum)
-
Protein (pleural fluid and serum)
-
Bacterial culture (some fluid should be additionally placed in blood culture bottles to improve diagnostic accuracy [23, 24]) and Gram Stain
-
Cytology (to detect malignancy)
-
CBC (to identify WBCs from infection, or RBCs from blood)
-
Acid-fast bacilli (AFB) PCR (if lymphocytic effusion is found or TB is a concern especially in endemic regions)
-
-
Light’s Criteria: used to distinguish exudative from transudative pleural effusions. If 1 or more are positive, effusion is exudative [25].
-
Pleural Fluid/Serum Protein ratio >0.5
-
Pleural Fluid/Serum LHD ratio >0.6
-
Pleural Fluid LDH >2/3 the upper limit of normal serum LDH
-
-
-
Pleural Biopsy: can assist the diagnosis of tuberculosis, malignancy, and amyloidosis when diagnosis is uncertain [26].

Pleural Infections (Empyema)
-
Infection of the pleural space (exudative effusion) [27].
-
70–80 % patients may be managed with non-surgical management (drainage + antibiotics + fibrinolytic therapy) [28, 29].
-
Increased incidence in alcoholic and intravenous drug users (risk of aspiration) [30].
Symptoms
-
Similar to pneumonia: pleuritic chest pain, fever, cough, dyspnea, malaise [20]
-
Constitutional symptoms (malaise, fatigue, weight loss, anorexia) in malignant pleural effusions
Causes
-
Direct contamination of pleural space (trauma, surgery)
-
Hematologic spread (bacteremia/sepsis)
-
Direct extension from lung parenchyma (parapneumonic)
-
Rupture of intrapulmonary abscess or infected cavity
-
Bronchopleural fistula
-
Extension from mediastinum (esophageal perforation)
Classification
-
Progression through stages occurs over 3–6 weeks (Fig. 4.4) [27, 31].
Fig. 4.4. 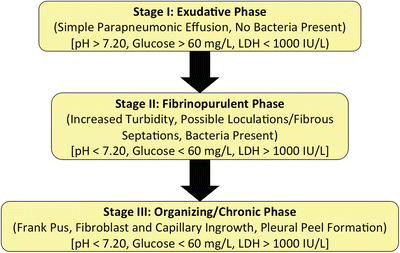
Classification and natural history of empyema.
-
Untreated empyema eventually progresses to fibro-thorax [32].

Microbiology [33]:
-
Community Acquired (85 %):
-
Aerobes (73 %): Streptococci (72 %; S. milleri/anginosus (46 %), S. pneumonia (40 %)), Staphylococci (14 %; MSSA (77 %), MRSA (20 %)), gram-negative (12 %), others (2 %)
-
Anaerobes (22 %)
-
Other (5 %)
-
-
Nosocomial (15 %):
-
Aerobes (88 %): Staphylococci (40 %; MRSA (71 %), MSSA (29 %)), gram-negative (26 %), Streptococci (21 %), Enterococci (13 %)
-
Anaerobes (8 %)
-
Other (4 %)
-
Management
-
Drainage:
-
Historically large bore chest tubes (30–36 Fr) were advocated for drainage of pleural infections due to fear of tube blockage by thick viscous drainage [20].
-
A recent case series using 10–16 Fr tubes of pleural infections reported a 72 % success rate, comparable to large bore (>30 Fr) chest tubes [34].
-
A retrospective analysis of 405 patients treated with chest tube drainage of various sizes (<10 Fr, 10–14 Fr, 15–20 Fr, >20 Fr) revealed no difference in mortality or requirement for decortication [35].
-
No differences in chest radiograph change following drainage, length of stay or pulmonary function after 3 months were noted between tube size groups.
-
Irrigation of pleural cavity can be done with sterile saline following drain insertion, however evidence supporting this practice is lacking [20].
-
-
-
Antibiotics:
-
Patients often present with signs of sepsis.
-
Broad-spectrum antibiotic therapy covering gram-positive, gram-negative (including Pseudomonas) and anaerobic bacteria is indicated.
-
Focus antibiotics once cultures obtained.
-
Antibiotics in pleural fluid typically reach approximately 75 % of serum levels [20].
-
Duration of antibiotics: minimal evidence suggesting optimal duration, however therapy is generally continued for 2–4 weeks following resolution of signs and symptoms in order to achieve clinical resolution, depending on microbiology, response to therapy, extent of disease, adequacy of drainage and patient factors (e.g. immune status).
-
-
Fibrinolytic Therapy (Streptokinase/tPA +/− DNAse):
-
Used as treatment of loculated parapneumonic effusions and empyema.
-
Aimed to reduce incidence of surgical intervention.
-
Meta-analysis of 7 RCTs comparing fibrinolytic therapy to placebo shows reduction in surgical intervention but not in mortality or length of stay [28].
-
Double-blind RCT MIST2 trial evaluating t-PA and DNAse for patients with pleural infection [36].
-
Randomised to 1 of 4 treatments for 3 days: t-PA and DNAse, t-PA and placebo, placebo and DNAse, double placebo.
-
Primary outcome: change in pleural opacity (percentage of hemithorax occupied by effusion on chest X-ray [Mean (+/− SD) change in pleural opacity]).
-
t-PA + DNAse versus placebo:
-
Change in pleural opacity: −29.5 ± 23.3 % vs. −17.2 ± 19.6 %, p=0.005
-
Surgical referral at 3 months: OR 0.17; 95 % CI, 0.03 to 0.87; P = 0.03.
-
Hospital stay (mean difference): −6.7 days; 95 % CI, −12.0 to −1.9; P = 0.006.
-
-
Non-significant for t-PA or DNAse alone versus placebo.
-
-
-
Decortication:
-
Performed by open posterolateral thoracotomy or by VATS
-
Indications:
-
Stages II and III after failure of chest tube drainage, intrapleural fibrinolysis and antibiotic therapy.
-
Late chronic empyema with entrapped lung.
-
-
Provides surgical drainage and allows lung to re-expand eliminating potential space that harbours bacteria.
-
Complete decortication allows for lung re-expansion to tamponade air leak and bleeding [20, 27, 32].
-
VATS Decortication (VATSD) versus Open Thoracotomy Decortication (OD):
-
Risk Stratification
-
UK Multicentre Intrapleural Sepsis Trial (MIST) 1 and 2 RAPID Score [39]:
-
5 factors: age, serum urea, serum albumin, fluid purulence, likely origin of infection
-
Total score out of 7: low, medium and high-risk groups
-
Low-risk (0–2): 5 % mortality risk
-
High-risk (5–7): 50 % mortality risk
-
-
Decision-making tool for earlier fibrinolytic therapy versus surgery.
-
Chylothorax (Table 4.4)
-
A turbid milky white effusion resulting from transection (traumatic) or obstruction of the thoracic duct (TD) or its branches.
-
1.5–2.5 L of lymphatic fluid pass through the TD per day.
-
TD leak results in rapid volume, lymphocyte, nutrition, fat-soluble vitamin and electrolyte losses [40].
-
TD leak can induce immunosuppression in patients [41].
-
1/200 incidence post-thoracic surgery [18].
-
Chylous ascites can also be a source of chylothorax [42].
Pleural Fluid Investigations
-
Lipoprotein electrophoresis: the presence of chylomicrons confirms chyle leak [43].
-
Elevated pleural fluid triglyceride levels (>110 mg/dL).
-
CBC and differential demonstrates >80 % lymphocytes [44].
Thoracic Duct Anatomy
-
Intestinal/Lumbar lymphatics → cysterna chylii (anterior to L1/L2) → aortic hiatus of diaphragm (T12) → right chest (between aorta and azygous vein) → crosses midline at T4 (behind oesophagus) → left posterior mediastinum (behind aorta, left side of oesophagus, behind left subclavian artery) → crosses over left subclavian artery (anterolateral mediastinum) → enters confluence of left jugular and subclavian veins [40].
Treatment—Traumatic Chylothorax (Post-surgical, Trauma)
-
Pleural Effusion Drainage [27]:
-
Chest tube is used to drain the pleural cavity providing symptomatic relief.
-
Monitoring of drain output (milky colour indicating ongoing chyle leak)
-
-
-
Total Parenteral Nutrition (TPN), fasting, or reduced fat diet with Medium Chain Triglyceride (MCT) supplementation.
-
MCT are absorbed by intestinal epithelium into the portal venous circulation bypassing lymphatic absorption and decreasing lymphatic flow to allow duct closure.
-
-
Dietary control measures are usually maintained for 1–2 weeks followed by fat challenge (cream or olive oil PO/PT).
-
Increased milky chest tube drainage indicates failure of conservative management [27].
-
-
Conservative management with dietary control is successful in approximately 50 % of traumatic chylothorax patients [45]. Patients with high output (>1 L/day) are unlikely to respond to conservative management and will require early operative intervention [46].
-
-
Octreotide:
-
Octreotide is a somatostatin analogue with a longer half-life, theorised to decreased lymph flow rate, lymph volume, as well as digestive enzyme release and intestinal absorption of fatty acids.
-
Prescribed as 50 μg SC/IV q8h
-
Initial case series and case reports show some success using octreotide or somatostatin to decrease chyle leak rates however RCTs are lacking [47].
-
-
Surgical Management (TD Ligation):
-
Indications:
-
Failed conservative management
-
High output leaks (>1 L/day) [45]
-
-
Operative options include: mass ligation of tissue at diaphragmatic hiatus, duct ligation at diaphragmatic hiatus, direct closure of duct injury [27]
-
Can be approached via right thoracotomy or right-side VATS
-
Olive oil or cream is given PO prior to surgery to improve recognition of duct injury site [27]
-
Some surgeons recommend early operative treatment (within 1 week, if patient can tolerate additional surgery) to minimise nutrient loss and immunosuppression from ongoing leak [49–51].
-
-
TD Embolisation (available only in selected centres):
-
TD cannulation rate: 67 %; 90 % resolution of chyle leak post-embolisation [52].
-
-
Prevention:
-
Preoperative oral administration of milk has been shown to facilitate thoracic duct visualisation (95 % vs. 13 %) and decrease risk of duct injury (7 % vs. 13 %) [53].
-
Treatment—Non-traumatic Chylothorax
-
Treatment of non-traumatic chylothorax focuses on the treatment of the underlying disease responsible. Concurrent conservative therapy should be instigated (drainage, diet/TPN, +/− octreotide) [54].
-
Failure of resolution following treatment of disease requires further intervention [54].
-
For malignant chylothorax effusions sclerosant pleurodesis via chest tube or VATS is recommended.
-
For benign or idiopathic chylothorax effusions, thoracoscopic Talc pleurodesis and TD ligation is recommended [45, 58].
Malignant pleural effusion (MPE)
-
Exudative pleural effusion resulting from metastases to pleura
-
Approximately 22 % of pleural effusions in the United States; >150,000 cases annually [59]
-
Most common causes include metastatic lung, breast, colon and ovarian cancer [19, 60]
-
Mean life expectancy of 4–6 months from effusion onset [61, 62]
-
Treatment is aimed at palliation of symptoms. Small asymptomatic effusions can be followed [19, 60].
Therapeutic Thoracocentesis
-
Symptomatic patients can receive serial thoracocentesis, due to the high likelihood of recurrence within weeks following each drainage [19].
-
Appropriate for patients with low life expectancy (less than time for recurrence), too frail to receive pleurodesis, or slow pleural effusion recurrence (time to recurrence >1 month) [60].
-
Risk of re-expansion pulmonary edema from rapid drainage of large effusions, pneumothorax, and empyema with repeated drainages. Repeated thoracocenteses also produce adhesions which can diminish success of subsequent procedures [62].
Permanent Indwelling Pleural Catheters (IPC)
-
Indwelling pleural catheter, which patients can drain manually and achieve long-term control.
-
Day procedure inserted under local anaesthesia.
-
Spontaneous pleurodesis following placement in 40–50 % of patients. When drainage <50 cc/day for 3 days, catheter can be removed [60, 63].
-
Indications for catheter placement [60]:
-
Rapid effusion accumulation (<1 month)
-
Life expectancy <3 months
-
Trapped lung
-
Poor operative candidate
-
Failure of chemical pleurodesis
-
-
Contraindications [60]:
-
Slow effusion accumulation (>1 month)
-
Intrapleural adhesions preventing insertion
-
-
Disadvantages: home nursing care of catheter required
-
Complications: re-expansion pulmonary edema (patients instructed not to drain >1000 mL/h), catheter malfunction (9.1 %), pneumothorax requiring chest tube (5.9 %), pain (5.6 %), blocked catheter (3.7 %), empyema (2.8 %), cellulitis (3.4 %), IPC fracture during removal [64]
Pleurodesis
-
Involves initial drainage of effusion, pulmonary re-expansion, and injection of sclerosant into pleural cavity via thoracostomy tube.
-
Sclerosants include Talc powder, bleomycin and tetracycline derivatives with success rates of 81–100 %, 61 and 65–76 % respectively using tube thoracostomy instillation [64].
-
Local anaesthetics such as lidocaine are often co-injected with sclerosants [65].
-
A cost-effective analysis demonstrated chest tube chemical pleurodesis as more cost-effective than IPC placement when patient survival >6 weeks [66].
-
Contraindicated in patients who are extremely frail, have an extremely short life expectancy or have trapped lung preventing lung re-expansion (requirement for success of pleurodesis) [19].
-
Appropriately selected patients with trapped lung and MPE (a contraindication to simple bed-side pleurodesis) can receive symptomatic benefit from VATS pleurectomy, decortication and pleurodesis [32].
-
Cochrane Review Pleurodesis for Malignant Effusions (2004) [67]:
-
Relative Risk (RR) of effusion non-recurrence with sclerosant versus tube thoracostomy drainage alone 1.20 (95 % CI 1.04–1.38) favours using sclerosant [5 studies, 228 subjects].
-
RR of effusion non-recurrence using Talc versus all other sclerosants (tetracycline, bleomycin, mustine and tube thoracostomy drainage alone) 1.34 (95 % CI 1.16–1.55) favours Talc [10 studies, 308 subjects].
-
RR of effusion non-recurrence using thoracoscopic versus bedside tube thoracostomy instillation of Talc 1.19 (95 % CI 1.04–1.36) favours thoracoscopic instillation [2 studies, 112 subjects].
-
RR of effusion non-recurrence using thoracoscopic versus tube thoracostomy bedside instillation of all sclerosants (Talc, tetracycline, bleomycin, mustine) 1.68 (95 % CI 1.35–2.10) favours thoracoscopic instillation [five studies, 145 subjects].
-
General Tube Thoracostomy Pleurodesis Technique (Malignant Effusion)
-
Chest Drainage:
-
Tube thoracostomy placement, effusion drainage and lung re-expansion
-
-
Analgesia:
-
Prior to sclerosant injection intrapleural injection of lidocaine 3 mg/kg (maximum 250 mg) via chest tube is recommended [62]. Alternatively lidocaine may be added to a normal saline Talc solution.
-
Narcotic analgesia is recommended (+/− amnestic agent i.e. midazolam).
-
-
Sclerosant Options:
-
Talc: 5 g of Talc are dissolved in 100 cc normal saline and placed in two 60 cc Toomey syringes (3 g of Talc are sufficient for pleurodesis for pneumothorax).
-
Size-calibrated Talc, <10 % 5–10 μm diameter, is preferred as small particle Talc has been linked to systemic absorption, systemic inflammation and ARDS [68].
-
-
Injection of Sclerosant:
-
Total volume of sclerosant is injected via tube thoracostomy with patient in supine position.
-
Tube thoracostomy is clamped for 1 h.
-
Some recommend periodic patient reposition every 15 min (supine, left lateral decubitus, prone, right lateral decubitus) during pleurodesis to allow sclerosant to pool throughout pleural cavity, however this technique is equivalent to patients remaining supine [71].
-
After 1 h, the chest tube is placed under −20 cm H2O wall suction.
-
-
Drain Removal:
-
Chest tubes are removed after 24 h or when drainage is <150 cc/day.
-
A randomised trial of 41 patients who received pleurodesis for malignant effusion showed no difference in complications or pleurodesis success between short-term and long-term drainage following pleurodesis [72].
-
Tumours of the Pleura: Malignant Pleural Mesothelioma
-
Primary tumours of the pleura are very rare. There are two main types:
-
Malignant Pleural Mesothelioma (MM): most common primary tumour of the pleura. Highly aggressive tumour with grave prognosis.
-
Localised Fibrous Tumour of the Pleura: significantly less aggressive than MM, also referred to as “localised mesothelioma.”
Epidemiology
-
Strong association with asbestos exposure (>80 % of cases), with 20-years latency until the development of MM.
-
5:1 Male predominance, with peak incidence in the sixth-seventh decade.
-
Other causes: radiation, mineral fibres, simian virus 40.
Clinical Presentation
-
Dyspnea
-
Pain—secondary to chest wall invasion and involvement of somatic nerves of the parietal pleura
-
Malignant pleural effusion
-
Pleural thickening, subtle pleural masses on radiographic images
-
Thick, restrictive pleural rind (late finding) with encasement of the lung
-
Work-Up
-
CT chest with IV contrast +/− FDG-PET
-
MRI as an adjunct to determine depth of chest wall invasion or diaphragmatic involvement
-
Thoracocentesis of malignant effusion: cytology and elevated pleural hyaluronic acid have a 50 % diagnostic accuracy.
-
Gold standard for diagnosis is thoracoscopic pleural biopsy.
-
80 % Diagnostic accuracy
-
Management
-
Most patients present with locally advanced disease—not amenable to surgical treatment options.
-
Surgery is reserved for patients with localised and selected locally advanced disease.
-
Surgery is provided in the context of multi-modality therapy (neoadjuvant or adjuvant chemotherapy and adjuvant whole thorax radiation therapy), with improvement in overall survival and disease-free survival depending on tumour histopathology and regimen.
-
-
Extrapleural Pneumonectomy (EPP): en-bloc resection of the lung, visceral pleura, parietal pleura, pericardium, hemidiaphragm.
-
Extended Pleurectomy/Decortication: less aggressive surgical option than EPP.
-
Mortality: 0–2 %
-
>95 % patient compliance with multimodality therapy [74]
-
-
The optimal surgical option remains controversial. Despite the decrease in cytoreduction compared to EPP, one recent non-randomised trial reports extended pleurectomy/decortication to have improved median survival (23 months vs. 13 months), 2-years survival (49 % vs. 18 %) and 5-years survival (30 % vs. 9 %) [74].
-
Whole thorax radiation therapy in conjunction with surgery improves local control.
-
Unfortunately, patients with locoregional control from radiotherapy develop systemic disease with limited benefit from chemotherapy (cisplatin/premetrexed: 12-months median survival) [75].
-
Palliative options: pleurodesis or indwelling pleural catheter drainage to improve quality of life.
References
Noppen M et al. Volume and cellular content of normal pleural fluid in humans examined by pleural lavage. Am J Respir Crit Care Med. 2000;162(3 Pt 1):1023–6.
Miserocchi G. Physiology and pathophysiology of pleural fluid turnover. Eur Respir J. 1997;10(1):219–25.
Melton 3rd LJ, Hepper NG, Offord KP. Incidence of spontaneous pneumothorax in Olmsted County, Minnesota, 1950 to 1974. Am Rev Respir Dis. 1979;120(6):1379–82.
Bense L et al. Nonsmoking, non-alpha 1-antitrypsin deficiency-induced emphysema in nonsmokers with healed spontaneous pneumothorax, identified by computed tomography of the lungs. Chest. 1993;103(2):433–8.
Alifano M et al. Atmospheric pressure influences the risk of pneumothorax: beware of the storm! Chest. 2007;131(6):1877–82.
Dulchavsky SA et al. Prospective evaluation of thoracic ultrasound in the detection of pneumothorax. J Trauma. 2001;50(2):201–5.
Blaivas M, Lyon M, Duggal S. A prospective comparison of supine chest radiography and bedside ultrasound for the diagnosis of traumatic pneumothorax. Acad Emerg Med. 2005;12(9):844–9.
Kelly AM et al. Estimating the rate of re-expansion of spontaneous pneumothorax by a formula derived from computed tomography volumetry studies. Emerg Med J. 2006;23(10):780–2.
Baumann MH, Strange C. Treatment of spontaneous pneumothorax: a more aggressive approach? Chest. 1997;112(3):789–804.
Brims FJ, Maskell NA. Ambulatory treatment in the management of pneumothorax: a systematic review of the literature. Thorax. 2013;68(7):664–9.
MacDuff A et al. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65 Suppl 2:ii18–31.
O’Rourke JP, Yee ES. Civilian spontaneous pneumothorax. Treatment options and long-term results. Chest. 1989;96(6):1302–6.
Lippert HL et al. Independent risk factors for cumulative recurrence rate after first spontaneous pneumothorax. Eur Respir J. 1991;4(3):324–31.
Baumann MH et al. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest. 2001;119(2):590–602.
Naunheim KS et al. Safety and efficacy of video-assisted thoracic surgical techniques for the treatment of spontaneous pneumothorax. J Thorac Cardiovasc Surg. 1995;109(6):1198–203. discussion 1203-4.
Heffner JE et al. Clinical efficacy of doxycycline for pleurodesis. Chest. 1994;105(6):1743–7.
Kennedy L, Sahn SA. Talc pleurodesis for the treatment of pneumothorax and pleural effusion. Chest. 1994;106(4):1215–22.
Thomas R, Lee YC. Causes and management of common benign pleural effusions. Thorac Surg Clin. 2013;23(1):25–42. v-vi.
Quinn T et al. Decision making and algorithm for the management of pleural effusions. Thorac Surg Clin. 2013;23(1):11–6. v.
Bhatnagar R, Maskell NA. Treatment of complicated pleural effusions in 2013. Clin Chest Med. 2013;34(1):47–62.
Aquino SL, Webb WR, Gushiken BJ. Pleural exudates and transudates: diagnosis with contrast-enhanced CT. Radiology. 1994;192(3):803–8.
McGrath EE, Anderson PB. Diagnosis of pleural effusion: a systematic approach. Am J Crit Care. 2011;20(2):119–27. quiz 128.
Ferrer A et al. Prospective clinical and microbiological study of pleural effusions. Eur J Clin Microbiol Infect Dis. 1999;18(4):237–41.
Menzies SM et al. Blood culture bottle culture of pleural fluid in pleural infection. Thorax. 2011;66(8):658–62.
Light RW et al. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med. 1972;77(4):507–13.
Maskell NA, Butland RJ. BTS guidelines for the investigation of a unilateral pleural effusion in adults. Thorax. 2003;58 Suppl 2:ii8–17.
Sugarbaker DJ, Lukanich JM. Lung, chest wall, pleura and mediastinum. In: Townsend CM et al., editors. Sabiston textbook of surgery. Philadelphia, PA, USA: Elsevier Inc.; 2012. p. 1564–610.
Janda S, Swiston J. Intrapleural fibrinolytic therapy for treatment of adult parapneumonic effusions and empyemas: a systematic review and meta-analysis. Chest. 2012;142(2):401–11.
Abu-Daff S et al. Intrapleural fibrinolytic therapy (IPFT) in loculated pleural effusions-analysis of predictors for failure of therapy and bleeding: a cohort study. BMJ Open. 2013;3(2). pii: e001887.
Chalmers JD et al. Risk factors for complicated parapneumonic effusion and empyema on presentation to hospital with community-acquired pneumonia. Thorax. 2009;64(7):592–7.
MacIver RH. Benign pleural disease. In: Meury CM, Turek JW, editors. TRSA review of cardiothoracic surgery. Chicago, IL, USA: TRSA/TSDA; 2011. p. 54–5.
Rathinam S, Waller DA. Pleurectomy decortication in the treatment of the “trapped lung” in benign and malignant pleural effusions. Thorac Surg Clin. 2013;23(1):51–61. vi.
Bartlett JG et al. Bacteriology of empyema. Lancet. 1974;1(7853):338–40.
Liu YH et al. Ultrasound-guided pigtail catheters for drainage of various pleural diseases. Am J Emerg Med. 2010;28(8):915–21.
Rahman NM et al. The relationship between chest tube size and clinical outcome in pleural infection. Chest. 2010;137(3):536–43.
Rahman NM et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection. N Engl J Med. 2011;365(6):518–26.
Chambers A et al. Is video-assisted thoracoscopic surgical decortication superior to open surgery in the management of adults with primary empyema? Interact Cardiovasc Thorac Surg. 2010;11(2):171–7.
Luh SP et al. Video-assisted thoracoscopic surgery in the treatment of complicated parapneumonic effusions or empyemas: outcome of 234 patients. Chest. 2005;127(4):1427–32.
Rahman NM, Kahan BC, Miller RF, Gleeson FV, Nunn AJ, Maskell NA. A clinical score (RAPID) to identify those at risk for poor outcome at presentation in patients with pleural infection. Chest. 2014;145(4):848–55.
Valentine VG, Raffin TA. The management of chylothorax. Chest. 1992;102(2):586–91.
Franksson C et al. Drainage of thoracic duct lymph in renal transplant patients. Transplantation. 1976;21(2):133–40.
Doerr CH et al. Etiology of chylothorax in 203 patients. Mayo Clin Proc. 2005;80(7):867–70.
Maldonado F et al. Pleural fluid characteristics of chylothorax. Mayo Clin Proc. 2009;84(2):129–33.
Huggins JT. Chylothorax and cholesterol pleural effusion. Semin Respir Crit Care Med. 2010;31(6):743–50.
Maldonado F et al. Medical and surgical management of chylothorax and associated outcomes. Am J Med Sci. 2010;339(4):314–8.
Cerfolio RJ et al. Postoperative chylothorax. J Thorac Cardiovasc Surg. 1996;112(5):1361–5. discussion 1365–6.
Kalomenidis I. Octreotide and chylothorax. Curr Opin Pulm Med. 2006;12(4):264–7.
Paul S et al. Surgical management of chylothorax. Thorac Cardiovasc Surg. 2009;57(4):226–8.
Orringer MB, Bluett M, Deeb GM. Aggressive treatment of chylothorax complicating transhiatal esophagectomy without thoracotomy. Surgery. 1988;104(4):720–6.
Lagarde SM et al. Incidence and management of chyle leakage after esophagectomy. Ann Thorac Surg. 2005;80(2):449–54.
Shirai T, Amano J, Takabe K. Thoracoscopic diagnosis and treatment of chylothorax after pneumonectomy. Ann Thorac Surg. 1991;52(2):306–7.
Itkin M et al. Nonoperative thoracic duct embolization for traumatic thoracic duct leak: experience in 109 patients. J Thorac Cardiovasc Surg. 2010;139(3):584–9. discussion 589–90.
Shen Y et al. A simple method minimizes chylothorax after minimally invasive esophagectomy. J Am Coll Surg. 2014;218(1):108–12.
McGrath EE, Blades Z, Anderson PB. Chylothorax: aetiology, diagnosis and therapeutic options. Respir Med. 2010;104(1):1–8.
Andalib A et al. Influence of postoperative infectious complications on long-term survival of lung cancer patients: a population-based cohort study. J Thorac Oncol. 2013;8(5):554–61.
Mares DC, Mathur PN. Medical thoracoscopic talc pleurodesis for chylothorax due to lymphoma: a case series. Chest. 1998;114(3):731–5.
Ferguson MK. Thoracoscopy for empyema, bronchopleural fistula, and chylothorax. Ann Thorac Surg. 1993;56(3):644–5.
Graham DD et al. Use of video-assisted thoracic surgery in the treatment of chylothorax. Ann Thorac Surg. 1994;57(6):1507–11. discussion 1511–2.
American Thoracic Society. Management of malignant pleural effusions. Am J Respir Crit Care Med. 2000;162(5):1987–2001.
Gillen J, Lau C. Permanent indwelling catheters in the management of pleural effusions. Thorac Surg Clin. 2013;23(1):63–71. vi.
Burrows CM, Mathews WC, Colt HG. Predicting survival in patients with recurrent symptomatic malignant pleural effusions: an assessment of the prognostic values of physiologic, morphologic, and quality of life measures of extent of disease. Chest. 2000;117(1):73–8.
Roberts ME et al. Management of a malignant pleural effusion: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65 Suppl 2:ii32–40.
Light RW. Counterpoint: should thoracoscopic talc pleurodesis be the first choice management for malignant pleural effusion? No Chest. 2012;142(1):17–9. discussion 19–20.
Lee P. Point: should thoracoscopic talc pleurodesis be the first choice management for malignant effusion? Yes Chest. 2012;142(1):15–7. discussion 20–1.
Feller-Kopman D et al. The relationship of pleural pressure to symptom development during therapeutic thoracentesis. Chest. 2006;129(6):1556–60.
Olden AM, Holloway R. Treatment of malignant pleural effusion: PleuRx catheter or talc pleurodesis? A cost-effectiveness analysis. J Palliat Med. 2010;13(1):59–65.
Shaw P, Agarwal R. Pleurodesis for malignant pleural effusions. Cochrane Database Syst Rev. 2004;1, CD002916.
Gonzalez AV et al. Lung injury following thoracoscopic talc insufflation: experience of a single North American center. Chest. 2010;137(6):1375–81.
Putnam Jr JB et al. A randomized comparison of indwelling pleural catheter and doxycycline pleurodesis in the management of malignant pleural effusions. Cancer. 1999;86(10):1992–9.
Nikbakhsh N, Pourhasan Amiri A, Hoseinzadeh D. Bleomycin in the treatment of 50 cases with malignant pleural effusion. Caspian J Intern Med. 2011;2(3):274–8.
Tan C et al. The evidence on the effectiveness of management for malignant pleural effusion: a systematic review. Eur J Cardiothorac Surg. 2006;29(5):829–38.
Goodman A, Davies CW. Efficacy of short-term versus long-term chest tube drainage following talc slurry pleurodesis in patients with malignant pleural effusions: a randomised trial. Lung Cancer. 2006;54(1):51–5.
Cao C et al. Systematic review of trimodality therapy for patients with malignant pleural mesothelioma. Ann Cardiothorac Surg. 2012;1(4):428–37.
Lang-Lazdunski L et al. Pleurectomy/decortication is superior to extrapleural pneumonectomy in the multimodality management of patients with malignant pleural mesothelioma. J Thorac Oncol. 2012;7(4):737–43.
Vogelzang NJ et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol. 2003;21(14):2636–44.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Gowing, S.D., Madani, A. (2015). Pleural Disorders. In: Madani, A., Ferri, L., Seely, A. (eds) Pocket Manual of General Thoracic Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-17497-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-17497-6_4
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-17496-9
Online ISBN: 978-3-319-17497-6
eBook Packages: MedicineMedicine (R0)